
The Burden of Hidradenitis Suppurativa Signs and Symptoms in Quality of Life: Systematic Review and Meta-Analysis

 ,
,  ,
, 
Abstract
:1. Introduction
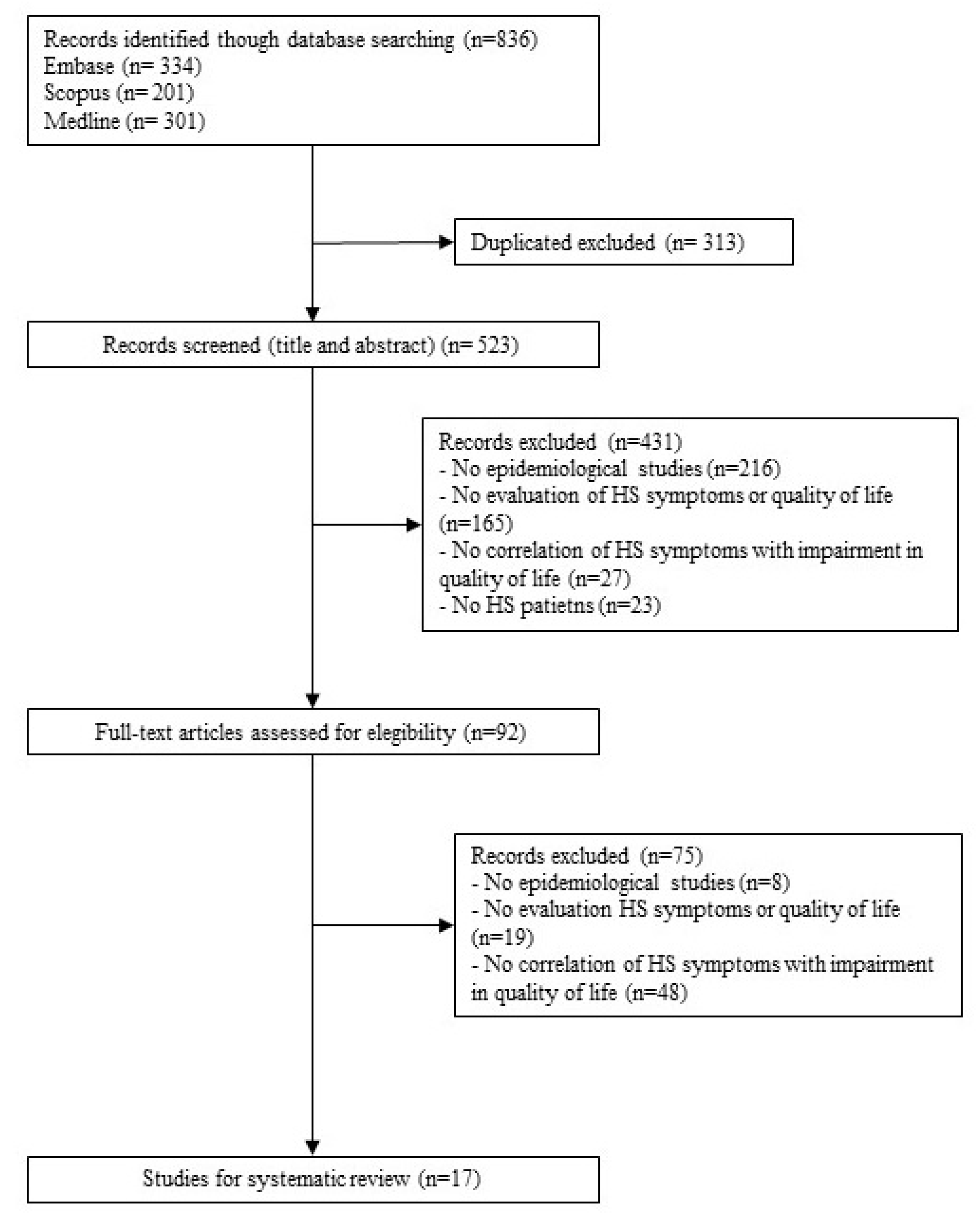
2. Materials and Methods
3. Results
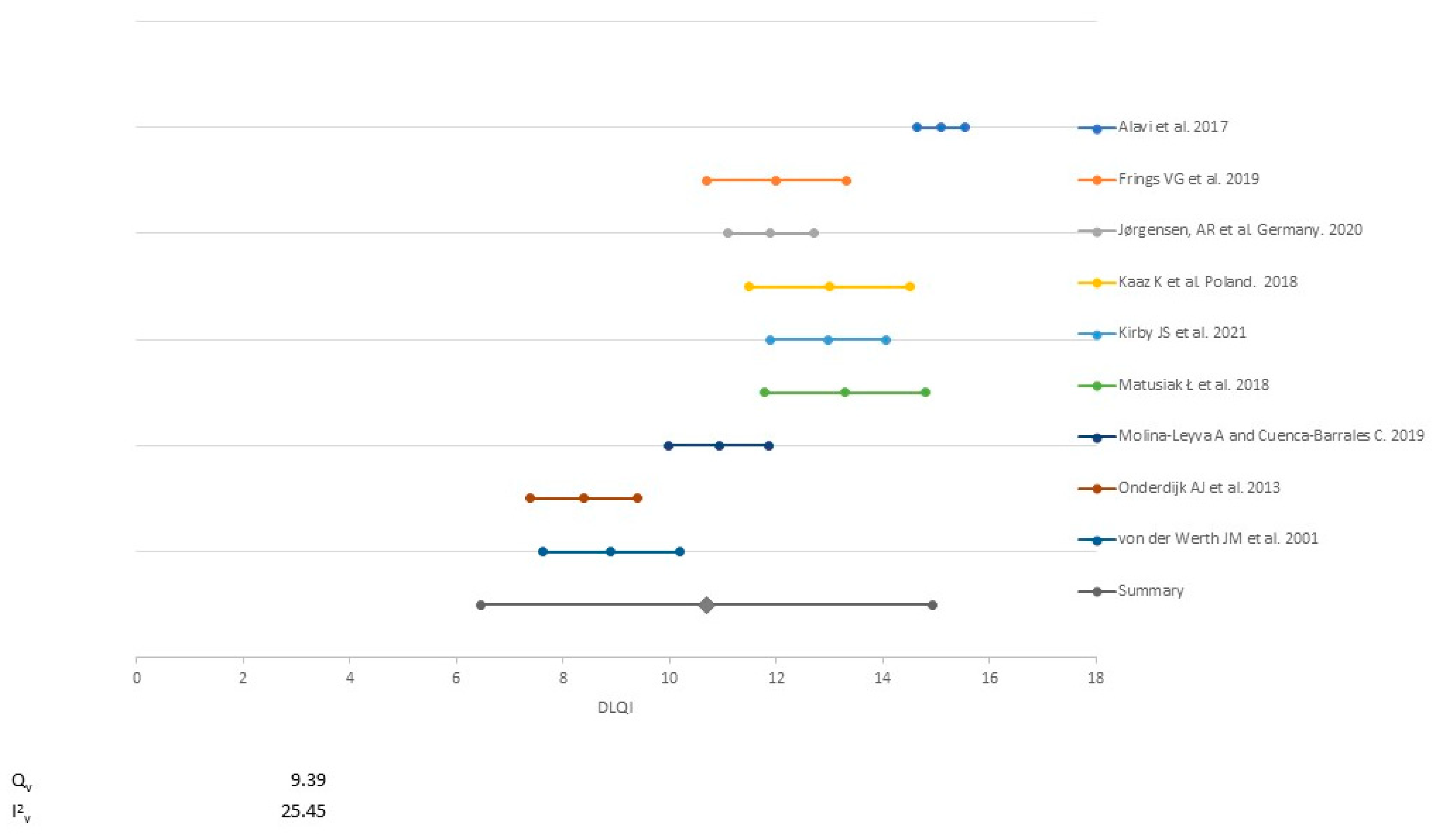
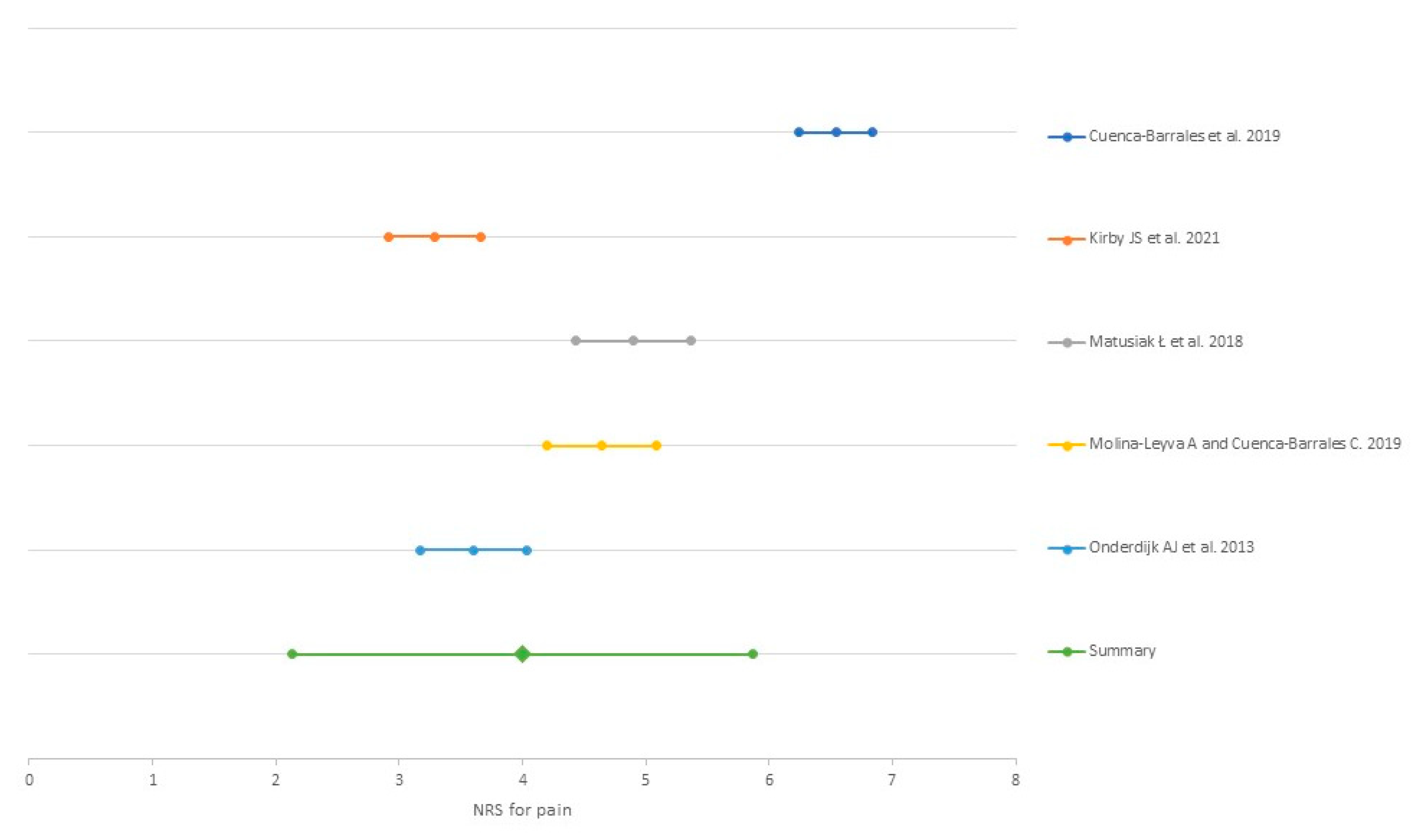
3.1. Pain
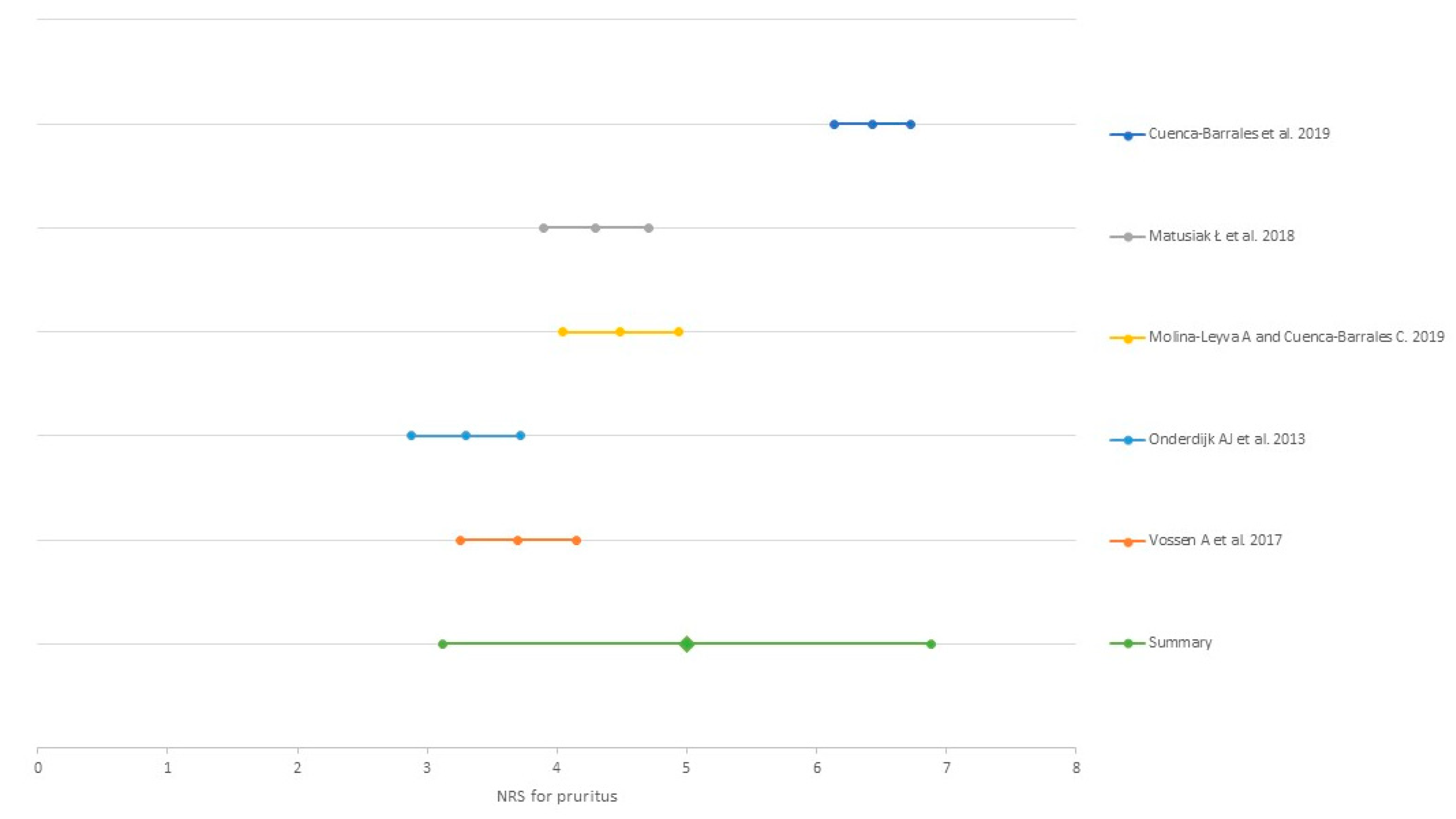
3.2. Pruritus
3.3. Malodour
3.4. Suppuration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen, T.V.; Damiani, G.; Orenstein, L.A.V.; Hamzavi, I.; Jemec, G.B. Hidradenitis suppurativa: An update on epidemiology, phenotypes, diagnosis, pathogenesis, comorbidities and quality of life. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 50–61. [Google Scholar] [CrossRef]
- Orenstein, L.A.V.; Nguyen, T.V.; Damiani, G.; Sayed, C.; Jemec, G.B.E.; Hamzavi, I. Medical and Surgical Management of Hidradenitis Suppurativa: A Review of International Treatment Guidelines and Implementation in General Dermatology Practice. Dermatology 2020, 236, 393–412. [Google Scholar] [CrossRef]
- Alikhan, A.; Lynch, P.J.; Eisen, D.B. Hidradenitis suppurativa: A comprehensive review. J. Am. Acad. Dermatol. 2009, 60, 539–561. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Bechara, F.G.; Dickinson-Blok, J.L.; Gulliver, W.; Horvath, B.; Hughes, R.; Kimball, A.B.; Kirby, B.; Martorell, A.; Podda, M.; et al. Hidradenitis suppurativa/acne inversa: A practical framework for treatment optimization-systematic review and recommendations from the HS ALLIANCE working group. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Alavi, A.; Anooshirvani, N.; Kim, W.B.; Coutts, P.; Sibbald, R.G. Quality-of-life impairment in patients with hidradenitis suppurativa: A Canadian study. Am. J. Clin. Dermatol. 2015, 16, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Matusiak, L.; Bieniek, A.; Szepietowski, J.C. Psychophysical aspects of hidradenitis suppurativa. Acta. Derm. Venereol. 2010, 90, 264–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matusiak, Ł. Profound consequences of hidradenitis suppurativa: A review. Br. J. Dermatol. 2020, 183, e171–e177. [Google Scholar] [CrossRef]
