
The Role of Acceptance and Commitment Therapy in Cardiovascular and Diabetes Healthcare: A Scoping Review

 , , , ,
, , , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
2.2. Study Selection and Inclusion Criteria
2.3. Quality Appraisal and Data Extraction
2.4. Data Synthesis
3. Results
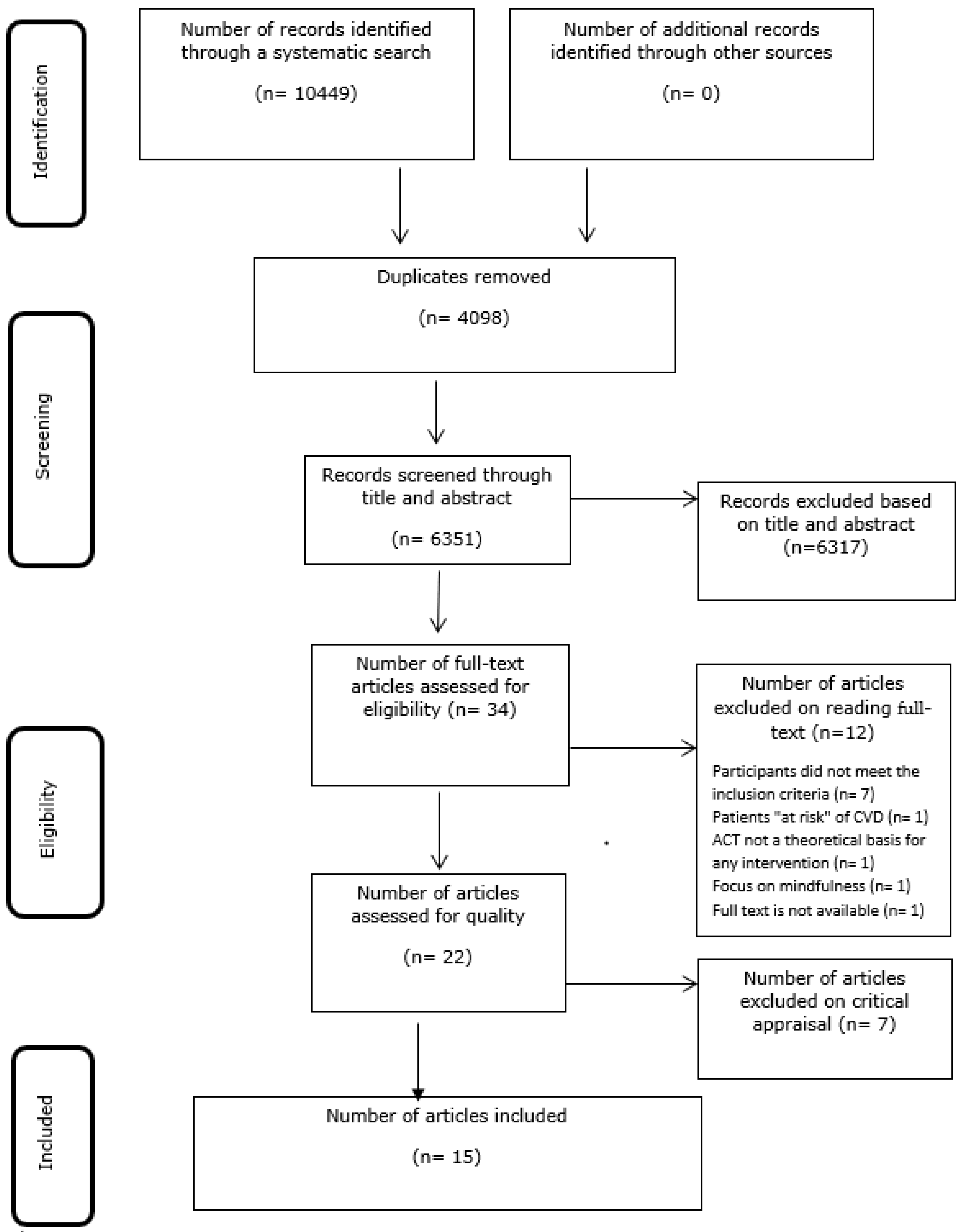
3.1. Study Inclusion
3.2. Characteristics of Included Studies
3.3. Methodological Quality of Included Studies
3.4. Review Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Country | Study | Study Design & Setting | Participants Characteristics Sample Size | Intervention & Another Comparator | Intervention Delivered By | Intervention Description | Outcomes Measured | Intervention Frequency and Duration | Description Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Iran | Aghayosefi (2018) [20] | Quasi-experimental Diabetes centre (community) | n = 40 T2DM Mean age 36.9 years (range 22–55),and 10% of participants had Master degree | Control vs. ACT case group | Unclear | Group ACT Familiarity and communication between members, familiarity with meaning based on cognitive flexibility, understanding of languages, recognizing performance, openness and receptivity, consciousness, values and use of the acceptance of the recipient | Stress Quality of life Coping strategies | 8 sessions and the duration not reported | Significant differences between I vs. C in post-test mean scores of problem-and emotion-oriented coping strategies and stress (p < 0.010). No significant differences in QoL between I vs. C |
| Iran | Ahmadsaraei (2017) [31] | Quasi experimental Community | n = 40 T2DM with DSM-IV and BDI-diagnosed depression. Patients were diagnosed with depression if they scored 29–63 based on a Structured Clinical Interview according to DSM-IV and BDI-criteria. | Control vs ACT | Unclear | Group ACT Education, information and the limits of control, values. cognitive diffusion, mindfulness, committed action, review and continued action in support of values | Depression | 8 sessions 2 h per session | Mean BDI scores: ACT group Baseline 30.70 at 3-month FU 21.84 (p = 0.001) Comparator group Baseline 31.45, 3-month FU 30.95 (p = 0.75) Significant between group difference in BDI at 3-months only (p = 0.001) |
| Iran | Ahmadsaraei (2016) [21] | Quasi experimental Community | n = 40 T2DM aged 45–60 years Mean age: Intervention group 44.4 Control group 41.2 | Control vs ACT n = 20 per group | Unclear | Group ACT Creator helplessness, separation of physical illness from the whole process of life, focus on the whole life and not just the disease process. emotion control and disease and conclusions | Quality of life | 8 sessions 2 h per session | No significant difference between groups. |
| Iran | Amiri (2019) [22] | Experimental (pre- & post-test) Hospital. | n = 40 CHD 100% male Mean age 43 (20 treatment, 20 control) | Control vs. ACT n = 20 per group | Unclear | Group ACT Admission, separation of physical illness from the whole process of life, consciousness, openness and receptivity values committed action | Perceived stress | 8 sessions 1.5 h per session | ACT significantly reduced stress (p < 0.001) Mean (SD) pre– & post-test scores: Intervention: 31.75 (7.60) and 29.07 (6.33), respectively. Control: 22.21 (6.8) and 31.56 (7.5) |
| Iran | Amiri (2017) [32] | Quasi-experimental Community | n = 30 CHD and angina aged 45–70 30% female | Control vs. ACT n = 15 per group | Not reported | Not reported | Psychological, social, and spiritual health | Number of sessions and duration not clear | Significant difference between groups in psychological, social, and spiritual health |
