
Supporting Medical Staff from Psycho-Oncology with Smart Mobile Devices: Insights into the Development Process and First Results

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Related Work in mHealth and Psycho-Oncology
2.1. Related Work in the Context of Mobile Data Collection and mHealth Applications
2.2. Related Work in the Context of Psycho-Oncology
3. Requirements for Developing a Psycho-Oncological Platform
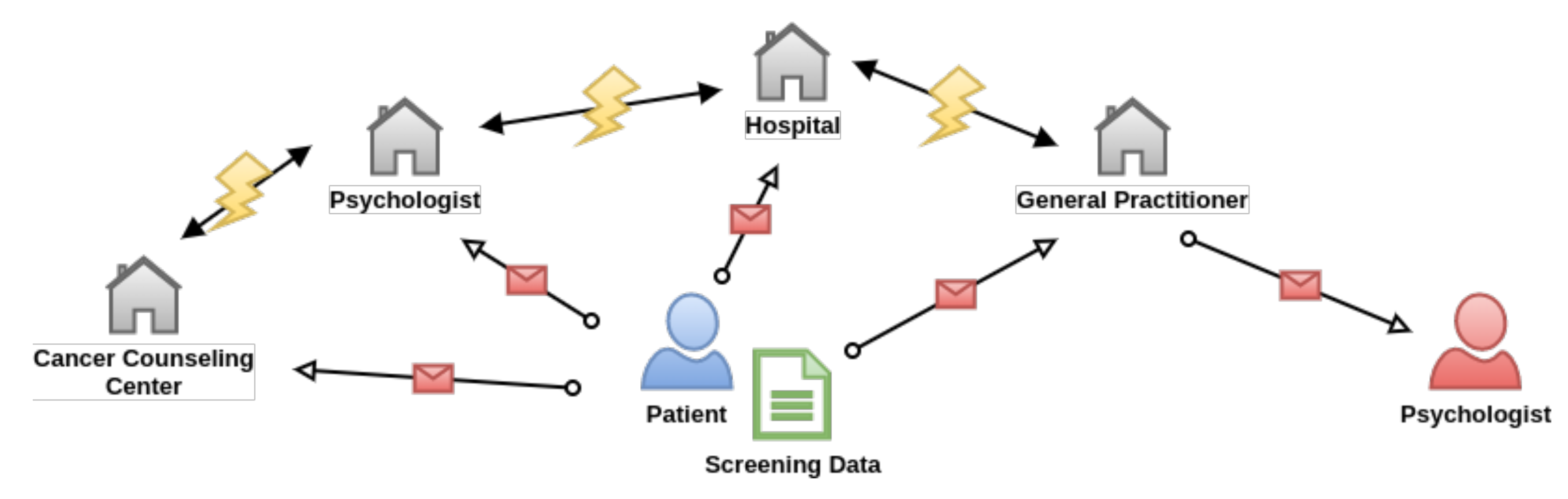
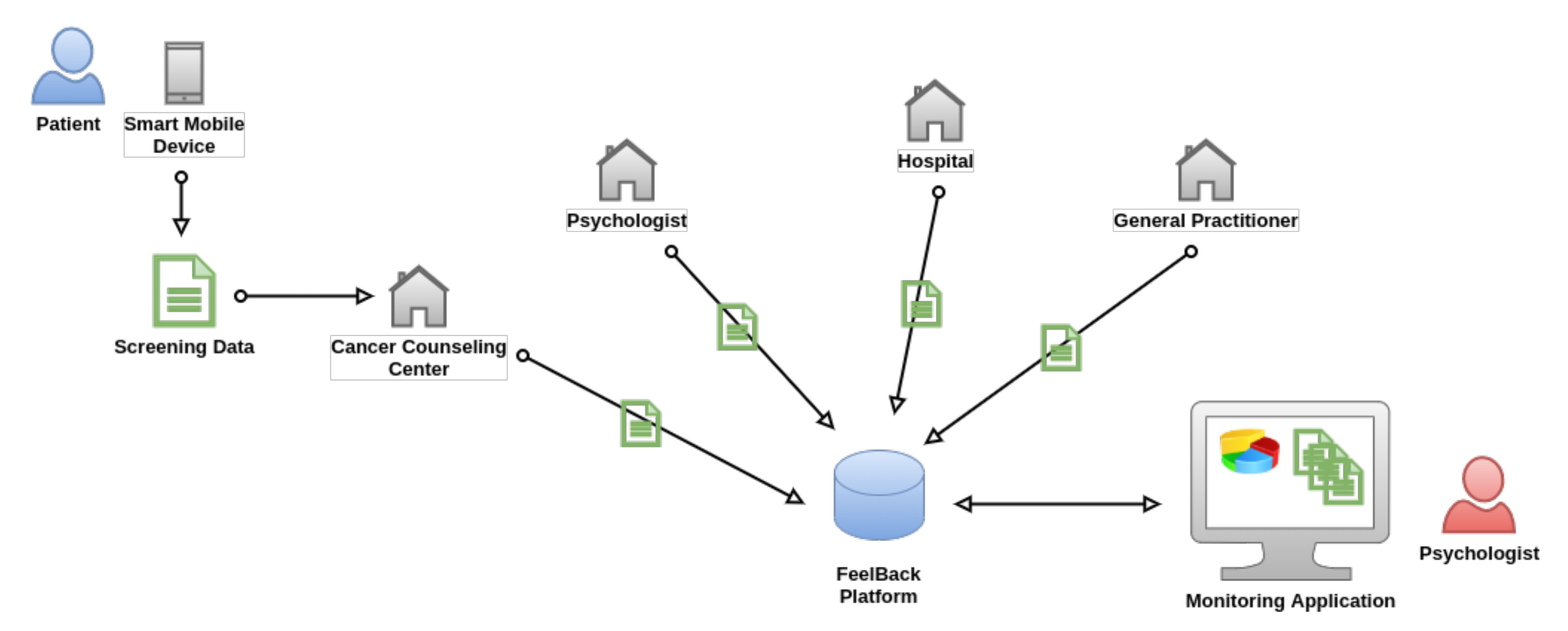
3.1. Application Scenario
3.2. Requirements for the FeelBack Platform
- Req-01 (Various Screening Instruments): an extendable framework should allow to add other well-established screening instruments (i.e., Hornheider Screening Instrument) at a later stage to deal with new requirements of caregivers.
- Req-02 (Mobile Data Collection): data should be collected in a digital manner by relying on smart mobile devices (i.e., smartphones or tablets). For this purpose, a mobile application has to be developed that is capable of visualizing respective instruments and storing collected data.
- Req-03 (Adaptive User-Interface): because the majority of the patients are elderly, a very simplistic user-interface has to be designed for the mobile application to not overburden the patients and streamline data input process.
