
Association of Treated and Untreated Gastroesophageal Reflux Disease in the First Year of Life with the Subsequent Development of Asthma

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Exposure to GERD
2.3. Outcomes
2.3.1. Clinical Asthma
2.3.2. Treated Asthma
2.3.3. Wheezing
2.4. Covariates
2.5. Statistical Analyses
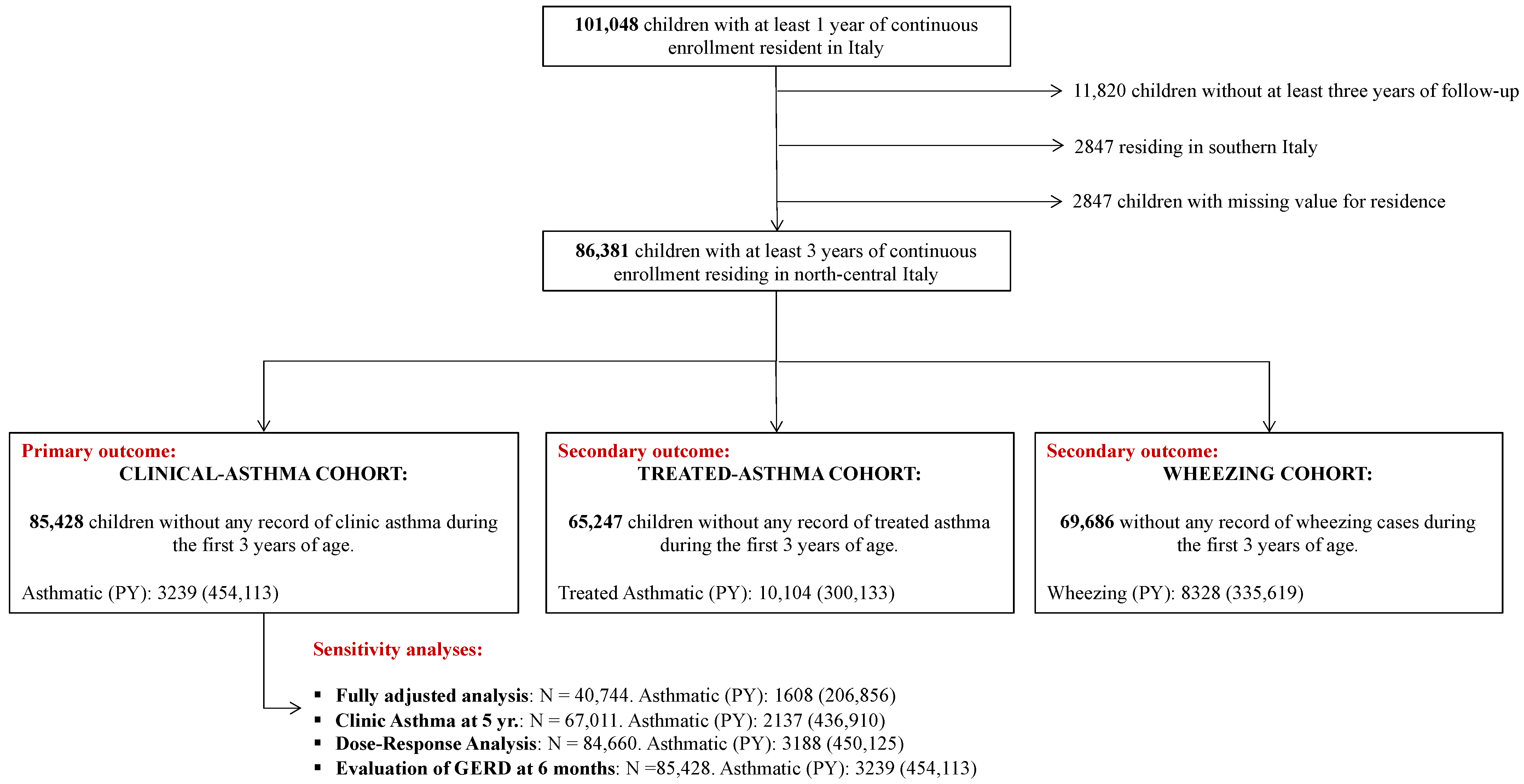
2.6. Primary Outcome: Clinical Asthma
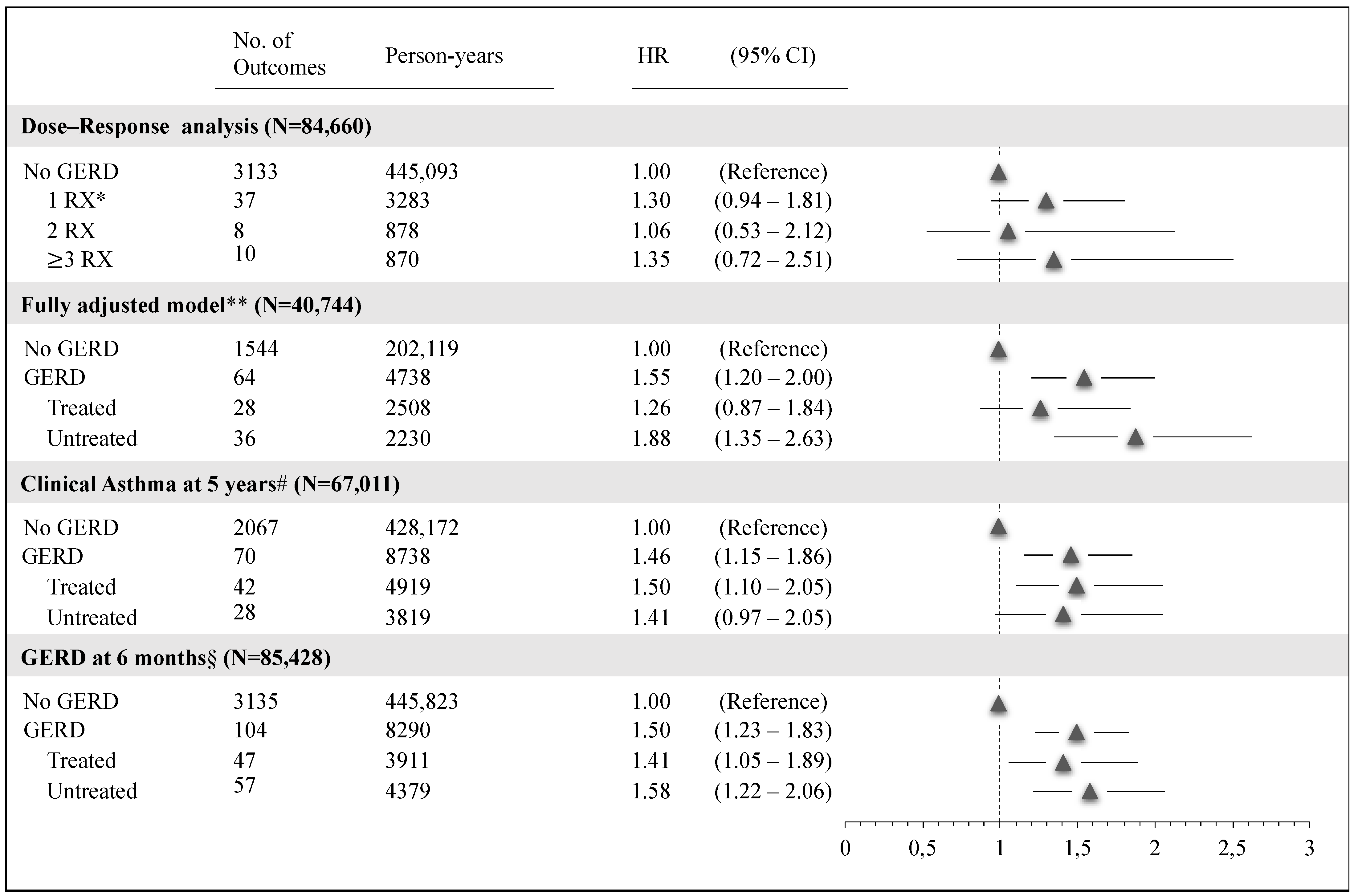
