Development of a Self-Harm Monitoring System for Victoria

 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Objective
3. Materials and Methods
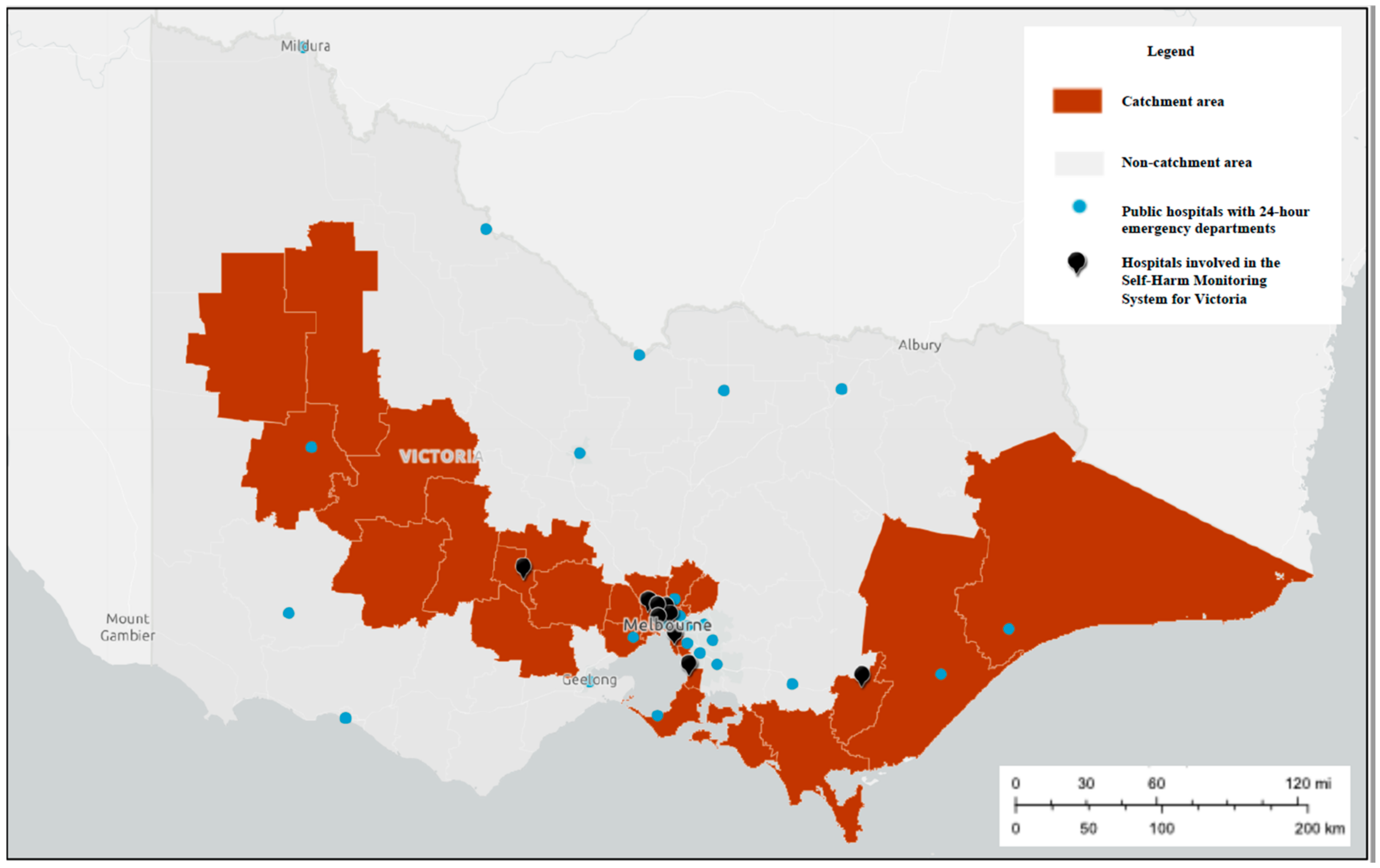
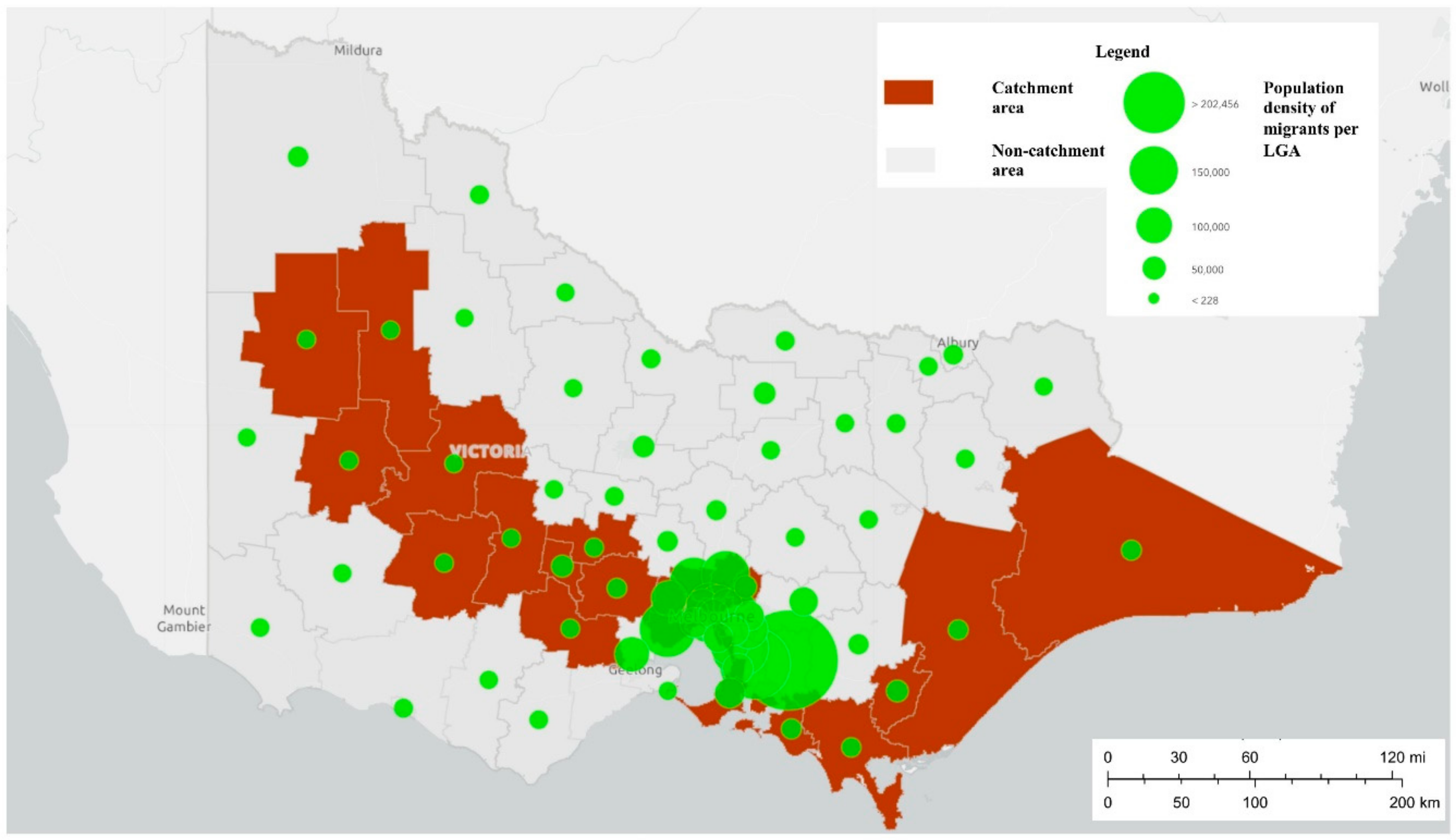
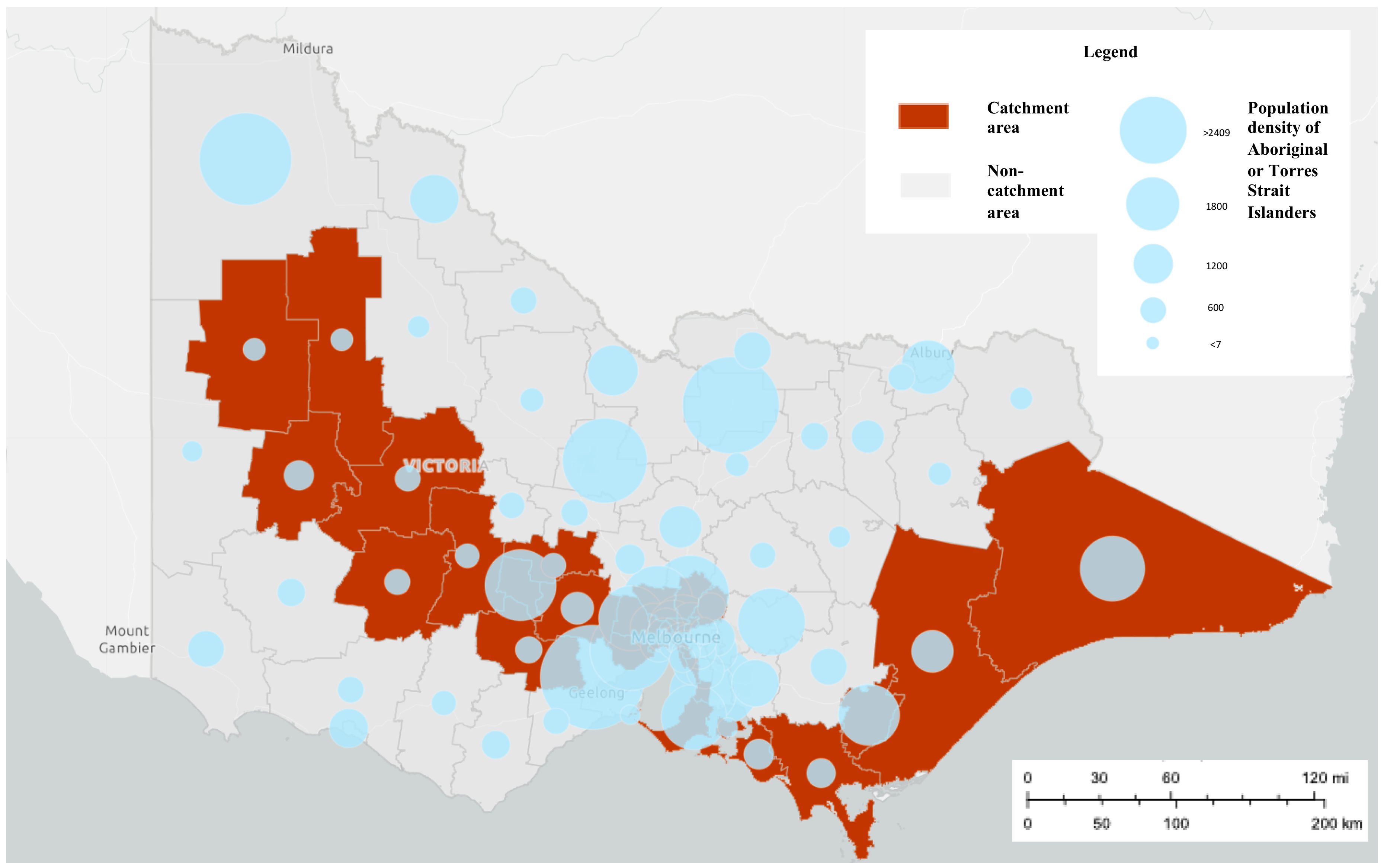
