
Definitions and Operationalization of Mental Health Problems, Wellbeing and Participation Constructs in Children with NDD: Distinctions and Clarifications

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Issues of Classification of Mental Disorders and NDD in Diagnostic Manuals
“Mental, behavioral and neurodevelopmental disorders are syndromes characterized by clinically significant disturbance in an individual’s cognition, emotional regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes that underlie mental and behavioral functioning. These disturbances are usually associated with distress or impairment in personal, family, social, educational, occupational, or other important areas of functioning.”(Chapter 6, p.1 ICD-11, 2020)
3. Core Difficulties with the Definition and Operationalization of the Constructs Defined for Children with NDD
3.1. Problem 1: Distinguishing Mental Health Problems from Mental Illness and Mental Disorders in Children with NDD
3.1.1. Mental Disorders and Mental Illness—The Example of NDD
3.1.2. Mental Illness and Mental Health Problems
3.1.3. Difficulties in Defining and Operationalizing Mental Health Problems Following from Conceptual Diffuseness
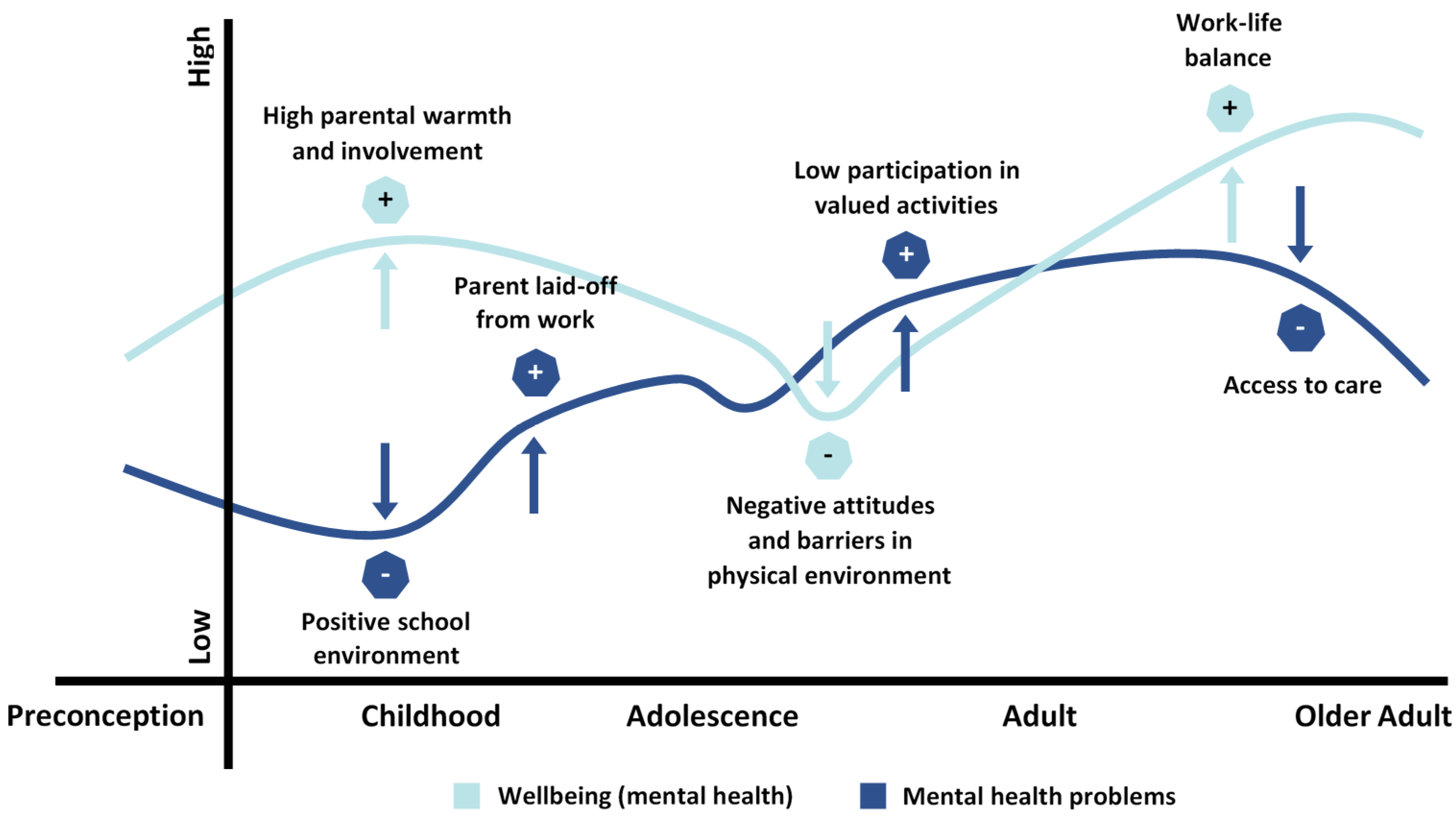
3.1.4. Mental Health Problems and Wellbeing (Mental Health) over the Life Course
3.2. Problem 2: Distinguishing Mental Health Problems and Wellbeing as Separate Constructs in Children with NDD
3.2.1. Mental Health—A Multidimensional Wellbeing Concept
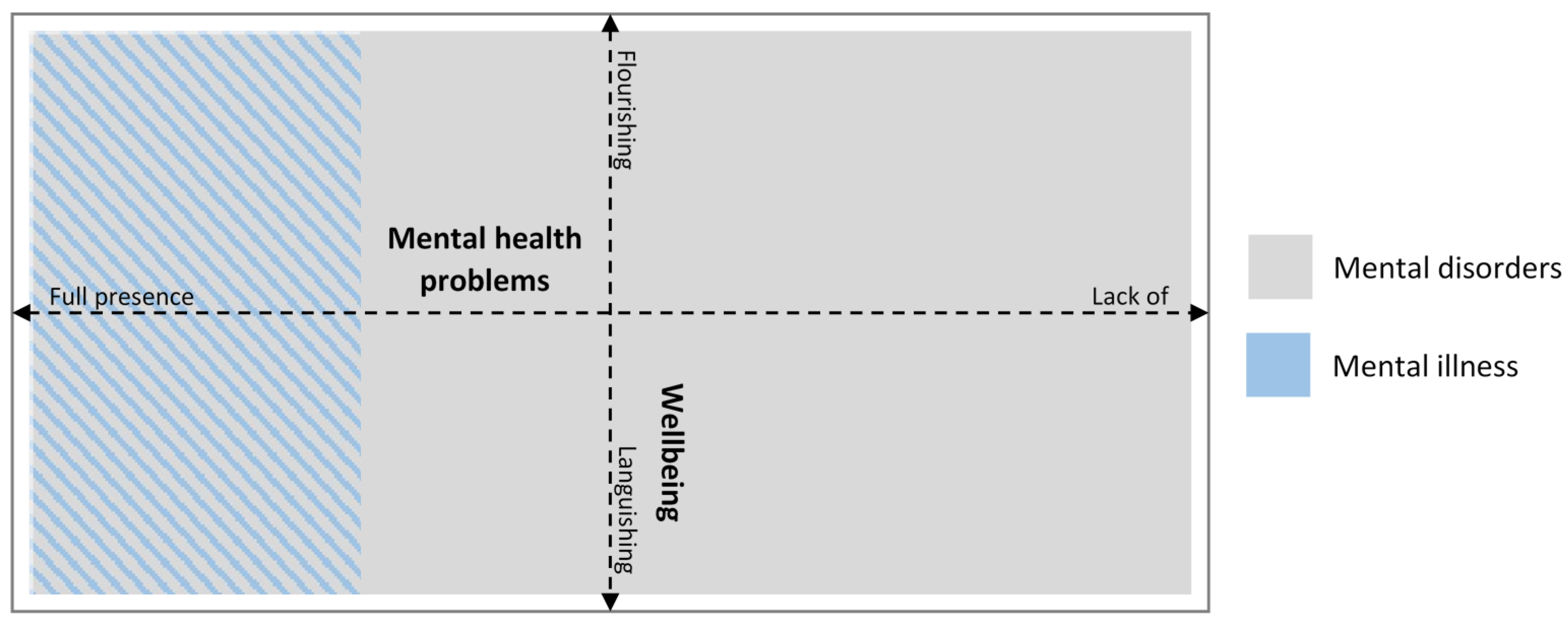