- Req-04 (Passwordless Login): another login mechanism has to be provided, as most of the users do not have an e-mail address or may not want to share this information in the platform. Best-case, patients do not need to remember their own credentials (i.e., username and password).
- Req-05 (Automatic Evaluation): submitted screening instruments should be automatically evaluated based on given rules (i.e., cut-off values). The results should be displayed to assigned caregivers, which may use this information in psychological counselings.
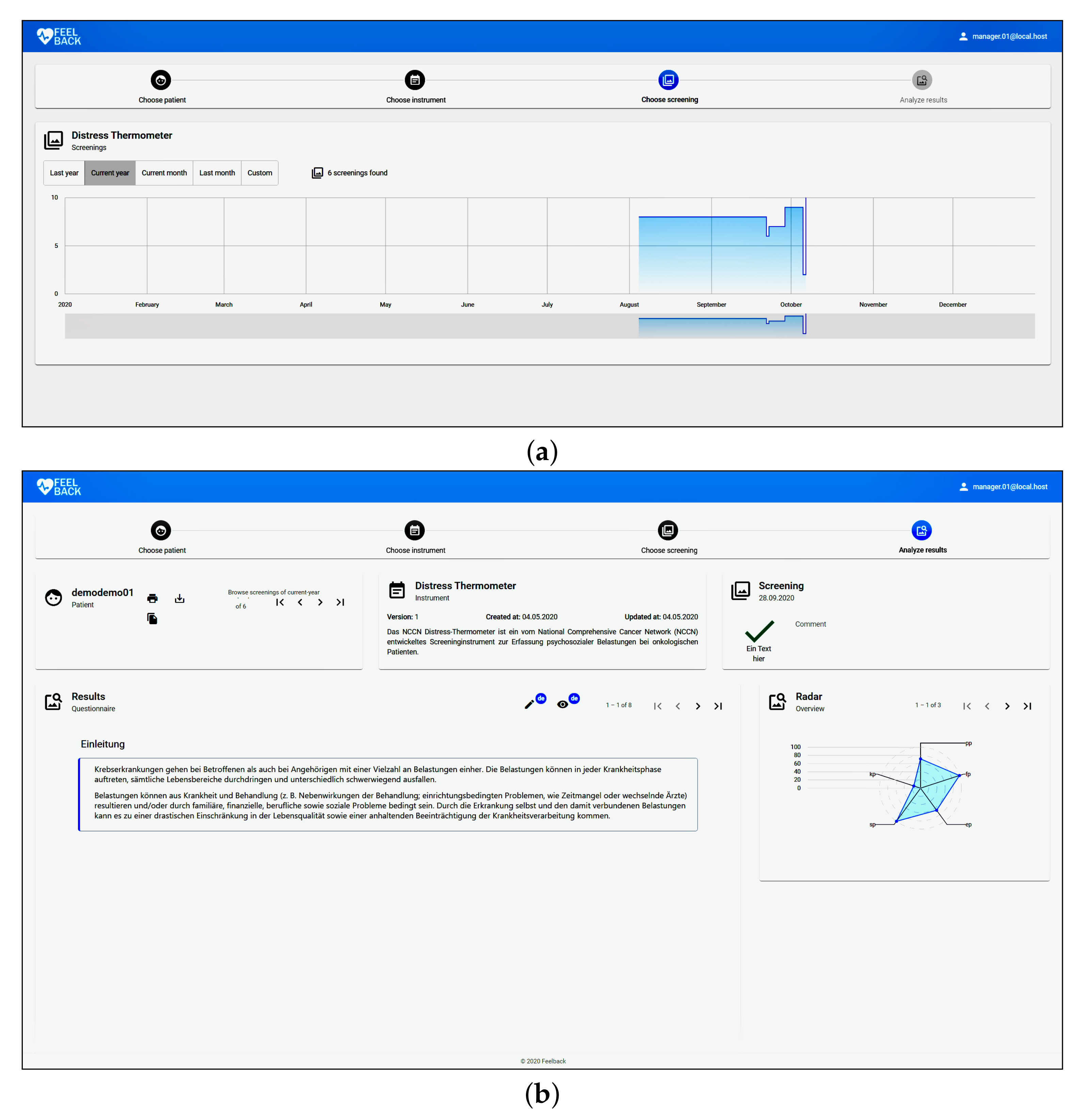
- Req-06 (Visualize Results): the collected data should be visualized according pre-defined rules. This should help the caregivers to obtain an immediate overview of a patient. More specifically, the original data of a particular filled in screening instrument should be accessible by caregivers.
- Req-07 (Patient History): when using the application for a longer period (i.e., several months and ongoing), caregivers should be able to see the history of the patient. This history should visualize the self-assessed distress over selected period as line-charts.
- Req-08 (Data Export): it should be possible to export data collected in a an electronic data exchange format (i.e., HL7 FHIR compliant resources). This should allow for attaching the history to an electronic health record stored within a hospital information system (HIS).
- Req-09 (Split Patient and Medical Data): for security reasons, patient data (i.e., name or address) should not be stored in the same database as medical data (i.e., screening data). This should prevent leaking sensitive information. Data are only aggregated via the backend API, which should be secured via state-of-the-art techniques.
- Req-10 (Patient Empowerment): patients should be empowered to control the flow of their own data. For example, patients shall give access or revoke access to their data.
