
Evaluation of the Use of Shared Decision Making in Breast Cancer: International Survey

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Measurement
2.2. Period and Scope of the Study
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Participants
3.2. Global Analysis of the Survey and Comparison between Countries
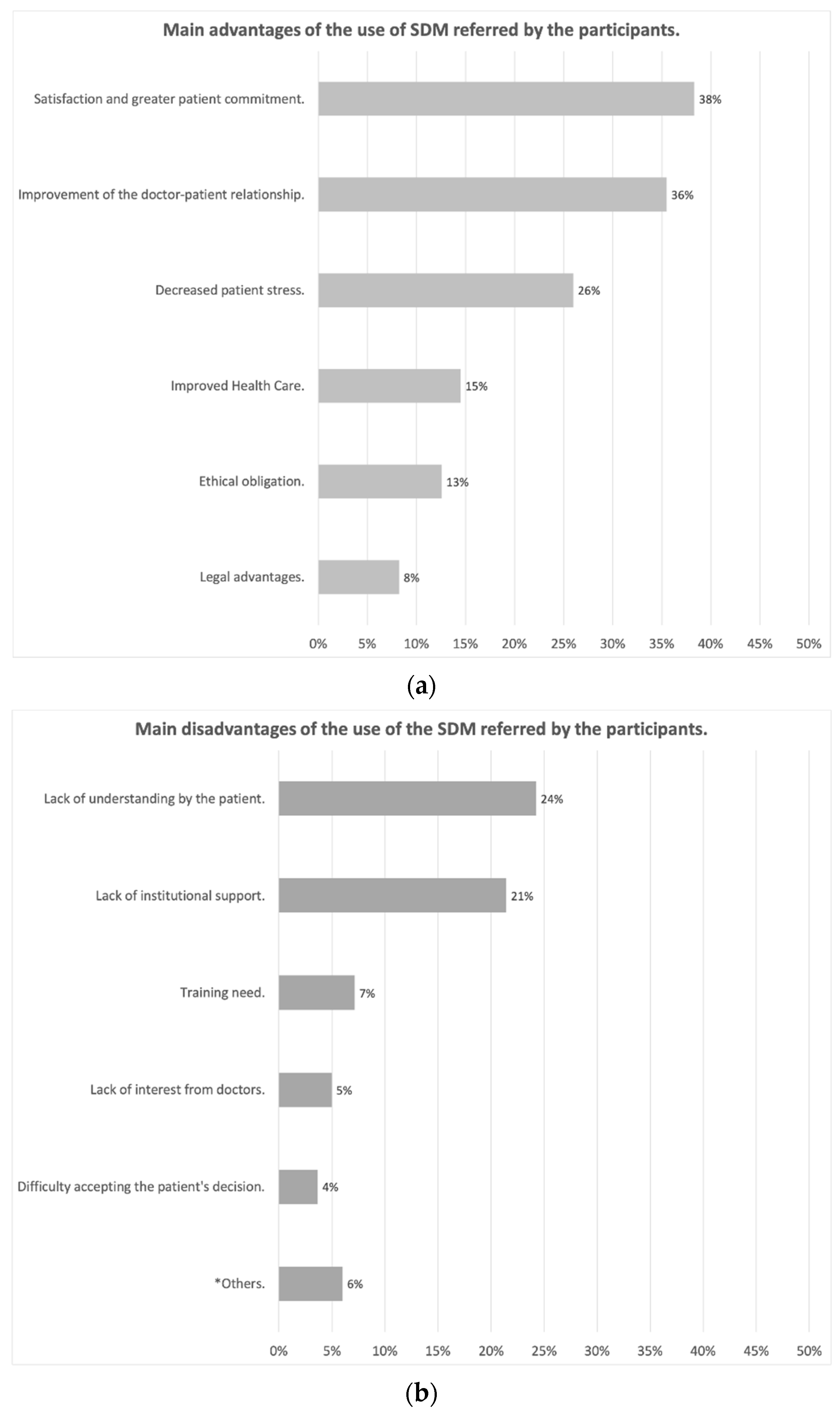
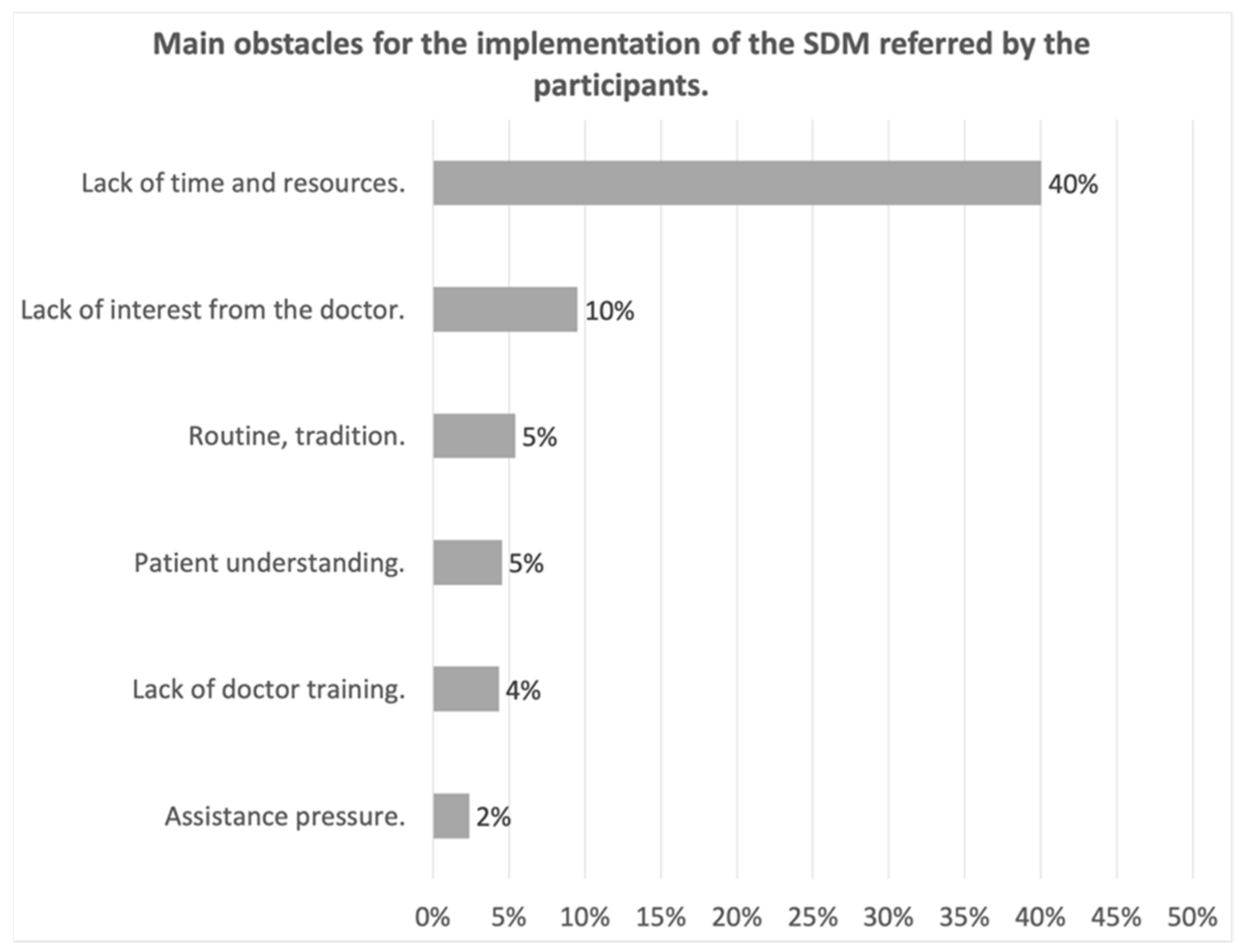
3.3. Advantages, Disadvantages and Main Obstacles to the Implementation of the SDM
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- ◯
- Sexo:
- ◯
- Hombre.
- ◯
- Mujer.
- ◯
- Edad:
- ◯
- <35 años.
- ◯
- 36–50 años.
- ◯
- 51–65 años.
- ◯
- >65 años.
- ◯
- ¿En qué periodo de su carrera profesional se encuentra?
- ◯
- Médico Interno Residente (MIR).
- ◯
- Facultativo Especialista de Área (FEA).
- ◯
- Responsable de Servicio o Unidad.
- ◯
- Otros: __________
- ◯
- ¿Qué tipo de especialidad tiene?
- ◯
- Cirugía General
- ◯
- Ginecología y Obstetricia
- ◯
- Anatomía Patológica
- ◯
- Radiología
- ◯
- Oncología
- ◯
- Medicina de Familia
- ◯
- Otros: _________________
- ◯
- Tipo de Servicio o Unidad donde desarrolla su ejercicio:
- ◯
- Servicio de Cirugía General y del Aparato Digestivo o Ginecología y Obstetricia.
- ◯
- Servicio de Cirugía General o Ginecología con especial dedicación a la Mama.
- ◯
- Unidad de Mama.
- ◯
- Otros: __________________
- ◯
- Ámbito donde desarrolla su ejercicio (puede marcar más de una opción):
- ◯
- Hospital público o perteneciente al Servicio Sanitario Público.