3.2.2. A Dual Model of Mental Health and Mental Health Problems
3.3. Problem 3: The Relationship between Participation and Wellbeing in Children with NDD
3.3.1. How Participation Is Conceptualized in Various Bodies of Literature
3.3.2. Antecedents and Consequences to Wellbeing and Participation
3.3.3. Relationships between Participation and Wellbeing
4. Implications for Measurement and Intervention with Children with NDD Following from the Three Propositions
4.1. Implications for Measurement: The Risk of Confusion between NDD-Core Symptoms, Mental Health Problems, and Wellbeing
4.2. Implications for Measurement: The Issue of Inclusiveness
4.3. Interventions Focused on Decreasing Mental Health Problems in Persons with NDD
4.4. Participation Interventions as a Means to Enhancing Wellbeing in Children and Adolescents with NDD
5. Conclusions
- (1)
- Mental disorders include both diagnoses related to impairments in the developmental period, i.e., NDD and diagnoses related to mental illness. These two types of mental disorders must be separated when measuring mental health in children with disabilities. Thus, summary indexes such as externalizing and internalizing problems should be avoided, since more stable characteristics related to impairment are conflated with mental health problem indicators. Measures of mental health problems involving only mental illness indicators and not NDD impairment-related symptoms need to be developed for children diagnosed within the NDD spectrum.