2.7. Sensitivity and Subgroup Analyses
2.8. Secondary Outcomes
3. Results
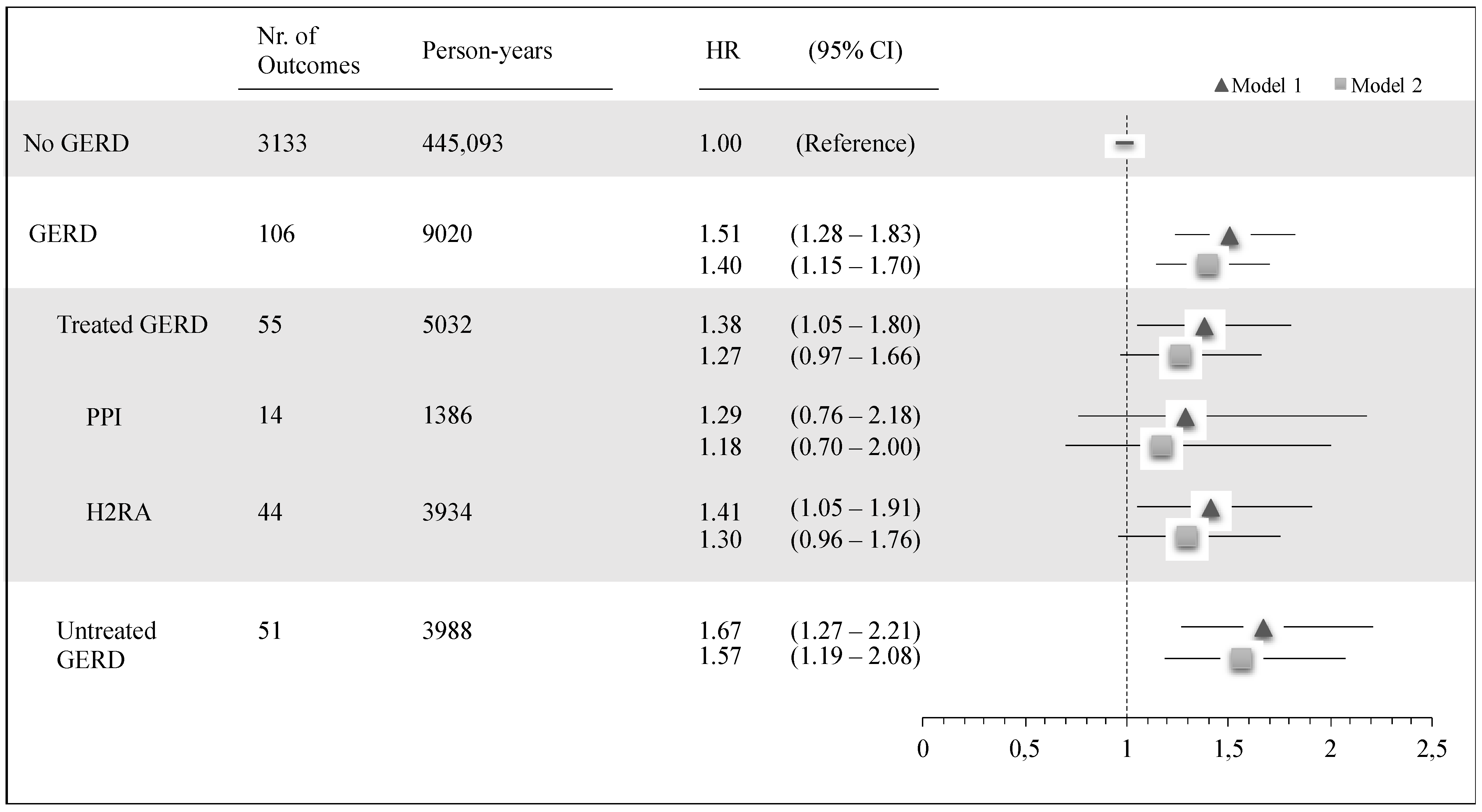
3.1. Clinical Asthma
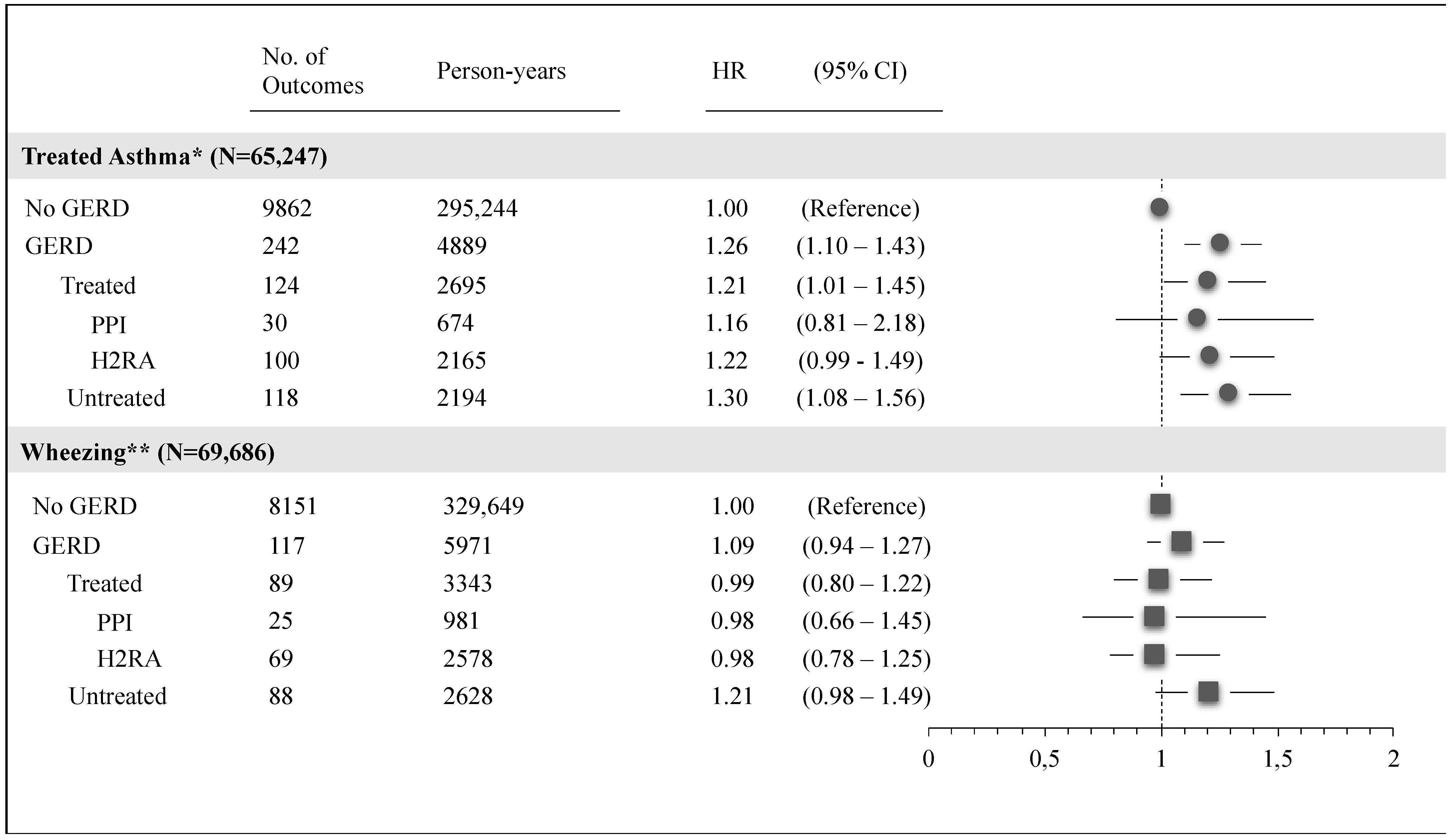
3.2. Treated Asthma and Wheezing
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Infant Reflux—Symptoms and Causes [WWW Document], n.d. Mayo Clin. URL. Available online: https://www.mayoclinic.org/diseases-conditions/infant-acid-reflux/symptoms-causes/syc-20351408 (accessed on 26 December 2020).