- ◯
- Compañía u Hospital Privado.
- ◯
- Otras situaciones: ______________________
- ◯
- Hospital regional o de referencia
- ◯
- Hospital de especialidades
- ◯
- Hospital de área o comarcal
- ◯
- Hospital de alta resolución
- ◯
- Número de casos de Cáncer de Mama atendidos por su Servicio o Unidad al año:
- ◯
- <100
- ◯
- 100–149
- ◯
- 150–199.
- ◯
- 200–249
- ◯
- 250 o más
- ◯
- Número de pacientes con Cáncer de Mama atendidos en consulta por usted al año:
- ◯
- <100
- ◯
- 100–149
- ◯
- 150–199.
- ◯
- 200–249
- ◯
- 250 o más
- ◯
- Porcentaje de casos de Cáncer de Mama atendidos en su hospital en los que se realiza una toma de decisiones compartidas
- ◯
- <33%
- ◯
- 33–66%
- ◯
- >66%
- ◯
- No lo sé
| Totalmente en Desacuerdo | En Desacuerdo | Ni de Acuerdo ni en Desacuerdo | De Acuerdo | Totalmente de Acuerdo | ||
| 1 | Conozco el concepto y los fundamentos de la Toma de Decisiones Compartida (TDC) | 1 | 2 | 3 | 4 | 5 |
| 2 | La TDC es una herramienta necesaria para proporcionar una asistencia de calidad. | 1 | 2 | 3 | 4 | 5 |
| 3 | La importancia de la TDC aumenta cuando existen diversas opciones de tratamiento con resultados similares, en las que la selección de una u otra opción depende de las preferencias del paciente. | 1 | 2 | 3 | 4 | 5 |
| 4 | La TDC aumenta la satisfacción del paciente, mejora la rentabilidad y reduce las demandas por negligencia. | 1 | 2 | 3 | 4 | 5 |
| 5 | La TDC es un elemento básico en la relación del cirujano con los pacientes con Cáncer de Mama (CM). | 1 | 2 | 3 | 4 | 5 |
| 6 | Todos los médicos deberían preguntar a sus pacientes exactamente cómo les gustaría participar en la toma de decisiones. | 1 | 2 | 3 | 4 | 5 |
| 7 | Todos los médicos deberían informar a sus pacientes sobre las diferentes opciones de tratamiento existentes para su problema de salud. | 1 | 2 | 3 | 4 | 5 |
| 8 | Todos los médicos deberían explicar a sus pacientes todas las opciones de tratamiento, incluyendo la posibilidad de no realizar ningún tratamiento. | 1 | 2 | 3 | 4 | 5 |
| 9 | Todos los médicos deberían explicar a sus pacientes los beneficios, riesgos y efectos secundarios de los posibles tratamientos. | 1 | 2 | 3 | 4 | 5 |
| 10 | Todos los médicos deberían ayudar a sus pacientes a entender toda la información que se les proporciona. | 1 | 2 | 3 | 4 | 5 |
| 11 | Todos los médicos deberían preguntar a sus pacientes qué opción de tratamiento prefieren. | 1 | 2 | 3 | 4 | 5 |
| 12 | La mayor parte de los pacientes considera que el médico es la persona más adecuada para decidir cuál es la mejor opción terapéutica. | 1 | 2 | 3 | 4 | 5 |
| 13 | Todos los médicos deberían proporcionar a sus pacientes el tiempo suficiente para que puedan valorar las diferentes opciones de tratamiento. | 1 | 2 | 3 | 4 | 5 |
| 14 | Todos los médicos deberían escoger conjuntamente con sus pacientes la opción de tratamiento. | 1 | 2 | 3 | 4 | 5 |
| 15 | Todos los médicos deberían consensuar con sus pacientes el seguimiento de su proceso. | 1 | 2 | 3 | 4 | 5 |
| 16 | Mi Unidad tiene experiencia en el uso de la TDC en cáncer de mama. | 1 | 2 | 3 | 4 | 5 |
| Totalmente en Desacuerdo | En Desacuerdo | Ni de Acuerdo ni en Desacuerdo | De Acuerdo | Totalmente de Acuerdo | ||
| 17 | Mi Unidad dispone de una consulta específica para explicar las opciones de tratamiento y facilitar la TDC. | 1 | 2 | 3 | 4 | 5 |
| 18 | Mi Unidad dispone del tiempo necesario para practicar la TDC en la asistencia del CM | 1 | 2 | 3 | 4 | 5 |
| 19 | Mi Unidad dispone de los materiales necesarios para practicar la TDC en el CM | 1 | 2 | 3 | 4 | 5 |