4. Methods
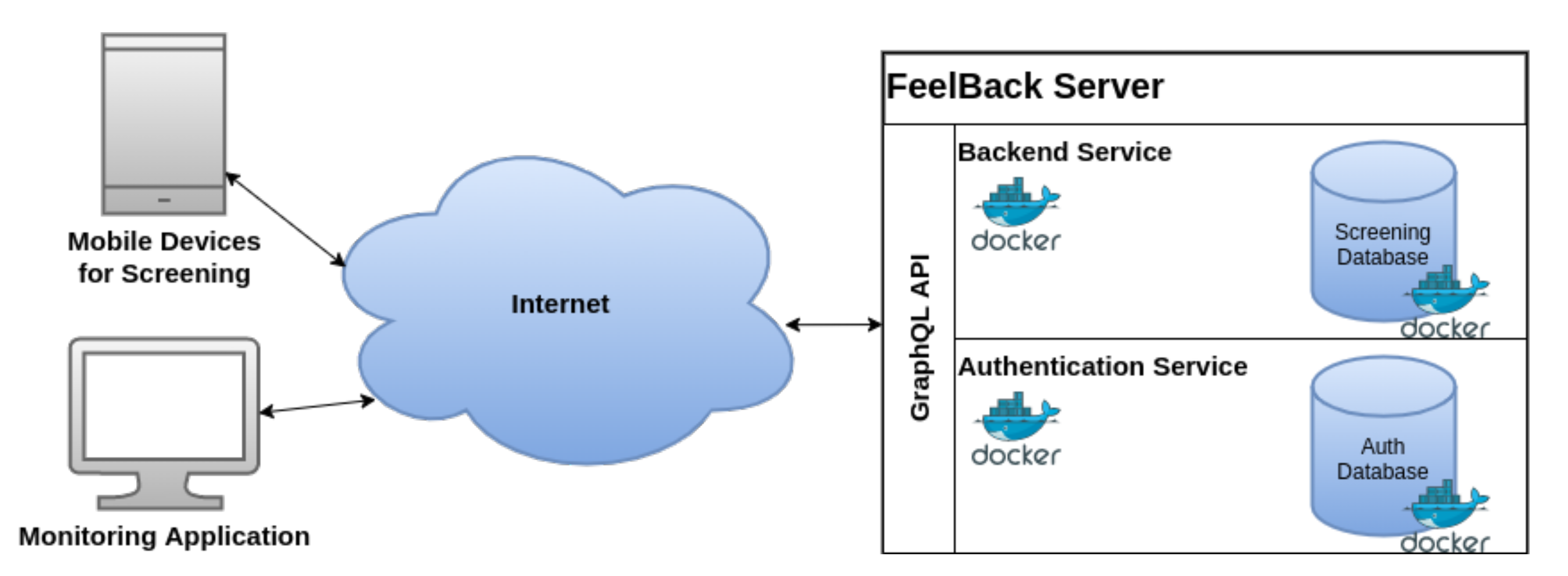
4.1. FeelBack Software Architecture
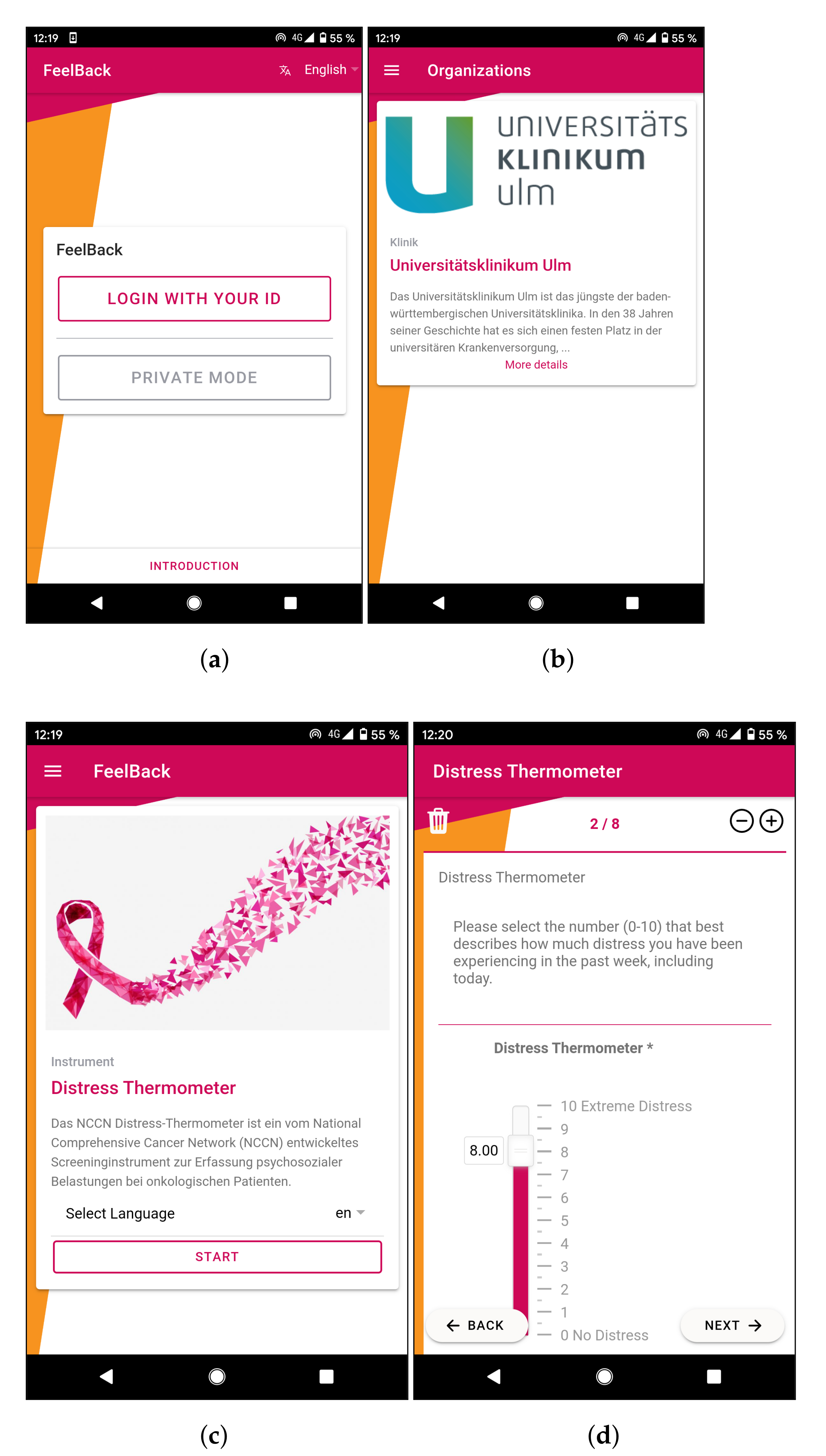
4.2. Technical Implementation of the FeelBack Application
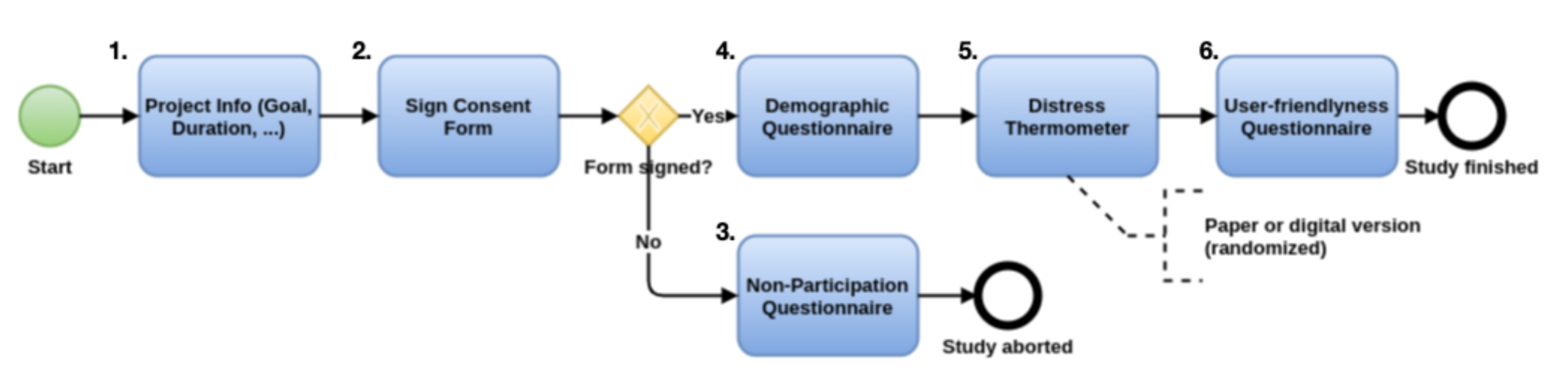
4.3. Evaluation of the Pilot Feasibility Study
4.4. Participants for the FeelBack Pilot Feasibility Study
4.5. Statistics
4.6. Data Availability