- (2)
- Mental health problems and wellbeing are two related but different continua where one focuses on mental health problems and illness and the other on different degrees of wellbeing; therefore, they must be measured separately. Children with NDD, just like other people, may exhibit aspects of both mental health problems and wellbeing simultaneously. Measures of wellbeing defined as a continuum from flourishing to languishing for children with NDD need to be designed and evaluated.
- (3)
- Wellbeing and participation are distinct from each other. Wellbeing is situated within the person and can be seen as a generalized measure of a person’s mental health within generalized contexts, while participation is always situated within a more specific context or activity. The relationship between the constructs can be seen as a spiral, where participation can be both an antecedent to wellbeing and a consequence of wellbeing. Because participation is contextualized, it can be the focus of direct interventions (targeted at the context or the person) that aim to enhance wellbeing. The relationship between participation and mental health problems is hypothesized to be indirect. By increasing or sustaining participation, wellbeing can be affected. Wellbeing will lead to further participation but also act as protection from mental health problems. The proposal that participation interventions can enhance wellbeing and indirectly lessen mental health problems needs to be tested in intervention research.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- King, G.; Law, M.; Hurley, P.; Petrenchik, T.; Schwellnus, H. A Developmental Comparison of the Out-of-school Recreation and Leisure Activity Participation of Boys and Girls With and Without Physical Disabilities. Int. J. Disabil. Dev. Educ. 2010, 57, 77–107. [Google Scholar] [CrossRef]
- Carlberg, L.; Granlund, M. Achievement and participation in schools for young adolescents with self-reported neuropsychiatric disabilities: A cross-sectional study from the southern part of Sweden. Scand. J. Public Health 2019, 47, 199–206. [Google Scholar] [CrossRef]
- Missiuna, C.; Moll, S.E.; King, S.; King, G.; Law, M. A trajectory of troubles: Parents’ impressions of the impact of developmental coordination disorder. Phys. Occup. Ther. Pediatr. 2007, 27, 81–101. [Google Scholar] [CrossRef]
- World Health Organization. ICD 11 Version 09/2020 [Internet]; World Health Organisation: Geneva, Switzerland, 2020; Available online: https://icd.who.int/en (accessed on 3 February 2021).
- Imms, C.; Granlund, M.; Wilson, P.H.; Steenbergen, B.; Rosenbaum, P.L.; Gordon, A.M. Participation, both a means and an end: A conceptual analysis of processes and outcomes in childhood disability. Dev. Med. Child Neurol. 2017, 59, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. ICF: International Classification of Functioning, Disability, and Health; World Health Organization: Geneva, Switzerland, 2001; Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 3 February 2021).
- Jewett, R.; Sabiston, C.M.; Brunet, J.; O’Loughlin, E.K.; Scarapicchia, T.; O’Loughlin, J. School sport participation during adolescence and mental health in early adulthood. J. Adolesc. Health 2014, 55, 640–644. [Google Scholar] [CrossRef]
- Augustin, L.; Granlund, M.; Lygnegård, F. Trajectories of participation, mental health and mental health problems in adolescents with self-reported neurodevelopmental disorders. Unpublished work, submitted D&R.
- Bremberg, S.; Dalman, C. Begrepp, Mätmetoder Och Förekomst Av Psykisk Hälsa, Psykisk Ohälsa Och Psykiatriska Tillstånd: En Kunskapsöversikt. (Constructs, Assessment Methods and Prevalence, Mental Health, Mental Illness and Mental Health Disorders); FORTE: Stockholm, Sweden, 2015; Available online: https://forte.se/publikation/begrepp-matmetoder/ (accessed on 3 February 2021).
- Jahoda, M. Joint Commission on Mental Health and Illness Monograph Series: Vol. 1. Current Concepts of Positive Mental Health; Basic Books: New York, NY, USA, 1958. [Google Scholar] [CrossRef]
- Westerhof, G.J.; Keyes, C.L. Mental Illness and Mental Health: The Two Continua Model Across the Lifespan. J. Adult Dev. 2009, 17, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Brooks, R.; Lambert, C.; Coulthard, L.; Pennington, L.; Kolehmainen, N. Social participation to support good mental health in neurodisability. Child. Care Health and Development. submitted.