| USA | Gregg (2007) [33] | RCT Community | n = 81 T2DM for ≥5 years 51.9% male 32.6% Caucasian, 53.5% married 25.6% unemployed | Education vs. ACT plus education | Group-based ACT manual | Session manual available at http://www.psych.sjsu.edu/jgregg | HbA1C, self-management and understanding of diabetes and satisfaction with treatment | One day workshop 7 h duration | After 3 months, ACT plus education group more likely to use coping strategies, report better diabetes self-care, and have HbA1C values within target compared to education alone. |
| Iran | Hor (2018) [23] | Quasi-experimental Community | n = 45 T2DM ≥ 1 post-diagnosis aged 46–60 years 100% female most middle school education | Health lifestyle with ACT vs. Mindfulness-based therapy group vs. control | Not reported | Group ACT Introduction, familiarity with the first stage of health lifestyle, familiarity with self-observation, cognitive faulting, clarifying the values, mindfulness lifestyle, increase happiness and spirituality, improving health lifestyle and one’s relationship, mental flexibility and increased psychological flexibility | ACT-based healthy lifestyle Mindfulness-based therapy on self-care and glycated haemoglobin (HbA1C) | 12 sessions 3 h per session | Significant difference between ACT group, mindfulness-based therapy and the control. Significant difference between mindfulness-based therapy and the control. Significant difference between the intervention and control groups in HbA1C |
| Iran | Kaboudi (2017) [34] | Quasi experimental RCT (pre/post test) Community | n = 26 T2DM aged 25–65 years 100% female | Control vs ACT n = 13 each group | Not reported | Group ACT Limits of control, values, cognitive defusion, mindfulness, committed action, self as context, review and continued action in support of values and moving forward | Mental health | 8 sessions 1.5 h per session | At 8 weeks significant improvement in mental health score with ACT |
| Iran | Khashouei (2016) [35] | Quasi-experimental Research Centre | n = 32 T2DM Mean age 48 100% female | Control vs. ACT n = 16 each group | No reported | Not reported | Self-efficacy, perceived stress and resiliency | 8 sessions 1.5 h per session | ACT significantly improved self-efficacy and reduced perceived stress at all stages, and resilience at follow-up |
| Iran | Maghsoudi,(2019) [36] | RCT Community | n = 80 T2DM Mean (SD) age Intervention 62.85 (3.86) Control 63.18 (3.57) 42 (52.5%) male | Control vs. ACT n = 40 each group | Clinical psychologist and nurse | Group ACT Familiarity and creating therapeutic communication, continuing the discussion on the concepts in ACT, acceptance of thoughts, making a distinction between conceptualized self and observing self, discussion on values, the relationship between objectives and performances, identification of obstacles, playing the victim and planning the post-therapy program | Emotional distress | 8 sessions 1.5 h per session | Lower emotional distress in ACT group immediately post-intervention and 2-months later |
