
Impact of COVID-19 on the Health of the General and More Vulnerable Population and Its Determinants: Health Care and Social Survey–ESSOC, Study Protocol


 ,
,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
1.1. Background
- COVID-19
- impact on ethnic minorities
- COVID-19
- impact on people with chronic diseases
- COVID-19
- impact on elderly population
1.2. The ESSOC Study Framework
1.3. Hypotheses
- Perceptions of general health, mental health, and emotional well-being could have deteriorated in the short- (one year) and mid-term (three years) since the beginning of the pandemic, with a greater impact perhaps being observed in women, young people, and those diagnosed with COVID-19.
- The socioeconomic, psychosocial, behavioural, occupational, environmental, and clinical determinants of health could have deteriorated since the onset of the pandemic.
- Health inequalities may have increased along the axes of social class, gender, age, ethnicity, and territory as a result of COVID-19, and may be even greater in the mid-term compared with the short-term.
- Chronicity and resulting disability may have increased significantly since the beginning of the pandemic.
- Since the beginning of the pandemic, the care burden has increased significantly for women in the short-term and this might have had a highly negative impact on their health and well-being.
- Social and emotional support in the population aged over 55 years might have decreased significantly since the beginning of the pandemic, with the greatest differences perhaps being observed in single-person households in urban areas.
1.4. Objectives
- To determine the short- and mid-term impact of the COVID-19 pandemic on the health and emotional well-being of the general population of Andalusia.
- To analyse the evolution of the socioeconomic, psychosocial, behavioural, clinical, and environmental determinants of health in the context of the COVID-19 pandemic in the population under study.
- To identify health inequalities along the axes of social class, gender, age, ethnicity, and territory, and their evolution in the context of the COVID-19 pandemic.
- To evaluate different research sampling techniques to improve the reliability and precision of estimates obtained through surveys using longitudinal designs.
2. Materials and Methods
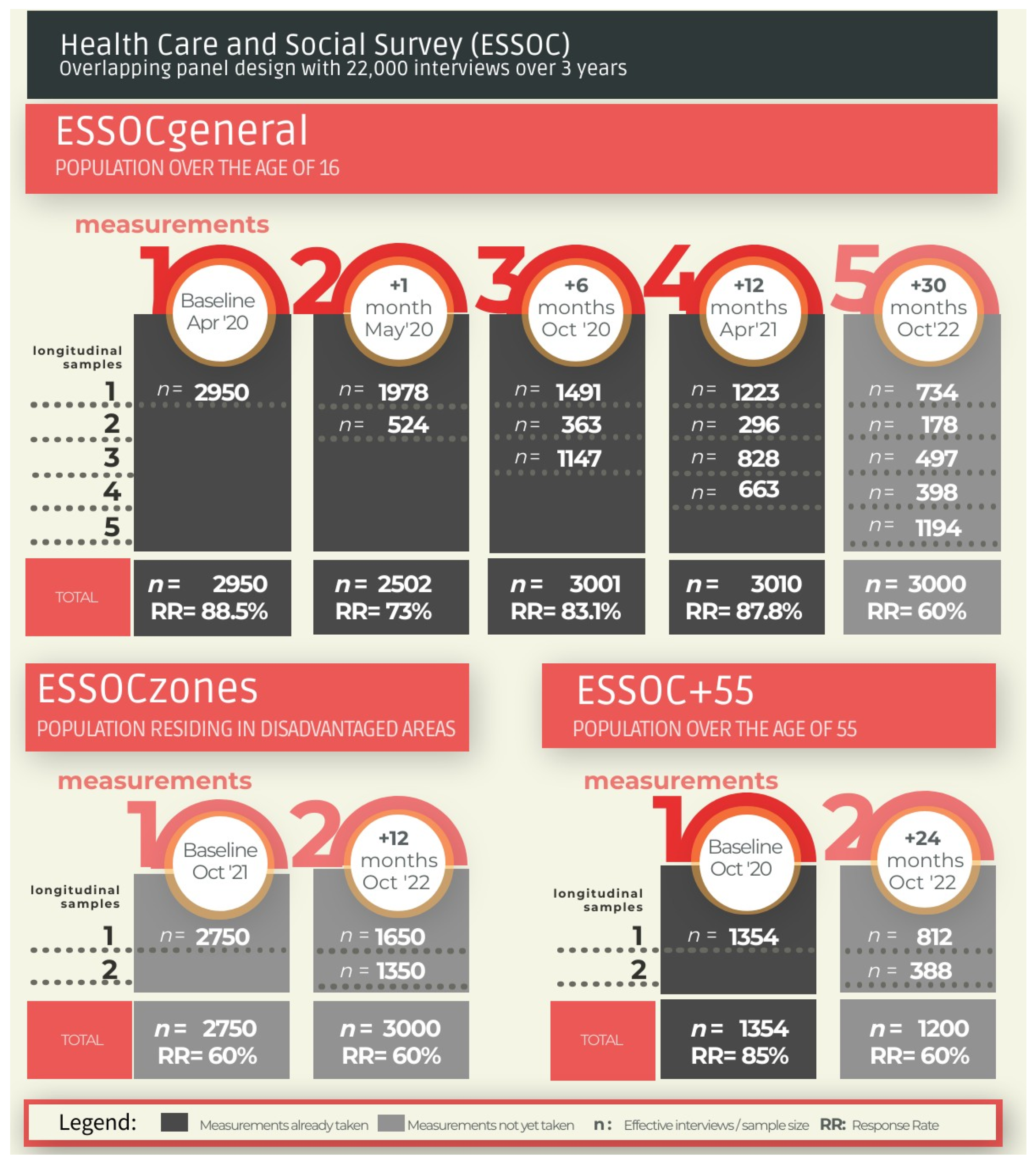
2.1. Study Design
2.2. Geographical, Population, and Temporal Scopes
2.3. Sampling Frame
2.4. Sample Size
- from the sampling frame (e.g., incorrect or unreachable telephone number, or person residing in a place other than the one selected);
- when conducting the interview (e.g., person who cannot be reached, appointment outside the fieldwork time, or insufficient number of attempts to finish the fieldwork, that is, most would be cases that would have answered the interview if it had been extended to the end of the fieldwork);