5. Results
5.1. Baseline Comparison
5.2. Results for Research Questions
5.2.1. Do Participants Accept Screening Instruments in Psycho-Oncology?
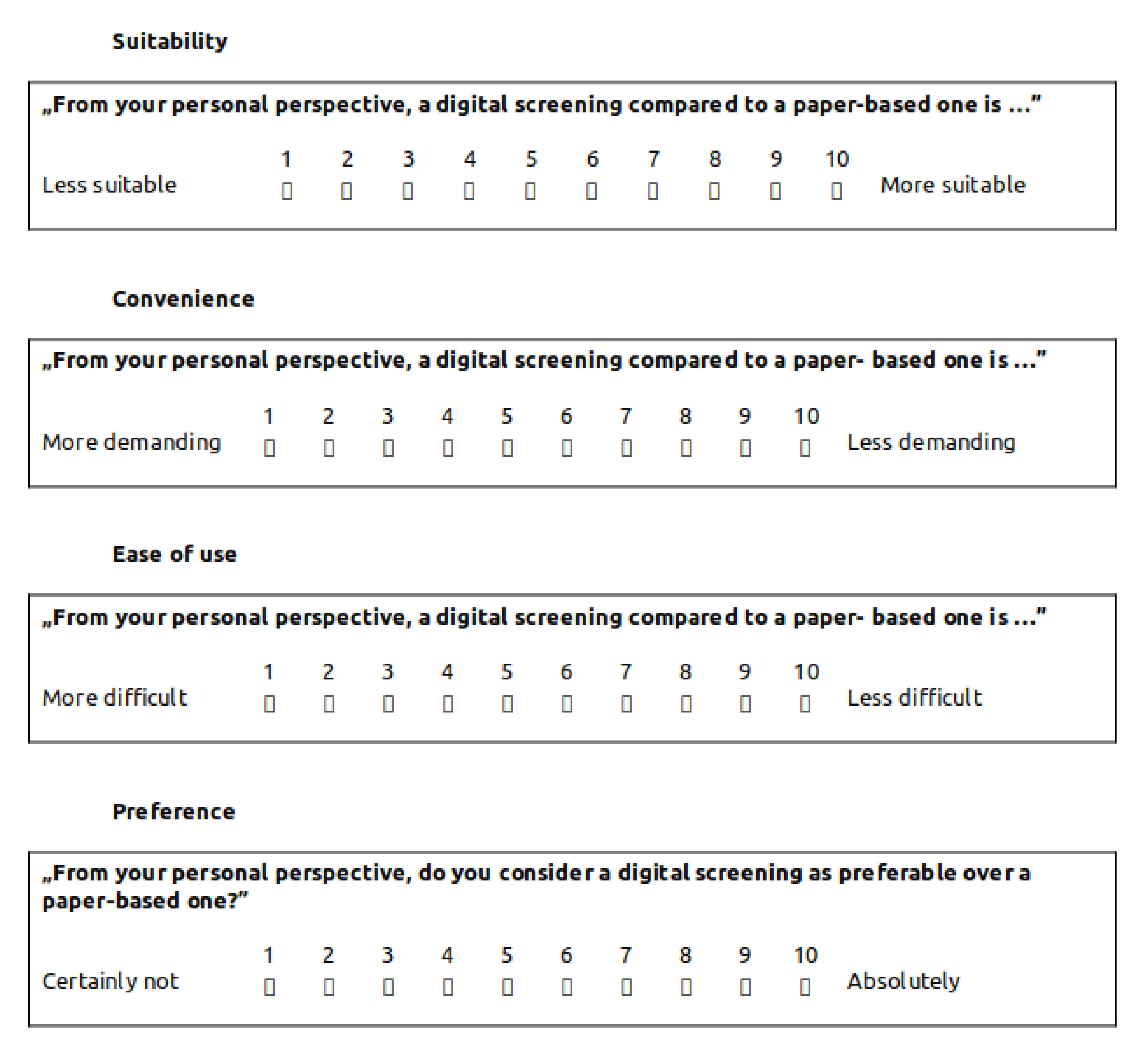
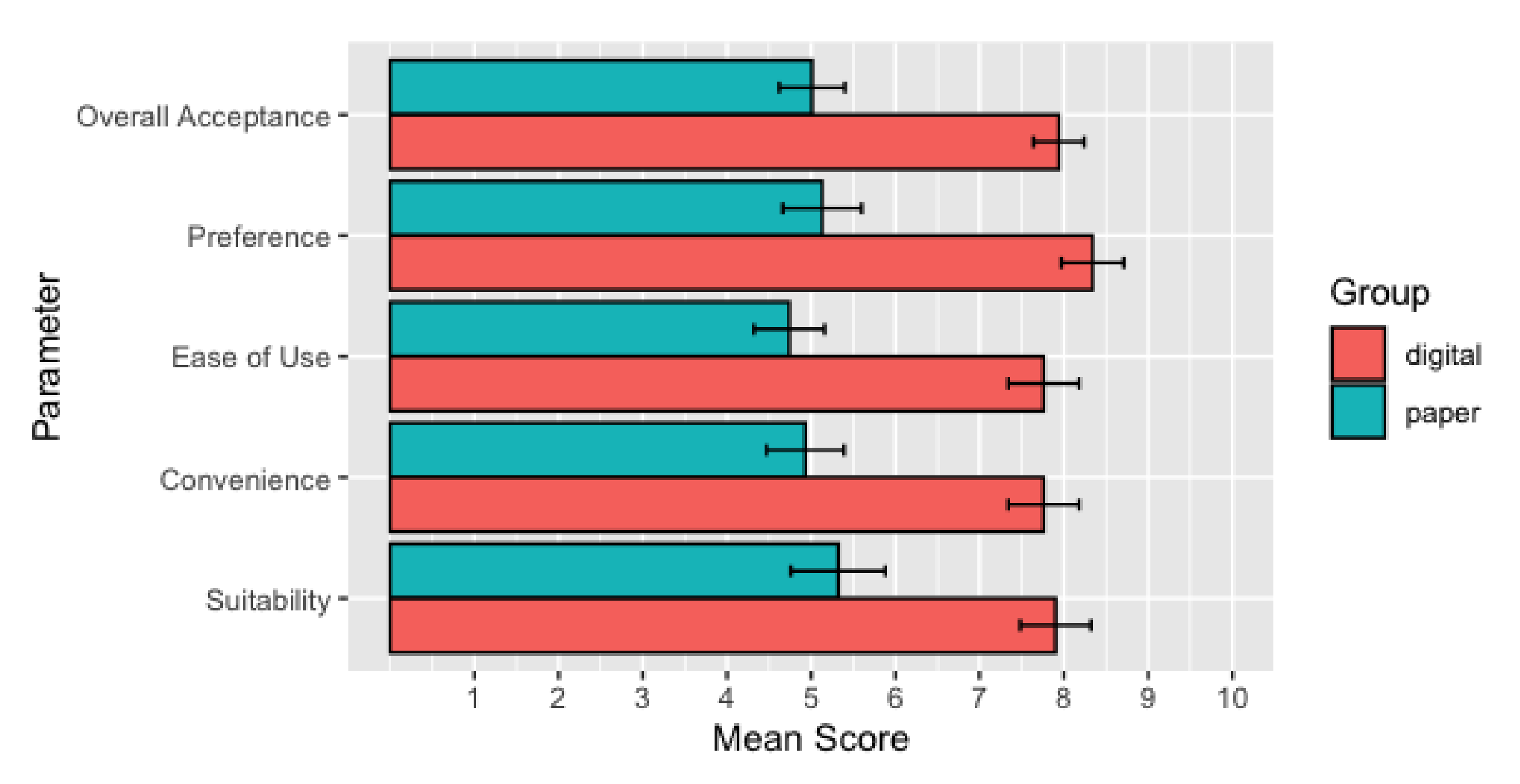
5.2.2. Are There Any Differences with Respect to the Acceptance of Instruments between the Groups Using the Digital versus the Paper-Based One?
