
Association between Crystalline Silica Dust Exposure and Silicosis Development in Artificial Stone Workers

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
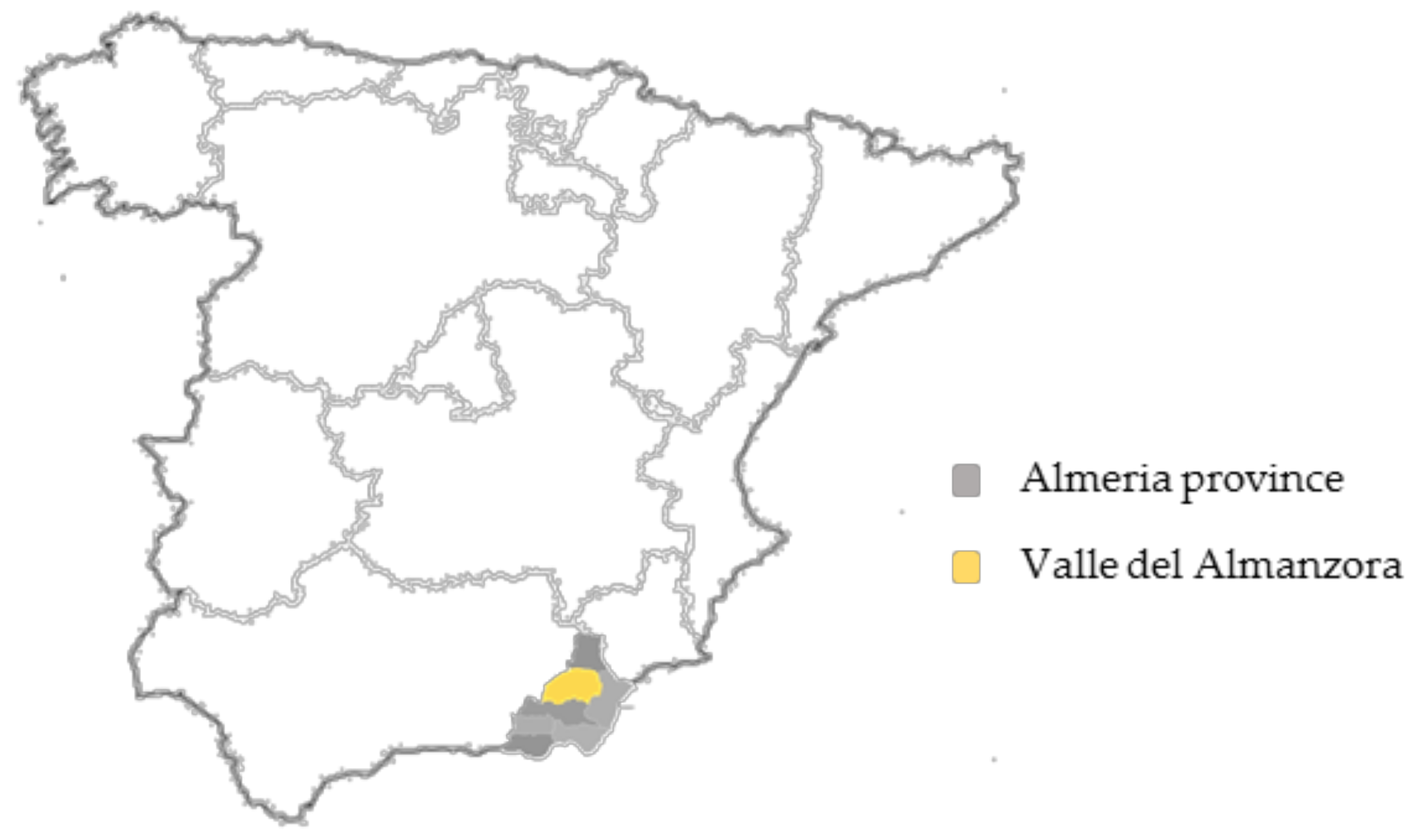
2.1. Study Design and Geographical Location
2.2. Study Population and Data Collection
2.3. Data Analysis
3. Results
4. Discussion
4.1. Cases of Silicosis and Respiratory Symptoms
4.2. Occupational Exposure Factors to Silica Dust
4.2.1. Exposure Time and Job Position
4.2.2. Smoking Habit
4.3. Use of Personal Protective Equipment (PPE)
4.4. Information and Training of Workers
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Occupational Safety and Health Administration, Department of Labor. Occupational exposure to respirable crystalline silica; final rule. Fed. Regist. 2016, 81, 16285–16890. [Google Scholar]
- Kauppinen, T.; Toikkanen, J.; Pedersen, D.; Young, R.; Ahrens, W.; Boffetta, P.; Hansen, J.; Kromhout, H.; Maqueda Blasco, J.; Mirabelli, D.; et al. Occupational exposure to carcinogens in the European Union. Occup. Environ. Med. 2000, 57, 10–18. [Google Scholar] [CrossRef]
- Henneberger, P.K.; Weissman, D.N. Old adversaries in new places. Occup. Environ. Med. 2018, 75, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Calvert, G.M.; Rice, F.L.; Boiano, J.M.; Sheehy, J.W.; Sanderson, W.T. Occupational silica exposure and risk of various diseases: An analysis using death certificates from 27 states of the United States. Occup. Environ. Med. 2003, 60, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Leung, C.C.; Yu, I.T.; Chen, W. Silicosis. Lancet 2012, 379, 2008–2018. [Google Scholar] [CrossRef]
- National Institute for Occupational Safety and Health. Health Effects of Occupational Exposure to Respirable Crystalline Silica. Available online: https://www.cdc.gov/niosh/docs/2002-129/default.html (accessed on 1 December 2020).
- Hedlund, U.; Jonsson, H.; Eriksson, K.; Järvholm, B. Exposure–response of silicosis mortality in Swedish iron ore miners. Ann. Occup. Hyg. 2008, 52, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossman, B.T.; Churg, A. Mechanisms in the pathogenesis of asbestosis and silicosis. Am. J. Respir. Crit. Care Med. 1998, 157, 1666–1680. [Google Scholar] [CrossRef] [Green Version]