3.1. Setting
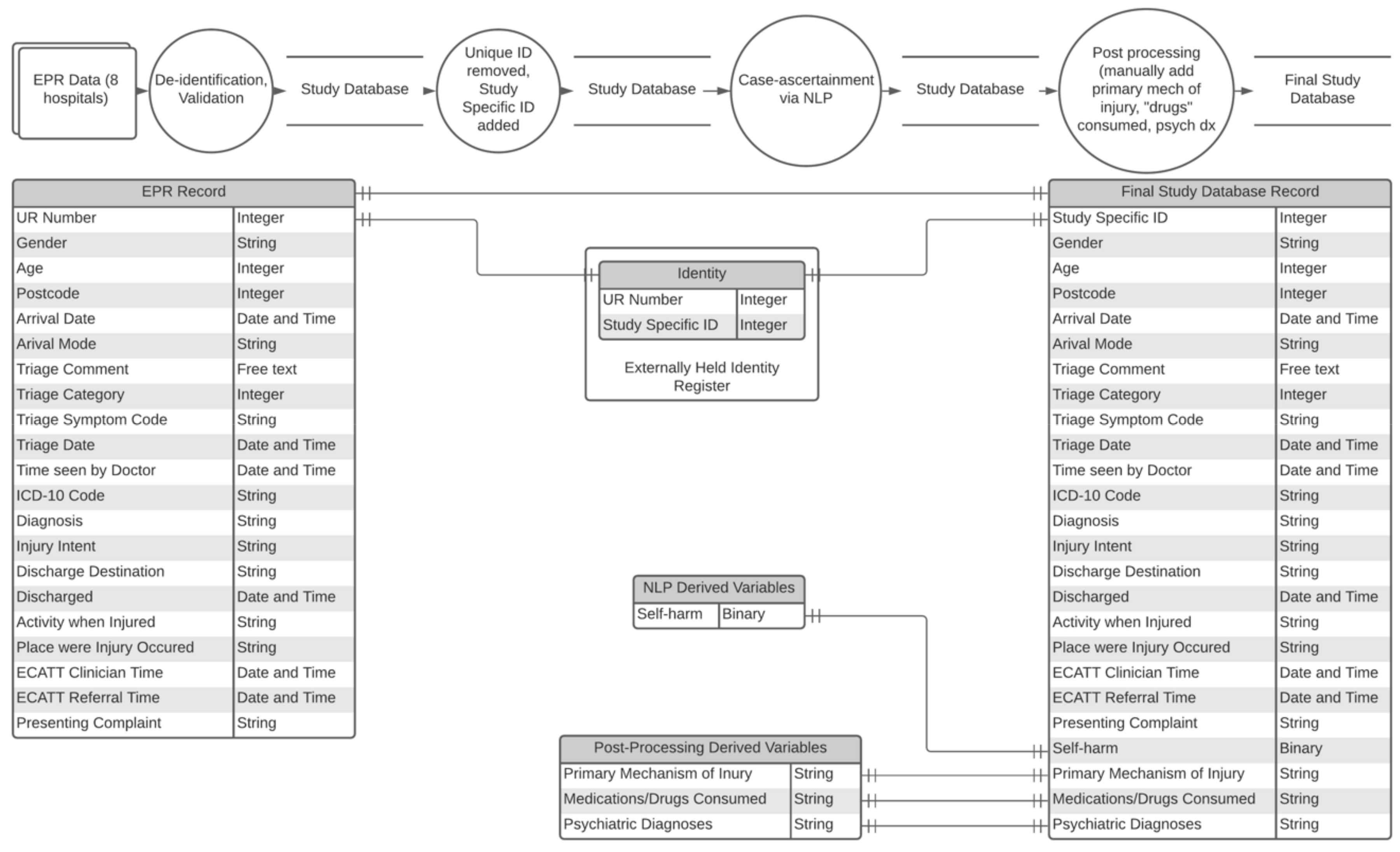
3.2. Data Sources
3.3. Inclusion and Exclusion Criteria
3.4. Natural Language Processing for Case Ascertainment
3.5. Post-Processing
3.6. Quality
3.7. Data Analysis
3.8. Prevalence and Characteristics of Self-Harm Presentations
3.9. Characterising the Demographic, Clinical and Treatment Characteristics of Those Who Present to EDs Following Self-Harm
3.10. Informing Real-Time (or Close to Real-Time) Responses to Self-Harm
3.11. Inform the Development, and Evaluation, of Clinical and Policy Initiatives
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Australian Bureau of Statistics. 3303.0 Causes of Death, Australia, 2018; Australian Bureau of Statistics: Canberra, ACT, Australia, 2019.