- Hartley, M.; Dorstyn, D.; Due, C. Mindfulness for Children and Adults with Autism Spectrum Disorder and Their Caregivers: A Meta-analysis. J. Autism Dev. Disord. 2019, 49, 4306–4319. [Google Scholar] [CrossRef] [PubMed]
- Anaby, D.; Avery, L.; Gorter, J.W.; Levin, M.F.; Teplicky, R.; Turner, L.; Cormier, I.; Hanes, J. Improving body functions through participation in community activities among young people with physical disabilities. Dev. Med. Child Neurol. 2019, 62, 640–646. [Google Scholar] [CrossRef]
- Nguyen, M.N.; Watanabe-Galloway, S.; Hill, J.L.; Siahpush, M.; Tibbits, M.K.; Wichman, C. Ecological model of school engagement and attention-deficit/hyperactivity disorder in school-aged children. Eur. Child Adolesc. Psychiatry 2018, 28, 795–805. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; p. 5. [Google Scholar]
- Improving the Mental Health of the Population. Towards a Strategy on Mental Health for the European Union. Available online: https://ec.europa.eu/health/ph_determinants/life_style/mental/green_paper/mental_gp_en.pdf (accessed on 14 October 2005).
- World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice [Internet]; World Health Organization: Geneva, Switzerland, 2005; Available online: https://www.who.int/mental_health/evidence/en/promoting_mhh.pdf (accessed on 3 February 2021).
- Boniwell, I.; Henry, J. Developing conceptions of well-being: Advancing subjective, hedonic and hedonic theories. Soc. Psychol. Rev. 2007, 9, 3–18. [Google Scholar]
- Keyes, C.L.; Shmotkin, D.; Ryff, C.D. Optimizing well-being: The empirical encounter of two traditions. J. Personal. Soc. Psychol. 2002, 82, 1007–1022. [Google Scholar] [CrossRef]
- Copeland, W.E.; Adair, C.E.; Smetanin, P.; Stiff, D.; Briante, C.; Colman, I.; Fergusson, D.; Horwood, J.; Poulton, R.; Costello, E.J.; et al. Diagnostic transitions from childhood to adolescence to early adulthood. J. Child Psychol. Psychiatry 2013, 54, 791–799. [Google Scholar] [CrossRef]
- Bailey, T.; Totsika, V.; Hastings, R.P.; Hatton, C.; Emerson, E. Developmental trajectories of behaviour problems and prosocial behaviours of children with intellectual disabilities in a population-based cohort. J. Child Psychol. Psychiatry 2019, 60, 1210–1218. [Google Scholar] [CrossRef]
- Goodman, A.; Lamping, D.L.; Ploubidis, G.B. When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British Parents, Teachers and Children. J. Abnorm. Child Psychol. 2010, 38, 1179–1191. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Ruffle, T.M. The Child Behavior Checklist and Related Forms for Assessing Behavioral/Emotional Problems and Competencies. Pediatr. Rev. 2000, 21, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Will, M.N.; Wilson, B.J. A longitudinal analysis of parent and teacher ratings of problem behavior in boys with and without developmental delays. J. Intellect. Disabil. 2014, 18, 176–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halfon, N.; Larson, K.; Lu, M.; Tullis, E.; Russ, S. Lifecourse Health Development: Past, Present and Future. Matern. Child Health J. 2014, 18, 344–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Manderscheid, R.W.; Ryff, C.D.; Freeman, E.J.; McKnight-Eily, L.R.; Dhingra, S.; Strine, T.W. Evolving Definitions of Mental Illness and Wellness. Prev. Chronic Dis. 2009, 7, A19. [Google Scholar]
- Brown, T.M. “Hitting the Streets”: Youth Street Involvement as Adaptive Well-Being. Harv. Educ. Rev. 2016, 86, 48–71. [Google Scholar] [CrossRef]
- Halliday, A.J.; Kern, M.L.; Garrett, D.K.; Turnbull, D.A. The student voice in well-being: A case study of participatory action research in positive education. Educ. Action Res. 2019, 27, 173–196. [Google Scholar] [CrossRef] [Green Version]
- Herke, M.; Rathmann, K.; Richter, M. Trajectories of students’ well-being in secondary education in Germany and differences by social background. Eur. J. Public Health 2019, 29, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Kahana, E.; Bhatta, T.; Lovegreen, L.D.; Kahana, B.; Midlarsky, E. Altruism, helping, and volunteering: Pathways to well-being in late life. J. Aging Health 2013, 25, 159–187. [Google Scholar] [CrossRef] [Green Version]
- Goetzel, R.Z.; Ozminkowski, R.J.; Sederer, L.I.; Mark, T.L. The business case for quality mental health services: Why employers should care about the mental health and well-being of their employees. J. Occup. Environ. Med. 2002, 44, 320–330. [Google Scholar] [CrossRef]
- Dodge, R.; Daly, A.P.; Huyton, J.; Sanders, L.D. The challenge of defining wellbeing. Int. J. Wellbeing 2012, 2, 222–235. [Google Scholar] [CrossRef] [Green Version]