- leaving the cohort (e.g., deceased, long-term hospital admissions, change of residence etc.).
2.5. Sample Selection and Sample Allocation
2.6. Fieldwork
2.7. Quality Control
2.8. Sampling Weights
2.9. Variables
2.10. Data Analysis
2.11. Data Management Plan
3. Discussion
- institutional alliances of great social value between the public administration, health care services, and the scientific and academic community;
- large, integrated, quality, and open databases containing information extracted from clinical and non-clinical population registries; data concerning social, economic, and environmental contexts and the perception of the population, along with foreseeing the future incorporation of genomic information [90];
- the systematic review throughout the entire project of the scientific evidence obtained through this type of study;
- training with a view to transmitting the available knowledge and increasing capacities and skills in designs, sources, and methodologies;
- measuring the short- and mid-term impact of COVID-19 at different times and on different populations since the beginning of the official State of Alarm.
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BDLPA | Longitudinal Andalusian Population Database |
| BDU | User Database from the Andalusian Health Survey |
| BPS | Andalusian Population Health Database |
| CIBERESP | Network Biomedical Research Centre of Epidemiology and Public Health |
| CSyF | Department of Health and Families of the Andalusian Regional Government |
| DPIA | Data Protection Impact Assessment |
| EASP | Andalusian School of Public Health |
| ESSOC | Health Care and Social Survey |
| IECA | Andalusian Institute of Statistics and Cartography |
| MNP | Natural Movement of the Population |
| REDIAM | Andalusian Environmental Information Network |
| RWD | Real-World Data |
| SVEA | Andalusian Epidemiological Surveillance System |
References
- Department of Social Policy and Intervention. University of Oxford Surveys|Oxford Supertracker. The Global Directory for COVID Policy Trackers and Surveys. Available online: https://supertracker.spi.ox.ac.uk/surveys/ (accessed on 25 March 2021).
- MRC C for G.I.D.A. COVID-19 Reports|Faculty of Medicine|Imperial College London. Available online: http://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/covid-19-reports/ (accessed on 14 March 2021).
- ISCIII. EpiGraph—COVID-19 Simulator. Available online: https://www.arcos.inf.uc3m.es/epigraph/ (accessed on 14 March 2021).
- IECA. Portal IECA sobre el COVID19 en Andalucía. Datos Sanitarios|Instituto de Estadística y Cartografía de Andalucía. Available online: http://www.juntadeandalucia.es/institutodeestadisticaycartografia/salud/datosSanitarios.html (accessed on 14 March 2021).