| Iran | Mahzooni (2018) [24] | Quasi-experimental Outpatient clinic | n = 26 DM Type I or T2DM (>3 months) 100% female | ACT vs. waiting list control | Not reported | Group ACT Familiarity and communication of members, familiarity with ACT therapeutic concepts, mindfulness training, increasing tolerance, emotion management training, increasing individual and inter-individual efficiency and understand the nature of willingness and commitment | Mental health, anger depression, anxiety, positive affection and emotion control | 8 sessions 1.5 h per session | Significant difference between groups in mean scores on emotion control scale favouring ACT |
| Iran | Shayeghian (2016) [37] | RCT Hospital | n = 106 T2DM (1–10 years duration), no change in D.M. medication for ≥3 months prior Overall mean (S.D.) age: 55.44 (8.44) years 60 (60%) female Mean (S.D.) diabetes duration 4.22 (1.49) years | Education vs education plus ACT | Not reported | Reference to ACT manual adapted for a workshop day (content not explained) | Self-management of T2DM, moderating role of coping styles | 10 sessions 2 h per session | After 3 months, ACT plus education group more likely to use effective coping strategies, report better diabetes self-care, and optimum HbAiC compared to education alone |
| USA | Welch (2014) [38] | Pre- and post-test comparative design. Community | n = 20 T2DM aged 32–53 years 45% Caucasian 70% female, Mean age 42.95 years | Education vs. education plus ACT | Principal investigator- student of a doctorate in psychologyunclear if ACT trained | Group ACT Values, values identification, identifying thought barriers to valued living, begin with a short present moment exercise, emotion, control our feeling, introduce acceptance, commitment to actions and values even with barriers and stand and commit | Acceptance of diabetes, levels of diabetes self-care, diabetes-related distress, depression, anxiety, stress, and thought suppression | One day workshop 8 h duration | No significant differences across all regimen areas following treatment Diabetes-related distress decreased and acceptance increased in ACT group. Thought suppression and depression significantly decreased after ACT |
| New Zealand | Whitehead (2017) [40] | Qualitative Community | n = 27 T2DM aged 43–65 years Mean age 55 years 14 (51.8%) male | Education vs Education plus ACT | Primary care nurses vs. primary care nurse plus mental health nurse with expertise in ACT who received supervision from a clinical psychologist | Group ACT Mindfulness and acceptance training in relation to difficult thoughts and feelings about diabetes, exploration of personal values related to diabetes, and a focus on the ability to act in a valued direction while contacting difficult experiences | Improved glycaemic control, increased diabetes knowledge, self-management skills and self-efficacy | One day workshop 6.5 h duration | Most reported increase in knowledge in diabetes self-management and increased sense of personal responsibility Improvements in self-management activities and reflection on challenges in instigating and maintaining change to improve diabetes management |
| New Zealand | Whitehead (2017) [39] | RCT Community | n = 118 T2DM aged ≥18 year | Education vs. education plus ACT n = 34 education group n = 39 education plus ACT n = 45 control | Primary care nurses vs primary care nurse plus mental health nurse with expertise in ACT who received supervision from a clinical psychologist | Group ACT Mindfulness and acceptance training in relation to difficult thoughts and feelings about diabetes, exploration of personal values related to diabetes, and a focus on the ability to act in a valued direction while contacting difficult experiences | HbA1c, acceptance of diabetes-related thoughts and feelings, understanding of diabetes, satisfactionwith diabetes management, self-management activities, anxiety and depression | One day workshop 6.5 h duration | Significant reduction in HbA1c in the education intervention group (p = 0.011 [7.48, 8.14]). At 6 months, HbA1c was reduced in both intervention groups HbA1c reduction in 50 participants overall. Twice as many participants in the intervention groups demonstrated an improvement in HbA1C compared to the control group |