| 20 | Mi hospital debería promocionar más la comunicación con el paciente y la TDC | 1 | 2 | 3 | 4 | 5 |
| 21 | En general, debería haber más formación sobre comunicación con el paciente y la TDC | 1 | 2 | 3 | 4 | 5 |
| 22 | La TDC puede ser útil para la asistencia sanitaria de carácter privado, pero no tiene aplicación en la asistencia sanitaria pública, el paciente no puede decidir sobre la opción de tratamiento más eficiente | 1 | 2 | 3 | 4 | 5 |
| 23 | En el futuro se aplicará cada vez más la TDC en la atención al CM | 1 | 2 | 3 | 4 | 5 |
References
- SEOM. The Numbers of Breast Cancer in Spain; SEOM: Madrid, Spain, 2020. [Google Scholar]
- Abt Sacks, A.; Perestelo-Perez, L.; Rodriguez-Martin, B.; Cuellar-Pompa, L.; Algara López, M.; González Hernández, N.; Serrano-Aguilar, P. Breast cancer patients’ narrative experiences about communication during the oncology care process: A qualitative study. Eurp. J. Cancer Care 2016, 25, 719–733. [Google Scholar] [CrossRef] [PubMed]
- Acebal Blanco, M.M.; Alba Conejo, E.; Alvarez Benito, M.; Bayo Lozano, E.; Del Río Urenda, S.; Dotor Gracia, M.; Dueñas Rodríguez, B.; Fernández Echegaray, R.; Fernández Temprano, J.M.; Galván Ruiz, A.; et al. Breast Cancer Integrating Health Care Process, 3rd ed.; Consejería de Salud: Sevilla, Spain, 2011. [Google Scholar]
- Elwyn, G.; Frosch, D.L.; Kobrin, S. Implementing shared decision-making: Consider all the consequences. Implement Sci. 2016, 11, 114. [Google Scholar] [CrossRef] [Green Version]
- AECC. Estudio de Investigación “Necesidades no Clínicas de los Pacientes con Cáncer y Sus; AECC University College: Bournemouth, UK, 2018. [Google Scholar]
- Acompañantes en España: Research Study “Non-Clinical Needs of Cancer Patients and Their Companions in Spain: A Multidisciplinary Vision”; Half of Cancer Patients do not Participate in Decision-Making about Their Treatment; Consejería de Salud: Seville, Spain, 2018.
- International Shared Decision Making Society. 2018. Available online: https://www.isdmsociety.org/ (accessed on 1 January 2021).
- The Patients Association. Shared Decision Making. 2020. Available online: https://www.patients-association.org.uk/shared-decision-making (accessed on 15 January 2021).
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Stephen, R.; et al. Shared Decision Making: A Model for Clinical Practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef] [Green Version]
- Perestelo-Perez, L.; Rivero-Santana, A.; Perez-Ramos, J.; Gonzalez-Lorenzo, M.; Roman, J.G.; Serrano-Aguilar, P. Shared decision making in Spain: Current state and future perspectives. Z. Evid. Fortbild. Qual. Gesundhwes. 2011, 105, 289–295. [Google Scholar] [CrossRef]
- Levit, L.; Balogh, E.; Nass, S.; Ganz, P. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis; The National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Estado BOE. Basic Law 41/2002 Regulating the Autonomy of the Patient and Rights and Obligations Regarding Information and Clinical Documentation; Estado BOE: Madrid, Spain, 2002. [Google Scholar]
- Department of Health. Equity and Excellence: Liberating the NHS; Department of Health: London, UK, 2010.
- Senate and House of Representatives. Patient Protection and Affordable Care Act. HR 3590; United States Congress: Washington, DC, USA, 2010. [Google Scholar]
- Department of Health (DoH), UK. Liberating the NHS: No Decision about Me without Me. 2010. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/216980/Liberating-the-NHS-No-decision-about-me-without-me-Government-response.pdf (accessed on 15 January 2021).