- Prieto-Alhambra, D.; Balló, E.; Coma, E.; Mora, N.; Aragón, M.; Prats-Uribe, A.; Fina-Aviles, F.; Benítez, M.; Guiriguet, C.; Fàbregas, M.; et al. Hospitalization and 30-day fatality in 121,263 COVID-19 outpatient cases. medRxiv 2020. [Google Scholar] [CrossRef]
- Burn, E.; You, S.C.; Sena, A.G.; Kostka, K.; Abedtash, H.; Abrahão, M.T.F.; Alberga, A.; Alghoul, H.; Alser, O.; Alshammari, T.M.; et al. Deep phenotyping of 34,128 patients hospitalised with COVID-19 and a comparison with 81,596 influenza patients in America, Europe and Asia: An international network study. medRxiv 2020, 21, 26. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Orte, C.; Sánchez-Prieto, L.; Domínguez, D.C.; Barrientos-Báez, A. Evaluation of Distress and Risk Perception Associated with COVID-19 in Vulnerable Groups. Int. J. Environ. Res. Public Health 2020, 17, 9207. [Google Scholar] [CrossRef]
- Rose, T.C.; Mason, K.; Pennington, A.; McHale, P.; Buchan, I.; Taylor-Robinson, D.C.; Barr, B. Inequalities in COVID19 mortality related to ethnicity and socioeconomic deprivation. medRxiv 2020. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain. Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Ministerio de la Presidencia, R. con las C. y M.D. Real Decreto 463/2020. Available online: https://boe.es/buscar/pdf/2020/BOE-A-2020-3692-consolidado.pdf (accessed on 3 March 2021).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Jeong, H.; Yim, H.W.; Song, Y.J.; Ki, M.; Min, J.A.; Cho, J.; Chae, J.H. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol. Health 2016, 38, e2016048. [Google Scholar] [CrossRef]
- Ricci-Cabello, I.; Meneses-Echavez, J.F.; Serrano-Ripoll, M.J.; Fraile-Navarro, D.; de Roque, M.A.F.; Moreno, G.P.; Castro, A.; Ruiz-Pérez, I.; Campos, R.Z.; Gonçalves-Bradley, D. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review. medRxiv 2020, 4. [Google Scholar] [CrossRef]
- Armitage, R.; Nellums, L.B. COVID-19 and the consequences of isolating the elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef] [Green Version]
- Luo, M.; Guo, L.; Yu, M.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain. Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Drosten, C. Entrevista Christian Drosten. Eldiazrio.es 2020. Available online: https://www.eldiario.es/internacional/theguardian/christian-drosten-principal-coronavirus-hundiendo_128_5948822.html (accessed on 14 March 2021).
- Fundación Secretariado Gitano Encuesta Impacto Social de la COVID-19. 2020. Available online: https://www.gitanos.org/actualidad/archivo/131067.html (accessed on 14 March 2021).
- Federación de Asociaciones de Mujeres Gitanas Informe Antigitanismo y COVID 19. Available online: https://fakali.org/wp-content/uploads/2020/12/Informe-FAKALI-Antigitanismo-y-Covid-19.pdf (accessed on 14 March 2021).
- Vallejo-Slocker, L.; Fresneda, J.; Vallejo, M.A. Psychological wellbeing of vulnerable children during the COVID-19 pandemic. Psicothema 2020, 32, 501–507. [Google Scholar] [CrossRef]
- Prats-Uribe, A.; Paredes, R.; Prieto-Alhambra, D. Ethnicity, comorbidity, socioeconomic status, and their associations with COVID-19 infection in England: A cohort analysis of UK Biobank data. medRxiv 2020. [Google Scholar] [CrossRef]
- Guijarro, C.; Pérez-Fernández, E.; González-Piñeiro, B.; Meléndez, V.; Goyanes, M.J.; Renilla, M.E.; Casas, M.L.; Sastre, I.; Velasco, M.; Algora, A.; et al. Differential risk for COVID-19 in the first wave of the disease among Spaniards and migrants from different areas of the world living in Spain. Rev. Clin. Esp. 2020. [Google Scholar] [CrossRef]
- Platt, L.; Warwick, R. Are Some Ethnic Groups More Vulnerable to COVID-19 Than Others? Inequality: The IFS Deaton Review 2020. Available online: https://www.ifs.org.uk/inequality/chapter/are-some-ethnic-groups-more-vulnerable-to-covid-19-than-others/ (accessed on 11 April 2021).