- Jemec, G.B. Quality of life considerations and pain management in hidradenitis suppurativa. Semin. Cutan. Med. Surg. 2017, 36, 75–78. [Google Scholar] [CrossRef]
- Schneider-Burrus, S.; Jost, A.; Peters, E.M.J.; Witte-Haendel, E.; Sterry, W.; Sabat, R. Association of Hidradenitis Suppurativa With Body Image. JAMA Dermatol. 2018, 154, 447–451. [Google Scholar] [CrossRef]
- Tugnoli, S.; Agnoli, C.; Silvestri, A.; Giari, S.; Bettoli, V.; Caracciolo, S. Anger, Emotional Fragility, Self-esteem, and Psychiatric Comorbidity in Patients with Hidradenitis Suppurativa/Acne Inversa. J. Clin. Psychol. Med. Settings 2019. [Google Scholar] [CrossRef]
- Machado, M.O.; Stergiopoulos, V.; Maes, M.; Kurdyak, P.A.; Lin, P.Y.; Wang, L.J.; Shyu, Y.C.; Firth, J.; Koyanagi, A.; Solmi, M.; et al. Depression and Anxiety in Adults With Hidradenitis Suppurativa: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019, 155, 939–945. [Google Scholar] [CrossRef]
- Thorlacius, L.; Cohen, A.D.; Gislason, G.H.; Jemec, G.B.E.; Egeberg, A. Increased Suicide Risk in Patients with Hidradenitis Suppurativa. J. Investig. Dermatol. 2018, 138, 52–57. [Google Scholar] [CrossRef] [Green Version]
- Cuenca-Barrales, C.; Montero-Vilchez, T.; Szepietowski, J.C.; Matusiak, L.; Molina-Leyva, A. Sexual impairment in patients with hidradenitis suppurativa: A systematic review. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 345–352. [Google Scholar] [CrossRef]
- Chernyshov, P.V.; Zouboulis, C.C.; Tomas-Aragones, L.; Jemec, G.B.; Svensson, A.; Manolache, L.; Tzellos, T.; Sampogna, F.; Pustisek, N.; van der Zee, H.H.; et al. Quality of life measurement in hidradenitis suppurativa: Position statement of the European Academy of Dermatology and Venereology task forces on Quality of Life and Patient-Oriented Outcomes and Acne, Rosacea and Hidradenitis Suppurativa. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1633–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marron, S.E.; Gomez-Barrera, M.; Tomas-Aragones, L.; Diaz Diaz, R.M.; Vilarrasa Rull, E.; Madrid Alvarez, M.B.; Puig, L. Development and Preliminary Validation of the HSQoL-24 Tool to Assess Quality of Life in Patients With Hidradenitis Suppurativa. Actas Dermo-Sifiliográficas 2019, 110, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Zouboulis, C.C.; Desai, N.; Emtestam, L.; Hunger, R.E.; Ioannides, D.; Juhasz, I.; Lapins, J.; Matusiak, L.; Prens, E.P.; Revuz, J.; et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 619–644. [Google Scholar] [CrossRef] [PubMed]
- Kluger, N.; Ranta, M.; Serlachius, M. The Burden of Hidradenitis Suppurativa in a Cohort of Patients in Southern Finland: A Pilot Study. Skin Appendage Disord. 2017, 3, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Smith, H.S.; Chao, J.D.; Teitelbaum, J. Painful hidradenitis suppurativa. Clin. J. Pain 2010, 26, 435–444. [Google Scholar] [CrossRef]
- Nielsen, R.M.; Lindso Andersen, P.; Sigsgaard, V.; Theut Riis, P.; Jemec, G.B. Pain perception in patients with hidradenitis suppurativa. Br. J. Dermatol. 2020, 182, 166–174. [Google Scholar] [CrossRef]
- Esmann, S.; Jemec, G.B. Psychosocial impact of hidradenitis suppurativa: A qualitative study. Acta Derm. Venereol. 2011, 91, 328–332. [Google Scholar] [CrossRef] [Green Version]
- Dufour, D.N.; Emtestam, L.; Jemec, G.B. Hidradenitis suppurativa: A common and burdensome, yet under-recognised, inflammatory skin disease. Postgrad. Med. J. 2014, 90, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Neyeloff, J.L.; Fuchs, S.C.; Moreira, L.B. Meta-analyses and Forest plots using a microsoft excel spreadsheet: Step-by-step guide focusing on descriptive data analysis. BMC Res. Notes 2012, 5, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The National Institutes of Health. Study Quality Assessment Tools. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 2020. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 16 June 2021).