- Schoenfeld, E.M.; Mader, S.; Houghton, C.; Wenger, R.; Probst, M.A.; Schoenfeld, D.A.; Lindenauer, P.K.; Mazor, K.M. The Effect of Shared Decisionmaking on Patients’ Likelihood of Filing a Complaint or Lawsuit: A Simulation Study. Ann. Emerg. Med. 2019, 74, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Pope, T.M. Certified Patient Decision Aids: Solving Persistent Problems with Informed Consent Law. J. Law Med. Ethics 2017, 45, 12–40. [Google Scholar] [CrossRef]
- Légaré, F.; Adekpedjou, R.; Stacey, D.; Turcotte, S.; Kryworuchko, J.; Graham, I.D.; Lyddiatt, A.; Politi, M.C.; Thomson, R.; Elwyn, G.; et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database Sys. Rev. 2018. [Google Scholar] [CrossRef]
- Staveley, I.; Sullivan, P. We need more guidance on shared decision making. Br. J. Gen. Pract. 2015, 65, 663–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennke, S.; Yuan, P.; Monash, B.; Blankenburg, R.; Chua, I.; Harman, S.; Sakai, D.; Khan, A.; Hilton, J.; Sieh, L.; et al. The SDM 3 circle model: A literature synthesis and adaptation for shared decision-making in the hospital. J. Hosp. Med. 2017, 12, 1001. [Google Scholar] [CrossRef] [Green Version]
- Legare, F.; Ratte, S.; Gravel, K.; Graham, I.D. Barriers and facilitators to implementing shared decision-making in clinical practice: Update of a systematic review of health professionals’ perceptions. Patient Educ. Couns. 2008, 73, 526–535. [Google Scholar] [CrossRef]
- McCune, L.M.; Kubota, C.; Stendell-Hollis, N.R.; Thomson, C.A. Cherries and health: A review. Crit. Rev. Food Sci. Nutr. 2010, 51, 1–12. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Rodriguez, J.A. Improving the quality of Spanish web surveys: Spanish adaptation of the checklist for reporting results of internet e-surveys (CHERRIES) to the Spanish context. Atención Primaria 2019, 51, 586–589. [Google Scholar]
- Maes-Carballo, M.; Munoz-Nunez, I.; Martin-Diaz, M.; Mignini, L.; Bueno-Cavanillas, A.; Khan, K.S. Shared decision making in breast cancer treatment guidelines: Development of a quality assessment tool and a systematic review. Health Expect. 2020, 23, 1045–1064. [Google Scholar] [CrossRef]
- Maes-Carballo, M.; Martín-Díaz, M.; Mignini, L. Shared decision-making: Looking towards the future of high-quality medical practice in breast cancer. Rev. Senol. Patol. Mamaria 2021. [Google Scholar] [CrossRef]
- Rensis, L. A technique for the measurement of attitudes. Arch. Psych. 1932, 140, 1–55. [Google Scholar]
- Krosnick, J.A. Chapter 9: Question and Questionnaire Design. In The Palgrave Handbook of Survey Research; Palgrave Macmillan: Cham, Switzerland, 2010; pp. 263–313. [Google Scholar]
- VanGeest, J.B.; Johnson, T.P.; Welch, V.L. Methodologies for improving response rates in surveys of physicians: A systematic review. Eval. Health Prof. 2007, 30, 303–321. [Google Scholar] [CrossRef]
- Lensing, S.Y.; Gillaspy, S.R.; Simpson, P.M.; Jones, S.M.; James, J.M.; Smith, J.M. Encouraging physicians to respond to surveys through the use of fax technology. Eval. Health Prof. 2000, 23, 348–359. [Google Scholar] [CrossRef]
- Google. Google Forms. 2020. Available online: https://www.google.com/intl/es_es/forms/about/ (accessed on 15 January 2021).
- Expansión/Datosmacro.com. Comparing Economy of Countries: Argentina vs. Spain. 2019. Available online: https://datosmacro.expansion.com/paises/comparar/argentina/espana (accessed on 19 February 2021).
- Ong, A.D.; Weiss, D.J. The impact of anonymity on responses to sensitive questions. J. Appl. Soc. Psychol. 2000, 30, 1691–1708. [Google Scholar] [CrossRef]
- Phillips, D.L.; Clancy, K.J. Some effects of “social desirability” in survey studies. Am. J. Sociol. 1972, 77, 921–940. [Google Scholar] [CrossRef]
