Translation, Reliability and Validity of the Spanish Version of the Modified New Mobility Score (NMS-ES)

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. New Mobility Score
2.2. Translation of the NMS-ES
2.3. Reliability
2.4. Statistical Analysis
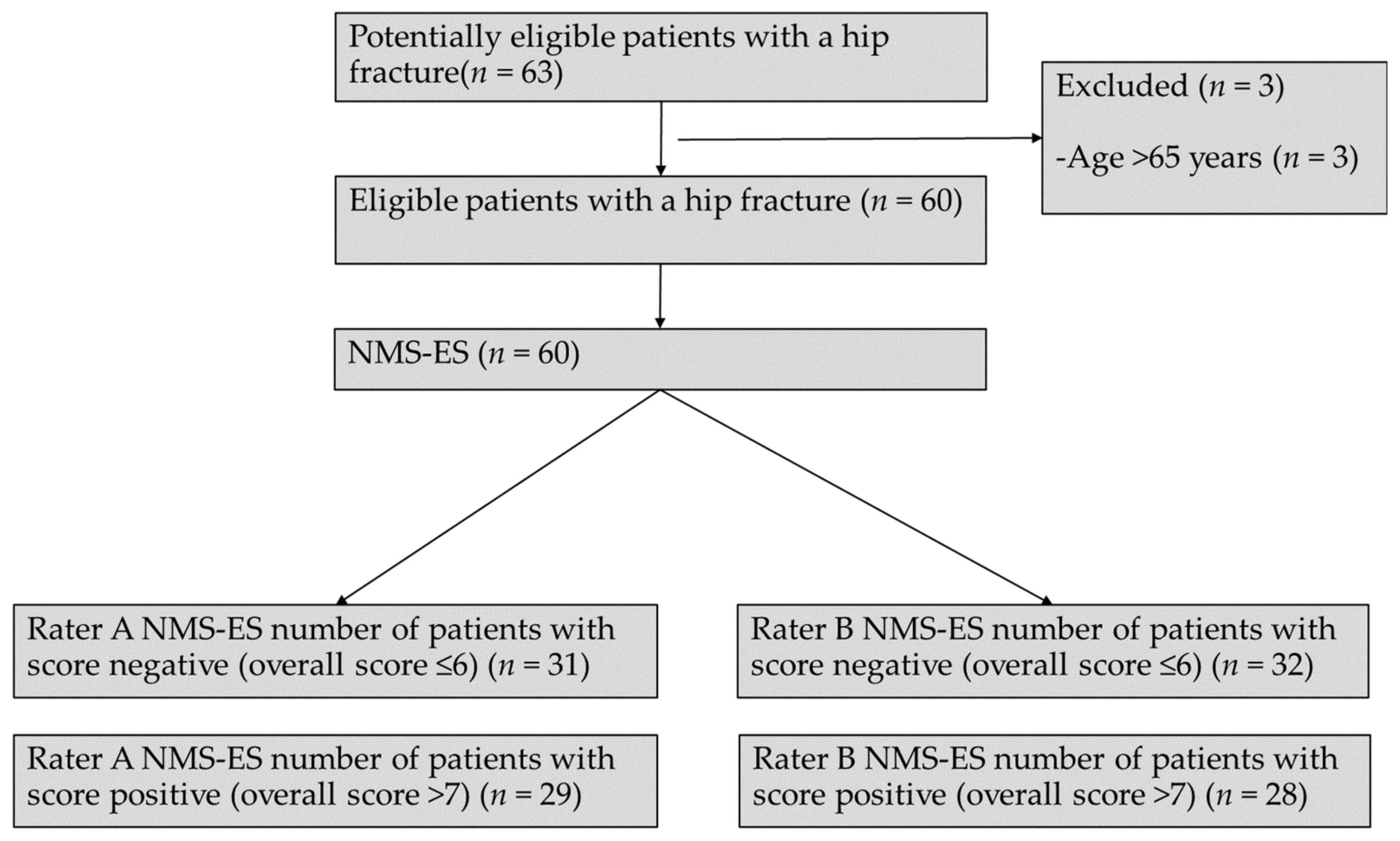
3. Results
3.1. Translating the NMS-ES
3.2. Reliability and Validity of the NMS-ES
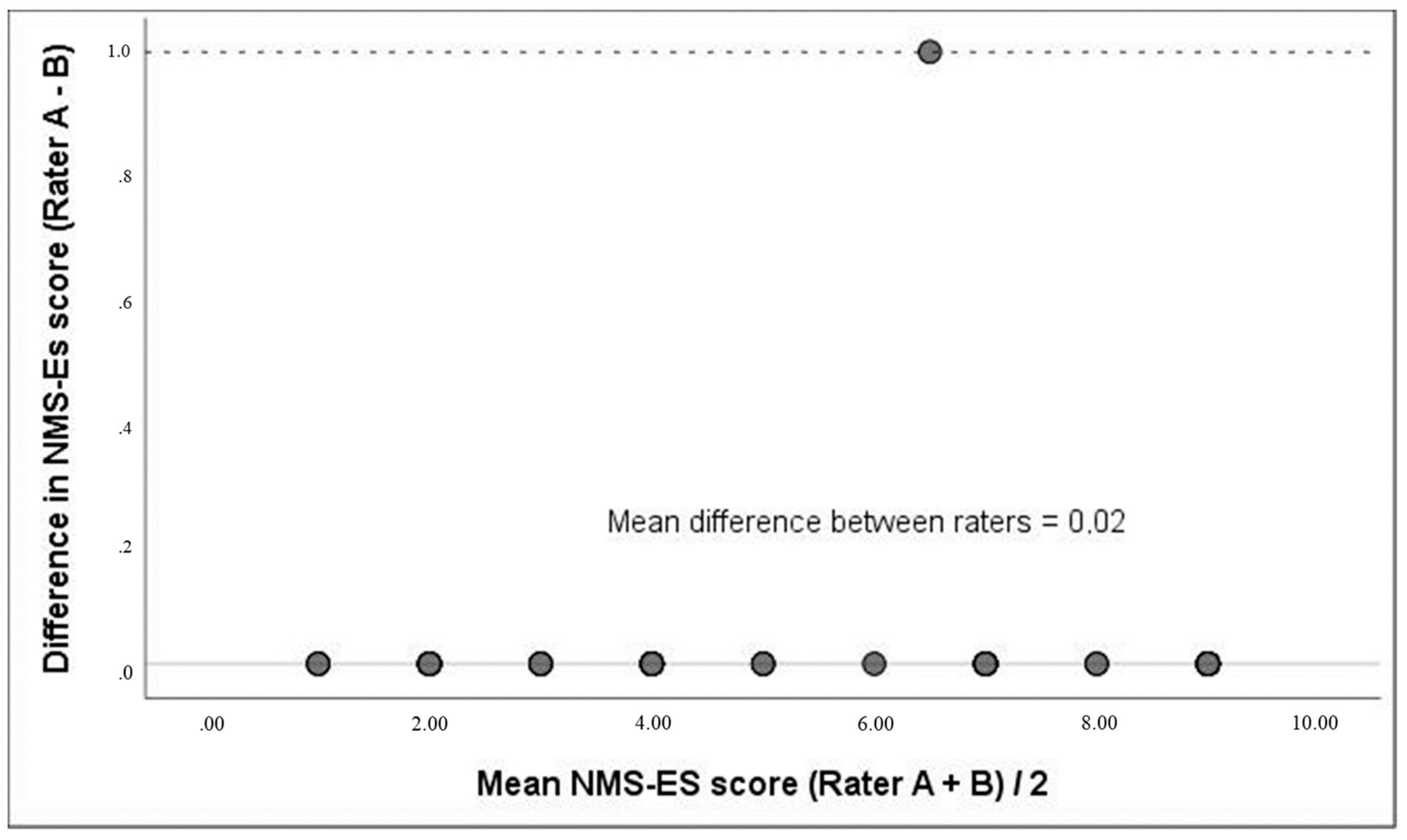
3.3. Reliability
3.4. Validity
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Spanish Version of the Modified New Mobility Score (NMS-ES)

{kind=link}
{kind=link}
| Nuevo Test de Movilidad (NMS-ES, 0–9 Puntos) | ||||
|---|---|---|---|---|
| Movilidad | Sin dificultad Y sin ningún dispositivo de apoyo | Con un dispositivo de apoyo para caminar | Con ayuda de otra persona | De ningún modo |
| Capaz de moverse por la casa (Caminar dentro) | 3 | 2 | 1 | 0 |
| Capaz de salir de la casa (Caminar fuera) | 3 | 2 | 1 | 0 |
| Capaz de ir de compras (Caminar cuando va de compras) | 3 | 2 | 1 | 0 |
References
- Dyer, S.M.; Crotty, M.; Fairhall, N.; Magaziner, J.; Beaupre, L.A.; Cameron, I.D.; Sherrington, C. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, M.-Y.; Shyu, Y.-I.L.; Liang, J. Functional Recovery of Older Hip-Fracture Patients After Interdisciplinary Intervention Follows Three Distinct Trajectories. Gerontologist 2012, 52, 833–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Zabaleta, J.; Pita-Fernandez, S.; Seoane-Pillado, T.; López-Calviño, B.; Gonzalez-Zabaleta, J.L. Comorbidity as a predictor of mortality and mobility after hip fracture: Mortality and mobility after hip fracture. Geriatr. Gerontol. Int. 2016, 16, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.T.; Foss, N.B.; Ekdahl, C.; Kehlet, H. Prefracture functional level evaluated by the New Mobility Score predicts in-hospital outcome after hip fracture surgery. Acta Orthop. 2010, 81, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Klestil, T.; Röder, C.; Stotter, C.; Winkler, B.; Nehrer, S.; Lutz, M.; Klerings, I.; Wagner, G.; Gartlehner, G.; Nussbaumer-Streit, B. Impact of timing of surgery in elderly hip fracture patients: A systematic review and meta-analysis. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Morri, M.; Forni, C.; Marchioni, M.; Bonetti, E.; Marseglia, F.; Cotti, A. Which factors are independent predictors of early recovery of mobility in the older adults’ population after hip fracture? A cohort prognostic study. Arch. Orthop. Trauma Surg. 2018, 138, 35–41. [Google Scholar] [CrossRef]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The reliability of the functional independence measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef]
