
Environmental and Occupational Short-Term Exposure to Airborne Particles and FEV1 and FVC in Healthy Adults: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
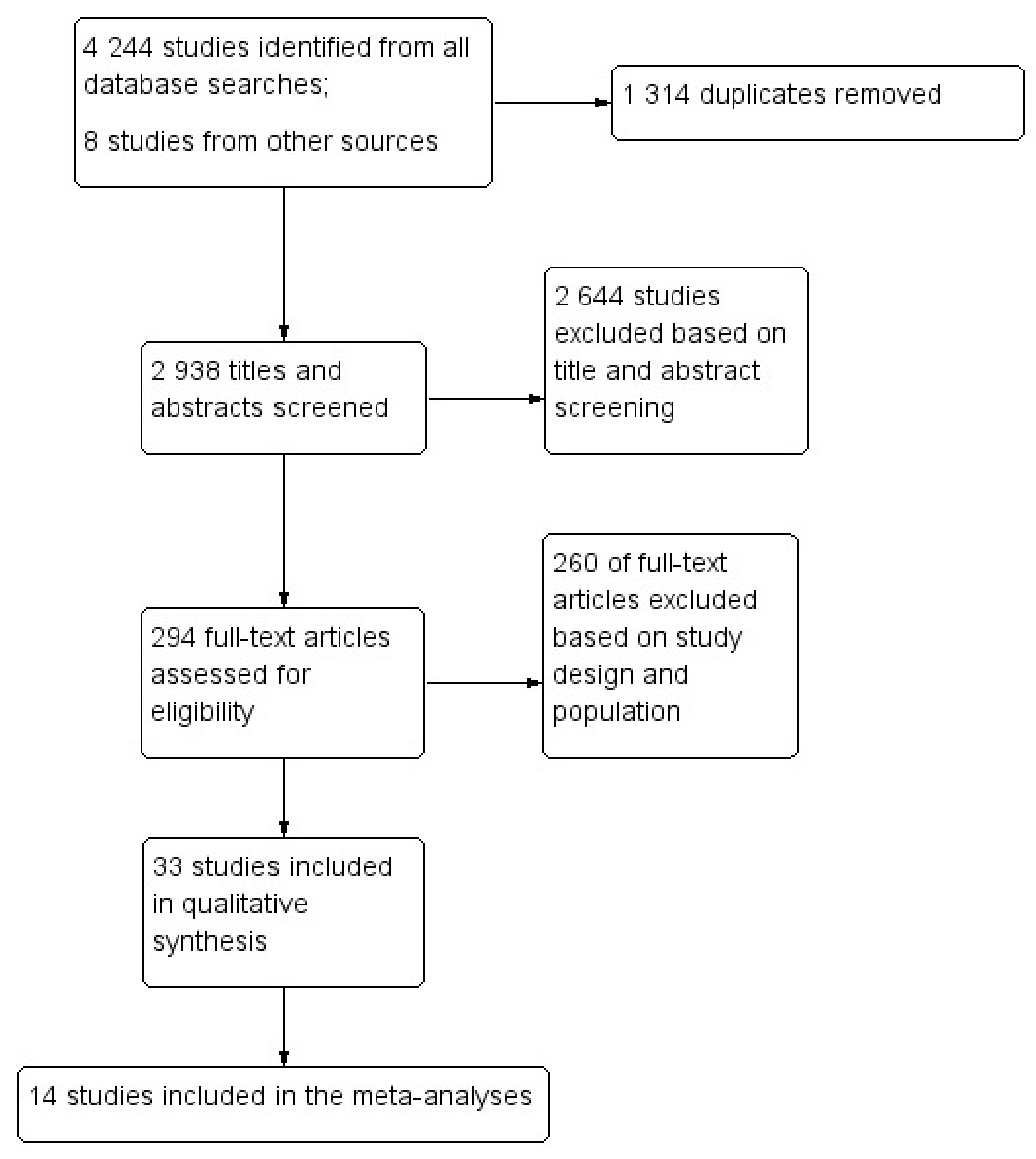
2.4. Studies Selection and Data Extraction
2.5. Quality Assessment
2.6. Meta-Analyses
3. Results
3.1. Characteristics of the Selected Studies