- Bergen, H.; Hawton, K.; Waters, K.; Ness, J.; Cooper, J.; Steeg, S.; Kapur, N. Premature death after self-harm: A multicentre cohort study. Lancet 2012, 380, 1568–1574. [Google Scholar] [CrossRef]
- Pointer, S. Trends in Hospitalised Injury, AUSTRALIA 1999/2000 to 2012/2013; Australian Institute of Health and Welfare: Canberra, ACT, Australia, 2015.
- Australian Bureau of Statistics. 3303.0 Causes of Death, Australia, 2013; Australian Bureau of Statistics: Canberra, ACT, Australia, 2014.
- Mars, B.; Heron, J.; Crane, C.; Hawton, K.; Lewis, G.; MacLeod, J.; Tilling, K.; Gunnell, D. Clinical and social outcomes of adolescent self harm: Population based birth cohort study. BMJ 2014, 349, g5954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, P.; Coffey, C.; Romaniuk, H.; Degenhardt, L.; Borschmann, R.; Patton, G.C. Substance use in adulthood following adolescent self-harm: A population-based cohort study. Acta Psychiatr. Scand. 2014, 131, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman-Mellor, S.J.; Caspi, A.; Harrington, H.; Hogan, S.; Nada-Raja, S.; Poulton, R.; Moffitt, T.E. Suicide Attempt in Young People. JAMA Psychiatry 2014, 71, 119–127. [Google Scholar] [CrossRef]
- Pridmore, S.; Auchincloss, S. Book reviews: Preventing suicide: A global imperative. Australas. Psychiatry 2015, 23, 81–82. [Google Scholar] [CrossRef]
- National Suicide Prevention Project Reference Group. National Suicide Prevention Implementation Strategy 2020–2025: Working Together to Save Lives; National Suicide Prevention Project: Canberra, ACT, Australia, 2019.
- Commonwealth of Australia. The Fifth National Mental Health and Suicide Prevention Plan; Department of Health: Canberra, ACT, Australia, 2017.
- National Mental Health Commission. National Suicide and Self-Harm Monitoring System; National Mental Health Commission: Canberra, ACT, Australia, 2020.
- Gill, P.J.; Saunders, N.; Gandhi, S.; Gonzalez, A.; Kurdyak, P.; Vigod, S.; Guttmann, A. Emergency Department as a First Contact for Mental Health Problems in Children and Youth. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 475–482.e4. [Google Scholar] [CrossRef] [Green Version]
- Saunders, N.R.; Gill, P.J.; Holder, L.; Vigod, S.; Kurdyak, P.; Gandhi, S.; Guttmann, A. Use of the emergency department as a first point of contact for mental health care by immigrant youth in Canada: A population-based study. Can. Med. Assoc. J. 2018, 190, E1183–E1191. [Google Scholar] [CrossRef] [Green Version]
- Gairin, I.; House, A.; Owens, D. Attendance at the accident and emergency department in the year before suicide: Retrospective study. Br. J. Psychiatry 2003, 183, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Guelayov, G.; Casey, D.; Bale, L.; Brand, F.; Clements, C.; Farooq, B.; Kapur, N.; Ness, J.; Waters, K.; Tsiachristas, A.; et al. Suicide following presentation to hospital for non-fatal self-harm in the Multicentre Study of Self-harm: A long-term follow-up study. Lancet Psychiatry 2019, 6, 1021–1030. [Google Scholar] [CrossRef] [Green Version]
- Kuramoto-Crawford, S.J.; Spies, E.L.; Davies-Cole, J. Detecting Suicide-Related Emergency Department Visits Among Adults Using the District of Columbia Syndromic Surveillance System. Public Health Rep. 2017, 132, 88S–94S. [Google Scholar] [CrossRef]
- Public Health Agency. Northern Ireland Register of Self-harm: Regional Three-Year Report, 2012/13 to 2014/15. 2015. Available online: https://www.publichealth.hscni.net/sites/default/files/NIRSH%203%20year%20report%2014.11.06.pdf (accessed on 27 November 2020).