- Powell, M.A.; Graham, A.; Fitzgerald, R.; Thomas, N.P.; White, N.E. Wellbeing in schools: What do students tell us? Aust. Educ. Res. 2018, 45, 515–531. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. Mental health in adolescence: Is America’s youth flourishing? Am. J. Orthopsychiatry 2006, 76, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Skrzypiec, G.; Askell-Williams, H.; Slee, P.; Rudzinski, A. Students with Self-identified Special Educational Needs and Disabilities (si-SEND): Flourishing or Languishing! Int. J. Disabil. Dev. Educ. 2015, 63, 7–26. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Mental Illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boström, P.; Johnels, J.Å.; Thorson, M.; Broberg, M. Subjective Mental Health, Peer Relations, Family, and School Environment in Adolescents with Intellectual Developmental Disorder: A First Report of a New Questionnaire Administered on Tablet PCs. J. Ment. Health Res. Intellect. Disabil. 2016, 9, 207–231. [Google Scholar] [CrossRef]
- Franken, K.; Lamers, S.M.; Klooster, P.M.T.; Bohlmeijer, E.T.; Westerhof, G.J. Validation of the Mental Health Continuum-Short Form and the dual continua model of well-being and psychopathology in an adult mental health setting. J. Clin. Psychol. 2018, 74, 2187–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, K.A.; Turner, N.; Barling, J.; Kelloway, E.K.; McKee, M.C. Transformational leadership and psychological well-being: The mediating role of meaningful work. J. Occup. Health Psychol. 2007, 12, 193–203. [Google Scholar] [CrossRef] [Green Version]
- Donald, I.; Taylor, P.; Johnson, S.; Cooper, C.; Cartwright, S.; Robertson, S. Work environments, stress, and productivity: An examination using ASSET. Int. J. Stress Manag. 2005, 12, 409–423. [Google Scholar] [CrossRef] [Green Version]
- Nagin, D.S.; Smith, D.A. Participation in and frequency of delinquent behavior: A test for structural differences. J. Quant. Criminol. 1990, 6, 335–356. [Google Scholar] [CrossRef]
- Richard, L.; Gauvin, L.; Kestens, Y.; Shatenstein, B.; Payette, H.; Daniel, M.; Moore, S.; Levasseur, M.; Mercille, G. Neighborhood resources and social participation among older adults: Results from the VoisiNuage Study. J. Aging Health 2012, 25, 296–318. [Google Scholar] [CrossRef]
- Vaughan, M.W.; LaValley, M.P.; AlHeresh, R.; Keysor, J.J. Which features of the environment impact community participation of older adults? J. Aging Health 2016, 28, 957–978. [Google Scholar] [CrossRef]
- McEvoy, R.; Tierney, E.; Macfarlane, A.E. ‘Participation is integral’: Understanding the levers and barriers to the implementation of community participation in primary healthcare: A qualitative study using normalisation process theory. BMC Health Serv. Res. 2019, 19, 515. [Google Scholar] [CrossRef] [Green Version]
- Kupchik, A.; Catlaw, T.J. Discipline and Participation: The long term effects of suspension and school security on the political and civic engagement of youth. Youth Soc. 2012, 47, 95–124. [Google Scholar] [CrossRef]
- Zorec, M.B. Children’s Participation in Slovene Preschools: The Teachers’ Viewpoints and Practice. Eur. Educ. 2015, 47, 154–168. [Google Scholar] [CrossRef]
- Puritz, P.; Majd, K. ensuring authentic youth participation in delinquency cases: Creating a paradigm for specialized juvenile defense practice. Fam. Court. Rev. 2007, 45, 466–484. [Google Scholar] [CrossRef]
- Sierens, S.; Van Avermaet, P.; Van Houtte, M.; Agirdag, O. Does pre-schooling contribute to equity in education? Participation in universal pre-school and fourth-grade academic achievement. Eur. Educ. Res. J. 2020, 19, 564–586. [Google Scholar] [CrossRef]
- Frydenberg, E.; Ainley, M.; Russell, V. Schooling Issue Digest: Student Motivation and Engagement. In Australian Government Department of Education; Australian Government Department of Education: Canberra, Australia, 2005. [Google Scholar]
- Bergqvist, L.; Öhrvall, A.-M.; Himmelmann, K.; Peny-Dahlstrand, M. When I do, I become someone: Experiences of occupational performance in young adults with cerebral palsy. Disabil. Rehabil. 2017, 41, 341–347. [Google Scholar] [CrossRef]
- Hoogsteen, L.; Woodgate, R.L. Can I play? A conceptual analysis of participation in children with disabilities. Phys. Occup. Ther. Pediatr. 2010, 30, 325–339. [Google Scholar] [CrossRef]
- King, G.; Rigby, P.; Batorowicz, B. Conceptualizing participation in context for children and youth with disabilities: An activity setting perspective. Disabil. Rehabil. 2013, 35, 1578–1585. [Google Scholar] [CrossRef] [Green Version]