3.1.1. Environmental Studies
3.1.2. Occupational Studies
3.2. Quality Assessment
3.3. Forest Plots and Meta-Analyses
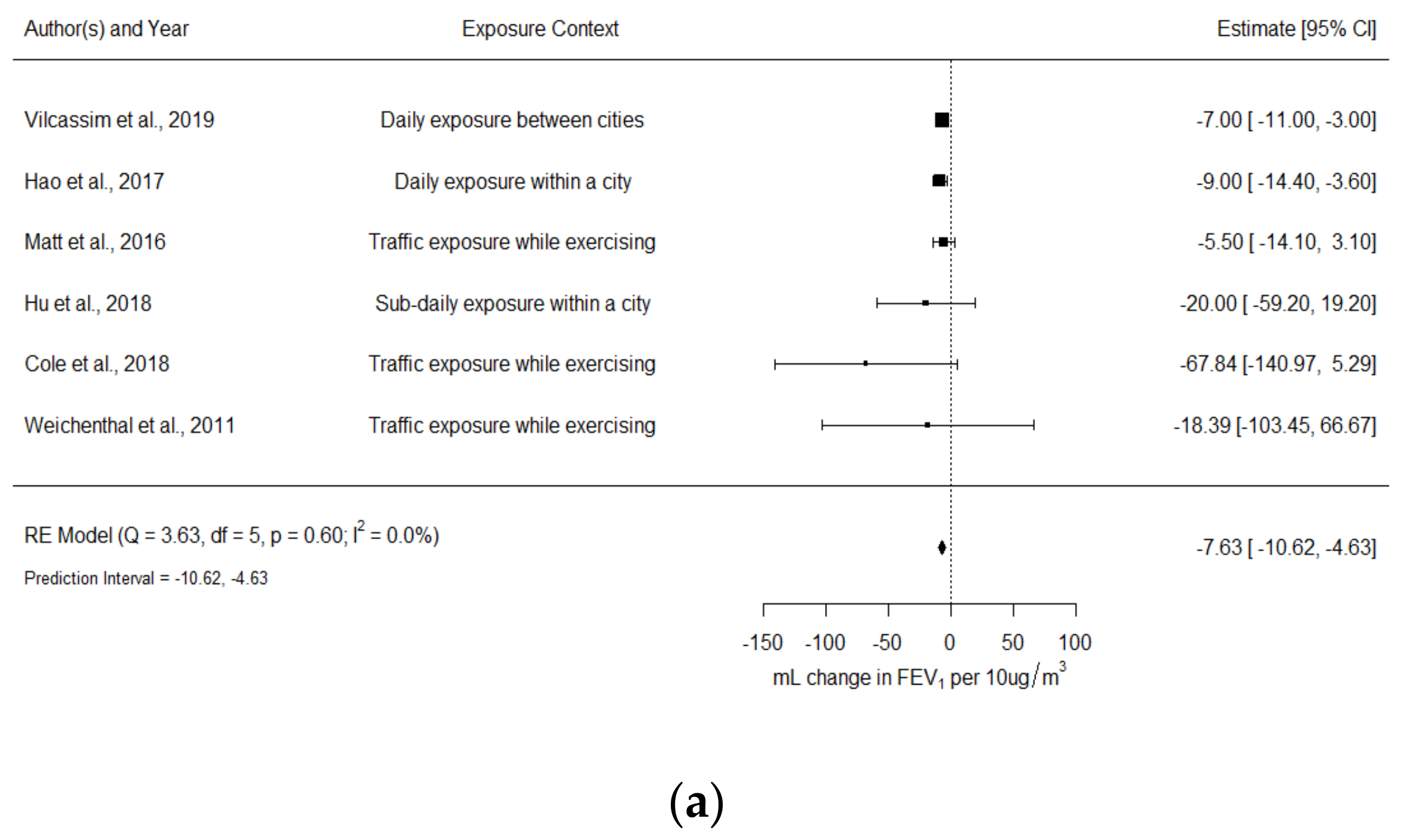
3.3.1. FEV1 (mL Change)
- FEV1 and PM2.5 in environmental studies
- FEV1 and PM4 in occupational studies
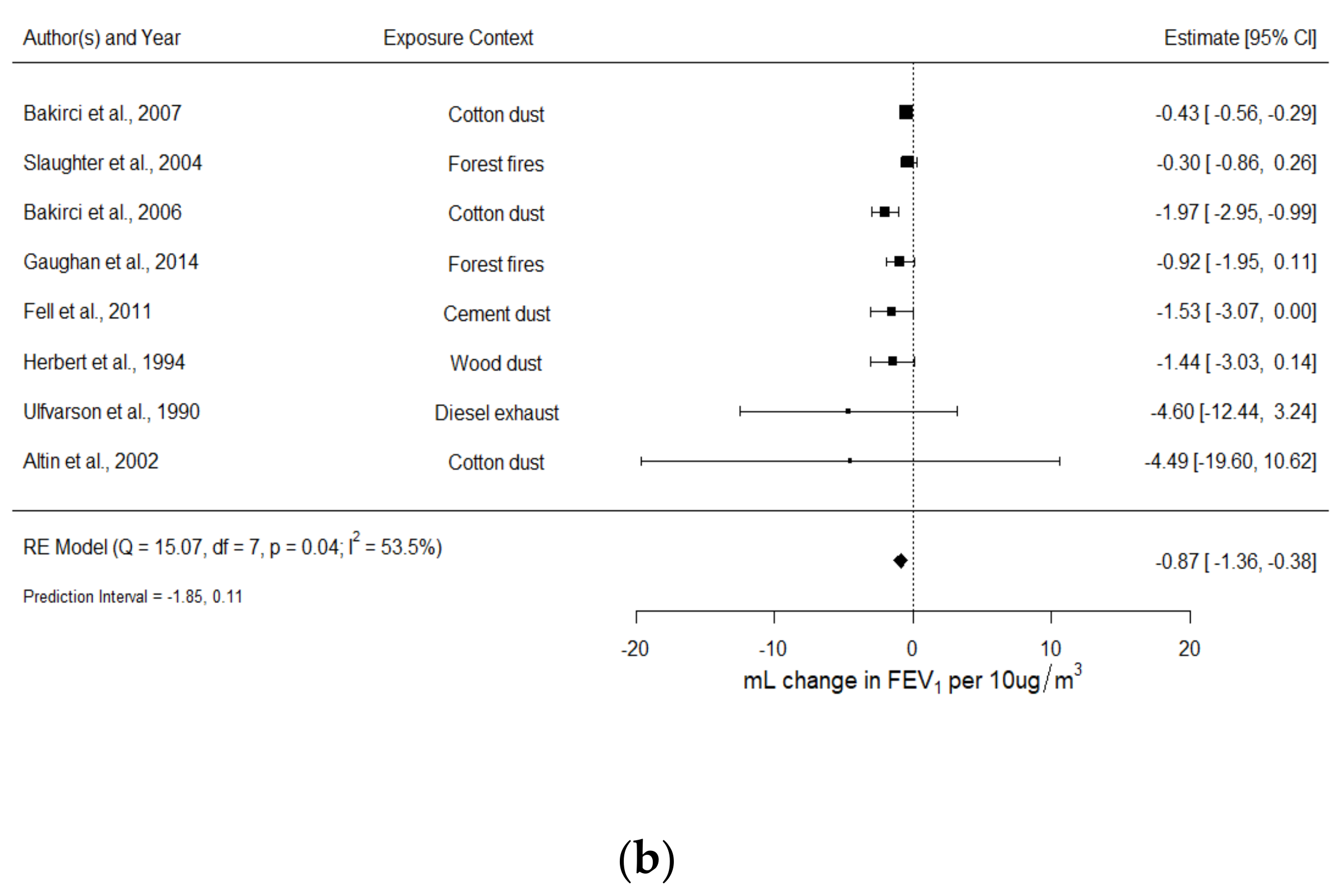
3.3.2. FVC (mL Changes)
- FVC and PM2.5 in environmental studies
- FVC and PM4 in occupational studies
3.4. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- US Environmental Protection Agency. Integrated Science Assessment (ISA) for Particulate Matter (Final Report, 2019); U.S. Environmental Protection Agency: Washington, DC, USA, 2019.