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| JSON | JavaScript Object Notation |
| JWT | JSON Web Tokens |
| M | Mean |
| QL | Query Language |
| QR | Quick Response |
| Req | Requirement |
| RQ | Research Question |
| SD | Standard Deviation |
References
- LeBlanc, V.R.; Regehr, C.; Tavares, W.; Scott, A.K.; MacDonald, R.; King, K. The Impact of Stress on Paramedic Performance During Simulated Critical Events. Prehospital Disaster Med. 2012, 27, 369–374. [Google Scholar] [PubMed]
- Calman, K.C. Quality of life in cancer patients—An hypothesis. J. Med. Ethics 1984, 10, 124–127. [Google Scholar] [PubMed] [Green Version]
- Karabulutlu, E.Y. Coping with stress of family caregivers of cancer patients in Turkey. Asia Pac. J. Oncol. Nurs. 2014, 1, 55–60. [Google Scholar]
- Dai, S.; Mo, Y.; Wang, Y.; Xiang, B.; Liao, Q.; Zhou, M.; Li, X.; Li, Y.; Xiong, W.; Li, G.; et al. Chronic Stress Promotes Cancer Development. Front. Oncol. 2020, 10, 1492. [Google Scholar] [PubMed]
- Kiecolt-Glaser, J.; Robles, T.; Heffner, K.; Loving, T.; Glaser, R. Psycho-oncology and cancer: Psychoneuroimmunology and cancer. Ann. Oncol. 2002, 13, 165–169. [Google Scholar]
- McGregor, B.A.; Antoni, M.H. Psychological intervention and health outcomes among women treated for breast cancer: A review of stress pathways and biological mediators. Brain Behav. Immun. 2009, 23, 159–166. [Google Scholar] [PubMed] [Green Version]
- Sperner-Unterweger, B. Psychoonkologie—Psychosoziale Onkologie. Der Nervenarzt 2010, 82, 371–381. [Google Scholar]
- Holland, J.C. History of psycho-oncology: Overcoming attitudinal and conceptual barriers. Psychosom. Med. 2002, 64, 206–221. [Google Scholar]
- Hühne, R.; Kessler, V.; Fürstberger, A.; Kühlwein, S.; Platzer, M.; Sühnel, J.; Lausser, L.; Kestler, H.A. 3D Network exploration and visualisation for lifespan data. BMC Bioinform. 2018, 19, 390. [Google Scholar]
- Song, Z.; Von Figura, G.; Liu, Y.; Kraus, J.M.; Torrice, C.; Dillon, P.; Rudolph-Watabe, M.; Ju, Z.; Kestler, H.A.; Sanoff, H.; et al. Lifestyle impacts on the aging-associated expression of biomarkers of DNA damage and telomere dysfunction in human blood. Aging Cell 2010, 9, 607–615. [Google Scholar]
- Fernandez-Ballesteros, R. Self-Report Questionnaires. In Comprehensive Handbook of Psychological Assessment; Hersen, M., Haynes, S.N., Heiby, E.M., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 3, pp. 194–221. [Google Scholar]
- Wicksell, R.K.; Lekander, M.; Sorjonen, K.; Olsson, G.L. The Psychological Inflexibility in Pain Scale (PIPS)–statistical properties and model fit of an instrument to assess change processes in pain related disability. Eur. J. Pain 2010, 14, 771.e1–771.e14. [Google Scholar]
- Thiam, P.; Bellmann, P.; Kestler, H.A.; Schwenker, F. Exploring Deep Physiological Models for Nociceptive Pain Recognition. Sensors 2019, 19, 4503. [Google Scholar] [CrossRef] [Green Version]
- Thiam, P.; Kestler, H.A.; Schwenker, F. Two-Stream Attention Network for Pain Recognition from Video Sequences. Sensors 2020, 20, 839. [Google Scholar] [CrossRef] [Green Version]
- Ullah, P. The association between income, financial strain and psychological well-being among unemployed youths. J. Occup. Psychol. 1990, 63, 317–330. [Google Scholar]
- Sumnitsch, P.; Hartmann, B.; Zanolin, D.; Saely, C.; Lang, A. Screening in der Psychoonkologie. ProCare 2017, 22, 7–14. [Google Scholar]
- Fayers, P.; Bottomley, A.; on behalf of the EORTC Quality of Life Group; of the Quality of Life Unit. Quality of life research within the EORTC—The EORTC QLQ-C30. Eur. J. Cancer 2002, 38, 125–133. [Google Scholar]
- Pavlović, I.; Kern, T.; Miklavčič, D. Comparison of Paper-Based and Electronic Data Collection Process in Clinical Trials: Costs Simulation Study. Contemp. Clin. Trials 2009, 30, 300–316. [Google Scholar]
- Kraus, J.M.; Lausser, L.; Kuhn, P.; Jobst, F.; Bock, M.; Halanke, C.; Hummel, M.; Heuschmann, P.; Kestler, H.A. Big data and precision medicine: Challenges and strategies with healthcare data. Int. J. Data Sci. Anal. 2018, 6, 241–249. [Google Scholar]
- Palermo, T.M.; Valenzuela, D.; Stork, P.P. A Randomized Trial of Electronic versus Paper Pain Diaries in Children: Impact on Compliance, Accuracy, and Acceptability. Pain 2004, 107, 213–219. [Google Scholar] [PubMed]
- Lane, S.J.; Heddle, N.M.; Arnold, E.; Walker, I. A Review of Randomized Controlled Trials Comparing the Effectiveness of Hand Held Computers with Paper Methods for Data Collection. BMC Med. Inf. Decis. Mak. 2006, 6, 23. [Google Scholar]
- Carlbring, P.; Brunt, S.; Bohman, S.; Austin, D.; Richards, J.; Öst, L.G.; Andersson, G. Internet vs. Paper and Pencil Administration of Questionnaires Commonly Used in Panic/Agoraphobia Research. Comput. Hum. Behav. 2007, 23, 1421–1434. [Google Scholar]
- Jacobsen, P.B.; Donovan, K.A.; Trask, P.C.; Fleishman, S.B.; Zabora, J.; Baker, F.; Holland, J.C. Screening for psychologic distress in ambulatory cancer patients. Cancer 2005, 103, 1494–1502. [Google Scholar]
- Tuinman, M.A.; Gazendam-Donofrio, S.M.; Hoekstra-Weebers, J.E. Screening and referral for psychosocial distress in oncologic practice: Use of the Distress Thermometer. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2008, 113, 870–878. [Google Scholar]