- Griffin, E.; McTernan, N.; Wrigley, C.; Nicholson, S.; Arensman, E.; Williamson, E.; Corcoran, P. National Self-Harm Registry Ireland Annual Report 2018; National Suicide Research Foundation: Cork, Ireland, 2019. [Google Scholar]
- Metzger, M.-H.; Tvardik, N.; Gicquel, Q.; Bouvry, C.; Poulet, E.; Potinet-Pagliaroli, V. Use of emergency department electronic medical records for automated epidemiological surveillance of suicide attempts: A French pilot study. Int. J. Methods Psychiatr. Res. 2016, 26, e1522. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Bergen, H.; Casey, D.; Simkin, S.; Palmer, B.; Cooper, J.; Kapur, N.; Horrocks, J.; House, A.; Lilley, R.; et al. Self-harm in England: A tale of three cities. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 513–521. [Google Scholar] [CrossRef]
- Williams, S. Establishing a self-harm surveillance register to improve care in a general hospital. Br. J. Ment. Health Nurs. 2015, 4, 20–25. [Google Scholar] [CrossRef]
- Multicentre Study of Self-Harm in England Multicentre Study of Self-Harm in England. 2018. Available online: http://cebmh.warne.ox.ac.uk/csr/mcm/index.html (accessed on 27 November 2020).
- Witt, K.; Robinson, J. Sentinel Surveillance for Self-Harm. Crisis 2019, 40, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, H.; Schoenbaum, M.; Claassen, C.; Crosby, A.; Holland, K.; Proescholdbell, S. Issues in Developing a Surveillance Case Definition for Nonfatal Suicide Attempt and Intentional Self-harm Using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) Coded Data. Natl. Health Stat. Rep. 2018, 108, 1–19. [Google Scholar]
- Sveticic, J.; Stapelberg, N.C.; Turner, K. Suicidal and self-harm presentations to Emergency Departments: The challenges of identification through diagnostic codes and presenting complaints. Health Inf. Manag. J. 2019, 49, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Saunders, L.D.; Parsons, G.A.; Nilsson, C.I.; Alibhai, A.; Ghali, W.A.; for the IMECCHI Investigators. Assessing Validity of ICD-9-CM and ICD-10 Administrative Data in Recording Clinical Conditions in a Unique Dually Coded Database. Health Serv. Res. 2008, 43, 1424–1441. [Google Scholar] [CrossRef] [Green Version]
- Walkup, J.T.; Townsend, L.; Crystal, S.; Olfson, M. A systematic review of validated methods for identifying suicide or suicidal ideation using administrative or claims data. Pharmacoepidemiol. Drug Saf. 2012, 21, 174–182. [Google Scholar] [CrossRef]
- Bethell, J.; Bondy, S.J.; Lou, W.Y.W.; Guttmann, A.; Rhodes, A.E. Emergency Department Presentations for Self-harm Among Ontario Youth. Can. J. Public Health 2013, 104, e124–e130. [Google Scholar] [CrossRef]
- Randall, J.R.; Roos, N.P.; Lix, L.M.; Katz, L.Y.; Bolton, J. Emergency department and inpatient coding for self-harm and suicide attempts: Validation using clinician assessment data. Int. J. Methods Psychiatr. Res. 2017, 26, 1559. [Google Scholar] [CrossRef] [Green Version]
- Hiles, S.A.; Bergen, H.; Hawton, K.; Lewin, T.; Whyte, I.; Carter, G. General hospital-treated self-poisoning in England and Australia: Comparison of presentation rates, clinical characteristics and aftercare based on sentinel unit data. J. Psychosom. Res. 2015, 78, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.; McGill, K.; Lewin, T.J.; Bryant, J.; Whyte, I.; Carter, G. Hospital-treated deliberate self-poisoning in the older adult: Identifying specific clinical assessment needs. Aust. N. Z. J. Psychiatry 2020, 54, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.J.; Hammond, T.E.; Brownhill, S.; Anand, M.; De La Riva, A.; Hawkins, J.; Chapman, T.; Baldacchino, R.; Micallef, J.-A.; Andepalli, J.; et al. SMS SOS: A randomized controlled trial to reduce self-harm and suicide attempts using SMS text messaging. BMC Psychiatry 2019, 19, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clapperton, A. Identifying typologies among persons admitted to hospital for non-fatal intentional self-harm in Victoria, Australia. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 1497–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Bureau of Statistics. 3101.0—Australian Demographic Statistics, 2018; Australian Burearu of Statistics: Canberra, ACT, Australia, 2019.