- Ruiz-Azarola, A.; Carretero, M.E.; López-Fernández, L.A.; García, E.G.; Cerdà, J.C.M.; Jaramillo, D.L. The perspective of migrants on access to health care in the context of austerity policies in Andalusia. Gac. Sanit. 2020, 34, 261–267. [Google Scholar] [CrossRef]
- Holt, E. COVID-19 lockdown of Roma settlements in Slovakia. Lancet. Infect. Dis. 2020, 20, 659. [Google Scholar] [CrossRef]
- Blanco, E.C.; Manzanares, I.; Centeno, M.; Khawaja, M.; Betrán, O.; Donaire, A.; Carreño, M. Epilepsy and lockdown: A survey of patients normally attending a Spanish centre. Acta Neurol. Scand. 2021, 143, 206–209. [Google Scholar] [CrossRef]
- López-Bravo, A.; García-Azorín, D.; Belvís, R.; González-Oria, C.; Latorre, G.; Santos-Lasaosa, S.; Guerrero-Peral, L. Impact of the COVID-19 pandemic on headache management in Spain: An analysis of the current situation and future perspectives. Neurologia 2020, 35, 372–380. [Google Scholar] [CrossRef]
- Lara, B.; Carnes, A.; Dakterzada, F.; Benitez, I.; Piñol-Ripoll, G. Neuropsychiatric symptoms and quality of life in Spanish patients with Alzheimer’s disease during the COVID-19 lockdown. Eur. J. Neurol. 2020, 27, 1744–1747. [Google Scholar] [CrossRef]
- Elbarbary, N.S.; dos Santos, T.J.; de Beaufort, C.; Agwu, J.C.; Calliari, L.E.; Scaramuzza, A.E. COVID-19 outbreak and pediatric diabetes: Perceptions of health care professionals worldwide. Pediatr. Diabetes 2020, 21, 1083–1092. [Google Scholar] [CrossRef]
- Pleguezuelos, E.; Del Carmen, A.; Moreno, E.; Ortega, P.; Vila, X.; Ovejero, L.; Serra-Prat, M.; Palomera, E.; Garnacho-Castaño, M.V.; Loeb, E.; et al. The experience of COPD patients in lockdown due to the COVID-19 pandemic. Int. J. COPD 2020, 15, 2621–2627. [Google Scholar] [CrossRef]
- Beisani, M.; Vilallonga, R.; Petrola, C.; Acosta, A.; Casimiro Pérez, J.A.; de Gordejuela, A.G.R.; Quesada, C.F.; Gonzalez, O.; de Tudela, A.C.; Caubet, E.; et al. Effects of COVID-19 lockdown on a bariatric surgery waiting list cohort and its influence in surgical risk perception. Langenbeck’s Arch. Surg. 2020, 406, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Hartmann-Boyce, J.; Mahtani, K.R. Supporting People with Long-Term Conditions (LTCs) during National Emergencies—The Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/covid-19/supporting-people-with-long-term-conditions-ltcs-during-national-emergencies (accessed on 14 March 2021).
- Prieto, M.; March, J.; Martín, A.; Escudero, M.; López, M.; Luque, N. Repercusiones del Confinamiento Por COVID-19 en Pacientes Crónicos de Andalucía. Available online: https://www.easp.es/web/coronavirusysaludpublica/pacientes-cronicos-en-casa-la-experiencia-del-confinamiento-como-se-cuidan-que-necesitan-como-apoyarles/ (accessed on 11 April 2021).
- Ministerio de Sanidad. Centro de Coordinación de Alertas y Emergencias Sanitarias. Actualización no 96. Enfermedad por el coronavirus (COVID-19). 05.05.2020 (datos consolidados a las 21:00 horas del 04.05.2020). Situación en España. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_96_COVID-19.pdf (accessed on 15 March 2021).
- Pastor-Barriuso, R.; Pérez-Gómez, B.; Hernán, M.A.; Pérez-Olmeda, M.; Yotti, R.; Oteo-Iglesias, J.; Sanmartín, J.L.; León-Gómez, I.; Fernández-García, A.; Fernández-Navarro, P.; et al. Infection fatality risk for SARS-CoV-2 in community dwelling population of Spain: Nationwide seroepidemiological study. BMJ 2020, 371. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Garg, S.; Kim, L.; Whitaker, M.; O’Halloran, A.; Cummings, C.; Holstein, R.; Prill, M.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; et al. Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019—COVID-NET, 14 States, March 1–30, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 458–464. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in coronavirus disease 2019 patients: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18. [Google Scholar] [CrossRef]
- Pinazo-Hernandis, S. Psychosocial impact of COVID-19 on older people: Problems and challenges. Rev. Esp. Geriatr. Gerontol. 2020, 55, 249–252. [Google Scholar] [CrossRef]
- Losada-Baltar, A.; Martínez-Huertas, J.; Jiménez-Gonzalo, L.; Pedroso-Chaparro, M.; Gallego-Alberto, L.; Fernandes-Pires, J.; Márquez-González, M. Longitudinal Correlates of Loneliness and Psychological Distress During the Lockdown Situation due to COVID-19. Effects of Age and Self-Perceptions of Aging. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2021. [Google Scholar] [CrossRef]
- Arpino, B.; Pasqualini, M.; Bordone, V.; Solé-Auró, A. Older People’s Nonphysical Contacts and Depression During the COVID-19 Lockdown. Gerontologist 2021, 61, 176–186. [Google Scholar] [CrossRef]
- Alonso, J.C.D.; Rivero, J.B.; Puerto, F.V.; de los Rios, J.P.F.; Alba, M.B.C.; Barrios, P.C.; Martín-Lázaro, E.S. Atención al Mayor, Abordaje Multidisciplinar de su Complejidad; Sociedad Andaluza de Geriatria y Gerontología (SAGG): Málaga, Spain, 2019; ISBN 978-84-09-13336-9. (In Spanish) [Google Scholar]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- ISCIII. Estudio Ene-Covid: Informe Final Estudio Nacional De Sero-Epidemiología De La Infección Por Sars-Cov-2 En España. Available online: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736 (accessed on 15 March 2021).