- Lelkes, Y.; Krosnick, J.A.; Marx, D.M.; Judd, C.M.; Park, B. Complete Anonymity Compromises the Accuracy of Self-Reports. J. Exp. Soc. Psych. 2011, 48, 1291–1299. [Google Scholar] [CrossRef]
- Field, T.S.; Cadoret, C.A.; Brown, M.L.; Ford, M.; Greene, S.M.; Hill, D.; Hornbrook, M.C.; Meenan, R.T.; White, M.J.; Zapka, J.M. Surveying physicians: Do components of the “Total Design Approach” to optimizing survey response rates apply to physicians? Med. Care 2002, 40, 596–606. [Google Scholar] [CrossRef]
- Kellerman, S.E.; Herold, J. Physician response to surveys: A review of the literature. Am. J. Prev. Med. 2001, 20, 61–67. [Google Scholar] [CrossRef]
- McFarlane, E.; Olmsted, M.G.; Murphy, J.; Hill, C.A. Nonresponse bias in a mail survey of physicians. Paper presented at the annual conference of the American Association for Public Opinion Research, Montreal, Quebec. Eval. Health Prof. 2006, 30, 170–185. [Google Scholar] [CrossRef]
- Masino, C.; Lam, T.C. Choice of rating scale labels: Implication for minimizing patient satisfaction response ceiling effect in telemedicine surveys. Telemed. J. e-Health 2014, 20, 1150–1155. [Google Scholar] [CrossRef]
- Birkett, N.J. Selecting the Number of Response Categories for a Likert-type Scale. J. Am. Stat. Assoc. 1986, 81, 488–492. [Google Scholar]
- Masters, J.R. The relationship between number of response categories and reliability of likert-type questionnaires. J. Educ. Meas. 1974, 11, 49–53. [Google Scholar] [CrossRef]
- Biganzoli, L.; Cardoso, F.; Beishon, M.; Cameron, D.; Cataliotti, L.; Coles, C.E.; Delgado Bolton, R.C.; Die Trill, M.; Erdem, S.; Fjell, M.; et al. The requirements of a specialist breast centre. Breast 2020, 51, 65–84. [Google Scholar] [CrossRef] [PubMed]
- Manhas, K.P.; Olson, K.; Churchill, K.; Faris, P.; Vohra, S.; Wasylak, T. Measuring shared decision-making and collaborative goal setting in community rehabilitation: A focused ethnography using cross-sectional surveys in Canada. BMJ Open 2020, 10, e034745. [Google Scholar] [CrossRef] [PubMed]
- Haesebaert, J.; Adekpedjou, R.; Croteau, J.; Robitaille, H.; Légaré, F. Shared decision-making experienced by Canadians facing health care decisions: A Web-based survey. CMAJ Open 2019, 7, E210–E216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, H.; Freeman, K.; Clark, K.U.S. Survey of Shared Decision Making Use for Treating Pregnant Women Presenting with Opioid Use Disorder. Subst. Use Misuse 2019, 54, 2241–2250. [Google Scholar] [CrossRef]
- Yen, R.W.; Barr, P.J.; Cochran, N.; Aarts, J.W.; Légaré, F.; Reed, M.; O’Malley, A.J.; Scalia, P.; Guérard, G.P.; Backer, G.; et al. Medical Students’ Knowledge and Attitudes Toward Shared Decision Making: Results From a Multinational, Cross-Sectional Survey. MDM Policy Pract. 2019, 4, 2381468319885871. [Google Scholar] [CrossRef] [PubMed]
- Wieringa, T.H.; Kunneman, M.; Rodriguez-Gutierrez, R.; Montori, V.M.; de Wit, M.; Smets, E.M.A.; Schoonmade, L.J.; Spencer-Bonilla, G.; Snoek, F.J. A systematic review of decision aids that facilitate elements of shared decision-making in chronic illnesses: A review protocol. Syst. Rev. 2017, 6, 155. [Google Scholar] [CrossRef] [Green Version]
- Legare, F.; Thompson-Leduc, P. Twelve myths about shared decision making. Patient Educ. Couns. 2014, 96, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stacey, D.; Hill, S.; McCaffery, K.; Boland, L.; Lewis, K.B.; Horvat, L. Shared Decision Making Interventions: Theoretical and Empirical Evidence with Implications for Health Literacy. In Health Literacy: New Directions in Research, Theory and Practice; Logan, R.A., Siegel, E.R., Eds.; Studies in Health Technology and Informatics; IOS Press: Amsterdam, The Netherlands, 2017; pp. 263–283. [Google Scholar]
- Gillick, M.R. Re-engineering shared decision-making. J. Med. Ethics 2015, 41, 785–788. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Argentina | Spain | Total | p-Value | |