- Leung, A.K.; Hon, K.L. Gastroesophageal reflux in children: An updated review. Drugs Context 2019, 8, 1–12. [Google Scholar] [CrossRef]
- Poddar, U. Gastroesophageal reflux disease (GERD) in children. Paediatr. Int. Child Health 2019, 39, 7–12. [Google Scholar] [CrossRef]
- Bruno, G.; Zaccari, P.; Rocco, G.; Scalese, G.; Panetta, C.; Porowska, B.; Pontone, S.; Severi, C. Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World J. Gastroenterol. 2019, 25, 2706–2719. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Wahlin, K.; Engstrand, L.; Lagergren, J. Maintenance therapy with proton pump inhibitors and risk of gastric cancer: A nationwide population-based cohort study in Sweden. BMJ Open 2017, 7, e017739. [Google Scholar] [CrossRef]
- Knox, N.C.; Forbes, J.D.; Peterson, C.-L.; Van Domselaar, G.; Bernstein, C.N. The gut microbiome in inflammatory bowel disease: Lessons learned from other immune-mediated inflammatory diseases. Am. J. Gastroenterol. 2019, 114, 1051–1070. [Google Scholar] [CrossRef] [PubMed]
- Knight, R.; Vrbanac, A.; Taylor, B.C.; Aksenov, A.; Callewaert, C.; Debelius, J.; Gonzalez, A.; Kosciolek, T.; McCall, L.-I.; McDonald, D.; et al. Best practices for analysing microbiomes. Nat. Rev. Microbiol. 2018, 16, 410–422. [Google Scholar] [CrossRef]
- Frati, F.; Salvatori, C.; Incorvaia, C.; Bellucci, A.; Di Cara, G.; Marcucci, F.; Esposito, S. The role of the microbiome in asthma: The gut-lung axis. Int. J. Mol. Sci. 2018, 20, 123. [Google Scholar] [CrossRef]
- Fujimura, K.E.; Lynch, S.V. Microbiota in allergy and asthma and the emerging relationship with the gut microbiome. Cell Host Microbe 2015, 17, 592–602. [Google Scholar] [CrossRef]
- Amidei, C.B.; Comoretto, R.; Zanier, L.; Donà, D.; Cantarutti, A.; Canova, C. Acid-suppressive medications in the first year of life and risk of childhood asthma: A population-based birth cohort study. Eur. Respir. J. 2020, 56, 2000197. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-H.; Wintzell, V.; Ludvigsson, J.F.; Svanström, H.; Pasternak, B. Association between proton pump inhibitor use and risk of asthma in children. JAMA Pediatr. 2021, 175, 394–403. [Google Scholar] [CrossRef]
- Mitre, E.; Susi, A.; Kropp, L.E.; Schwartz, D.J.; Gorman, G.H.; Nylund, C.M. Association between use of acid-suppressive medications and antibiotics during infancy and allergic diseases in early childhood. JAMA Pediatr. 2018, 172, e180315. [Google Scholar] [CrossRef] [PubMed]
- Valet, R.S.; Carroll, K.N.; Gebretsadik, T.; Minton, P.A.; Woodward, K.B.; Liu, Z.; Hartert, T.V. Gastroesophageal reflux disease increases infant acute respiratory illness severity, but not childhood asthma. Pediatr. Allergy Immunol. Pulmonol. 2014, 27, 30–33. [Google Scholar] [CrossRef]
- Thakkar, K.; Boatright, R.O.; Gilger, M.A.; El-Serag, H.B. Gastroesophageal reflux and asthma in children: A systematic review. Pediatrics 2010, 125, e925–e930. [Google Scholar] [CrossRef]
- Rubak, S.; Høst, A.; Christensen, L.B.; Langfrits, M.S.; Thomsen, R.W. Validity of asthma diagnoses and patterns of anti-asthmatic drug use in a cohort of 2053 Danish children. Health Sci. Rep. 2018, 1, e77. [Google Scholar] [CrossRef]