- Katz, S. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914. [Google Scholar] [CrossRef]
- Parker, M.; Palmer, C. A new mobility score for predicting mortality after hip fracture. J. Bone Joint Surg. Br. 1993, 75, 797–798. [Google Scholar] [CrossRef]
- Martínez-Martín, P.; Fernández-Mayoralas, G.; Frades-Payo, B.; Rojo-Pérez, F.; Petidier, R.; Rodríguez-Rodríguez, V.; Forjaz, M.J.; Prieto-Flores, M.E.; de Pedro Cuesta, J. Validación de la Escala de Independencia Funcional. [Validity of Functional Independence Measure]. Gac. Sanit. 2009, 23, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cid-Ruzafa, J.; Damián-Moreno, J. Disability evaluation: Barthel’s index. Rev. Esp. Salud Publica 1997, 71, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Solar, M.; de Alaiz Rojo, A.T.; Brun Gurpegui, E.; Cabañeros Vicente, J.J.; Calzón Frechoso, M.; Cosío Rodríguez, I.; García López, P.; García-Cañedo Fernández, R.; Pardo González, I.; Suárez-González, A. Functional capacity of patients over 65 according to the Katz index. Reliability of the method. Aten. Primaria 1992, 10, 812–816. [Google Scholar] [PubMed]
- Suárez, S. Incidencia y pronósticos general y funcional de fracturas de cadera en población anciana. [Incidence and general and functional forecasts of hip fracture in elderly]. Canar. Médica Quirúrgica 2012, 9, 4. [Google Scholar]
- Kristensen, M.T.; Kehlet, H. Most patients regain prefracture basic mobility after hip fracture surgery in a fast-track programme. Dan Med. J. 2012, 59, A4447. [Google Scholar]
- Kristensen, M.T.; Kehlet, H. The basic mobility status upon acute hospital discharge is an independent risk factor for mortality up to 5 years after hip fracture surgery: Survival rates of 444 pre-fracture ambulatory patients evaluated with the Cumulated Ambulation Score. Acta Orthop. 2018, 89, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, M.; Blake, C.; Askin, D.; Quinlan, J.; Coughlan, T.; Cunningham, C. Mobility one week after a hip fracture—Can it be predicted? Int. J. Orthop. Trauma Nurs. 2018, 29, 3–9. [Google Scholar] [CrossRef]
- Kristensen, M.; Bandholm, T.; Foss, N.; Ekdahl, C.; Kehlet, H. High inter-tester reliability of the new mobility score in patients with hip fracture. J. Rehabil. Med. 2008, 40, 589–591. [Google Scholar] [CrossRef] [Green Version]
- Ariza-Vega, P.; Lozano-Lozano, M.; Olmedo-Requena, R.; Martín-Martín, L.; Jiménez-Moleón, J.J. Influence of Cognitive Impairment on Mobility Recovery of Patients with Hip Fracture. Am. J. Phys. Med. Rehabil. 2017, 96, 109–115. [Google Scholar] [CrossRef]