- Mehnert, A.; Müller, D.; Lehmann, C.; Koch, U. Die Deutsche Version des NCCN Distress-Thermometers: Empirische Prüfung eines Screening-Instruments zur Erfassung Psychosozialer Belastung bei Krebspatienten. Z. Psychiatr. Psychol. Psychother. 2006, 54, 213–223. [Google Scholar]
- Luxton, D.D.; McCann, R.A.; Bush, N.E.; Mishkind, M.C.; Reger, G.M. mHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof. Psychol. Res. Pract. 2011, 42, 505–512. [Google Scholar]
- Morilla, M.D.R.; Sans, M.; Casasa, A.; Giménez, N. Implementing technology in healthcare: Insights from physicians. BMC Med. Inf. Decis. Mak. 2017, 17, 92. [Google Scholar]
- Jacob, C.; Sanchez-Vazquez, A.; Ivory, C. Factors Impacting Clinicians’ Adoption of a Clinical Photo Documentation App and its Implications for Clinical Workflows and Quality of Care: Qualitative Case Study. JMIR mHealth uHealth 2020, 8, e20203. [Google Scholar] [PubMed]
- Shaballout, N.; Aloumar, A.; Neubert, T.A.; Dusch, M.; Beissner, F. Digital Pain Drawings Can Improve Doctors’ Understanding of Acute Pain Patients: Survey and Pain Drawing Analysis. JMIR mHealth uHealth 2019, 7, e11412. [Google Scholar] [PubMed]
- Krebs, P.; Burkhalter, J.; Fiske, J.; Snow, H.; Schofield, E.; Iocolano, M.; Borderud, S.; Ostroff, J.S. The QuitIT Coping Skills Game for Promoting Tobacco Cessation Among Smokers Diagnosed With Cancer: Pilot Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e10071. [Google Scholar] [PubMed] [Green Version]
- Schlee, W.; Pryss, R.C.; Probst, T.; Schobel, J.; Bachmeier, A.; Reichert, M.; Langguth, B. Measuring the moment-to-moment variability of tinnitus: The TrackYourTinnitus smart phone app. Front. Aging Neurosci. 2016, 8, 294. [Google Scholar] [PubMed] [Green Version]
- Pryss, R.; Probst, T.; Schlee, W.; Schobel, J.; Langguth, B.; Neff, P.; Spiliopoulou, M.; Reichert, M. Prospective crowdsensing versus retrospective ratings of tinnitus variability and tinnitus–stress associations based on the TrackYourTinnitus mobile platform. Int. J. Data Sci. Anal. 2019, 8, 327–338. [Google Scholar]
- Weinrib, A.; Azam, M.A.; Latman, V.V.; Janmohamed, T.; Clarke, H.; Katz, J. Manage My Pain: A patient-driven mobile platform to prevent and manage chronic postsurgical pain. In Novel Applications of Virtual Communities in Healthcare Settings; IGI Global: Hershey, PA, USA, 2018; pp. 93–126. [Google Scholar]
- Gaggioli, A.; Pioggia, G.; Tartarisco, G.; Baldus, G.; Corda, D.; Cipresso, P.; Riva, G. A mobile data collection platform for mental health research. Pers. Ubiquitous Comput. 2013, 17, 241–251. [Google Scholar]
- Ben-Zeev, D.; Schueller, S.M.; Begale, M.; Duffecy, J.; Kane, J.M.; Mohr, D.C. Strategies for mHealth research: Lessons from 3 mobile intervention studies. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 157–167. [Google Scholar]
- Schobel, J. A Model-Driven Framework for Enabling Flexible and Robust Mobile Data Collection Applications. Ph.D. Thesis, Ulm University, Ulm, Germany, 2018. [Google Scholar]
- Schobel, J.; Pryss, R.; Schickler, M.; Reichert, M. A Lightweight Process Engine for Enabling Advanced Mobile Applications. In Proceedings of the On the Move to Meaningful Internet Systems: OTM 2016 Conferences, Rhodes, Greece, 24–28 October 2016; Debruyne, C., Panetto, H., Meersman, R., Dillon, T., Kühn, E., O’Sullivan, D., Ardagna, C.A., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 552–569. [Google Scholar]
- Schobel, J.; Pryss, R.; Wipp, W.; Schickler, M.; Reichert, M. A Mobile Service Engine Enabling Complex Data Collection Applications. In Proceedings of the Service-Oriented Computing, Banff, AB, Canada, 10–13 October 2016; Sheng, Q.Z., Stroulia, E., Tata, S., Bhiri, S., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 626–633. [Google Scholar]
- Schobel, J.; Pryss, R.; Probst, T.; Schlee, W.; Schickler, M.; Reichert, M. Learnability of a Configurator Empowering End Users to Create Mobile Data Collection Instruments: Usability Study. JMIR mHealth uHealth 2018, 6, e148. [Google Scholar] [PubMed] [Green Version]
- Schobel, J.; Probst, T.; Reichert, M.; Schlee, W.; Schickler, M.; Kestler, H.A.; Pryss, R. Measuring mental effort for creating mobile data collection applications. Int. J. Environ. Res. Public Health 2020, 17, 1649. [Google Scholar] [CrossRef] [Green Version]
- Guo, B.; Wang, Z.; Yu, Z.; Wang, Y.; Yen, N.Y.; Huang, R.; Zhou, X. Mobile crowd sensing and computing: The review of an emerging human-powered sensing paradigm. ACM Comput. Surv. CSUR 2015, 48, 1–31. [Google Scholar]
- Liu, J.; Shen, H.; Narman, H.S.; Chung, W.; Lin, Z. A survey of mobile crowdsensing techniques: A critical component for the internet of things. ACM Trans. Cyber Phys. Syst. 2018, 2, 1–26. [Google Scholar]
- Shu, L.; Chen, Y.; Huo, Z.; Bergmann, N.; Wang, L. When mobile crowd sensing meets traditional industry. IEEE Access 2017, 5, 15300–15307. [Google Scholar]
- Seifert, A.; Hofer, M.; Allemand, M. Mobile data collection: Smart, but not (yet) smart enough. Front. Neurosci. 2018, 12, 971. [Google Scholar] [CrossRef]