- Cabrera-León, A.; Sánchez-Cantalejo, C. Características y Resultados De Encuestas Sobre El Impacto De La Enfermedad COVID-19|Comprender El COVID-19 Desde Una Perspectiva De Salud Pública. Available online: https://www.easp.es/web/coronavirusysaludpublica/caracteristicas-y-resultados-de-encuestas-sobre-el-impacto-de-la-enfermedad-covid-19/ (accessed on 15 March 2021).
- Mansilla Domínguez, J.M.; Font Jiménez, I.; Belzunegui Eraso, A.; Peña Otero, D.; Díaz Pérez, D.; Recio Vivas, A.M. Risk Perception of COVID−19 Community Transmission among the Spanish Population. Int. J. Environ. Res. Public Health 2020, 17, 8967. [Google Scholar] [CrossRef]
- Kim, J.K.; Wang, Z. Sampling Techniques for Big Data Analysis. Int. Stat. Rev. 2019, 87, S177–S191. [Google Scholar] [CrossRef] [Green Version]
- Cabrera-León, A.; Daponte Codina, A.; Mateo, I.; Arroyo-Borrell, E.; Bartoll, X.; Bravo, M.J.; Domínguez-Berjón, M.F.; Renart, G.; Álvarez-Dardet, C.; Marí-Dell’Olmo, M.; et al. Contextual indicators to assess social determinants of health and the Spanish economic recession. Gac. Sanit. 2017, 31, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Hernán, M.; Robins, J. Causal Inference: What If; Chapman & Hall/CRC: Boca Raton, FL, USA, 2020. [Google Scholar]
- Beaumont, J. Are Probability Surveys Bound to Disappear for the Production of Official Statistics? Available online: https://www150.statcan.gc.ca/n1/pub/12-001-x/2020001/article/00001-eng.htm (accessed on 11 April 2021).
- Burgelman, J.-C.; Pascu, C.; Szkuta, K.; Von Schomberg, R.; Karalopoulos, A.; Repanas, K.; Schouppe, M. Open Science, Open Data, and Open Scholarship: European Policies to Make Science Fit for the Twenty-First Century. Front. Big Data 2019, 2, 43. [Google Scholar] [CrossRef] [Green Version]
- Kalton, G.; Citro, C.F. Panel Surveys: Adding the Fourth Dimension. Innov. Eur. J. Soc. Sci. Res. 1995, 8, 25–39. [Google Scholar] [CrossRef]
- Junta de Andalucía Junta de Andalucía—Zonas Desfavorecidas. Available online: https://www.juntadeandalucia.es/organismos/igualdadpoliticassocialesyconciliacion/areas/inclusion/zonas-transformacion.html (accessed on 30 April 2021).
- Merlo, J.; Viciana-Fernández, F.J.; Ramiro-Fariñas, D. Bringing the individual back to small-area variation studies: A multilevel analysis of all-cause mortality in Andalusia, Spain. Soc. Sci. Med. 2012, 75, 1477–1487. [Google Scholar] [CrossRef] [Green Version]
- IECA. Base de Datos Longitudinal de Población de Andalucía 2018. Available online: https://www.juntadeandalucia.es/institutodeestadisticaycartografia/metodologias/IME010101.pdf (accessed on 15 March 2021).
- Junta de Andalucía, C. de S. y F. Base de Datos de Usuarios del Sistema Sanitario Público de Andalucía 2018. Available online: https://www.juntadeandalucia.es/organismos/saludyfamilias/servicios/estadistica-cartografia/actividad/detalle/175259.html (accessed on 15 March 2021).
- Consorcio Fernando de los Ríos Guadalinfo. Available online: http://www.guadalinfo.es/ (accessed on 15 March 2021).
- Junta de Andalucía. Estrategia Regional Andaluza Para La Cohesión E Inclusión Social. Available online: https://www.juntadeandalucia.es/export/drupaljda/ESTRATEGIA_ZONAS_2018_01_24.pdf (accessed on 28 July 2021).
- IECA. Clasificación del Grado de Urbanización|Instituto de Estadística y Cartografía de Andalucía. Available online: http://www.juntadeandalucia.es/institutodeestadisticaycartografia/gradourbanizacion/index.htm (accessed on 15 March 2021).
- Singh, S. Advanced Sampling Theory with Applications; Springer Science & Business Media: St. Cloud, MN, USA, 2003. [Google Scholar]
- Yves Tillé, A.; Matei, A.; Alina Matei, M. Package “Sampling” Title Survey Sampling. 2021. Available online: https://cran.r-project.org/web/packages/sampling/sampling.pdf (accessed on 28 July 2021).
- INE. La Encuesta Continua de Hogares 2019. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176952&menu=ultiDatos&idp=1254735572981 (accessed on 15 March 2021).