- Cuenca-Barrales, C.; Molina-Leyva, A. Risk Factors of Sexual Dysfunction in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study. Dermatology 2020, 236, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-Barrales, C.; Ruiz-Villaverde, R.; Molina-Leyva, A. Sexual Distress in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study. J. Clin. Med. 2019, 8, 532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frings, V.G.; Bauer, B.; Glöditzsch, M.; Goebeler, M.; Presser, D. Assessing the psychological burden of patients with hidradenitis suppurativa. Eur. J. Dermatol. 2019, 29, 294–301. [Google Scholar] [CrossRef]
- Huilaja, L.; Hirvonen, M.J.; Lipitsä, T.; Vihervaara, A.; Harvima, R.; Sintonen, H.; Kouri, J.P.; Ranta, M.; Pasternack, R. Patients with hidradenitis suppurativa may suffer from neuropathic pain: A Finnish multicenter study. J. Am. Acad. Dermatol. 2020, 82, 1232–1234. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, A.R.; Holm, J.G.; Ghazanfar, M.N.; Yao, Y.; Ring, H.C.; Thomsen, S.F. Factors affecting quality of life in patients with hidradenitis suppurativa. Arch. Dermatol. Res. 2020, 312, 427–436. [Google Scholar] [CrossRef]
- Kaaz, K.; Szepietowski, J.C.; Matusiak, Ł. Influence of Itch and Pain on Sleep Quality in Patients with Hidradenitis Suppurativa. Acta Derm. Venereol. 2018, 98, 757–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirby, J.S.; Hereford, B.; Thorlacius, L.; Villumsen, B.; Ingram, J.R.; Garg, A.; Butt, M.; Esmann, S.; King, T.; Tan, J.; et al. Validation of global item for assessing impact on quality of life of patients with hidradenitis suppurativa. Br. J. Dermatol. 2021, 184, 681–687. [Google Scholar] [CrossRef]
- Krajewski, P.K.; Matusiak, Ł.; von Stebut, E.; Schultheis, M.; Kirschner, U.; Nikolakis, G.; Szepietowski, J.C. Quality-of-Life Impairment among Patients with Hidradenitis Suppurativa: A Cross-Sectional Study of 1795 Patients. Life 2021, 11, 34. [Google Scholar] [CrossRef]
- Matusiak, Ł.; Szczęch, J.; Kaaz, K.; Lelonek, E.; Szepietowski, J.C. Clinical Characteristics of Pruritus and Pain in Patients with Hidradenitis Suppurativa. Acta Derm. Venereol. 2018, 98, 191–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Leyva, A.; Cuenca-Barrales, C. Pruritus and Malodour in Patients with Hidradenitis Suppurativa: Impact on Quality of Life and Clinical Features Associated with Symptom Severity. Dermatology 2020, 236, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Onderdijk, A.J.; van der Zee, H.H.; Esmann, S.; Lophaven, S.; Dufour, D.N.; Jemec, G.B.; Boer, J. Depression in patients with hidradenitis suppurativa. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Sampogna, F.; Fania, L.; Mazzanti, C.; Caggiati, A.; Pallotta, S.; Panebianco, A.; Mastroeni, S.; Didona, B.; Pintori, G.; Abeni, D. The Broad-Spectrum Impact of Hidradenitis Suppurativa on Quality of Life: A Comparison with Psoriasis. Dermatology 2019, 235, 308–314. [Google Scholar] [CrossRef]
- von der Werth, J.M.; Jemec, G.B. Morbidity in patients with hidradenitis suppurativa. Br. J. Dermatol. 2001, 144, 809–813. [Google Scholar] [CrossRef] [Green Version]
- Alavi, A.; Farzanfar, D.; Lee, R.K.; Almutairi, D. The Contribution of Malodour in Quality of Life of Patients with Hidradenitis Suppurativa. J. Cutan. Med. Surg. 2018, 22, 166–174. [Google Scholar] [CrossRef]
- Machado, M.O.; Lu, J.D.; Brar, R.; Kirby, J.S.; Garg, A.; Lowes, M.L.; Piguet, V.; Alavi, A. Hidradenitis suppurativa odour and drainage scale: A novel method for evaluating odour and drainage in patients with hidradenitis suppurativa. Br. J. Dermatol. 2021, 184, 772–774. [Google Scholar] [CrossRef]
- Riis, P.T.; Vinding, G.R.; Ring, H.C.; Jemec, G.B. Disutility in Patients with Hidradenitis Suppurativa: A Cross-sectional Study Using EuroQoL-5D. Acta Derm. Venereol. 2016, 96, 222–226. [Google Scholar] [CrossRef] [Green Version]
- Vossen, A.; Schoenmakers, A.; van Straalen, K.R.; Prens, E.P.; van der Zee, H.H. Assessing Pruritus in Hidradenitis Suppurativa: A Cross-Sectional Study. Am. J. Clin. Dermatol. 2017, 18, 687–695. [Google Scholar] [CrossRef] [Green Version]
- Patel, Z.S.; Hoffman, L.K.; Buse, D.C.; Grinberg, A.S.; Afifi, L.; Cohen, S.R.; Lowes, M.A.; Seng, E.K. Pain, Psychological Comorbidities, Disability, and Impaired Quality of Life in Hidradenitis Suppurativa [corrected]. Curr. Pain Headache Rep. 2017, 21, 49. [Google Scholar] [CrossRef]