- Wangler, J.; Jansky, M. The use of health apps in primary care—Results from a survey amongst general practitioners in Germany. Wien. Med. Wochenschr. 2021, 171, 148–156. [Google Scholar]
- El Kefi, S.; Asan, O. How technology impacts communication between cancer patients and their health care providers: A systematic literature review. Int. J. Med. Inf. 2021, 149, 104430. [Google Scholar] [CrossRef]
- Wicks, P.; Chiauzzi, E. ‘Trust but verify’—Five approaches to ensure safe medical apps. BMC Med. 2015, 13, 1–5. [Google Scholar]
- Zhou, L.; Bao, J.; Watzlaf, V.; Parmanto, B. Barriers to and facilitators of the use of mobile health apps from a security perspective: Mixed-methods study. JMIR mHealth and uHealth 2019, 7, e11223. [Google Scholar] [PubMed]
- Llorens-Vernet, P.; Miró, J. Standards for Mobile Health–Related Apps: Systematic Review and Development of a Guide. JMIR Mhealth Uhealth 2020, 8, e13057. [Google Scholar] [CrossRef]
- Guo, C.; Ashrafian, H.; Ghafur, S.; Fontana, G.; Gardner, C.; Prime, M. Challenges for the evaluation of digital health solutions—A call for innovative evidence generation approaches. npj Digit. Med. 2020, 3, 110. [Google Scholar] [PubMed]
- Delgado, G.V.; de Carvalho, R.B.; Choo, C.W.; Leite, R.S.; de Castro, J.M. Patient empowerment through mobile health: Case study with a Brazilian application for pregnancy support. Proc. Assoc. Inf. Sci. Technol. 2020, 57, e221. [Google Scholar] [CrossRef]
- Schreiweis, B.; Pobiruchin, M.; Strotbaum, V.; Suleder, J.; Wiesner, M.; Bergh, B. Barriers and Facilitators to the Implementation of eHealth Services: Systematic Literature Analysis. J. Med. Internet Res. 2019, 21, e14197. [Google Scholar] [CrossRef] [Green Version]
- Ringwald, J.; Marwedel, L.; Junne, F.; Ziser, K.; Schäffeler, N.; Gerstner, L.; Wallwiener, M.; Brucker, S.Y.; Hautzinger, M.; Zipfel, S.; et al. Demands and Needs for Psycho-Oncological eHealth Interventions in Women With Cancer: Cross-Sectional Study. JMIR Cancer 2017, 3, e19. [Google Scholar] [CrossRef]
- Børøsund, E.; Mirkovic, J.; Clark, M.M.; Ehlers, S.L.; Andrykowski, M.A.; Bergland, A.; Westeng, M.; Solberg Nes, L. A Stress Management App Intervention for Cancer Survivors: Design, Development, and Usability Testing. JMIR Form. Res. 2018, 2, e19. [Google Scholar] [CrossRef]
- Koehler, M.; Hornemann, B.; Holzner, B.; Schäffeler, N.; Zimmermann, T.; Nest, A.; Wifling, K.; Herschbach, P. Zukunft jetzt—Implementierung eines IT-gestützten Distress-Screenings. Der Onkologe 2017, 23, 453–461. [Google Scholar]
- Pichler, T.; Haerdtner, M.; Pipia, I.; Kiechle, M.; Lackman, K.G.; Meier, V.; Troester, F.; Kokaras, G.; Nest, A.; Herschbach, P. Screen2Care-digital capture of psycho-oncological support needs. Der Onkologe 2020, 26, 66–72. [Google Scholar]
- Trautmann, F.; Hentschel, L.; Hornemann, B.; Rentsch, A.; Baumann, M.; Ehninger, G.; Schmitt, J.; Schuler, M. Electronic real-time assessment of patient-reported outcomes in routine care—First findings and experiences from the implementation in a comprehensive cancer center. Support. Care Cancer 2016, 24, 3047–3056. [Google Scholar]
- Christie, M.A.; Bhandar, A.; Nakandala, S.; Marru, S.; Abeysinghe, E.; Pamidighantam, S.; Pierce, M.E. Managing authentication and authorization in distributed science gateway middleware. Future Gener. Comput. Syst. 2020, 111, 780–785. [Google Scholar]
- Solapurkar, P. Building secure healthcare services using OAuth 2.0 and JSON web token in IOT cloud scenario. In Proceedings of the 2016 2nd International Conference on Contemporary Computing and Informatics (IC3I), Greater Noida, India, 14–17 December 2016; pp. 99–104. [Google Scholar]
- Mayer, G.; Müller, W.; Schork, K.; Uszkoreit, J.; Weidemann, A.; Wittig, U.; Rey, M.; Quast, C.; Felden, J.; Glöckner, F.O.; et al. Implementing FAIR data management within the German Network for Bioinformatics Infrastructure (de.NBI) exemplified by selected use cases. Brief. Bioinform. 2021, bbab010. [Google Scholar] [CrossRef]
- Schobel, J.; Schickler, M.; Pryss, R.; Nienhaus, H.; Reichert, M. Using Vital Sensors in Mobile Healthcare Business Applications: Challenges, Examples, Lessons Learned. In Proceedings of the 9th Int’l Conference on Web Information Systems and Technologies (WEBIST 2013), Special Session on Business Apps, Aachen, Germany, 8–10 May 2013; pp. 509–518. [Google Scholar]
- National Comprehensive Cancer Network. Distress management clinical practice guidelines. J. Natl. Compr. Cancer Netw. 2003, 1, 344–374. [Google Scholar]
- Schäffeler, N.; Pfeiffer, K.; Grischke, E.M.; Wallwiener, D.; Garbe, C.; Zipfel, S.; Teufel, M. Akzeptanz und Reliabilität eines elektronischen psychoonkologischen Screenings bei Patientinnen mit Brustkrebs: Eine randomisiert-kontrollierte Studie. Psychother. Psychosom. Med. Psychol. 2013, 63, 374–380. [Google Scholar] [PubMed]
- Wohlin, C.; Runeson, P.; Höst, M.; Ohlsson, M.C.; Regnell, B.; Wesslén, A. Experimentation in Software Engineering; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Giesler, J.; Weis, J.; Schreib, M.; Eichhorn, S.; Kuhnt, S.; Faust, T.; Mehnert, A.; Ernst, J. Ambulante psychoonkologische Versorgung durch Krebsberatungsstellen–Leistungsspektrum und Inanspruchnahme durch Patienten und Angehörige. Psychother. Psychosom. Med. Psychol. 2015, 65, 450–458. [Google Scholar]