- Papadopoulos, N.G.; Arakawa, H.; Carlsen, K.-H.; Custovic, A.; Gern, J.; Lemanske, R.; Le Souef, P.; Mäkelä, M.; Roberts, G.; Wong, G.; et al. International Consensus On (ICON) Pediatric Asthma. Allergy 2012, 67, 976–997. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.-C.; Tsai, Y.-G.; Chang, Y.-H.; Kuo, C.-H.; Lin, Y.-C.; Hung, C.-H. Allergic rhinitis as a key factor for the development of gastroesophageal reflux disease in children. J. Microbiol. Immunol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mahdavinia, M.; Bishehsari, F.; Hayat, W.; Codispoti, C.D.; Sarrafi, S.; Husain, I.; Mehta, A.; Benhammuda, M.; Tobin, M.C.; Bandi, S.; et al. Prevalence of allergic rhinitis and asthma in patients with chronic rhinosinusitis and gastroesophageal reflux disease. Ann. Allergy Asthma Immunol. 2016, 117, 158–162.e1. [Google Scholar] [CrossRef] [PubMed]
- Cinquetti, M.; Micelli, S.; Voltolina, C.; Zoppi, G. The pattern of gastroesophageal reflux in asthmatic children. J. Asthma 2002, 39, 135–142. [Google Scholar] [CrossRef]
- Teixeira, B.C.; Norton, R.C.; Penna, F.J.; Camargos, P.A.; Lasmar, L.M.L.B.F.; Macedo, A.V. Gastroesophageal reflux and asthma in childhood: A study on their relationship using esophageal PH monitoring. J. Pediatr. 2007, 83, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, P.M.; Kjellman, N.I.; Tibbling, L. Bronchial asthma and acid reflux into the distal and proximal oesophagus. Arch. Dis. Child. 1990, 65, 1255–1258. [Google Scholar] [CrossRef]
- Rachid, R.; Chatila, T.A. The role of the gut microbiota in food allergy. Curr. Opin. Pediatr. 2016, 28, 748–753. [Google Scholar] [CrossRef]
- Rosen, R.; Vandenplas, Y.; Singendonk, M.; Cabana, M.; DiLorenzo, C.; Gottrand, F.; Gupta, S.; Langendam, M.; Staiano, A.; Thapar, N.; et al. Pediatric gastroesophageal reflux clinical practice guidelines: Joint recommendations of the North American society for pediatric gastroenterology, hepatology, and nutrition (NASPGHAN) and the European society for pediatric gastroenterology, hepatology, and nutrition (ESPGHAN). J. Pediatr. Gastroenterol. Nutr. 2018, 66, 516–554. [Google Scholar] [CrossRef] [PubMed]
- Mahant, S. Pharmacological treatment of children with gastro-oesophageal reflux. Paediatr. Child Health 2017, 22, 30–32. [Google Scholar] [CrossRef]
- Hassall, E. Over-prescription of acid-suppressing medications in infants: How it came about, why it’s wrong, and what to do about it. J. Pediatr. 2012, 160, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Hudson, B.; Alderton, A.; Doocey, C.; Nicholson, D.; Toop, L.; Day, A.S. Crying and spilling--time to stop the overmedicalisation of normal infant behaviour. N. Z. Med. J. 2012, 125, 119–126. [Google Scholar]
- Griffiths, T.L.; Nassar, M.; Soubani, A.O. Pulmonary manifestations of gastroesophageal reflux disease. Expert Rev. Respir. Med. 2020, 14, 767–775. [Google Scholar] [CrossRef] [PubMed]
- GINA 2019 Main Report WWW Document, n.d. URL. Available online: https://ginasthma.org/wp-content/uploads/2019/06/GINA-2019-main-report-June-2019-wms.pdf (accessed on 24 June 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GERD | GERD | No GERD | p-Value | |||
|---|---|---|---|---|---|---|