- Lopes-Pacheco, M.; Bandeira, E.; Morales, M.M. Cell-Based Therapy for Silicosis. Stem. Cells Int. 2016, 2016, 5091838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoy, R.F.; Baird, T.; Hammerschlag, G.; Hart, D.; Johnson, A.R.; King, P.; Putt, M.; Yates, D.H. Artificial stone-associated silicosis: A rapidly emerging occupational lung disease. Occup. Environ. Med. 2018, 75, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ophir, N.; Shai, A.B.; Alkalay, Y.; Israeli, S.; Korenstein, R.; Kramer, M.R.; Fireman, E. Artificial stone dust-induced functional and inflammatory abnormalities in exposed workers monitored quantitatively by biometrics. ERJ Open Res. 2016, 2, 00086-2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, D.; Miller, B.G.; Soutar, C.A. Quantitative relations between exposure to respirable quartz and risk of silicosis. Occup. Environ. Med. 2003, 60, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.H.; Johnson, D.L.; Phillips, M.L. Respirable silica dust suppression during artificial stone countertop cutting. Ann. Occup. Hyg. 2015, 59, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Guarnieri, G.; Bizzotto, R.; Gottardo, O.; Velo, E.; Cassaro, M.; Vio, S.; Putzu, M.G.; Rossi, F.; Zuliani, P.; Liviero, F.; et al. Multiorgan accelerated silicosis misdiagnosed as sarcoidosis in two workers exposed to quartz conglomerate dust. Occup. Environ. Med. 2018, 2018, 105462–105476. [Google Scholar] [CrossRef]
- Kreuzer, M.; Sogl, M.; Brüske, I.; Möhner, M.; Nowak, D.; Schnelzer, M.; Walsh, L. Silica dust, radon and death from non-malignant respiratory diseases in German uranium miners. Occup. Environ. Med. 2013, 70, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, Y.; Wang, H.; Hnizdo, E.; Sun, Y.; Su, L.; Zhang, X.; Weng, S.; Bochmann, F.; Hearl, F.J.; et al. Long-term exposure to silica dust and risk of total and cause-specific mortality in Chinese workers: A cohort study. PLoS Med. 2012, 9, e1001206. [Google Scholar] [CrossRef] [PubMed]
- Vacek, P.M.; Verma, D.K.; Graham, W.G.; Callas, P.W.; Gibbs, G.W. Mortality in Vermont granite workers and its association with silica exposure. Occup. Environ. Med. 2011, 68, 312–318. [Google Scholar] [CrossRef] [Green Version]
- ‘t Mannetje, A.; Steenland, K.; Attfield, M.; Boffetta, P.; Checkoway, H.; DeKlerk, N.; Koskela, R.S. Exposure-response analysis and risk assessment for silica and silicosis mortality in a pooled analysis of six cohorts. Occup. Environ. Med. 2002, 59, 723–728. [Google Scholar] [CrossRef]
- Occupation Safety Health Administration. Worker Exposure to Silica during Countertop Manufacturing, Finishing and Installation. Available online: https://www.osha.gov/Publications/OSHA3768.pdf (accessed on 1 December 2020).