References
- World Population Prospects 2019: Highlights; United Nations: New York, NY, USA, 2019; p. 43.
- WHO. World Health Organisation. Cardiovascular Diseases (CVDs) Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 12 December 2020).
- IDF Diabetes Atlas, 9th ed.; International Diabetes Federation, IDF: Brussels, Belgium, 2019.
- Ahmed, B.; Davis, H.T.; Laskey, W.K. In-Hospital Mortality Among Patients with Type 2 Diabetes Mellitus and Acute Myocardial Infarction: Results From the National Inpatient Sample, 2000–2010. J. Am. Hear. Assoc. 2014, 3, e001090. [Google Scholar] [CrossRef] [Green Version]
- Prevention of Cardiovascular Disease: Guidelines for Assessment and Management of Total Cardiovascular Risk; World Health Organization: Switzerland, Geneva, 2007.
- Global Strategy on Diet, Physical Activity and Health; World Health Organization: Switzerland, Geneva, 2004.
- Patel, T.; Umeh, K.; Poole, H.; Vaja, I.; Newson, L. Cultural Identity Conflict Informs Engagement with Self-Management Behaviours for South Asian Patients Living with Type-2 Diabetes: A Critical Interpretative Synthesis of Qualitative Research Studies. Int. J. Environ. Res. Public Health 2021, 18, 2641. [Google Scholar] [CrossRef]
- Pimple, P.; Lima, B.B.; Hammadah, M.; Wilmot, K.; Ramadan, R.; Levantsevych, O.; Sullivan, S.; Kim, J.H.; Kaseer, B.; Shah, A.; et al. Psychological Distress and Subsequent Cardiovascular Events in Individuals with Coronary Artery Disease. J. Am. Hear. Assoc. 2019, 8, e011866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennick, K.; Sturt, J.; Speight, J. What is Diabetes Distress and How Can We Measure it? A Narrative Review and Conceptual Model. J. Diabetes Complicat. 2017, 31, 898–911. [Google Scholar] [CrossRef] [Green Version]
- Perrin, N.E.; Davies, M.J.; Robertson, N.; Snoek, F.J.; Khunti, K. The Prevalence of Diabetes-Specific Emotional Distress in People with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabet. Med. 2017, 34, 1508–1520. [Google Scholar] [CrossRef] [PubMed]
- Moss-Morris, R. Adjusting to Chronic Illness: Time for a Unified Theory. Br. J. Health Psychol. 2013, 18, 681–686. [Google Scholar] [CrossRef]
- Hayes, S.C. Acceptance and Commitment Therapy, Relational Frame Theory, and the Third Wave of Behavioral and Cognitive Therapies. Behav. Ther. 2004, 35, 639–665. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.; Pistorello, J.; Levin, M.E. Acceptance and Commitment Therapy as a Unified Model of Behavior Change. Couns. Psychol. 2012, 40, 976–1002. [Google Scholar] [CrossRef]
