Views of the Future of Partners of People with Multiple Sclerosis Who Attended a Lifestyle Modification Workshop: A Qualitative Analysis of Perspectives and Experiences

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. The Residential Lifestyle Modification Workshop (RLMW)
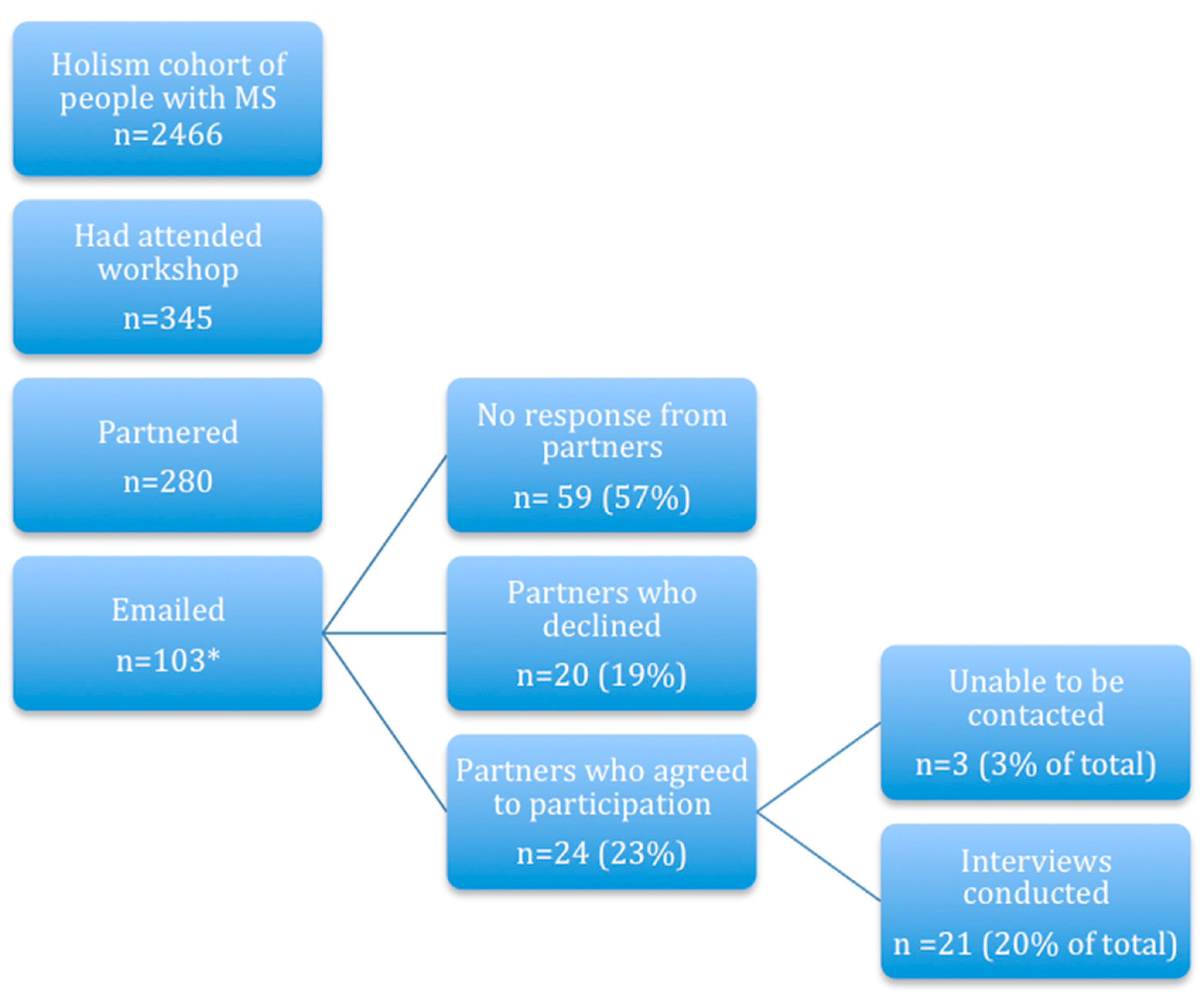
2.3. Participant Recruitment
2.4. The Interviewers
2.5. The Interview
2.6. Analysis
2.7. Rigour
2.8. Ethics Approval
3. Results
3.1. Characteristics of the Person with MS and Their Partners (Participants)
3.2. Themes
3.2.1. Uncertainty
It’s about the unknown…how we might manage if he does reach a point where he is not able to walk. I’m hoping I just don’t die. (P3, F)
It’s still a demon that’s in your life. (P21, M)
It’s so unpredictable. I need to stop trying to predict what’s going to happen (P7, F)
But then every now and again you’ll hit a small bump that brings you back to the reality of…living with MS every day. (P21, M)
So we are more concerned about just (adopting) a day by day, month by month kind of approach to life. (P9, M)
To be honest, I have not thought about [partner] being incapacitated in any way. I don’t know if that, or when that, might happen, but it’s something that we would handle when it does happen. (P11, M)
3.2.2. Planning for the Future
We sort of have the MS thing. It’s part of the decision…Yeah, the fourth person in the family. (P5, M)
We’ve made changes in our lives...Even in terms of how we spend money, we’re more frugal I guess because there is a possibility that in 15 years time…(P5, M)
It’s definitely changed our plans…One of the things is that we planned on having children much later on life…we ended up having [child] much earlier. (P7, F)
In fact, I used it as a reason—I retired about a year (earlier)...and we took quite a few overseas trips (P12, M)
We’re not going to live life waiting. If we really want to do it we’re not going to wait until we’re retired to do it. We’ll do it now...so there’s a bit more urgency I guess, which isn’t a bad thing. (P5, M)
She would never have travelled to Central America and backpacked pre-MS. It’s almost like we’re saying MS isn’t holding us back in any way. (P5, M)
3.2.3. Control, Empowerment and Confidence