| Treated | Untreated | GERD vs. No GERD | Treated vs. Untreated | |||
| (N = 1652) | (N = 871) | (N = 781) | (N = 84,729) | |||
| Year of birth | ||||||
| 2004–2007 | 509 (30.8) | 267 (30.7) | 242 (31.0) | 29,767 (35.1) | 0.0011 | <0.0001 |
| 2008–2011 | 575 (34.8) | 367 (42.1) | 208 (26.6) | 28,159 (33.2) | ||
| 2012–2015 | 568 (34.4) | 237 (27.2) | 331 (42.4) | 26,803 (31.6) | ||
| Gender | ||||||
| Female | 785 (47.5) | 418 (48.0) | 367 (47.0) | 40,974 (48.4) | 0.4983 | 0.6846 |
| Male | 867 (52.5) | 453 (52.0) | 414 (53.0) | 43,755 (51.6) | ||
| No. of Antibiotics | ||||||
| 0 | 803 (48.6) | 404 (46.4) | 339 (51.1) | 54,923 (64.8) | <0.0001 | 0.0047 |
| 1 | 402 (24.3) | 201 (23.1) | 201 (25.7) | 15,491 (18.3) | ||
| 2 | 208 (12.6) | 117 (13.4) | 91 (11.6) | 7442 (8.8) | ||
| ≥3 | 239 (14.5) | 149 (17.1) | 90 (11.5) | 6873 (8.1) | ||
| No. of medical visits—mean (STD) | 14.92 (6.2) | 15.57 (6.6) | 14.20 (5.7) | 9.09 (5.8) | <0.0001 | <0.0001 |
| 5 | 38 (2.3) | 16 (1.8) | 22 (2.8) | 20,157 (23.8) | <0.0001 | 0.0273 |
| 6–9 | 247 (14.9) | 114 (13.1) | 133 (17.0) | 26,669 (31.5) | ||
| ≥10 | 1367 (82.8) | 741 (85.1) | 626 (80.2) | 37,903 (44.7) | ||
| Gestational age—mean (STD) ⱡ | 38.70 (1.9) | 38.50 (2.0) | 38.90 (1.8) | 39.03 (1.7) | <0.0001 | 0.0012 |
| ≤28 GW | 0 (0.0) | 0 (0.0) | 0 (0.0) | 41 (0.1) | <0.0001 | 0.3814 |
| 29–35 GW | 54 (5.9) | 30 (6.6) | 24 (5.3) | 1341 (3.3) | ||
| ≥36 GW | 854 (94.1) | 422 (93.4) | 432 (94.7) | 39,015 (96.6) | ||
| Birth weight—mean (STD) ⱡ | 3158.15 (523.7) | 3120.76 (546.1) | 3195.21 (498.3) | 3276.47 (498.6) | <0.0001 | 0.0321 |
| <2500 gr. | 82 (9.0) | 51 (11.3) | 31 (6.8) | 2345 (5.8) | <0.0001 | 0.0184 |
| ≥2500 gr. | 826 (91.0) | 401 (88.7) | 425 (93.2) | 38,052 (94.2) | ||
| Apgar 1 score—mean (STD) ⱡ | 8.86 (1.0) | 8.81 (1.1) | 8.91 (0.8) | 8.95 (0.9) | 0.0038 | 0.1577 |
| <7 | 28 (3.1) | 19 (4.2) | 9 (2.0) | 1021 (2.5) | 0.2920 | 0.0520 |
| ≥7 | 880 (96.9) | 433 (95.8) | 477 (98.0) | 39,376 (97.5) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantarutti, A.; Barbiellini Amidei, C.; Valsecchi, C.; Scamarcia, A.; Corrao, G.; Gregori, D.; Giaquinto, C.; Ludvigsson, J.F.; Canova, C. Association of Treated and Untreated Gastroesophageal Reflux Disease in the First Year of Life with the Subsequent Development of Asthma. Int. J. Environ. Res. Public Health 2021, 18, 9633. https://doi.org/10.3390/ijerph18189633
Cantarutti A, Barbiellini Amidei C, Valsecchi C, Scamarcia A, Corrao G, Gregori D, Giaquinto C, Ludvigsson JF, Canova C. Association of Treated and Untreated Gastroesophageal Reflux Disease in the First Year of Life with the Subsequent Development of Asthma. International Journal of Environmental Research and Public Health. 2021; 18(18):9633. https://doi.org/10.3390/ijerph18189633
Chicago/Turabian StyleCantarutti, Anna, Claudio Barbiellini Amidei, Camilla Valsecchi, Antonio Scamarcia, Giovanni Corrao, Dario Gregori, Carlo Giaquinto, Jonas F. Ludvigsson, and Cristina Canova. 2021. "Association of Treated and Untreated Gastroesophageal Reflux Disease in the First Year of Life with the Subsequent Development of Asthma" International Journal of Environmental Research and Public Health 18, no. 18: 9633. https://doi.org/10.3390/ijerph18189633