- García Vadillo, C.; Gómez, J.S.; Morillo, J.R. Silicosis in quartz conglomerate workers. Arch. Bronconeumol. 2011, 47, 53. [Google Scholar] [CrossRef]
- Martínez, C.; Prieto, A.; García, L.; Quero, A.; González, S.; Casan, P. Silicosis: A disease with an active present. Arch. Bronconeumol. 2010, 46, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, V.; Romeo, R.; Sisinni, A.G.; Bartoli, D.; Mazzei, M.A.; Sartorelli, P. Silicosis in Workers Exposed to Artificial Quartz Conglomerates: Does It Differ from Chronic Simple Silicosis? Arch. Bronconeumol. 2015, 51, e57–e60. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Alonso, A.; Córdoba-Doña, J.A.; García-Vadillo, C. Silicosis: Relevant differences between marble workers and miners. Arch. Bronconeumol. 2015, 51, 53–54. [Google Scholar] [CrossRef] [PubMed]
- Shtraichman, O.; Blanc, P.; Ollech, J.; Fridel, L.; Fuks, L.; Fireman, E.; Kramer, M. Outbreak of autoimmune disease in a silicosis linked to artificial stone. Occup. Med. 2015, 65, 444–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leso, V.; Fontana, L.; Romano, R.; Gervetti, P.; Iavicoli, I. Artificial Stone Associated Silicosis: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 568. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.R.; Blanc, P.D.; Fireman, E.; Amital, A.; Guber, A.; Rhahman, N.A.; Shitrit, D. Artificial Stone silicosis [corrected]: Disease resurgence among artificial Stone workers. Chest 2012, 142, 419–424. [Google Scholar] [CrossRef]
- Grubstein, A.; Osnat Shtraichman, M.D.; Fireman, E.; Bachar, G.N.; Noach-Ophir, N.; Kramer, M.R. Radiological Evaluation of Artificial Stone Silicosis Outbreak: Emphasizing Findings in Lung Transplant Recipients. J. Comput. Assist. Tomogr. 2016, 40, 923–927. [Google Scholar] [CrossRef]
- Rosengarten, D.; Fox, B.D.; Fireman, E.; Blanc, P.D.; Rusanov, V.; Fruchter, O.; Raviv, Y.; Shtraichman, O.; Saute, M.; Kramer, M.R. Survival following lung transplantation for artificial stone silicosis relative to idiopathic pulmonary fibrosis. Am. J. Ind. Med. 2017, 60, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Alonso, A.; Córdoba-Doña, J.A.; Millares-Lorenzo, J.L.; Figueroa-Murillo, E.; García-Vadillo, C.; Romero-Morillos, J. Outbreak of silicosis in Spanish quartz conglomerate workers. Int. J. Occup. Environ. Health 2014, 20, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual, S.; Urrutia, I.; Ballaz, A.; Arrizubieta, I.; Altube, L.; Salinas, C. Prevalence of silicosis in a marble factory after exposure to quartz conglomerates. Arch. Bronconeumol. 2011, 47, 50–51. [Google Scholar] [CrossRef] [PubMed]
- Pascual Del Pobil, Y.; Ferré, M.A.; García Sevila, R.; García Rodenas, M.D.M.; Barroso Medel, E.; Flores Reos, E.; Gil Carbonell, J. Silicosis: A former occupational disease with new occupational exposure escenarios. Rev. Clin. Esp. 2019, 219, 16–19. [Google Scholar] [CrossRef]
- Pérez-Alonso, A.; Córdoba-Doña, J.A.; León-Jiménez, A. Silicosis Caused by Artificial Quartz Conglomerates: Keys to Controlling an Emerging Disease. Arch. Bronconeumol. 2019, 55, 394–395. [Google Scholar] [CrossRef]
- Instituto Nacional de Silicosis. Nuevos Casos de Silicosis Registrados en el INS Durante el año 2019. Available online: https://ins.astursalud.es/documents/102310/0/Estad%C3%ADsticas+del+2019.pdf/bf7fd36d-cb7f-215a-7c44-45ccf7dcaea1 (accessed on 4 May 2021).