I think the future is looking very good. Interviewer: So those initial fears and uncertainties are they still lurking there somewhere? P9: I think they’ve gone. (P9, M)
That’s what I love the most about OMS and that’s what really appeals to me more than anything else, was the fact that you were in control. (P7, F.)
MS certainly isn’t stopping us from planning for the future...We’re so far at the opposite end of that spectrum. (P21, M)
I remember saying when we bought this house. We would never have gone and done all of that (taken a mortgage) if we weren’t confident in paying it off. (P1, F)
Really completely positive. I guess I feel how I felt when we got married before we found out about MS, what I thought our lives were going to be like, like that is just how I see our lives now and better in a way than how I would have felt then. (P20, F)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Semi-Structured Interview Guide
- (1)
- How has MS and any lifestyle modification that you/your partner have undertaken affected your life?
- (a)
- Has there been little change or significant change?
- (b)
- Have there been positive changes?
- (c)
- Have there been negative changes?
- (d)
- What have been the easiest changes and what have been the hardest?
- (e)
- What barriers have you identified to implementing lifestyle change?
- (f)
- Have other health care professionals (e.g., GP or neurologist) supported any changes you have made/tried to make?
- (g)
- What other resources have you found useful?
- (h)
- Do you have any tips/advice for others?
- (2)
- How has MS and any lifestyle modification that you/your partner have undertaken affected your relationship with the person with MS?
- (a)
- Have there been positives for your relationship due the diagnosis of MS or the changes you have made?
- (b)
- Have there been difficulties in your relationship due the diagnosis of MS or the changes you have made?
- (c)
- What strategies have you found helpful in managing the issues you have described?
- (d)
- How have you dealt with any changes to the relationship?
- (3)
- How do you see your future and what has influenced this view?
- (a)
- Your life plans/children/career
- (b)
- Your health
- (c)
- Your relationship
- (d)
- Do you feel in control of your future?