- Asplin, G.; Carlsson, G.; Zidén, L.; Kjellby-Wendt, G. Early coordinated rehabilitation in acute phase after hip fracture—A model for increased patient participation. BMC Geriatr. 2017, 17. [Google Scholar] [CrossRef] [Green Version]
- Maranesi, E.; Riccardi, G.R.; Lattanzio, F.; Di Rosa, M.; Luzi, R.; Casoni, E.; Rinaldi, N.; Baldoni, R.; Di Donna, V.; Bevilacqua, R. Randomised controlled trial assessing the effect of a technology-assisted gait and balance training on mobility in older people after hip fracture: Study protocol. BMJ Open 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Schnell, S.; Friedman, S.M.; Mendelson, D.A.; Bingham, K.W.; Kates, S.L. The 1-Year Mortality of Patients Treated in a Hip Fracture Program for Elders. Geriatr. Orthop. Surg. Rehabil. 2010, 1, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Office of Clinical Audit. Irish Hip Fracture Database National Report 2017; National Office of Clinical Audit: Dublin, Germany, 2018. [Google Scholar]
- Azagra, R.; López-Expósito, F.; Martin-Sánchez, J.C.; Aguyé-Batista, A.; Gabriel-Escoda, P.; Zwart, M.; Díaz-Herrera, M.A.; Pujol-Salud, J.; Iglesias Martínez, M.; Puchol-Ruiz, N. Incidence of hip fracture in Spain (1997–2010). Med. Clín. 2015, 145, 465–470. [Google Scholar] [CrossRef]
- Ramada-Rodilla, J.M.; Serra-Pujadas, C.; Delclós-Clanchet, G.L. Cross-cultural adaptation and health questionnaires validation: Revision and methodological recommendations. Salud Publica Mex. 2013, 55, 57–66. [Google Scholar] [CrossRef]
- Kristensen, M.T.; Nielsen, A.Ø.; Topp, U.M.; Holmehave-Brandt, J.; Petterson, C.F.; Gebuhr, P. Development and psychometric properties of the Basic Amputee Mobility Score for use in patients with a major lower extremity amputation: Basic Amputee Mobility Score. Geriatr. Gerontol. Int. 2018, 18, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Martínez De La Iglesia, J.; Herrero, R.D.; Vilches, M.C.O.; Taberné, C.A.; Colomer, C.A.; Luque, R.L. Cross-cultural adaptation and validation of Pfeiffer’s test (Short Portable Mental Status Questionnaire [SPMSQ]) to screen cognitive impairment in general population aged 65 or older. Med. Clin. 2001, 117, 129–134. [Google Scholar] [CrossRef]