- King, G.; McPherson, A.C.; Kingsnorth, S.; Gorter, J.W.; Avery, L.; Rudzik, A.; Ontario Independence Program Research (OIPR) Team. Opportunities, experiences, and outcomes of residential immersive life skills programs for youth with disabilities. Disabil. Rehabil. 2020, 2020, 1–11. [Google Scholar] [CrossRef]
- Hayslip, J.B.; Blumenthal, H.; Garner, A. Health and Grandparent–Grandchild Well-Being: One-Year Longitudinal Findings for Custodial Grandfamilies. J. Aging Health 2014, 26, 559–582. [Google Scholar] [CrossRef] [PubMed]
- Hanniball, K.B.; Aknin, L.B.; Douglas, K.S.; Viljoen, J.L. Does helping promote well-being in at-risk youth and ex-offender samples? J. Exp. Soc. Psychol. 2019, 82, 307–317. [Google Scholar] [CrossRef]
- Parasuraman, S.; Purohit, Y.S.; Godshalk, V.M.; Beutell, N.J. work and family variables, entrepreneurial career success, and psychological well-being. J. Vocat. Behav. 1996, 48, 275–300. [Google Scholar] [CrossRef]
- Beresford, B.; Clarke, S. Improving the Wellbeing of Disabled Children and Young People through Improving Access to Positive and Inclusive Activities; Centre for Excellence and Outcomes in Children and Young People’s Services (C4EO): London, UK, August 2009; p. 89. [Google Scholar]
- Thoits, P.A. Social Support and Psychological Wellbeing: Theoretical possibilities; Sarason, G., Sarason, B.R., Eds.; Springer Nature Switzerland AG: Cham, Switzerland, 1985; pp. 51–72. [Google Scholar]
- Torok, M.; Rasmussen, V.; Wong, Q.; Werner-Seidler, A.; O’Dea, B.; Toumbourou, J.; Calear, A. Examining the impact of the good behaviour game on emotional and behavioural problems in primary school children: A case for integrating well-being strategies into education. Aust. J. Educ. 2019, 63, 292–306. [Google Scholar] [CrossRef]
- Reschly, A.L.; Christenson, S.L. Prediction of Dropout Among Students With Mild Disabilities: A Case for the Inclusion of Student Engagement Variables. Remedial Spéc. Educ. 2006, 27, 276–292. [Google Scholar] [CrossRef]
- Dashner, J.; Tello, S.M.E.; Snyder, M.; Hollingsworth, H.; Keglovits, M.; Campbell, M.L.; Putnam, M.; Stark, S. Examination of Community Participation of Adults With Disabilities: Comparing Age and Disability Onset. J. Aging Health 2019, 31 (Suppl. 10), 169S–194S. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.; Twardzik, E.; Meade, M.A.; Peterson, M.D.; Tate, D. Social participation among adults aging with long-term physical disability: The role of socioenvironmental factors. J. Aging Health 2019, 31, 145S–168S. [Google Scholar] [CrossRef] [PubMed]
- Woestehoff, S.A.; Redlich, A.D.; Cathcart, E.J.; Quas, J.A. Legal professionals’ perceptions of juvenile engagement in the plea process. Transl. Issues Psychol. Sci. 2019, 5, 121–131. [Google Scholar] [CrossRef]
- Bjerregaard, B.; Smith, C. Gender differences in gang participation, delinquency, and substance use. J. Quant. Criminol. 1993, 9, 329–355. [Google Scholar] [CrossRef]
- Gordon, R.A.; Rowe, H.L.; Pardini, D.; Loeber, R.; White, H.R.; Farrington, D.P. Serious Delinquency and Gang Participation: Combining and Specializing in Drug Selling, Theft, and Violence. J. Res. Adolesc. 2014, 24, 235–251. [Google Scholar] [CrossRef]
- Moon, N.W.; Todd, R.L.; Gregg, N.; Langston, C.L.; Wolfe, G. Determining the Efficacy of Communications Technologies and Practices to Broaden Participation in Education: Insights from a Theory of Change; Springer International Publishing: Cham, Switzerland, 2015; pp. 179–188. [Google Scholar]
- Roth, B.B.; Asbjørnsen, A.E.; Manger, T. The Relationship Between Prisoners’ Academic Self-efficacy and Participation in Education, Previous Convictions, Sentence Length, and Portion of Sentence Served. J. Prison. Educ. Reentry 2017, 3, 108–121. [Google Scholar] [CrossRef] [Green Version]
- Essuman, A.; Akyeampong, K. Decentralisation policy and practice in Ghana: The promise and reality of community participation in education in rural communities. J. Educ. Policy 2011, 26, 513–527. [Google Scholar] [CrossRef]
- Marston, C.; Hinton, R.; Kean, S.; Baral, S.; Ahuja, A.; Costello, A.; Portela, A. Community participation for transformative action on women’s, children’s and adolescents’ health. Bull. World Health Organ. 2016, 94, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Chenoweth, L.; Stehlik, D. Implications of social capital for the inclusion of people with disabilities and families in community life. Int. J. Incl. Educ. 2004, 8, 59–72. [Google Scholar] [CrossRef]