- Balieva, F.N.; Finlay, A.Y.; Kupfer, J.; Aragones, L.T.; Lien, L.; Gieler, U.; Poot, F.; Jemec, G.B.E.; Misery, L.; Kemeny, L.; et al. The Role of Therapy in Impairing Quality of Life in Dermatological Patients: A Multinational Study. Acta Derm. Venereol. 2018, 98, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Jedrzejczak, M.J.; Ingram, J.R.; Lowes, M.A.; Naik, H.B.; McKenzie-Brown, A.M.; Chen, S.C.; Orenstein, L.A.V. Expert Knowledge, Attitudes, and Practices in Management of Hidradenitis Suppurativa Pain. JAMA Dermatol. 2021, 157, 464–466. [Google Scholar] [CrossRef]
- Savage, K.T.; Singh, V.; Patel, Z.S.; Yannuzzi, C.A.; McKenzie-Brown, A.M.; Lowes, M.A.; Orenstein, L.A.V. Pain management in hidradenitis suppurativa and a proposed treatment algorithm. J. Am. Acad. Dermatol. 2020. [Google Scholar] [CrossRef]
- Krajewski, P.K.; Matusiak, L.; von Stebut, E.; Schultheis, M.; Kirschner, U.; Nikolakis, G.; Szepietowski, J.C. Pain in Hidradenitis Suppurativa: A Cross-sectional Study of 1,795 Patients. Acta Derm. Venereol. 2021, 101, adv00364. [Google Scholar] [CrossRef]
- Chien, C.W.; Bagraith, K.S.; Khan, A.; Deen, M.; Syu, J.J.; Strong, J. Establishment of cutpoints to categorize the severity of chronic pain using composite ratings with Rasch analysis. Eur. J. Pain 2017, 21, 82–91. [Google Scholar] [CrossRef]
- Balieva, F.; Kupfer, J.; Lien, L.; Gieler, U.; Finlay, A.Y.; Tomas-Aragones, L.; Poot, F.; Misery, L.; Sampogna, F.; van Middendorp, H.; et al. The burden of common skin diseases assessed with the EQ5D: A European multicentre study in 13 countries. Br. J. Dermatol. 2017, 176, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Kouris, A.; Platsidaki, E.; Christodoulou, C.; Efstathiou, V.; Dessinioti, C.; Tzanetakou, V.; Korkoliakou, P.; Zisimou, C.; Antoniou, C.; Kontochristopoulos, G. Quality of Life and Psychosocial Implications in Patients with Hidradenitis Suppurativa. Dermatology 2016, 232, 687–691. [Google Scholar] [CrossRef]
- Kirby, J.S.; Butt, M.; Esmann, S.; Jemec, G.B.E. Association of Resilience With Depression and Health-Related Quality of Life for Patients With Hidradenitis Suppurativa. JAMA Dermatol. 2017, 153, 1263–1269. [Google Scholar] [CrossRef] [PubMed]
- Bogels, S.M.; Alden, L.; Beidel, D.C.; Clark, L.A.; Pine, D.S.; Stein, M.B.; Voncken, M. Social anxiety disorder: Questions and answers for the DSM-V. Depress Anxiety 2010, 27, 168–189. [Google Scholar] [CrossRef] [PubMed]
- van der Zee, H.H.; de Ruiter, L.; van den Broecke, D.G.; Dik, W.A.; Laman, J.D.; Prens, E.P. Elevated levels of tumour necrosis factor (TNF)-alpha, interleukin (IL)-1beta and IL-10 in hidradenitis suppurativa skin: A rationale for targeting TNF-alpha and IL-1beta. Br. J. Dermatol. 2011, 164, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Henje Blom, E.; Lekander, M.; Ingvar, M.; Asberg, M.; Mobarrez, F.; Serlachius, E. Pro-inflammatory cytokines are elevated in adolescent females with emotional disorders not treated with SSRIs. J. Affect. Disord. 2012, 136, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Ceccherini, I.; Gattorno, M.; Fanoni, D.; Caroli, F.; Rusmini, M.; Grossi, A.; De Simone, C.; Borghi, O.M.; Meroni, P.L.; et al. Association of pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH) shares genetic and cytokine profiles with other autoinflammatory diseases. Medicine 2014, 93, e187. [Google Scholar] [CrossRef]
- Margiotta, D.P.E.; Basta, F.; Dolcini, G.; Batani, V.; Navarini, L.; Afeltra, A. The relation between, metabolic syndrome and quality of life in patients with Systemic Lupus Erythematosus. PLoS ONE 2017, 12, e0187645. [Google Scholar] [CrossRef] [PubMed]
- Aras, Y.G.; Tunc, A.; Gungen, B.D.; Gungen, A.C.; Aydemir, Y.; Demiyurek, B.E. The effects of depression, anxiety and sleep disturbances on cognitive impairment in patients with chronic obstructive pulmonary disease. Cogn. Neurodyn. 2017, 11, 565–571. [Google Scholar] [CrossRef]
- Ge, Y.; Xin, S.; Luan, D.; Zou, Z.; Liu, M.; Bai, X.; Gao, Q. Association of physical activity, sedentary time, and sleep duration on the health-related quality of life of college students in Northeast China. Health Qual. Life Outcomes 2019, 17, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Leyva, A.; Almodovar-Real, A.; Carrascosa, J.C.; Molina-Leyva, I.; Naranjo-Sintes, R.; Jimenez-Moleon, J.J. Distribution pattern of psoriasis, anxiety and depression as possible causes of sexual dysfunction in patients with moderate to severe psoriasis. An. Bras. Dermatol. 2015, 90, 338–345. [Google Scholar] [CrossRef]