- Pfeiffer, E. A Short Portable Mental Status Questionnaire for the Assessment of Organic Brain Deficit in Elderly Patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Ariza-Vega, P.; Mora-Traverso, M.; Ortiz-Piña, M.; Ashe, M.C.; Kristensen, M.T. Translation, inter-rater reliability, agreement, and internal consistency of the Spanish version of the cumulated ambulation score in patients after hip fracture. Disabil. Rehabil. 2019, 1–6. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory; McGraw Hill: New York, NY, USA, 1978. [Google Scholar]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sport. Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Gliem, J.A.; Gliem, R.R. Calculating, Interpreting, and Reporting Cronbach’s Alpha Reliability Coefficient for Likert-Type Scales. In Proceedings of the Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education, Columbus, OH, USA, 8–10 October 2003. [Google Scholar]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. Stat 1983, 32, 307. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Medica 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondragón Barrera, M.A. Uso de la correlacion de Spearman en un estudio de intervención en fisioterapia. [Use of the correlation Spearman in a study of intervention in physiotherapy]. Mov. Científico 2014, 8, 98. [Google Scholar] [CrossRef]
- Sheehan, K.J.; Fitzgerald, L.; Hatherley, S.; Potter, C.; Ayis, S.; Martin, F.C.; Gregson, C.L.; Cameron, I.D.; Beaupre, L.A.; Wyatt, D.; et al. Inequity in rehabilitation interventions after hip fracture: A systematic review. Age Ageing 2019, 48, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulsbæk, S.; Larsen, R.F.; Troelsen, A. Predictors of not regaining basic mobility after hip fracture surgery. Disabil. Rehabil. 2015, 37, 1739–1744. [Google Scholar] [CrossRef]
- Ranhoff, A.H.; Holvik, K.; Martinsen, M.I.; Domaas, K.; Solheim, L.F. Older hip fracture patients: Three groups with different needs. BMC Geriatr. 2010, 10. [Google Scholar] [CrossRef] [Green Version]
- Bodilsen, A.C.; Pedersen, M.M.; Petersen, J.; Beyer, N.; Andersen, O.; Smith, L.L.; Kehlet, H.; Bandholm, T. Acute hospitalization of the older patient: Changes in muscle strength and functional performance during hospitalization and 30 days after discharge. Am. J. Phys. Med. Rehabil. 2013, 92, 789–796. [Google Scholar] [CrossRef]
- Overgaard, J.; Kristensen, M.T. Feasibility of progressive strength training shortly after hip fracture surgery. World J. Orthop. 2013, 4, 248–258. [Google Scholar] [CrossRef] [Green Version]
- Steihaug, O.M.; Gjesdal, C.G.; Bogen, B.; Kristoffersen, M.H.; Lien, G.; Hufthammer, K.O.; Ranhoff, A.H. Does sarcopenia predict change in mobility after hip fracture? A multicenter observational study with one-year follow-up. BMC Geriatr. 2018, 18, 65. [Google Scholar] [CrossRef]


| Variable | N = 60 |
|---|---|
| Age, years: Mean (standard deviation), minimum–maximum | 81.7 (6.8), 65–96 |
| Gender n (%) | |
| Women | 46(77) |