- Rushton, L. Occupational causes of chronic obstructive pulmonary disease. Rev. Environ. Health 2007, 22, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Nery, L.E.; Florencio, R.T.; Sandoval, P.R.; Rodrigues, R.T.; Alonso, G.; Mason, G.R. Additive effects of exposure to silica dust and smoking on pulmonary epithelial permeability: A radio aerosol study with technetium-99m labelled DTPA. Thorax 1993, 48, 264–268. [Google Scholar] [CrossRef] [Green Version]
- Ge, C.; Peters, S.; Olsson, A.; Portengen, L.; Schüz, J.; Almansa, J.; Behrens, T.; Pesch, B.; Kendzia, B.; Ahrens, W.; et al. Respirable Crystalline Silica Exposure, Smoking, and Lung Cancer Subtype Risks. A Pooled Analysis of Case-Control Studies. Am. J. Respir. Crit. Care Med. 2020, 202, 412–421. [Google Scholar] [CrossRef]
- Manfreda, J.; Sidwall, G.; Maini, K.; West, P.; Cherniack, R.M. Respiratory abnormalities in employees of the hard rock mining industry. Am. Rev. Respir. Dis. 1982, 126, 629–634. [Google Scholar] [CrossRef]
- Kreiss, K.; Greenberg, L.M.; Kogut, S.J.; Lezotte, D.C.; Irvin, C.G.; Cherniack, R.M. Hard-rock mining exposure affects smokers and non-smokers differently. Am Rev. Respir. Dis. 1989, 139, 1487–1493. [Google Scholar] [CrossRef]
- Wang, D.; Yang, M.; Liu, Y.; Ma, J.; Shi, T.; Chen, W. Association of Silica Dust Exposure and Cigarette Smoking With Mortality Among Mine and Pottery Workers in China. JAMA Netw. Open 2020, 3, e202787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, H.; Liu, Y.; Zhou, M.; Shi, T.; Zhou, Y.; Weng, S.; Chen, W. Combined effect of silica dust exposure and cigarette smoking on total and cause-specific mortality in iron miners: A cohort study. Environ. Health 2018, 17, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Silicosis (n = 64) | No Silicosis (n = 247) | p Value | |
|---|---|---|---|---|
| Age, in years | 39.03 (7.90) | 40.13 (11.88) | 0.37 * | |
| Educational level | Non studies | 12 (18.8%) | 26 (10.5%) | 0.003 ** |
| Low | 44 (68.8%) | 133 (53.8%) | ||
| Medium | 6 (9.4%) | 77 (31.2%) | ||
| High | 2 (3.1%) | 11 (4.5%) | ||
| Tobacco | Yes | 33 (18.1%) | 149 (81.9%) | 0.07 ** |
| No | 10 (16.7%) | 50 (83.3%) | ||
| Former smoker | 21 (69.6%) | 48 (30.4%) | ||
| No. Cigarettes/day | 22.35 (9.72) | 21.21 (11.02) | 0.57 ** | |
| Smoking time (in years) | 22.30 (10.85) | 21.13 (11.43) | 0.59 ** | |
| Characteristic | Silicosis (n = 64) | No Silicosis (n = 247) | p Value | |
|---|---|---|---|---|
| Chronic Pathologies | None | 14 (21.9%) | 92 (37.2%) | 0.15 * |
| Cardiovascular | 10 (15.6%) | 29 (11.7%) | ||
| Endocrine–metabolic | 9 (14.1%) | 19 (7.7%) | ||
| Respiratory 1 | 28 (43.7%) | 96 (38.9%) | ||
| Urological | 3 (4.7%) | 11 (4.5%) | ||