- Graham, C.D.; Gouick, J.; Krahé, C.; Gillanders, D. A systematic Review of the Use of Acceptance and Commitment Therapy (ACT) in Chronic Disease and Long-Term Conditions. Clin. Psychol. Rev. 2016, 46, 46–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nes, A.A.; Van Dulmen, S.; Eide, E.; Finset, A.; Kristjánsdóttir Ólöf, B.; Steen, I.S.; Eide, H. The Development and Feasibility of a Web-Based Intervention with Diaries and Situational Feedback via Smartphone to support self-management in patients with diabetes type. Diabetes Res. Clin. Pr. 2012, 97, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Hadlandsmyth, K.; White, K.S.; Nesin, A.E.; Greco, L.A. Proposing an Acceptance and Commitment Therapy Intervention to Promote Improved Diabetes Management in Adolescents: A Treatment Conceptualization. Int. J. Behav. Consult. Ther. 2013, 7, 12–15. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, C.L.; Forman, E.M.; Herbert, J.D.; Butryn, M.L.; Ledley, G.S. A Pilot Study Examining the Initial Effectiveness of a Brief Acceptance-Based Behavior Therapy for Modifying Diet and Physical Activity Among Cardiac Patients. Behav. Modif. 2011, 36, 199–217. [Google Scholar] [CrossRef] [Green Version]
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A Scoping Review of Scoping Reviews: Advancing the Approach and Enhancing the Consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef]
- Hassannezhad, M.; Nejat, H.; Toozandejani, H. Acceptance and Commitment Group Yherapy on Self-care and Life SatisFaction Behaviors in Patients with Type 2 Diabetes. Middle East. J. Disabil. Stud. 2019, 9, 54. [Google Scholar]
- Aghayosefi, A.; Alipour, A.; Rahimi, M.; Abaspour, P. Investigation of the Efficacy of Acceptance and Commitment therapy (ACT) on psychological indices (stress, quality of life, and coping strategies) among the patients with type II diabetes. J. Isfahan Med. Sch. 2018, 35, 1859–1866. [Google Scholar]
- Ahmadsaraei, N.F.; Doost, H.T.N.; Manshaee, G.R.; Nadi, M.A. The Effectiveness of Acceptance and Commitment Therapy on Quality of Life Among Patients with Type 2 Diabetes. Iran. J. Health Educ. Health Promot. 2016, 4, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Amiri, L.; Hatami, M.; Asadi, J.; Ranjbairpoor, T. Acceptance and Commitment (ACT) Therapy on Perceived Stress in Coronary Artery Disease Patients. Middle East. J. Disabil. Stud. 2019, 9, 1–10. [Google Scholar]
- Hor, M.; Aghaei, A.; Abedi, A.; Golparvar, M. Effect of Combined Treatment Package (ACT-based healthy lifestyle) with Mindfulness-based Therapy on Self-care and Glycated hemoglobin in Patients with Diabetes Mellitus Type 2. Islamic Life J. 2018, 2, 65–70. [Google Scholar]
- Mahzooni, M.; Mazaheri, M.; Nikoofar, M. Application of Acceptance and Commitment Therapy for Emotional Control in Type II Diabetic patients. J. Diabetes Nurs. 2018, 7, 877–886. [Google Scholar]
- Rahnama, M.; Sajjadian, I.; Raoufi, A. The Effectiveness of Acceptance and Commitment Therapy on Psychological Distress and Medication Adherence of Coronary Heart Patients. Iran. J. Psychiatr. Nurs. 2017, 5, 34–43. [Google Scholar] [CrossRef]
- Faude-Lang, V.; Hartmann, M.; Schmidt, E.-M.; Humpert, P.; Nawroth, P.; Herzog, W. Acceptance-and Mindfulness-Based Group Intervention in Advanced Type 2 Diabetes Patients: Therapeutic Concept and Practical Experiences. Psychother. Psychosom. Med. Psychol. 2010, 60, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Kuba, K.; Weiflog, G. Acceptance and Commitment Therapy at Chronic Physical Illness. PPmP Psychother. Psychosom. Med. Psychol. 2017, 67, 525–536. [Google Scholar]
- Jackson, J.L.; Kuriyama, A.; Anton, A.; Choi, A.; Fournier, J.-P.; Geier, A.-K.; Jacquerioz, F.; Kogan, D.; Scholcoff, C.; Sun, R. The Accuracy of Google Translate for Abstracting Data from Non–English-Language Trials for Systematic Reviews. Ann. Intern. Med. 2019, 171, 677. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual, 2014th ed.; The Joanna Briggs Institute: Adelaide, Australia.