| Men | 14 (23) |
| Body Mass Index kg/ m2 Classification n (%) | |
| Underweight (<18.5) | 1 (2) |
| Normal (18.5–24.9) | 18 (30) |
| Overweight (≥25) | 41 (68) |
| Educational level n (%) | |
| Cannot read and write | 16 (27) |
| Can read and write | 25 (42) |
| Primary school | 13 (22) |
| High school | 3 (5) |
| College (University) | 3 (5) |
| Pre-fracture Functional Independence Measure: median (IQR) | 100.5 (79–123.8) |
| Cognitive Status (SPMSQ test, 0–11 points) n (%) | |
| No cognitive impairment (0–3 points) | 27 (45) |
| Mild cognitive impairment (3–4 points) | 15 (25) |
| Moderated cognitive impairment (5–7 points) | 9 (15) |
| Severe cognitive impairment (8–11 points) | 9 (15) |
| Type of fracture n (%) | |
| Cervical Femoral (Intracapsular) | 40 (67) |
| Trochanteric (Extracapsular) | 20 (33) |
| Type of surgery n (%) | |
| Prosthesis | 28 (47) |
| Intramedullary hip screw | 32 (53) |
| Falls in the previous year n (%) | |
| Yes | 18 (30) |
| No | 42 (70) |
| Pre-fracture residence n (%) | |
| Own home | 45 (75) |
| Nursing or relative´s home | 15 (25) |
| Change of residence at hospital discharge n (%) | |
| Yes | 17 (28) |
| No | 43 (72) |
| Support at hospital discharge n (%) | |
| Formal caregiver | 14 (23) |
| Informal caregiver (relative or friend) | 46 (77) |
| Post-surgery Cumulated Ambulation Score assessed during the first week (between day 2 and 6 from surgery): median (IQR) | 3 (2–5) |
| Item | α Coefficient if Item Deleted |
|---|---|
| Indoor walking | 0.92 |
| Outdoor walking | 0.79 |
| Walking during shopping | 0.84 |
| Total | 0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prieto-Moreno, R.; Ariza-Vega, P.; Ortiz-Piña, M.; Ashe, M.C.; Romero-Ayuso, D.; Kristensen, M.T. Translation, Reliability and Validity of the Spanish Version of the Modified New Mobility Score (NMS-ES). Int. J. Environ. Res. Public Health 2021, 18, 723. https://doi.org/10.3390/ijerph18020723
Prieto-Moreno R, Ariza-Vega P, Ortiz-Piña M, Ashe MC, Romero-Ayuso D, Kristensen MT. Translation, Reliability and Validity of the Spanish Version of the Modified New Mobility Score (NMS-ES). International Journal of Environmental Research and Public Health. 2021; 18(2):723. https://doi.org/10.3390/ijerph18020723
Chicago/Turabian StylePrieto-Moreno, Rafael, Patrocinio Ariza-Vega, Mariana Ortiz-Piña, Maureen C. Ashe, Dulce Romero-Ayuso, and Morten Tange Kristensen. 2021. "Translation, Reliability and Validity of the Spanish Version of the Modified New Mobility Score (NMS-ES)" International Journal of Environmental Research and Public Health 18, no. 2: 723. https://doi.org/10.3390/ijerph18020723