|---|---|---|---|---|
| Gender | ||||
| Men | 121 (51.27%) | 97 (44.10%) | 218 (47.80%) | p = 0.125 |
| Women | 115 (48.73%) | 123 (55.90%) | 238 (52.19%) | |
| Total | 236 (100%) | 220 (100%) | 456 (100%) | |
| Age | ||||
| <35 yo | 130 (54.62%) | 80 (36.36%) | 210 (45.85%) | p = 0.001 |
| 35–50 yo | 66 (27.73%) | 105 (47.73%) | 171 (37.35%) | |
| 51–65 yo | 16 (6.72%) | 17 (7.73%) | 33 (7.20%) | |
| >65 yo | 26 (10.93%) | 18 (8.18%) | 44 (9.60%) | |
| Total | 238 (100%) | 220 (100%) | 458 (100%) | |
| Professional career period | ||||
| MR | 0 (0%) | 8 (3.63%) | 8 (1.75%) | p = 0.001 |
| MAS | 169 (71.00%) | 127 (57.73%) | 296 (64.63%) | |
| Head of Service | 67 (28.99%) | 74 (33.64%) | 141 (30.78%) | |
| Other | 2 (0.01%) | 11 (5%) | 13 (2.84%) | |
| Total | 238 (100%) | 220 (100%) | 458 (100%) | |
| Speciality | ||||
| General Surgery | 0 (0%) | 126 (56.25%) | 126 (27.27%) | p = 0.001 |
| Plastic Surgery | 72 (30.25%) | 61 (27.23%) | 133 (28.78%) | |
| Mastology * | 122 (51.26%) | 0 (0%) | 122 (26.41%) | |
| Others Speciality | 44 (18.49%) | 37 (16.52%) | 81 (17.54%) | |
| Total | 238 (100%) | 224 (100%) | 462 (100%) | |
| Kind of service | ||||
| Breast Unit | 131 (39.70%) | 199 (88.83%) | 330 (71.42%) | p = 0.001 |
| Without Breast Unit | 107 (81.06%) | 25 (11.16%) | 132 (28.57%) | |
| Total | 236 (100%) | 224 (100%) | 462 (100%) | |
| Hospital | ||||
| Public | 94 (39.50%) | 172 (76.79%) | 266 (57.58%) | p = 0.001 |
| Private | 144 (60.50%) | 52 (23.21%) | 196 (42.42%) | |
| Total | 238 (100%) | 224 (100%) | 462 (100%) | |
| BC cases/year/hospital | ||||
| <100 | 106 (44.54%) | 54 (24.66%) | 160 (35.01%) | p = 0.001 |
| 100–149 | 52 (21.85%) | 41 (18.72%) | 93 (20.35%) | |
| 150–199 | 30 (12.61%) | 32 (14.61%) | 62 (13.56%) | |
| 200–249 | 19 (7.98%) | 24 (10.96%) | 43 (9.40%) | |
| >250 | 31 (13.02%) | 68 (31.05%) | 99 (21.66%) | |
| Total | 238 (100%) | 219 (100%) | 457 (100%) | |
| BC cases/year/doctor | ||||
| <100 | 151 (63.44%) | 94 (41.96%) | 245 (53.03%) | p = 0.001 |
| 100–149 | 42 (17.65%) | 48 (21.42%) | 90 (19.48%) | |
| 150–199 | 15 (6.30%) | 13 (5.80%) | 28 (6.06%) | |
| 200–249 | 12 (5.05%) | 14 (6.25%) | 26 (5.63%) | |
| >250 | 18 (7.56%) | 38 (16.96%) | 56 (12.12%) | |
| NSNC | 0 (0%) | 17 (7.58%) | 17 (3.68%) | |
| Total | 238 (100%) | 224 (100%) | 462 (100%) | |
| % of use of the SDM | ||||
| <33% | 49 (20.85%) | 19 (8.72%) | 68 (15.01%) | p = 0.001 |
| 33–66% | 53 (22.55%) | 28 (12.84%) | 81 (17.88%) | |
| >66% | 67 (28.51%) | 149 (68.35%) | 216 (47.69%) | |
| N/A | 66 (28.09%) | 22 (10.09%) | 88 (19.42%) | |
| Total | 235 (100%) | 218 (100%) | 453 (100%) |
| Survey Questions | Mean (CI 95%) | Argentina | Spain | p-Value | |
|---|---|---|---|---|---|
| 1 | I am familiar with the concept and rationale of Shared Decision Making (SDM) | 4.43 (4.36–4.50) | 4.51 (4.42–4.60) | 4.33 (4.22–4.45) | p = 0.027 |
| 2 | The SDM is a necessary survey to provide quality assistance. | 4.48 (4.42–4.55) | 4.45 (4.36–4.54) | 4.51 (4.42–4.61) | p = 0.289 |
| 3 | The importance of SDM increases when there are several treatment options with similar outcomes, where the selection of one or another option depends on the patient’s preferences. | 4.44 (4.37–4.50) | 4.43 (4.34–4.52) | 4.44 (4.35–4.54) | p = 0.741 |
| 4 | All physicians should ask their patients exactly how they would like to participate in decision-making. | 4.29 (4.22–4.36) | 4.32 (4.22–4.41) | 4.26 (4.16–4.36) | p = 0.429 |
| 5 | SDM increases patient satisfaction, improves cost-effectiveness and reduces malpractice claims. | 4.35 (4.28–4.41) | 4.34 (4.25–4.27) | 4.36 (4.23–4.44) | p = 0.708 |
| 6 | SDM is a basic element in the physician’s relationship with breast cancer (BC) patients. | 4.58 (4.51–4.64) | 4.79 (4.72–4.85) | 4.33 (4.23–4.44) | p = 0.001 |