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without Meta-Analysis (SWiM) in Systematic Reviews: Reporting Guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [Green Version]
- Ahmadsaraei, N.; NeshatDoost, H.T.; Manshaee, G.; Nadi, M. The effectiveness of acceptance and commitment therapy on Depression Among Patients with Type II Diabetes. Iran. J. Diabetes Obes. 2017, 9, 6–13. [Google Scholar]
- Amiri, M.; Sadeghi, M. The Effectiveness of ACT on Psychological, Social and Spiritual Health of the Patients with angina pectoris. Int. J. Educ. Psychol. Res. 2017, 3, 240. [Google Scholar] [CrossRef]
- Gregg, J.A.; Callaghan, G.; Hayes, S.C.; Glenn-Lawson, J.L. Improving Diabetes Self-Management Through Acceptance, Mindfulness, and Values: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2007, 75, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Kaboudi, M.; Ziapour, A. The Effect of Acceptance and Commitment Therapy on the Mental Health of Women Patients with Type II Diabetes. Ann. Trop. Med. Public Healyh 2017, 10, 1709. [Google Scholar] [CrossRef]
- Khashouei, M.M.; Ghorbani, M.; Tabatabaei, F. The Effectiveness of Acceptance and Commitment Therapy (ACT) on Self-Efficacy, Perceived Stress and Resiliency in Type II Diabetes Patients. Glob. J. Health Sci. 2017, 9, 18–26. [Google Scholar] [CrossRef]
- Maghsoudi, Z.; Razavi, Z.; Razavi, M.; Javadi, M. Efficacy of Acceptance and Commitment Therapy for Emotional Distress in the Elderly with Type 2 Diabetes: A Randomized Controlled Trial. Diabetes. Metab. Syndr. Obesity. Targets Ther. 2019, 12, 2137–2143. [Google Scholar] [CrossRef] [Green Version]
- Shayeghian, Z.; Hassanabadi, H.; Aguilar-Vafaie, M.E.; Amiri, P.; Besharat, M.A. A Randomized Controlled Trial of Acceptance and Commitment Therapy for Type 2 Diabetes Management: The Moderating Role of Coping Styles. PLoS ONE 2016, 11, e0166599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, B. A Pilot Study of the Efficacy of Acceptance and Commitment Therapy for Adults with Type Two Diabetes. Ph.D. Thesis, The Wright Institute, Berkeley, CA, USA, 2014. [Google Scholar]
- Whitehead, L.C.; Crowe, M.T.; Carter, J.D.; Maskill, V.R.; Carlyle, D.; Bugge, C.; Frampton, C.M.A. A Nurse-led Education and Cognitive Behaviour Therapy-Based Intervention among Adults with Uncontrolled Ttype 2 Diabetes: A Randomised Controlled Trial. J. Eval. Clin. Pr. 2017, 23, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, L.C.; Crowe, M.T.; Carter, J.D.; Maskill, V.R.; Carlyle, D.; Bugge, C.; Frampton, C.M.A. A Nurse-led Interdisciplinary Approach to Promote Self-Management of Type 2 Diabetes: A Process Evaluation of Post-Intervention Experiences. J. Eval. Clin. Pr. 2016, 23, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Bigdeli, R.; Dehghan, F. The Effectiveness of Acceptance and Commitment Therapy (ACT) on Psychological Symptoms and Life Satisfaction in Patients with Type-2 Diabetes . Iran. J. Rehabil. Res. Nurs. 2019, 5, 34–42. [Google Scholar]
- Bistara, D.N.; Rusdianingseh, S.; Wardani, E.M.; Septianingrum, Y.; Ainiyah, N.; Fitriasari, A.; Noventi, I.; Hasina, S.N. Acceptance and Commitment Therapy (Act) On Increasing The Compliance Of Management Diabetes Mellitus Type 2. Int. J. Psychosoc. Rehabilittation 2020, 24, 942–946. [Google Scholar]