- Plewis, I. Non-response in a birth cohort study: The case of the millennium cohort study. Int. J. Soc. Res. Methodol. 2007, 10, 325–334. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco CA, USA, 13–17 August 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 785–794. [Google Scholar] [CrossRef] [Green Version]
- Kott, P.S.; Liao, D. One step or two? Calibration weighting from a complete list frame with nonresponse. Stat. Canada 2015, 41, 165–181. [Google Scholar]
- Kott, P.S.; Liao, D. Calibration Weighting for Nonresponse that is Not Missing at Random: Allowing More Calibration than Response-Model Variables. J. Surv. Stat. Methodol. 2017, 5, 159–174. [Google Scholar] [CrossRef]
- Ferri-García, R.; Del Mar Rueda, M. Efficiency of propensity score adjustment and calibration on the estimation from non-probabilistic online surveys. SORT 2018, 42, 159–182. [Google Scholar] [CrossRef]
- Ferri-García, R.; Rueda, M.D.M. Propensity score adjustment using machine learning classification algorithms to control selection bias in online surveys. PLoS ONE 2020, 15, e0231500. [Google Scholar] [CrossRef] [PubMed]
- Servicio Andaluz de Salud Base poblacional de Salud|Servicio Andaluz de Salud. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/profesionales/sistemas-de-informacion/base-poblacional-de-salud (accessed on 15 March 2021).
- Consejeria De Medioambiente. Junta de Andalucía REDIAM|IDEAndalucia. Available online: https://www.ideandalucia.es/portal/nodo-rediam (accessed on 25 March 2021).
- Consejería de Salud y Familias. Junta de Andalucía. Programas de Vigilancia de Enfermedades Transmisibles. Available online: https://www.juntadeandalucia.es/organismos/saludyfamilias/areas/salud-vida/vigilancia/paginas/vigilancia-transmisibles.html (accessed on 25 March 2021).
- Servicio Andaluz de Salud. Documento de identificacion de patologias crónicas de la BPS. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/sites/default/files/sincfiles/wsas-media-mediafile_sasdocumento/2019/patologias_bps.pdf (accessed on 15 March 2021).
- Bericat, E.; Excluidos de la Felicidad. Las Desigualdades de Bienestar Emocional en España y Europa 2015. Available online: https://www.researchgate.net/publication/287814426_EXCLUIDOS_DE_LA_FELICIDAD_Las_desigualdades_de_bienestar_emocional_en_Espana_y_Europa (accessed on 15 March 2021).
- Bellón, J.; Delgado, A.; Luna, J.; Lardelli, P. Validez y fiabilidad del cuestionario de apoyo social funcional Duke-UNC-11. Aten Primaria 1996, 18, 153–163. [Google Scholar]
- Broadhead, W.E.; Gehlbach, S.H.; de Gruy, F.V.; Kaplan, B.H. The Duke-UNC functional social support questionnaire: Measurement of social support in family medicine patients. Med. Care 1988, 26, 707–721. [Google Scholar] [CrossRef]
- OMS 10 datos sobre la obesidad. Available online: https://www.who.int/features/factfiles/obesity/facts/es/(accessed on 11 June 2021).
- Domingo-Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C. Propuestas de clase social neoweberiana y neomarxista a partir de la Clasificación Nacional de Ocupaciones 2011. Gac. Sanit. 2013, 27, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Chilet-Rosell, E.; Álvarez-Dardet, C.; Domingo-Salvany, A. Utilización de las propuestas espã nolas de medición de la clase social en salud Use of Spanish proposals for measuring social class in health sciences. Gac Sanit 2012, 26, 566–569. [Google Scholar] [CrossRef]
- R Core Team. R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 15 March 2021).
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Rue, H.; Riebler, A.; Sørbye, S.H.; Illian, J.B.; Simpson, D.P.; Lindgren, F.K. Bayesian Computing with INLA: A Review. Annu. Rev. Stat. Its Appl. 2017, 4, 395–421. [Google Scholar] [CrossRef] [Green Version]
- Simpson, D.; Rue, H.; Riebler, A.; Martins, T.G.; Sørbye, S.H. Penalising model component complexity: A principled, practical approach to constructing priors. Stat. Sci. 2017, 32, 1–28. [Google Scholar] [CrossRef]
- R-INLA Project. Available online: https://www.r-inla.org/home (accessed on 15 March 2021).
- Welcome to Python.org. Available online: https://www.python.org/ (accessed on 15 March 2021).
- Agencia Española de Protección de Datos Guía práctica para LAS Evaluaciones de Impacto en la Protección de LOS datos sujetas al RGPD. Available online: https://www.aepd.es/sites/default/files/2019-09/guia-evaluaciones-de-impacto-rgpd.pdf (accessed on 15 March 2021).
- European Commission Horizon 2020 Programme Guidance How to Complete Your Ethics Self-Assessment. 2019. Available online: https://ec.europa.eu/research/participants/data/ref/h2020/grants_manual/hi/ethics/h2020_hi_ethics-self-assess_en.pdf (accessed on 15 March 2021).