- World Health Organization. Practice Manual for Establishing and Maintaining Surveillance Systems for Suicide Attempts and Self-Harm; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Perry, I.; Corcoran, P.; Fitzgerald, A.; Keeley, H.; Reulbach, U.; Arensman, E. The incidence and repetition of hospital-treated deliberate self-harm: Findings from the world’s first national registry. PLoS ONE 2012, 7, e31663. [Google Scholar] [CrossRef] [PubMed]
- Whyte, I.M.; Dawson, A.H.; Carter, G.; Levey, C.M.; Buckley, N.A. A model for the management of self-poisoning. Med. J. Aust. 1997, 167, 142–146. [Google Scholar] [CrossRef]
- Andover, M.; Morris, B.W.; Wren, A.; Bruzzese, M.E. The co-occurrence of non-suicidal self-injury and attempted suicide among adolescents: Distinguishing risk factors and psychosocial correlates. Child. Adolesc. Psychiatry Ment. Health 2012, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- De Beurs, D.; Vancayseele, N.; Van Borkulo, C.; Portzky, G.; Van Heeringen, K. The association between motives, perceived problems and current thoughts of self-harm following an episode of self-harm. A network analysis. J. Affect. Disord. 2018, 240, 262–270. [Google Scholar] [CrossRef]
- Hammond, K.W.; Laundry, R.J.; Oleary, T.M.; Jones, W.P. Use of Text Search to Effectively Identify Lifetime Prevalence of Suicide Attempts among Veterans. In Proceedings of the 46th Hawaii Internatioanl Conference of Systems Science, Maui, HI, USA, 7–10 January 2013; Volume 46, pp. 2676–2683. [Google Scholar]
- Summers, P.; O’Loughlin, R.; O’Donnell, S.; Borschmann, R.; Carlin, J.; Hiscock, H. Repeated presentation of children and adolescents to the emergency department following self-harm: A retrospective audit of hospital data. Emerg. Med. Australas. 2020, 32, 320–326. [Google Scholar] [CrossRef]
- Kocbek, S.; Verspoor, K.; Buntine, W. Exploring temporal patterns in emergency department triage notes with topic models. In Proceedings of the Australasian Language Technology Association Workshop, Melbourne, VIC, Australia, 26–28 November 2014; Volume 1, pp. 113–117. [Google Scholar]
- Sterling, N.W.; Patzer, R.E.; Di, M.; Schrager, J. Prediction of emergency department patient disposition based on natural language processing of triage notes. Int. J. Med. Inform. 2019, 129, 184–188. [Google Scholar] [CrossRef]
- Horng, S.; Sontag, D.; Halpern, Y.; Jernite, Y.; Shapiro, N.I.; Nathanson, L.A. Creating an automated trigger for sepsis clinical decision support at emergency department triage using machine learning. PLoS ONE 2017, 12, e0174708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gligorijevic, D.; Gligorijevic, J.; Satz, W.; Stojkovic, I.; Schreyer, K.; Del Portal, D.; Obradovic, Z. Deep Attention Model for Triage of Emergency Department Patients. In Proceedings of the 2018 SIAM International Conference on Data Mining, San Diego, CA, USA, 3–5 May 2018; Volume 1, pp. 297–305. [Google Scholar]
- Vu, T.; Nguyen, A.; Brown, N.; Hughes, J. Identifying patients with pain in emergency departments using conventional machine learning and deep learning. In Proceedings of the 17th Annual Workshop of the Australasian Language Technology Association, Sydney, NSW, Australia, 4–6 December 2019; Volume 1, pp. 111–119. [Google Scholar]
- National Centre for Classification in Health. The International Statistical Classification of Diseases and Related Health Problems; 10th Revision, Australian Modification (ICD-10-AM); University of Sydney: Sydney, NSW, Australia, 1998.