- Ghahnaviyeh, L.A.; Bagherian, R.; Feizi, A.; Afshari, A.; Darani, F.M. The Effectiveness of Acceptance and Commitment Therapy on Quality of Life in a Patient with Myocardial Infarction: A Randomized Control Trial. Iran. J. Psychiatry 2020, 15, 1–9. [Google Scholar] [CrossRef]
- Rahimi, M.; Nouri, R.; Raimi, M. The Effectiveness of the Acceptance and Commitment Therapy (ACT) Approaon Quality of Life and Hemoglobin A1c among Patients with Type 2 Diabete. Int. J. Med. Investig. 2019, 8, 61–69. [Google Scholar]
- Shaibani, K.A. The Effectiveness of Intervention Based on Acceptance and Commitment on Emotions and Thoughts Control in Patients with Type II Diabetes. J. Fundam. Ment. Health 2017, 19, 341–347. [Google Scholar]
- Sheibani, H.; Sheibani, K.A.; Amreei, N.N.; Masrour, M.J. An Investigation of the Effects of the Acceptance and Commitment Therapy in Groups on the Cognitive Strategies of Emotion Regulation and Self-Control in Coronary Heart Disease Patients. J. Med. Life 2020, 12, 361–367. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred Reporting Items for Systematic Reviews and Meta Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) checklist and guide. Br. Med. J. 2014, 348, 1628–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Score /9 |
|---|---|---|---|---|---|---|---|---|---|---|
| [20] | Y | U | U | Y | Y | Y | Y | Y | Y | 7/9 |
| [21] | Y | Y | N | Y | Y | Y | Y | Y | Y | 8/9 |
| [31] | Y | Y | N | Y | Y | Y | Y | Y | Y | 8/9 |
| [22] | Y | Y | U | Y | Y | U | Y | Y | Y | 7/9 |
| [32] | Y | U | U | Y | Y | U | Y | Y | Y | 6/9 |
| [23] | Y | Y | Y | Y | Y | U | Y | Y | U | 7/9 |
| [34] | Y | Y | U | U | Y | U | U | Y | Y | 5/9 |
| [35] | Y | Y | N | Y | Y | Y | Y | Y | Y | 8/9 |
| [24] | Y | Y | N | Y | Y | Y | Y | Y | Y | 8/9 |
| [38] | Y | U | U | N | Y | Y | NA | Y | Y | 5/9 |
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Score /10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [40] | Y | Y | Y | Y | Y | N | U | Y | Y | Y | 8/10 |
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Score /13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [33] | Y | Y | Y | U | U | U | Y | Y | Y | Y | Y | Y | Y | 10/13 |
| [36] | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | Y | Y | 8/13 |
| [37] | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | Y | Y | 8/13 |
| [39] | Y | Y | Y | N | N | U | Y | Y | Y | Y | Y | Y | Y | 10/13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rashidi, A.; Whitehead, L.; Newson, L.; Astin, F.; Gill, P.; Lane, D.A.; Lip, G.Y.H.; Neubeck, L.; Ski, C.F.; Thompson, D.R.; et al. The Role of Acceptance and Commitment Therapy in Cardiovascular and Diabetes Healthcare: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 8126. https://doi.org/10.3390/ijerph18158126
Rashidi A, Whitehead L, Newson L, Astin F, Gill P, Lane DA, Lip GYH, Neubeck L, Ski CF, Thompson DR, et al. The Role of Acceptance and Commitment Therapy in Cardiovascular and Diabetes Healthcare: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(15):8126. https://doi.org/10.3390/ijerph18158126
Chicago/Turabian StyleRashidi, Amineh, Lisa Whitehead, Lisa Newson, Felicity Astin, Paramjit Gill, Deirdre A. Lane, Gregory Y. H. Lip, Lis Neubeck, Chantal F. Ski, David R. Thompson, and et al. 2021. "The Role of Acceptance and Commitment Therapy in Cardiovascular and Diabetes Healthcare: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 15: 8126. https://doi.org/10.3390/ijerph18158126