- Ring, H.C.; Theut Riis, P.; Zarchi, K.; Miller, I.M.; Saunte, D.M.; Jemec, G.B. Prodromal symptoms in hidradenitis suppurativa. Clin. Exp. Dermatol. 2017, 42, 261–265. [Google Scholar] [CrossRef]
- Yu, S.H.; Attarian, H.; Zee, P.; Silverberg, J.I. Burden of Sleep and Fatigue in US Adults With Atopic Dermatitis. Dermatitis 2016, 27, 50–58. [Google Scholar] [CrossRef]
- Henry, A.L.; Kyle, S.D.; Bhandari, S.; Chisholm, A.; Griffiths, C.E.; Bundy, C. Measurement, Classification and Evaluation of Sleep Disturbance in Psoriasis: A Systematic Review. PLoS ONE 2016, 11, e0157843. [Google Scholar] [CrossRef] [Green Version]
- Adeyemi, B.F.; Kolude, B.M.; Arigbede, A.O. Attitude and perception of mouth odour in 213 respondents. Niger. Postgrad. Med. J. 2012, 19, 97–101. [Google Scholar]
- Kurek, A.; Peters, E.M.; Chanwangpong, A.; Sabat, R.; Sterry, W.; Schneider-Burrus, S. Profound disturbances of sexual health in patients with acne inversa. J. Am. Acad. Dermatol. 2012, 67, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Ring, H.C.; Bay, L.; Nilsson, M.; Kallenbach, K.; Miller, I.M.; Saunte, D.M.; Bjarnsholt, T.; Tolker-Nielsen, T.; Jemec, G.B. Bacterial biofilm in chronic lesions of hidradenitis suppurativa. Br. J. Dermatol. 2017, 176, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Ring, H.C.; Bay, L.; Kallenbach, K.; Miller, I.M.; Prens, E.; Saunte, D.M.; Bjarnsholt, T.; Jemec, G.B. Normal Skin Microbiota is Altered in Pre-clinical Hidradenitis Suppurativa. Acta Derm. Venereol. 2017, 97, 208–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Site and Year | Design | CEBM | Participants | Age (Years) | Sex (Female:Male Ratio) | BMI (kg/m2) | Smoking Habit (Yes) | Disease Duration (Years) | Disease Severity (Hurley I/II/III) | HS Symptom Evaluated | Main Aspects Od QoL Evaluated |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alavi et al. Canada 2017 [37] | Cross-sectional | 4 | 51 | 32.50 ± 10.76 | 2.47:1 | NS | NS | 11.10 ± 8.57 | 13.7% (7)/45.1% (23)/41.2% (21) | Malodour | Overall QoL |
| Cuenca-Barrales et al. Spain. 2019 [25] | Cross-sectional | 4 | 386 | 37.81 ± 9.26 | 3.83:1 | 29.35 ± 6.71 | 42.2% (163) | 17.77 ± 9.62 | 17.6% (68)/45.1% (174)/37.3% (144) | Pain, pruritus, malodour, suppuration | Sexual distress |
| Cuenca-Barrales and Molina-Leyva. Spain. 2020 [24] | Cross-sectional | 4 | 386 | 37.81 ± 9.26 | 3.83:1 | 29.35 ± 6.71 | 42.2% (163) | 17.77 ± 9.62 | 17.6% (68)/45.1% (174)/37.3% (144) | Pain, pruritus, malodour, suppuration | Sexual dysfunction |
| Frings et al. Germany. 2019 [26] | Cross.sectional | 4 | 110 | 38 ± 12 | 1.24:1 | 30.5 ± 6.9 | 37% (41) | NS | 7% (8)/30% (33)/63% (69) | Pain | Overall QoL, anxiety and depression |
| Huilaja et al. Finland. 2020 [27] | Cross-sectional | 4 | 92 | NS * | NS * | NS * | NS * | NS * | NS * | Pain | Overall QoL and depression |
| Jørgensenet al. Germany. 2020 [28] | Cross-sectional | 4 | 339 | 39.4 ± 13.5 | 1.80:1 | 29 ± 7.6 | 75.2% (255) | 13.8 ± 11.5 | 28.3% (96)/ 57.5% (195)/14.2% (48) | Pain | Overall QoL |
| Kaaz et al. Poland. 2018 [29] | Cross-sectional | 4 | 108 | 36.3 ± 12.1 | 0.89:1 | 28.8 ± 5.4 | 18% (60) | 9.1 ± 8.3 | 46.3% (50)/45.4% (49)/ 8.3% (9) | Pain and pruritus | Sleep and insomnia |
| Kirby et al. Denmark and USA. 2021 [30] | Cross-sectional | 4 | 224 | 39.6 (19-77) | 6.72:1 | NS | NS | NS | NS | Pain | Overall QoL |
| Krajewski et al. Germany and Poland. 2021 [31] | Cross-sectional | 4 | 1795 | 40.0 ± 11.8 | 1.79:1 | 28.1 ± 6.2 | 55.6% (998) | NS | NS | Pain | Overall QoL |
| Machado et al. Canada. 2021 [38] | Cross-sectional | 4 | 30 | 40.87 ± 2.55 | 2.33:1 | NS | NS | NS | NS | Malodour and drainage | Overall QoL |
| Matusiak et al. Poland 2018. [32] | Cross-sectional | 4 | 103 | 35.6 ± 13.2 | 0.94:1 | 29.4 ± 5.7 | 54.4% (56) | 8.9 ± 7.5 | 40.8% (42)/45.6% (47)/13.6% (14) | Pain and pruritus | Overall QoL |
| Molina-Leyva and Cuenca-Barrales. Spain. 2019 [33] | Cross-sectional | 4 | 233 | 40.14 ± 13.46 | 1.14:1 | 30.68 ± 7.05 | NS | 13.99 ± 10.59 | 30.04% (70); 41.63% (97); 28.33% (66) | Pruritus, malodour | Overall QoL |
| Onderdijk et al. Netherlands. 2013 [34] | Cross-sectional | 4 | 211 | 43.0 ± 11.8 | NS | NS | NS | 16.8 ± 11.6 | 30.1% (64)/56.4% (119)/13.5% (28) | Pain and pruritus | Overall QoL and depression |
| Riis et al. Denmark. 2016 [39] | Cross-sectional | 4 | 421 | 42.4 (19-77) | 3.74:1 | NS | NS | NS | NS | Pain, pruritus and malodour | Health-realted overall utility |
| Sampogna et al. Italy 2019 [35] | Cross-sectional | 4 | 69 | 34.5 ± 12.5 | 1.16:1 | NS | NS | NS | 27.5% (19)/43.5% (30)/29.0% (20) | Pain | Overaal QoL |