References
- Alschuler, K.N.; Beier, M.L. Intolerance of Uncertainty: Shaping an Agenda for Research on Coping with Multiple Sclerosis. Int. J. MS Care 2015, 17, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, H.R.; das Nair, R. The psychological impact of the unpredictability of multiple sclerosis: A qualitative literature meta-synthesis. Br. J. Neurosci. Nurs. 2013, 9, 172–178. [Google Scholar] [CrossRef]
- Uccelli, M.M. The impact of multiple sclerosis on family members: A review of the literature. Neurodegener Dis. Manag. 2014, 4, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Davies, F.; Edwards, A.; Brain, K.; Edwards, M.; Jones, R.; Wallbank, R.; Robertson, N.P.; Wood, F. You are just left to get on with it: Qualitative study of patient and carer experiences of the transition to secondary progressive multiple sclerosis. BMJ Open 2015, 5, e007674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killner, L.; Soundy, A. Motivation and experiences of role transition in spousal caregivers of people with multiple sclerosis. Int. J. Ther. Rehabil. 2018, 25, 405–413. [Google Scholar] [CrossRef] [Green Version]
- Cheung, J.; Hocking, P. Caring as worrying: The experience of spousal carers. J. Adv. Nurs. 2004, 47, 475–482. [Google Scholar] [CrossRef]
- Rollero, C. The Experience of Men Caring for a Partner With Multiple Sclerosis. J. Nurs. Sch. 2016, 48, 482–489. [Google Scholar] [CrossRef] [Green Version]
- Appleton, D.; Robertson, N.; Mitchell, L.; Lesley, R. Our disease: A qualitative meta-synthesis of the experiences of spousal/partner caregivers of people with multiple sclerosis. Scand J. Caring Sci. 2018, 32, 1262–1278. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Tyry, T.; Salter, A.; Cofield, S.S.; Cutter, G.; Fox, R.; Marrie, R.A. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology 2018, 90, e1–e11. [Google Scholar] [CrossRef]
- Hempel, S.; Graham, G.D.; Fu, N.; Estrada, E.; Chen, A.Y.; Miake-Lye, I.; Miles, J.N.; Shanman, R.; Shekelle, P.G.; Beroes, J.M.; et al. A systematic review of modifiable risk factors in the progression of multiple sclerosis. Mult. Scler. 2017. [Google Scholar] [CrossRef]
- Marck, C.H.; Hadgkiss, E.; Weiland, T.J.; van der Meer, D.M.; Pereira, N.; Jelinek, G.A. Physical activity and associated levels of disability and quality of life in people with multiple sclerosis: A large international survey. BMC Neurol. 2014, 14, 143. [Google Scholar] [CrossRef] [PubMed]
- Weiland, T.J.; Jelinek, G.A.; Marck, C.H.; Hadgkiss, E.J.; van der Meer, D.M.; Pereira, N.G.; Taylor, K.L. Clinically significant fatigue: Prevalence and associated factors in an international sample of adults with multiple sclerosis recruited via the internet. PLoS ONE 2015, 10, e0115541. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.L.; Hadgkiss, E.J.; Jelinek, G.A.; Weiland, T.J.; Pereira, N.G.; Marck, C.H.; van der Meer, D.M. Lifestyle factors, demographics and medications associated with depression risk in an international sample of people with multiple sclerosis. BMC Psychiatry 2014, 14, 327. [Google Scholar] [CrossRef] [PubMed]
- D’Hooghe, M.B.; Nagels, G.; Bissay, V.; De Keyser, J. Modifiable factors influencing relapses and disability in multiple sclerosis. Mult. Scler. 2010, 16, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Jelinek, G.A.; De Livera, A.M.; Marck, C.H.; Brown, C.R.; Neate, S.L.; Taylor, K.L.; Weiland, T.J. Associations of Lifestyle, Medication, and Socio-Demographic Factors with Disability in People with Multiple Sclerosis: An International Cross-Sectional Study. PLoS ONE 2016, 11, e0161701. [Google Scholar] [CrossRef] [PubMed]