- Agencia Española de Protección de Datos Herramienta GESTIONA EIPD. Available online: https://gestiona.aepd.es/ (accessed on 15 March 2021).
- Consejería de Salud y Familias. Junta de Andalucía. Sistema Integrado de Epidemiología Genómica de Andalucía. Available online: https://www.juntadeandalucia.es/organismos/saludyfamilias/areas/seguridad-alimentaria/salud-alimentos/paginas/siega.html (accessed on 26 March 2021).


{kind=link}
| Focus | Design | Dissemination | Management |
|---|---|---|---|
| Public Health | Real-World Data | Open Science | Collaborative and Multidisciplinary Research |
| Community participation to obtain information on people’s health and quality of life to be able to intervene both individually and collectively in the face of the pandemic | Integration of observational data extracted from multiple sources from different perspectives based on probabilistic samples and administrative registries | Results, methodologies, processes, and collected data distributed, reused, and freely and openly accessible | Andalusian School of Public Health, Andalusian Health Service, Department of Health and Families (Andalusian Regional Government), Universities of Granada and Girona, Andalusian Institute of Statistics and Cartography and Guadalinfo Network |
| Incidence | Incidence | Description | Protocol |
|---|---|---|---|
| Frame incidence (reasons that make it impossible to complete the survey due to problems related to the sampling frame; for example, a telephone number with which to contact the sample person could not be obtained or the housing frame was not sufficiently up to date). | The telephone number does not exist. | Wrong number: the telephone number dialled does not exist, corresponds to a fax, or has restricted calls. | Direct removal. |
| Not contactable. | Out-of-date frame: the selected person is living in a different municipality, a telephone frame without a telephone number, a person unreachable through the telephone number/home address provided due to circumstances such as death, divorce/separation, etc. | Direct removal. | |
| Relationship-situation incidences (reasons that make it impossible to complete the survey due to several types of situations affecting the surveyed people, for instance, they cannot be located, they refuse to participate in the survey, or any other aspect that prevents the survey being conducted). | No contact. | The household cannot be contacted (e.g., nobody answers the telephone, or the answering machine goes off). | Removal after four attempts performed on two different days, at two different times. |
| Absent. | The selected person cannot be contacted. | Removal after four attempts performed on two different days and at two different times. | |
| Inability to answer. | The selected person cannot complete the survey due to an inability to respond to it because of disability, age, illness, lack of knowledge of the language, or any other circumstance. If possible, the survey should be completed by a close relative. | Direct removal. | |
| Refusal. | The selected person refuses to complete the survey or refuses to continue it after it has begun. | Direct removal. |
| Type of Adjustment | ||
|---|---|---|
| Sample Type (Effective) | 1st Phase | 2nd Phase |
| New | Non-response adjusted by proxy based on the effective sample size in each stratum. | Representativeness by truncated linear calibration with 0.1 and 10 limits based on the auxiliary variables |
| Longitudinal | Non-response adjusted using an XGBoost model based on variables from the previous measurement. | |
| Registry | Description | Information | Variables Extracted |
|---|---|---|---|
| BDLPA–Longitudinal Andalusian Population Database [71] | Information from the census coordination system and civil registries that give rise to a consolidated framework of the Andalusian population | Personal data | Name, surname, identification health number (NUHSA), geographical coordinates |
| BDU–User Database of the Andalusian Public Health Care System [58] | Contact Information of the Andalusian Public Health Care System | Personal contact information | Telephone numbers |
| BPS–Andalusian Population Health Database [71] | Personal health information from the Andalusian Population Health Database and Health care information | Health and health care information | Chronic diseases, functional and cognitive assessments, health resources (volume and cost), population stratification, drugs consumed |
| REDIAM–Andalusian Environmental Information Network [72] | Daily averages by collecting/meteorological station and at the census section level | Pollution, temperature | Mean daily values from pollution, air quality and temperature |
| SVEA–Andalusian Epidemiological Surveillance System [73] | Functional organisation for health surveillance that collects, among other things, epidemiological information related to SARS-COV-2 infection | Epidemiological information of COVID-19 | PCR results, symptoms’ date, close contact, health care professional, hospitalisation unit (specifying ICU), date of admission and discharge, need of mechanical ventilation and clinical data |
| Subject Area | 1st Measurement (M1) | 2nd Measurement (M2) | 3rd Measurement (M3) | 4th and 5th Measurements (M4 and M5) |
|---|---|---|---|---|