| von der Werth et al. Denmark. 2001 [36] | Cross-sectional | 4 | 160 | 40.9 ± 11.7 | 6.13:1 | NS | NS | NS | NS | Pain | Overall QoL |
| Vossen et al. Netherlands. 2017 [40] | Cross-sectional | 4 | 211 | 38.0 (29–49) | 1.78:1 | 28.5 ± 5.9 | 19.9% (62) | 14.0 (7–25) | 15% (32)/66% (140)/19% (39) | Pruritus | Activities of daily living and sleep |
| Study | Pain | QoL | Correlation between Pain and QoL | |||
|---|---|---|---|---|---|---|
| Assessment Tool | Score | Assessment Tool | Score | |||
| Cuenca-Barrales et al. Spain. 2019 [25] | NRS | 6.54 ± 2.95 | NRS for HS impact on sex life | 7.24 ± 2.77 in women 6.39 ± 3.44 in men | β = 0.15, p = 0.049 ** | |
| Cuenca-Barrales and Molina-Leyva. Spain. 2020 [24] | NRS | Women: 6.52 ± 2.98 | Prevalence of sexual dysfunction | FSFI-6 ≤ 19 | 51% (156) | β = 0.1, p < 0.05 ** |
| Men: 6.64 ± 2.81 | IIEF-5 ≤ 21 | 60% (48) | β = NS, p = 0.97 ** | |||
| Frings et al. Germany. 2019 [26] | VAS | NS | DLQI | 12 ± 7 | r = 0.457, p < 0.001 | |
| HADS-Depression | 6 ± 4 | r = 0.193, p = 0.105 | ||||
| HADS-Anxiety | 7 ± 4 | r = 0.304, p = 0.009 | ||||
| Skindex-29 symptom score | NS | r = 0.547, p < 0.001 | ||||
| Skindex-29 function score | r = 0.459, p < 0.001 | |||||
| Skindex-29 emotion score | r = 0.399, p < 0.001 | |||||
| Huilaja et al. Finland. 2020 [27] | VAS: -No pain (0–4 mm)/ -Mild pain (5–44 mm)/ -Moderate to severe pain (45–100 mm) | 37% (34)/ 45.7% (42)/ 17.4% (16)/ | DLQI | 3.03 (0–9) vs. 8.76 (0–23) vs. 13.69 (4–29) | p < 0.001 ¶ | |
| Beck’s Depression Inventory | 6.68 (0–4.0) vs. 9.26 (0–30) vs. 13.06 (1–32) | p = 0.019 ¶ | ||||
| PainDETECT: -Pain negative (0–12)/ -Unclear (13–18)/ -Pain positive (19–38) | 41.3% (38)/ 27.2% (25)/ 31.5% (29) | DLQI | 4.53 (0–16) vs. 8.84 (1–23) vs. 10.55 (0–29) | p < 0.001 ¶ | ||
| Beck’s Depression Inventory | 6.84 (0–20) vs. 7.68 (0–19) vs. 12.86 (0–32) | p = 0.003 ¶ | ||||
| Jørgensen et al. Germany. 2020 [28] | Boil-associated pain score (0–10) ≤5 boils/ >5 boils | 8.6 ± 7.4/ 15 ± 7.4 | DLQI | 11.9 ± 7.6 | Mean difference: 6.3 ± 1.85, p < 0.001 ʡ | |
| Kaaz et al. Poland. 2018 [29] | VAS | 4.9 ± 2.9 | DLQI | 13.0 ± 8.0 | NS | |
| AIS | 5.4 ± 4.3 | p < 0.05 ^ | ||||
| PSQI | 6.5 ± 3.6 | p < 0.05 ^ | ||||
| Kirby et al. Denmark and USA. 2021 [30] | NRS | 3.29 ± 2.83 | DLQI | 12.97 ± 8.33 | NS | |
| PtGA of QoL (0–4) | 2.09 ± 1.34 | r = 0.66 (0.6–0.71 95% CI) # | ||||
| Krajewski et al. Germany and Poland. 2021 [31] | NRS | NS | DLQI | 13.2 ± 8.1 | r = 0.581; p < 0.001 ^ | |
| Matusiak et al. Poland. 2018 [32] | Prevalence of pain | 77.5% (80) | DLQI | 13.3 ± 7.8 | NS | |
| VAS | 4.6 ± 2.5 | r = 0.48, p < 0.001 ^^ | ||||
| NRS | 4.9 ± 2.4 | r = 0.48, p < 0.001 ^^ | ||||
| Molina-Leyva and Cuenca-Barrales. Spain. 2019 [33] | NRS | 4.64 ± 3.43 | DLQI | 10.93 ± 7.3 | β = 0.91 ± 0.12, R2 = 0.36, p < 0.001 * | |
| Onderdijk et al. Netherlands. 2013 [34] | NRS | 3.6 ±3.2 | DLQI | 8.4 ± 7.5 | r = 0.60, p < 0.05 ʡ | |
| MDI | 4.3 ± 5.6 | r = 0.36, p < 0.05 ʡ | ||||
| Sampogna et al. Italy. 2019 [35] | VAS: <5/ 5–6/ ≥7 | 25.9% (11)/ 29% (20)/ 55.1% (38) | Skindex-17 Symptoms | 53.6 vs. 72.0 vs. 72.6, | p = 0.068¶ | |
| Skindex-17 psychosocial | 39.4 vs. 54.6 vs. 61.7 | p = 0.088 ¶ | ||||
| von der Werthet al. Denmark. 2001 [36] | Self-reported number of painful lesions | 2 | DLQI | 8.9 ± 8.3 | r = 0.384, p < 0.01 ʡ | |
| Study | Pruritus | QoL | Correlation between Pruritus and QoL | Factors Associated with Pruritus | |||
|---|---|---|---|---|---|---|---|
| Assessment Tool | Score | Assessment Tool | Score | ||||
| Cuenca-Barrales et al. Spain. 2019 [25] | NRS | 6.43 ± 2.96 | NRS for HS impact on sex life | 7.24 ± 2.77 in women and 6.39 ± 3.44 in men | β = 0.03, p = 0.615 ** | NS | |
| Cuenca-Barrales and Molina-Leyva. Spain. 2020 [24] | NRS | Women: 6.48 ± 3.03 | Prevalence of sexual dysfunction | FSFI-6 ≤ 19 | 51% (156) | β = NS, p = 0.36 ** | NS |
| Men: 6.24 ± 2.67 | IIEF-5 ≤ 21 | 60% (48) | β = NS, p = 0.28 ** | NS | |||
| Kaaz et al. Poland. 2018 [29] | VAS | 4.1 ± 2.9 | DLQI | 13.0 ± 8.0 | NS | NS | |
| AIS | 5.4 ± 4.3 | p < 0.05 ^ | |||||
| PSQI | 6.5 ± 3.6 | p < 0.05 ^ | |||||
| Matusiak et al. Poland. 2018 [32] | Prevalence of pruritus | 41.7% | DLQI | 13.3 ± 7.8 | p = 0.79¶ | Hurley III, active smokers ¶ | |
| VAS | 3.9 ± 2.2 | r = 0.45, p = 0.004 ^^ | |||||
| NRS | 4.3 ±2.1 | r = 0.48, p = 0.002 ^^ | |||||
| 4-item Itch Questionnaire | 4.6 ± 1.9 | NS | |||||