- Bayer, O.; Billaudelle, F.; Alt, J.; Heß, G.; Specht, M.; Höfinghoff, B.; Riedel, P.; Wickert, M.; Hechtner, M.; Singer, S. Was Männer davon abhält, ambulante Krebsberatungsstellen aufzusuchen. Eine qualitative Studie. Der Onkologe 2020, 26, 1047–1055. [Google Scholar]
- Wilcox, R.R. Robust testing procedures. In Encyclopedia of Statistics in Behavioral Science; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2005. [Google Scholar]
- Fann, J.R.; Berry, D.L.; Wolpin, S.; Austin-Seymour, M.; Bush, N.; Halpenny, B.; Lober, W.B.; McCorkle, R. Depression screening using the Patient Health Questionnaire-9 administered on a touch screen computer. J. Psychol. Soc. Behav. Dimens. Cancer 2009, 18, 14–22. [Google Scholar]
- Wolpin, S.; Berry, D.; Austin-Seymour, M.; Bush, N.; Fann, J.R.; Halpenny, B.; Lober, W.; McCorkle, R. Acceptability of an electronic self report assessment program for patients with cancer. Comput. Inf. Nurs. 2008, 26, 332–338. [Google Scholar]
- Perry, S.; Kowalski, T.L.; Chang, C.H. Quality of life assessment in women with breast cancer: Benefits, acceptability and utilization. Health Qual. Life Outcomes 2007, 5, 24. [Google Scholar] [PubMed] [Green Version]
- Velikova, G.; Wright, E.; Smith, A.; Cull, A.; Gould, A.; Forman, D.; Perren, T.; Stead, M.; Brown, J.; Selby, P. Automated collection of quality-of-life data: A comparison of paper and computer touch-screen questionnaires. J. Clin. Oncol. 1999, 17, 998. [Google Scholar] [CrossRef] [PubMed]
- Kühl, S.J.; Schneider, A.; Kestler, H.A.; Toberer, M.; Kühl, M.; Fischer, M.R. Investigating the self-study phase of an inverted biochemistry classroom—Collaborative dyadic learning makes the difference. BMC Med. Educ. 2019, 19, 64. [Google Scholar] [CrossRef]
- Graf, J.; Simoes, E.; Wißlicen, K.; Rava, L.; Walter, C.; Hartkopf, A.; Keilmann, L.; Taran, A.; Wallwiener, S.; Fasching, P.; et al. Willingness of patients with breast cancer in the adjuvant and metastatic setting to use electronic surveys (ePRO) depends on sociodemographic factors, health-related quality of life, disease status and computer skills. Geburtshilfe und Frauenheilkd 2016, 76, 535–541. [Google Scholar] [CrossRef] [Green Version]
- Saied, A.; Sherry, S.J.; Castricone, D.J.; Perry, K.M.; Katz, S.C.; Somasundar, P. Age-related trends in utilization of the internet and electronic communication devices for coordination of cancer care in elderly patients. J. Geriatr. Oncol. 2014, 5, 185–189. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Paper-Based Screening () | Digital Screening () | p-Value |
|---|---|---|---|
| Advice Seeker, n (%) | a | ||
| Patient | 18 (58) | 17 (59) | |
| Relative | 13 (42) | 12 (41) | |
| Gender, n (%) | a | ||
| Female | 24 (77) | 21 (72) | |
| Male | 7 (23) | 8 (28) | |
| Migration Background, n (%) | a | ||
| No | 28 (90) | 25 (86) | |
| Yes | 3 (10) | 4 (14) | |
| Age (years), mean (SD) | 55.1 (12.2) | 51.0 (13.4) | b |
| Highest education, n (%) | a | ||
| Apprenticeship | 12 (39) | 13 (45) | |
| Professional School | 1 (3) | 4 (14) | |
| University | 13 (42) | 11 (38) | |
| Other | 5 (16) | 1 (3) | |
| Currently Employed, n (%) 1 | a | ||
| No | 12 (39) | 11 (38) | |
| Yes | 18 (58) | 17 (59) | |
| Distress value, mean (SD) | 6.6 (2.1) | 6.2 (2.2) | b |
| Parameter | Mean | SD |
|---|---|---|
| Suitability | ||
| Convenience | ||
| Ease of Use | ||
| Preference | ||
| Overall Acceptance |
| Variable | Groups | Statistics | p-Value a | Cohen’s d | |
|---|---|---|---|---|---|
| Paper-Based Screening () Digital Screening () | |||||
| Suitability | 5.32 (3.11) | 7.90 (2.27) | |||
| Convenience b | 4.93 (2.52) | 7.76 (2.28) | |||
| Ease of Use | 4.74 (2.34) | 7.76 (2.25) | |||
| Preference | 5.13 (2.60) | 8.34 (2.00) | |||
| Overall Acceptance | 5.01 (2.19) | 7.94 (1.61) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schobel, J.; Volz, M.; Hörner, K.; Kuhn, P.; Jobst, F.; Schwab, J.D.; Ikonomi, N.; Werle, S.D.; Fürstberger, A.; Hoenig, K.; et al. Supporting Medical Staff from Psycho-Oncology with Smart Mobile Devices: Insights into the Development Process and First Results. Int. J. Environ. Res. Public Health 2021, 18, 5092. https://doi.org/10.3390/ijerph18105092
Schobel J, Volz M, Hörner K, Kuhn P, Jobst F, Schwab JD, Ikonomi N, Werle SD, Fürstberger A, Hoenig K, et al. Supporting Medical Staff from Psycho-Oncology with Smart Mobile Devices: Insights into the Development Process and First Results. International Journal of Environmental Research and Public Health. 2021; 18(10):5092. https://doi.org/10.3390/ijerph18105092
Chicago/Turabian StyleSchobel, Johannes, Madeleine Volz, Katharina Hörner, Peter Kuhn, Franz Jobst, Julian D. Schwab, Nensi Ikonomi, Silke D. Werle, Axel Fürstberger, Klaus Hoenig, and et al. 2021. "Supporting Medical Staff from Psycho-Oncology with Smart Mobile Devices: Insights into the Development Process and First Results" International Journal of Environmental Research and Public Health 18, no. 10: 5092. https://doi.org/10.3390/ijerph18105092