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Committee on the Medical Effects of Air Pollutants. Cardiovascular Disease and Air Pollution; United Kingdom Department of Health: London, UK, 2006.
- Ming, L.; Jin, L.; Li, J.; Fu, P.; Yang, W.; Liu, D.; Zhang, G.; Wang, Z.; Li, X. PM2.5 in the Yangtze River Delta, China: Chemical compositions, seasonal variations, and regional pollution events. Environ. Pollut. 2017, 223, 200–212. [Google Scholar] [CrossRef]
- World Health Organization. Air Quality Guidelines: Global Update 2005, Particulate Matter, Ozone, Nitrogen Dioxide, and Sulfur Dioxide; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Beelen, R.; Hoek, G.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.H.; et al. Natural-Cause Mortality and Long-Term Exposure to Particle Components: An Analysis of 19 European Cohorts within the Multi-Center ESCAPE Project. Environ. Health Perspect. 2015, 123, 525–533. [Google Scholar] [CrossRef]
- Lin, H.; Liu, T.; Xiao, J.; Zeng, W.; Li, X.; Guo, L.; Zhang, Y.; Xu, Y.; Tao, J.; Xian, H.; et al. Mortality burden of ambient fine particulate air pollution in six Chinese cities: Results from the Pearl River Delta study. Environ. Int. 2016, 96, 91–97. [Google Scholar] [CrossRef]
- Tao, J.; Zhang, L.; Cao, J.; Zhang, R. A review of current knowledge concerning PM2. 5 chemical composition, aerosol optical properties and their relationships across China. Atmos. Chem. Phys. Discuss. 2017, 17, 9485–9518. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Ruan, Z.; Wang, X.; Yang, Y.; Mason, T.G.; Lin, H.; Tian, L. Short-term and long-term exposures to fine particulate matter constituents and health: A systematic review and meta-analysis. Environ. Pollut. 2019, 247, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Di, Q.; Dai, L.; Wang, Y.; Zanobetti, A.; Choirat, C.; Schwartz, J.D.; Dominici, F. Association of Short-term Exposure to Air Pollution with Mortality in Older Adults. JAMA 2017, 318, 2446–2456. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Newell, K.; Kartsonaki, C.; Lam, K.B.H.; Kurmi, O.P. Cardiorespiratory health effects of particulate ambient air pollution exposure in low-income and middle-income countries: A systematic review and meta-analysis. Lancet Planet. Health 2017, 1, e368–e380. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.-Y.; Ding, H.; Jiang, L.-N.; Chen, S.-W.; Zheng, J.-P.; Qiu, M.; Zhou, Y.-X.; Chen, Q.; Guan, W.-J. Association between air pollutants and asthma emergency room visits and hospital admissions in time series studies: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef] [PubMed]
- Schraufnagel, D.E.; Balmes, J.R.; Cowl, C.T.; De Matteis, S.; Jung, S.-H.; Mortimer, K.; Perez-Padilla, R.; Rice, M.B.; Riojas-Rodriguez, H.; Sood, A.; et al. Air pollution and noncommunicable diseases: A review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air pollution and organ systems. Chest 2019, 155, 417–426. [Google Scholar] [CrossRef]