| Dyspnea | Dyspnea (little exertion) | 25 (39.1%) | 62 (25.1%) | 0.08 * |
| Dyspnea (great exertion) | 17 (26.6%) | 80 (32.4%) | ||
| No | 22 (34.4%) | 105 (42.5%) | ||
| COPD | Yes | 57 (34.4%) | 57 (23.1%) | 0.06 * |
| No | 42 (65.6%) | 190 (76.9%) | ||
| Silicosis Clinic | Acute | 27 (42.2%) | - | - |
| Accelerated | 21 (32.8%) | - | ||
| Chronic | 16 (25.0%) | - | ||
| Characteristic | Silicosis (n = 64) | No Silicosis (n = 247) | p-Value | |
|---|---|---|---|---|
| Time Worked with Exposure to SiO2 (years) | 8.40 (6.75) | 14.75 (9.47) | 0.001 * | |
| Job | Court | 23 (35.9%) | 83 (33.6%) | 0.07 ** |
| Elaboration | 13 (20.3%) | 64 (25.9%) | ||
| Polished | 8 (12.5%) | 51 (20.6%) | ||
| Honed | 7 (10.9%) | 27 (10.9%) | ||
| Setter | 13 (20.3%) | 22 (8.9%) | ||
| Workplace | Assembly at customers’ homes | 13 (20.3%) | 22 (8.9%) | 0.01 ** |
| Manufacturing workshops | 51 (79.7%) | 225 (91.1%) | ||
| Trained in ORP | Yes | 39 (60.9%) | 179 (72.5%) | 0.07 ** |
| No | 25 (39.1%) | 68 (27.5%) | ||
| PPE provided by the company | Yes | 41 (64.1%) | 198 (80.2%) | 0.007 ** |
| No | 23 (35.9%) | 49 (19.8%) | ||
| Use the mask | Yes | 54 (84.4%) | 240 (97.2%) | 0.001 ** |
| No | 10 (15.6%) | 7 (2.8%) | ||
| Parameters | OR | 95% C.I. | p-Value |
|---|---|---|---|
| Age (in years) | 1.13 | 1.06–1.19 | 0.001 |
| Educational levels (no studies) | 8.51 | 1.25–13.78 | 0.001 |
| Time exposed to SiO2 (years) | 0.77 | 0.71–0.83 | 0.001 |
| Workplace (assembly at customers’ homes) | 2.69 | 1.13–6.41 | 0.02 |
| PPE provided by the company (no) | 3.64 | 1.49–8.91 | 0.05 |
| Use the face mask (no) | 4.06 | 1.09–15.03 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requena-Mullor, M.; Alarcón-Rodríguez, R.; Parrón-Carreño, T.; Martínez-López, J.J.; Lozano-Paniagua, D.; Hernández, A.F. Association between Crystalline Silica Dust Exposure and Silicosis Development in Artificial Stone Workers. Int. J. Environ. Res. Public Health 2021, 18, 5625. https://doi.org/10.3390/ijerph18115625
Requena-Mullor M, Alarcón-Rodríguez R, Parrón-Carreño T, Martínez-López JJ, Lozano-Paniagua D, Hernández AF. Association between Crystalline Silica Dust Exposure and Silicosis Development in Artificial Stone Workers. International Journal of Environmental Research and Public Health. 2021; 18(11):5625. https://doi.org/10.3390/ijerph18115625
Chicago/Turabian StyleRequena-Mullor, Mar, Raquel Alarcón-Rodríguez, Tesifón Parrón-Carreño, Jose Joaquín Martínez-López, David Lozano-Paniagua, and Antonio F. Hernández. 2021. "Association between Crystalline Silica Dust Exposure and Silicosis Development in Artificial Stone Workers" International Journal of Environmental Research and Public Health 18, no. 11: 5625. https://doi.org/10.3390/ijerph18115625