- Van Campen, C.; Iedema, J. Are persons with physical disabilities who participate in society healthier and happier? Structural equation modelling of objective participation and subjective well-being. Qual. Life Res. 2007, 16, 635–645. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Sjöman, M.; Granlund, M.; Almqvist, L. Interaction processes as a mediating factor between children’s externalized behaviour difficulties and engagement in preschool. Early Child Dev. Care 2016, 186, 1649–1663. [Google Scholar] [CrossRef] [Green Version]
- Gómez, L.E.; Alcedo, M.Á.; Arias, B.; Fontanil, Y.; Arias, V.B.; Monsalve, A.; Verdugo, M. A new scale for the measurement of quality of life in children with intellectual disability. Res. Dev. Disabil. 2016, 54, 399–410. [Google Scholar] [CrossRef]
- Adair, B.; Ullenhag, A.; Rosenbaum, P.L.; Granlund, M.; Keen, D.; Imms, C. A systematic review of measures used to quantify participation in childhood disability and their alignment with the family of participation-related constructs. Dev. Med. Child Neurol. 2018, 60, 1101–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsyth, R.; Jarvis, S. Participation in childhood. Child Care Health Dev. 2002, 28, 277–279. [Google Scholar] [CrossRef]
- King, G.; Law, M.; King, S.; Hurley, P.; Hanna, S.; Kertoy, M.; Rosenbaum, P. Measuring children’s participation in recreation and leisure activities: Construct validation of the CAPE and PAC. Child Care Health Dev. 2006, 33, 28–39. [Google Scholar] [CrossRef]
- Williams, K.; Brignell, A.; Randall, M.; Silove, N.; Hazell, P. Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2013, 20, CD004677. [Google Scholar] [CrossRef]
- Luxford, S.; Hadwin, J.A.; Kovshoff, H. Evaluating the Effectiveness of a School-Based Cognitive Behavioural Therapy Intervention for Anxiety in Adolescents Diagnosed with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 3896–3908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hronis, A.; Roberts, R.M.; Roberts, L.; Kneebone, I. Fearless Me! ©: A feasibility case series of cognitive behavioral therapy for adolescents with intellectual disability. J. Clin. Psychol. 2019, 75, 919–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchiato, M.; Sacchi, C.; Simonelli, A.; Purgato, N. Evaluating the efficacy of psychodynamic treatment on a single case of autism. A qualitative research. Res. Psychother. Psychopathol. Process Outcome 2016, 19, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.J.; Ehrenreich-May, J.; Alessandri, M.; Fujii, C.; Renno, P.; Laugeson, E.; Piacentini, J.C.; De Nadai, A.S.; Arnold, E.; Lewin, A.B.; et al. Cognitive behavioral therapy for early adolescents with autism spectrum disorders and clinical anxiety: A randomized, controlled trial. Behav. Ther. 2015, 46, 7–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, B.; Smart, E.; King, G.; Curran, C.; Kingsnorth, S. Performance and visual arts-based programs for children with disabilities: A scoping review focusing on psychosocial outcomes. Disabil. Rehabil. 2018, 42, 574–585. [Google Scholar] [CrossRef]
- Martin, R.A.; Graham, F.P.; Taylor, W.J.; Levack, W. Mechanisms of Change for Children Participating in Therapeutic Horse Riding: A Grounded Theory. Phys. Occup. Ther. Pediatr. 2017, 38, 510–526. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, J.R.; Noh, S.; Laliberte, D.; Allan, D.E.; Lariviere, J. Therapeutic Horseback Riding: A review of the literature. Phys. Occup. Ther. Pediatr. 1995, 15, 1–15. [Google Scholar] [CrossRef]
- Schwellnus, H.; King, G.; Baldwin, P.; Keenan, S.; Hartman, L.R. A Solution-Focused Coaching Intervention with Children and Youth with Cerebral Palsy to Achieve Participation-Oriented Goals. Phys. Occup. Ther. Pediatr. 2020, 40, 423–440. [Google Scholar] [CrossRef]
- Graham, F.; Rodger, S.; Ziviani, J. Enabling Occupational Performance of Children Through Coaching Parents: Three Case Reports. Phys. Occup. Ther. Pediatr. 2010, 30, 4–15. [Google Scholar] [CrossRef]
- Grant, A.M. The impact of life coaching on goal attainment, metacognition and mental health. Soc. Behav. Pers. Int. J. 2003, 31, 253–263. [Google Scholar] [CrossRef]
- Dray, J.; Bowman, J.; Campbell, E.; Freund, M.; Wolfenden, L.; Hodder, R.K.; McElwaine, K.; Tremain, D.; Bartlem, K.; Bailey, J.; et al. Systematic Review of Universal Resilience-Focused Interventions Targeting Child and Adolescent Mental Health in the School Setting. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 813–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Mental disorder | Mental, behavioral, and neurodevelopmental disorders are syndromes characterized by clinically significant disturbance in an individual’s cognition, emotional regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes that underlie mental and behavioral functioning. These disturbances are usually associated with distress or impairment in personal, family, social, educational, occupational, or other important areas of functioning. ICD 11, version 09/2020, chapter 6 (http://id.who.int/icd/entity/334423054) [4] |