| 7 | All doctors should inform their patients about the different treatment options available for their health problem. | 4.61 (4.55–4.67) | 4.57 (4.48–4.67) | 4.66 (4.58–4.73) | p = 0.211 |
| 8 | All doctors should explain all treatment options to their patients, including the possibility of not providing any treatment at all. | 4.62 (4.56–4.69) | 4.79 (4.71–4.84) | 4.44 (4.32–4.55) | p = 0.001 |
| 9 | All doctors should explain to their patients the benefits, risks and side effects of possible treatments. | 4.72 (4.67–4.78) | 4.77 (4.71–4.83) | 4.67 (4.58–4.75) | p = 0.036 |
| 10 | All doctors should help their patients understand all the information provided to them. | 4.52 (4.46–4.59) | 4.35 (4.25–4.44) | 4.73 (4.66–4.80) | p = 0.001 |
| 11 | All doctors should ask their patients which treatment option they prefer. | 4.32 (4.25–4.38) | 4.19 (4.11–4.27) | 4.46 (4.37–4.55) | p = 0.001 |
| 12 | Most patients feel that the doctor is the best person to decide on the best treatment option. | 4.38 (4.31–4.44) | 4.57 (4.49–4.65) | 4.15 (4.07–4.24) | p = 0.001 |
| 13 | All doctors should give their patients enough time to assess the different treatment options. | 4.38 (4.32–4.45) | 4.25 (4.14–4.36) | 4.54 (4.46–4.62) | p = 0.001 |
| 14 | All doctors should choose the treatment option together with their patients. | 4.29 (4.21–4.37) | 4.35 (4.24–4.45) | 4.22 (4.11–4.34) | p = 0.135 |
| 15 | All doctors should agree with their patients to monitor their process. | 3.80 (3.71–3.89) | 3.64 (3.53–3.80) | 3.98 (3.84–4.11) | p = 0.001 |
| 16 | My Unit has experience in the use of SDM in breast cancer. | 3.80 (3.71–3.88) | 3.65 (3.54–3.76) | 3.97 (3.85–4.09) | p = 0.001 |
| 17 | My Unit has a specific consultation to explain treatment options and facilitate SDM. | 3.34 (3.24–3.44) | 3.41 (3.29–3.53) | 3.26 (3.10–3.42) | p = 0.179 |
| 18 | My Unit has the necessary time to practice the practice of MDS in the care of the BC | 3.45 (3.35–3.55) | 3.63 (3.50–3.76) | 3.24 (3.09–3.40) | p = 0.001 |
| 19 | My Unit has the necessary materials to practice the SDM in the BC | 3.46 (3.37–3.55) | 3.61 (3.49–3.72) | 3.29 (3.15–3.43) | p = 0.001 |
| 20 | My hospital should promote more patient communication and the BC | 3.96 (3.88–4.04) | 3.98 (3.87–4.08) | 3.93 (3.82–4.05) | p = 0.799 |
| 21 | In general, there should be more training on patient communication and BC | 4.33 (4.27–4.40) | 4.41 (4.33–4.48) | 4.25 (4.15–4.35) | p = 0.023 |
| 22 | SDM can be useful for private health care, but it has no application in public health care, the patient cannot decide on the most efficient treatment option. | 2.10 (2.00–2.20) | 2.49 (2.34–2.64) | 1.65 (1.53–1.76) | p = 0.001 |
| 23 | In the future, there will be an increasing application of SDM in BC care. | 4.33 (4.27–4.40) | 4.34 (4.25–4.42) | 4.33 (4.23–4.43) | p = 0.910 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maes-Carballo, M.; Martín-Díaz, M.; Mignini, L.; Khan, K.S.; Trigueros, R.; Bueno-Cavanillas, A. Evaluation of the Use of Shared Decision Making in Breast Cancer: International Survey. Int. J. Environ. Res. Public Health 2021, 18, 2128. https://doi.org/10.3390/ijerph18042128
Maes-Carballo M, Martín-Díaz M, Mignini L, Khan KS, Trigueros R, Bueno-Cavanillas A. Evaluation of the Use of Shared Decision Making in Breast Cancer: International Survey. International Journal of Environmental Research and Public Health. 2021; 18(4):2128. https://doi.org/10.3390/ijerph18042128
Chicago/Turabian StyleMaes-Carballo, Marta, Manuel Martín-Díaz, Luciano Mignini, Khalid Saeed Khan, Rubén Trigueros, and Aurora Bueno-Cavanillas. 2021. "Evaluation of the Use of Shared Decision Making in Breast Cancer: International Survey" International Journal of Environmental Research and Public Health 18, no. 4: 2128. https://doi.org/10.3390/ijerph18042128