- Sonego, M.; Pellegrin, M.C.; Becker, G.; Lazzerini, M. Risk Factors for Mortality from Acute Lower Respiratory Infections (ALRI) in Children under Five Years of Age in Low and Middle-Income Countries: A Systematic Review and Meta-Analysis of Observational Studies. PLoS ONE 2015, 10, e0116380. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, B.; Boogaard, H.; de Nazelle, A.; Andersen, Z.J.; Abramson, M.; Brauer, M.; Brunekreef, B.; Forastiere, F.; Huang, W.; Kan, H.; et al. WHO Air Quality Guidelines 2021–Aiming for Healthier Air for all: A Joint Statement by Medical, Public Health, Scientific Societies and Patient Representative Organisations. Int. J. Public Health 2021, 66, 1604465. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC). Air Pollution and Cancer; International Agency for Research on Cancer (IARC): Lyon, France, 2013. [Google Scholar]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Ni, Y.; Li, H.; Pan, L.; Yang, D.; Baccarelli, A.A.; Deng, F.; Chen, Y.; Shima, M.; Guo, X. Short-term exposure to high ambient air pollution increases airway inflammation and respiratory symptoms in chronic obstructive pulmonary disease patients in Beijing, China. Environ. Int. 2016, 94, 76–82. [Google Scholar] [CrossRef]
- Bloemsma, L.D.; Hoek, G.; Smit, L.A. Panel studies of air pollution in patients with COPD: Systematic review and meta-analysis. Environ. Res. 2016, 151, 458–468. [Google Scholar] [CrossRef]
- McCreanor, J.; Cullinan, P.; Nieuwenhuijsen, M.J.; Stewart-Evans, J.; Malliarou, E.; Jarup, L.; Harrington, R.; Svartengren, M.; Han, I.-K.; Ohman-Strickland, P.; et al. Respiratory Effects of Exposure to Diesel Traffic in Persons with Asthma. N. Engl. J. Med. 2007, 357, 2348–2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golan, R.; Ladva, C.; Greenwald, R.; Krall, J.; Raysoni, A.U.; Kewada, P.; Winquist, A.; Flanders, W.D.; Liang, D.; Sarnat, J.A. Acute pulmonary and inflammatory response in young adults following a scripted car commute. Air Qual. Atmos. Health 2017, 11, 123–136. [Google Scholar] [CrossRef]
- Cole, C.A.; Carlsten, C.; Koehle, M.; Brauer, M. Particulate matter exposure and health impacts of urban cyclists: A randomized crossover study. Environ. Health 2018, 17, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matt, F.; Cole-Hunter, T.; Donaire-Gonzalez, D.; Kubesch, N.; Martínez, D.; Carrasco-Turigas, G.; Nieuwenhuijsen, M. Acute respiratory response to traffic-related air pollution during physical activity performance. Environ. Int. 2016, 97, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Weichenthal, S.; Kulka, R.; Dubeau, A.; Martin, C.; Wang, D.; Dales, R. Traffic-Related Air Pollution and Acute Changes in Heart Rate Variability and Respiratory Function in Urban Cyclists. Environ. Health Perspect. 2011, 119, 1373–1378. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Zhu, T.; Kipen, H.; Wang, G.; Hu, M.; Guo, Q.; Ohman-Strickland, P.; Lu, S.-E.; Wang, Y.; Zhu, P.; et al. Comparisons of Ultrafine and Fine Particles in Their Associations with Biomarkers Reflecting Physiological Pathways. Environ. Sci. Technol. 2014, 48, 5264–5273. [Google Scholar] [CrossRef]
- Liu, J.-Y.; Hsiao, T.-C.; Lee, K.-Y.; Chuang, H.-C.; Cheng, T.-J.; Chuang, K.-J. Association of ultrafine particles with cardiopulmonary health among adult subjects in the urban areas of northern Taiwan. Sci. Total. Environ. 2018, 627, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.; Kauri, L.M.; Cakmak, S.; Mahmud, M.; Weichenthal, S.A.; Van Ryswyk, K.; Kumarathasan, P.; Thomson, E.; Vincent, R.; Broad, G.; et al. Acute changes in lung function associated with proximity to a steel plant: A randomized study. Environ. Int. 2013, 55, 15–19. [Google Scholar] [CrossRef]