| Neurodevelopmental disorder | Neurodevelopmental disorders are behavioral and cognitive disorders that arise during the developmental period that involve significant difficulties in the acquisition and execution of specific intellectual, motor, language, or social functions. Although behavioral and cognitive deficits are present in many mental and behavioral disorders that can arise during the developmental period (e.g., Schizophrenia, Bipolar disorder), only disorders whose core features are neurodevelopmental are included in this grouping. The presumptive etiology for neurodevelopmental disorders is complex, and in many individual cases is unknown. ICD 11, version 09/2020, chapter 6 (http://id.who.int/icd/entity/1516623224) [4] |
| Mental illness | Mental illness (mental ill health) includes severe mental health problems and strain, impaired functioning associated with distress, symptoms and diagnosable mental disorders (e.g., schizophrenia, bipolar disorder) (European Commission, 2005) [17] |
| Mental health problems | A broad concept covering both less serious mental strain and more severe symptoms, fulfilling criteria for a diagnosable mental illness [9] |
| Mental health | “is a state of wellbeing in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community’’ [18] (p. 2). Mental health defined as wellbeing vary over the life course. The description of wellbeing below is here used as an operationalization of mental health. |
| Wellbeing as mental health | Wellbeing’s positive emotional states include the two different ideas of happiness: hedonic (happiness or pleasure), that is living a pleasant life, or eudemonic (striving for, achieving something more—either personal growth or something outside the self), that is, living a goal directed or meaningful life [19,20]. |
| Flourishing | “Adults with complete mental health are flourishing in life with high levels of wellbeing. To be flourishing, then, is to be filled with positive emotion and to be functioning well psychologically and socially.” [20] |
| Languishing | A state of a low level of wellbeing described as unhappiness and experiencing difficulties: “Adults with incomplete mental health are languishing in life with low wellbeing. Thus, languishing may be conceived of as emptiness and stagnation, constituting a life of quiet despair that parallels accounts of individuals who describe themselves and life as “hollow”, “empty”, “a shell”, and “a void” [20]. The definition focuses on low levels of wellbeing rather than expressions of mental health problems. |
| Participation | Involvement in a life situation comprising of two dimensions: attendance and involvement [5]. |
| Participation as attendance | “Being there”, that is being present (physically or virtually) in the life situation [5]. |
| Participation as involvement | The “experience of participation while attending the life situation” [5]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granlund, M.; Imms, C.; King, G.; Andersson, A.K.; Augustine, L.; Brooks, R.; Danielsson, H.; Gothilander, J.; Ivarsson, M.; Lundqvist, L.-O.; et al. Definitions and Operationalization of Mental Health Problems, Wellbeing and Participation Constructs in Children with NDD: Distinctions and Clarifications. Int. J. Environ. Res. Public Health 2021, 18, 1656. https://doi.org/10.3390/ijerph18041656
Granlund M, Imms C, King G, Andersson AK, Augustine L, Brooks R, Danielsson H, Gothilander J, Ivarsson M, Lundqvist L-O, et al. Definitions and Operationalization of Mental Health Problems, Wellbeing and Participation Constructs in Children with NDD: Distinctions and Clarifications. International Journal of Environmental Research and Public Health. 2021; 18(4):1656. https://doi.org/10.3390/ijerph18041656
Chicago/Turabian StyleGranlund, Mats, Christine Imms, Gillian King, Anna Karin Andersson, Lilly Augustine, Rob Brooks, Henrik Danielsson, Jennifer Gothilander, Magnus Ivarsson, Lars-Olov Lundqvist, and et al. 2021. "Definitions and Operationalization of Mental Health Problems, Wellbeing and Participation Constructs in Children with NDD: Distinctions and Clarifications" International Journal of Environmental Research and Public Health 18, no. 4: 1656. https://doi.org/10.3390/ijerph18041656