| Molina-Leyva and Cuenca-Barrales. Spain. 2019 [33] | NRS (NRS pruritus> 3) | 4.49 ± 3.48 (61.8% (144)) | DLQI (DLQI> 10) | 10.93 ± 7.3 (49.79% (119)) | β = 0.42 ± 0.11, R2 = 0.20, p < 0.001 * | Number of regions affected (β = 0.51, p = 0.01), female sex (β = 0.46, p = 0.02), intensity of suppuration (β = 0.42, p < 0.001), Crohn’s disease (β = 1.24, p = 0.01), not statin use (β= 0.87, p = 0.03) # | |
| Onderdijk et al. Netherlands. 2013 [34] | NRS | 3.3 ± 3.1 | DLQI | 8.4 ± 7.5 | r = 0.53, p < 0.05 ʡ | NS | |
| MDI | 4.3 ± 5.6 | r = 0.33, p < 0.05 ʡ | |||||
| Riis et al. Denmark. 2016 [39] | NRS | NS | EQ-5D | NS | β= −0.017, p < 0.05 ** | NS | |
| Vossen et al. Netherlands. 2017 [40] | Prevalence of pruritus (NRS score ≥3) | 57.3% (121) | ADL Sleep | 70% (36/51) 53% (27/51) | NS | Hurley stage III (OR 7.73; p = 0.003) and higher levels of pain, (OR = 1.34 for each additional point on the NRS, p = 0.001) # | |
| NRS | 3.7 ± 3.3 | ||||||
| 5-D itch scale | 13.7 ± 3.6 | ||||||
| Study | Malodour | QoL Score | Correlation between Malodour and QoL | Risk Factors for Malodour | |||
|---|---|---|---|---|---|---|---|
| Assessment Tool | Score | Assessment Tool | Score | ||||
| Alavi et al. Canada 2017 [37] | NRS | 5.02 ± 3.06 | DLQI | 15.10 ± 1.64 | R2 = 0.17, F = 2.63, p = 0.064 a ** | Lesions groin, upper thighs, and buttocks (Pearson χ2 = 5.66, df = 1, p = 0.017). | |
| Skindex-19 | 65.33 ± 17.18 | R2 = 0.39, F = 8.11, p < 0.001 a ** | |||||
| Cuenca-Barrales et al. Spain. 2019 [25] | NRS | 5.6 ± 3.38 | NRS for HS impact on sex life | 7.24 ± 2.77 in women and 6.39 ± 3.44 in men | β = 0.13, p = 0.035 ** | NS | |
| Cuenca-Barrales and Molina-Leyva. Spain. 2020 [24] | NRS | Women: 5.47 ± 3.45 | Prevalence of sexual dysfunction | FSFI-6 ≤ 19 | 51% (156) | β = 0.07, p < 0.05 ** | NS |
| Men: 6.11 ± 3.05 | IIEF-5 ≤ 21 | 60% (48) | β = NS, p = 0.52 ** | NS | |||
| Machado et al. Canada. 2021 [38] | HODS-odour: | NS | Skindex-29 | NS | r = 0.726, p < 0.05 | NS | |
| Skindex-29 symptoms | NS | r = 0.733, p < 0.05 ^ | |||||
| Skindex-29 emotional | NS | r = 0.725, p < 0.05 ^ | |||||
| Skindex-29 functioning | NS | r = 0.719, p < 0.05 ^ | |||||
| HS-QoL overall | NS | r = 0.719, p < 0.05 ^ | |||||
| Molina-Leyva and Cuenca-Barrales. Spain. 2019 [33] | NRS (NRS > 3) | 3.28 ± 3.58 (40.77% (95)) | DLQI (DLQI > 10) | 10.93 ± 7.3 (49.79% (119)) | β = 0.44 ± 0.11, R2 = 0.23, p < 0.001 * | Higher BMI (β = 0.04, p = 0.07), Disease duration (β = 0.05, p = 0.01), Number of regions affected (β = 0.31, p = 0.08), Hurley stage (β = 0.60, p = 0.02), intensity of suppuration (β = 0.61, p < 0.001) | |
| Riis et al. Denmark. 2016 [39] | NRS | NS | EQ-5D | NS | β= −0.023, p < 0.05 ** | NS | |
| Study | Suppuration | QoL Score | Correlation between Suppuration and QoL | |||
|---|---|---|---|---|---|---|
| Assessment Tool | Score | Assessment Tool | Score | |||
| Cuenca-Barrales et al. Spain. 2019 [25] | NRS | 6.48 ± 3.18 | NRS for HS impact on sex life | 7.24 ± 2.77 in women and 6.39 ± 3.44 in men | β = 0.05, p = 0.489 ** | |
| Cuenca-Barrales and Molina-Leyva. Spain. 2020 [24] | NRS | Women: 6.39 ± 3.21 | Prevalence of sexual dysfunction | FSFI-6 ≤ 19 | 51% (156) | β = NS, p = 0.29 ** |
| Men: 6.48 ± 3.04 | IIEF-5 ≤ 21 | 60% (48) | β =NS, p = 0.98 ** | |||
| Machado et al. Canada. 2021 [38] | HODS-drainage: | NS | Skindex-29 | NS | r = 0.614, p < 0.05 ^ | |
| Skindex-29 symptoms | NS | r = 0.619, p < 0.05 ^ | ||||
| Skindex-29 emotional | NS | r = 0.616, p < 0.05 ^ | ||||
| Skindex-29 functioning | NS | r = 0.605, p < 0.05 ^ | ||||
| HS-QoL overall | NS | r = 0.745, p < 0.05 ^ | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montero-Vilchez, T.; Diaz-Calvillo, P.; Rodriguez-Pozo, J.-A.; Cuenca-Barrales, C.; Martinez-Lopez, A.; Arias-Santiago, S.; Molina-Leyva, A. The Burden of Hidradenitis Suppurativa Signs and Symptoms in Quality of Life: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6709. https://doi.org/10.3390/ijerph18136709
Montero-Vilchez T, Diaz-Calvillo P, Rodriguez-Pozo J-A, Cuenca-Barrales C, Martinez-Lopez A, Arias-Santiago S, Molina-Leyva A. The Burden of Hidradenitis Suppurativa Signs and Symptoms in Quality of Life: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(13):6709. https://doi.org/10.3390/ijerph18136709
Chicago/Turabian StyleMontero-Vilchez, Trinidad, Pablo Diaz-Calvillo, Juan-Angel Rodriguez-Pozo, Carlos Cuenca-Barrales, Antonio Martinez-Lopez, Salvador Arias-Santiago, and Alejandro Molina-Leyva. 2021. "The Burden of Hidradenitis Suppurativa Signs and Symptoms in Quality of Life: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 13: 6709. https://doi.org/10.3390/ijerph18136709