- Marck, C.H.; De Livera, A.M.; Brown, C.R.; Neate, S.L.; Taylor, K.L.; Weiland, T.J.; Hadgkiss, E.J.; Jelinek, G.A. Health outcomes and adherence to a healthy lifestyle after a multimodal intervention in people with multiple sclerosis: Three year follow-up. PLoS ONE 2018, 13, e0197759. [Google Scholar] [CrossRef] [Green Version]
- Hadgkiss, E.J.; Jelinek, G.A.; Weiland, T.J.; Rumbold, G.; Mackinlay, C.A.; Gutbrod, S.; Gawler, I. Health-related quality of life outcomes at 1 and 5 years after a residential retreat promoting lifestyle modification for people with multiple sclerosis. Neurol. Sci. 2013, 34, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Li, M.P.; Jelinek, G.A.; Weiland, T.J.; Mackinlay, C.A.; Dye, S.; Gawler, I. Effect of a residential retreat promoting lifestyle modifications on health-related quality of life in people with multiple sclerosis. Qual. Prim. Care 2010, 18, 379–389. [Google Scholar]
- Neate, S.L.; Taylor, K.L.; Jelinek, G.A.; De Livera, A.M.; Brown, C.R.; Weiland, T.J. Psychological Shift in Partners of People with Multiple Sclerosis Who Undertake Lifestyle Modification: An Interpretive Phenomenological Study. Front. Psychol. 2018, 9, 15. [Google Scholar] [CrossRef] [Green Version]
- Neate, S.L.; Taylor, K.L.; Jelinek, G.A.; De Livera, A.M.; Brown, C.R.; Weiland, T.J. Taking active steps: Changes made by partners of people with multiple sclerosis who undertake lifestyle modification. PLoS ONE 2019, 14, e0212422. [Google Scholar] [CrossRef]
- Neate, S.L.; Taylor, K.L.; Jelinek, G.A.; De Livera, A.M.; Simpson, S., Jr.; Bevens, W.; Weiland, T.J. On the path together: Experiences of partners of people with multiple sclerosis of the impact of lifestyle modification on their relationship. Health Soc. Care Community 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crist, J.D.; Tanner, C.A. Interpretation/analysis methods in hermeneutic interpretive phenomenology. Nurs. Res. 2003, 52, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Hadgkiss, E.J.; Jelinek, G.A.; Weiland, T.J.; Pereira, N.G.; Marck, C.H.; van der Meer, D.M. Methodology of an International Study of People with Multiple Sclerosis Recruited through Web 2.0 Platforms: Demographics, Lifestyle, and Disease Characteristics. Neurol. Res. Int. 2013, 2013, 580596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef] [PubMed]
- McConnell-Henry, T.; Chapman, Y.; Francis, K. Member checking and Heideggerian phenomenology: A redundant component. Nurse Res. 2011, 18, 28–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, C.T. Qualitative Research: The Evaluation of Its Credibility, Fittingness, and Auditability. West. J. Nurs. Res. 1993, 15, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Sandelowski, M. The problem of rigor in qualitative research. Adv. Nurs. Sci. 1986, 8, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Clancy, M. Is reflexivity the key to minimising problems of interpretation in phenomenological research? Nurse Res. 2013, 20, 12–16. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelinek, G.A. Overcoming Multiple Sclerosis, The Evidence-Based 7 Step Recovery Program, 2nd ed.; Allen and Unwin: Melbourne, Australia, 2016. [Google Scholar]