| Household and housing characteristics | Municipality, usual household, type of household, surface area, facilities, household changes, number of cohabitants (<6/<16/>60), type of household, and equipment. | Municipality, usual household, type of household, surface area, facilities, household changes b, number of cohabitants (<6/<16/>60), equipment, number of rooms, and number of inhabitants with disabilities or requiring care. | Municipality, usual household, type of household, surface area, household changes, number of cohabitants (<6/<16/>60), number of rooms, and number of inhabitants with disabilities or requiring care. | Municipality, usual household, type of household, surface area, household changes, number of cohabitants (<6/<16/>60), number of rooms, and number of inhabitants with disabilities or requiring care. |
| Time use and cohabitation | Household chores, care tasks, daily activities during the confinement period (at home and outside), cohabitation and relationships, and causes for optimism. | Household chores, care tasks, daily activities b during the confinement period (at home and outside), cohabitation and relationships, and causes for optimism. | ||
| Health and emotional well-being | COVID-19 diagnosis, severity, diagnosis within the person’s settings, self-perception of general and mental health (current and last year), emotional well-being c, difficulty to withstand the confinement, malaise, chronic illness, and change of medication. | COVID-19 diagnosis, severity, diagnostic tests, diagnosis within the person’s settings, self-perception of general and mental health, emotional well-being b, cohabitation, difficulty to withstand the confinement, happiness, social and emotional support c, malaise b, chronic diseases (suffering and limitations), and medication (use and change of use b). | COVID-19 diagnosis b, severity, diagnostic tests, diagnosis within the person’s settings, self-perception of general and mental health, emotional well-being b,c, happiness, social and emotional support b,c, malaise b, chronic diseases (suffering and limitations), and medication (use and change of use b). | COVID-19 diagnosis b, severity, diagnostic tests, diagnosis within the person’s settings, self-perception of general and mental health, emotional well-being b,c, happiness, social and emotional support b,c, malaise b, chronic diseases (suffering and limitations), and medication (use and change of use b). |
| Habits and lifestyle | Habit modification (exercising, smoking, alcohol consumption, sleep, and diet). | Habit modification b: exercising, drinking, smoking, sleep, food, daily intake of vegetables and fruit, exercising, weight and height c, smoking, alcohol consumption, sleep, and flu vaccination. | Habit modification b: exercising, drinking, smoking, sleep, food, daily intake of vegetables and fruit, exercising, weight and height c, smoking, alcohol consumption, sleep, and flu vaccination b. | Habit modification b: exercising, drinking, smoking, sleep, food, daily intake of vegetables and fruit, exercising, weight and height c, smoking, alcohol consumption, sleep, and flu and COVID-19 vaccination b. |
| Economic situation and socio-demographic characteristics | Educational level, employment situation, working from home, type of contract, occupation c, cohabitation with a partner, identification of the cohabitant with the greater income (educational level, employment situation, type of contract, occupation), difficulty in making ends meet, late payments, income, future worries, and degree of confidence in public institutions. | Employment situation, educational level, occupation c, development b, ability to work, identification of the cohabitant with the greater income (educational level, employment situation, occupation), difficulty in making ends meet, late payments, change in economic situation, parents’ educational level, and future worries. | Employment situation, educational level, occupation c, development, ability to work, identification of the cohabitant with the greater income (educational level, employment situation, occupation), difficulty in making ends meet, late payments b, change in economic situation, parents’ educational level, and future worries. | Employment situation, educational level, occupation c, development, ability to work, identification of the cohabitant with the greater income (educational level, employment situation, occupation), difficulty in making ends meet, late payments b, change in economic situation, parents’ educational level, and future worries. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Cantalejo, C.; Rueda, M.d.M.; Saez, M.; Enrique, I.; Ferri, R.; Fuente, M.d.L.; Villegas, R.; Castro, L.; Barceló, M.A.; Daponte-Codina, A.; et al. Impact of COVID-19 on the Health of the General and More Vulnerable Population and Its Determinants: Health Care and Social Survey–ESSOC, Study Protocol. Int. J. Environ. Res. Public Health 2021, 18, 8120. https://doi.org/10.3390/ijerph18158120
Sánchez-Cantalejo C, Rueda MdM, Saez M, Enrique I, Ferri R, Fuente MdL, Villegas R, Castro L, Barceló MA, Daponte-Codina A, et al. Impact of COVID-19 on the Health of the General and More Vulnerable Population and Its Determinants: Health Care and Social Survey–ESSOC, Study Protocol. International Journal of Environmental Research and Public Health. 2021; 18(15):8120. https://doi.org/10.3390/ijerph18158120
Chicago/Turabian StyleSánchez-Cantalejo, Carmen, María del Mar Rueda, Marc Saez, Iria Enrique, Ramón Ferri, Miguel de La Fuente, Román Villegas, Luis Castro, Maria Antònia Barceló, Antonio Daponte-Codina, and et al. 2021. "Impact of COVID-19 on the Health of the General and More Vulnerable Population and Its Determinants: Health Care and Social Survey–ESSOC, Study Protocol" International Journal of Environmental Research and Public Health 18, no. 15: 8120. https://doi.org/10.3390/ijerph18158120