- Spittal, M.J.; Pirkis, J.; Miller, M.; Studdert, D.M. Declines in the Lethality of Suicide Attempts Explain the Decline in Suicide Deaths in Australia. PLoS ONE 2012, 7, e44565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guidelines for ATC Classification and DDD Assignment; World Health Organization: Oslo, Norway, 2019. [Google Scholar]
- Department of Health. Poisons Standard July 2020; Department of Health: Canberra, ACT, Australia, 2020.
- Bridge, J.A.; Greenhouse, J.B.; Ruch, D.; Stevens, J.; Ackerman, J.; Sheftall, A.H.; Horowitz, L.M.; Kelleher, K.J.; Campo, J.V. Association Between the Release of Netflix’s 13 Reasons Why and Suicide Rates in the United States: An Interrupted Time Series Analysis. J. Am. Acad. Child. Adolesc. Psychiatry 2020, 59, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Cooper, T.; Bard, D.; Wallace, R.; Gillaspy, S.; DeLeon, S. Suicide Attempt Admissions From a Single Children’s Hospital Before and After the Introduction of Netflix Series 13 Reasons Why. J. Adolesc. Health 2018, 63, 688–693. [Google Scholar] [CrossRef]
- Hawton, K.; Simkin, S.; Deeks, J. Co-proxamol and suicide: A study of national mortality statistics and local non-fatal self poisonings. BMJ 2003, 326, 1006–1008. [Google Scholar] [CrossRef] [Green Version]
- Hawton, K.; Bergen, H.; Simkin, S.; Arensman, E.; Corcoran, P.; Cooper, J.; Waters, K.; Gunnell, D.; Kapur, N. Impact of different pack sizes of paracetamol in the United Kingdom and Ireland on intentional overdoses: A comparative study. BMC Public Health 2011, 11, 460. [Google Scholar] [CrossRef]
- Hawton, K.; Bergen, H.; Waters, K.; Murphy, E.; Cooper, J.; Kapur, N. Impact of Withdrawal of the Analgesic Co-proxamol on Nonfatal Self-Poisoning in the UK. Crisis 2011, 32, 81–87. [Google Scholar] [CrossRef]
- State of Victoria. Victorian Suicide Prevention Framework 2016–25; State of Victoria: Melbourne, VIC, Australia, 2016.
- Borschmann, R.; Young, J.T.; Moran, P.; Spittal, M.J.; Snow, K.; Mok, K.; Kinner, S.A. Accuracy and predictive value of incarcerated adults’ accounts of their self-harm histories: Findings froman Australian prospective data linkage study. CMAJ Open 2017, 5, E694–E701. [Google Scholar] [CrossRef] [Green Version]
- Boyd, J.H.; Ferrante, A.; O’Keefe, C.M.; Bass, A.J.; Randall, S.M.; Semmens, J.B. Data linkage infrastructure for cross-jurisdictional health-related research in Australia. BMC Health Serv. Res. 2012, 12, 480. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, R.; Cameron, C.M.; McClure, R.; Williamson, A.M. Data linkage capabilities in Australia: Practical issues identified by a Population Health Research Network ‘Proof of Concept project’. Aust. N. Z. J. Public Health 2015, 39, 319–325. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, J.; Witt, K.; Lamblin, M.; Spittal, M.J.; Carter, G.; Verspoor, K.; Page, A.; Rajaram, G.; Rozova, V.; Hill, N.T.M.; et al. Development of a Self-Harm Monitoring System for Victoria. Int. J. Environ. Res. Public Health 2020, 17, 9385. https://doi.org/10.3390/ijerph17249385
Robinson J, Witt K, Lamblin M, Spittal MJ, Carter G, Verspoor K, Page A, Rajaram G, Rozova V, Hill NTM, et al. Development of a Self-Harm Monitoring System for Victoria. International Journal of Environmental Research and Public Health. 2020; 17(24):9385. https://doi.org/10.3390/ijerph17249385
Chicago/Turabian StyleRobinson, Jo, Katrina Witt, Michelle Lamblin, Matthew J. Spittal, Greg Carter, Karin Verspoor, Andrew Page, Gowri Rajaram, Vlada Rozova, Nicole T. M. Hill, and et al. 2020. "Development of a Self-Harm Monitoring System for Victoria" International Journal of Environmental Research and Public Health 17, no. 24: 9385. https://doi.org/10.3390/ijerph17249385