- Ackroyd, K.; Fortune, D.G.; Price, S.; Howell, S.; Sharrack, B.; Isaac, C.L. Adversarial growth in patients with multiple sclerosis and their partners: Relationships with illness perceptions, disability and distress. J. Clin. Psychol. Med. Settings 2011, 18, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I. The positive impact of multiple sclerosis (MS) on carers: Associations between carer benefit finding and positive and negative adjustment domains. Disabil. Rehabil. 2005, 27, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Strickland, K.; Worth, A.; Kennedy, C. The experiences of support persons of people newly diagnosed with multiple sclerosis: An interpretative phenomenological study. J. Adv. Nurs. 2015, 71, 2811–2821. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I. Benefit finding in multiple sclerosis and associations with positive and negative outcomes. Health Psychol. 2005, 24, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Schooler, C. The structure of coping. J. Health Soc. Behav. 1978, 19, 2–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| People with MS | Partners | |||||||
|---|---|---|---|---|---|---|---|---|
| * Type of MS | Years since Diagnosis | Years since Workshop | ^ Disability | Sex | Age | Workshop Attendance with Person with MS | Employment | Years of Relationship with Person with MS |
| RRMS | 5–10 | >5 | No | Female | 30–39 | Yes | Full time | 11–20 |
| PPMS | 5–10 | 2–5 | No | Male | 20–29 | Yes | Full time | 1–10 |
| Unsure | 0–5 | 1–2 | No | Female | 40–49 | No | Full time | 21–30 |
| RRMS | 0–5 | 1–2 | No | Female | 50–59 | Yes | Part time | 21–30 |
| RRMS | 11–20 | >5 | No | Male | 40–49 | Yes | Part time | 1–10 |
| SPMS | 11–20 | >5 | Yes | Female | 70–79 | Yes | Retired | >50 |
| SPMS | 11–20 | >5 | Yes | Female | 60–69 | No | Retired | 41–50 |
| Unsure | 5–10 | 2–5 | No | Female | 40–49 | Yes | Full time | 1–10 |
| SPMS | 0–5 | 2–5 | No | Female | 20–29 | Yes | Part time | 1–10 |
| Unsure | 5–10 | >5 | No | Female | 60–69 | No | Full time | 21–30 |
| PPMS | 11–20 | >5 | Yes | Male | 60–69 | Yes | Full time | 41–50 |
| CIS | 0–5 | 2–5 | No | Female | 60–69 | Yes | Retired | 31–40 |
| RRMS | 5–10 | >5 | No | Male | 40–49 | No | Full time | 1–10 |
| Unsure | 5–10 | 1–2 | No | Female | 30–39 | No | Full time | 1–10 |
| Unsure | 11–20 | >5 | No | Female | 60–69 | No | Retired | 41–50 |
| Unsure | 0–5 | 1–2 | No | Female | 50–59 | No | Unable | 31–40 |
| RRMS | 0–5 | 1–2 | No | Male | 20–29 | No | On leave | 1–10 |
| PPMS | 5–10 | 2–5 | Yes | Male | 50–59 | No | Full time | 11–20 |
| RRMS | >40 | 2–5 | No | Male | 60–69 | Yes | Retired | 41–50 |
| RRMS | 5–10 | 2–5 | Yes | Male | 60–69 | No | Full time | 11–20 |
| Unsure | 11–20 | >5 | Yes | Male | 70–79 | Yes | Retired | 21–30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neate, S.L.; Taylor, K.L.; Nag, N.; Jelinek, G.A.; Simpson-Yap, S.; Bevens, W.; Weiland, T.J. Views of the Future of Partners of People with Multiple Sclerosis Who Attended a Lifestyle Modification Workshop: A Qualitative Analysis of Perspectives and Experiences. Int. J. Environ. Res. Public Health 2021, 18, 85. https://doi.org/10.3390/ijerph18010085
Neate SL, Taylor KL, Nag N, Jelinek GA, Simpson-Yap S, Bevens W, Weiland TJ. Views of the Future of Partners of People with Multiple Sclerosis Who Attended a Lifestyle Modification Workshop: A Qualitative Analysis of Perspectives and Experiences. International Journal of Environmental Research and Public Health. 2021; 18(1):85. https://doi.org/10.3390/ijerph18010085
Chicago/Turabian StyleNeate, Sandra L., Keryn L. Taylor, Nupur Nag, George A. Jelinek, Steve Simpson-Yap, William Bevens, and Tracey J. Weiland. 2021. "Views of the Future of Partners of People with Multiple Sclerosis Who Attended a Lifestyle Modification Workshop: A Qualitative Analysis of Perspectives and Experiences" International Journal of Environmental Research and Public Health 18, no. 1: 85. https://doi.org/10.3390/ijerph18010085