- Huang, J.; Deng, F.; Wu, S.; Zhao, Y.; Shima, M.; Guo, B.; Liu, Q.; Guo, X. Acute effects on pulmonary function in young healthy adults exposed to traffic-related air pollution in semi-closed transport hub in Beijing. Environ. Health Prev. Med. 2016, 21, 312–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirowsky, J.E.; Peltier, R.E.; Lippmann, M.; Thurston, G.; Chen, L.-C.; Neas, L.; Diaz-Sanchez, D.; Laumbach, R.; Carter, J.D.; Gordon, T. Repeated measures of inflammation, blood pressure, and heart rate variability associated with traffic exposures in healthy adults. Environ. Health 2015, 14, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strak, M.; Janssen, N.A.; Godri, K.J.; Gosens, I.; Mudway, I.S.; Cassee, F.R.; Lebret, E.; Kelly, F.J.; Harrison, R.M.; Brunekreef, B.; et al. Respiratory Health Effects of Airborne Particulate Matter: The Role of Particle Size, Composition, and Oxidative Potential—The RAPTES Project. Environ. Health Perspect. 2012, 120, 1183–1189. [Google Scholar] [CrossRef] [Green Version]
- Da Silveira Fleck, A.; Catto, C.; L’Espérance, G.; Masse, J.-P.; Roberge, B.; Debia, M. Characterization and Quantification of Ultrafine Particles and Carbonaceous Components from Occupational Exposures to Diesel Particulate Matter in Selected Workplaces. Ann. Work. Expo. Health 2020, 64, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Gaughan, D.M.; Piacitelli, C.A.; Chen, B.T.; Law, B.F.; Virji, M.A.; Edwards, N.T.; Enright, P.L.; Schwegler-Berry, D.E.; Leonard, S.S.; Wagner, G.R.; et al. Exposures and Cross-shift Lung Function Declines in Wildland Firefighters. J. Occup. Environ. Hyg. 2014, 11, 591–603. [Google Scholar] [CrossRef]
- Gu, J.; Kirsch, I.; Schripp, T.; Froning-Ponndorf, F.; Berthold, D.; Salthammer, T. Human exposure to airborne particles during wood processing. Atmos. Environ. 2018, 193, 101–108. [Google Scholar] [CrossRef]
- Viitanen, A.-K.; Uuksulainen, S.; Koivisto, A.J.; Hämeri, K.; Kauppinen, T. Workplace Measurements of Ultrafine Particles-A Literature Review. Ann. Work. Expo. Health 2017, 61, 749–758. [Google Scholar] [CrossRef]
- Cullinan, P.; Muñoz, X.; Suojalehto, H.; Agius, R.; Jindal, S.; Sigsgaard, T.; Blomberg, A.; Charpin, D.; Annesi-Maesano, I.; Gulati, M.; et al. Occupational lung diseases: From old and novel exposures to effective preventive strategies. Lancet Respir. Med. 2017, 5, 445–455. [Google Scholar] [CrossRef]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ACGIH®. American Conference of Governmental Industrial Hygienists: TLVs and BEIs Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents and Biological Exposure Indices; American Conference of Governmental Industrial Hygienists: Washington, DC, USA, 2016. [Google Scholar]
- National Toxicology Program. Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration; Office of Health Assessment and Translation, Division of the National Toxicology Program, National Institute of Environmental Health Sciences: Durham, NC, USA, 2015. [Google Scholar]
- Buteau, S.; Goldberg, M.S. Methodological issues related to pooling results from panel studies of heart rate variability and its association with ambient air pollution. Environ. Res. 2015, 140, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Altin, R.; Ozkurt, S.; Fisekçi, F.; Cimrin, A.; Zencir, M.; Sevinc, C. Prevalence of byssinosis and respiratory symptoms among cotton mill workers. Respiration 2002, 69, 52–56. [Google Scholar] [CrossRef]
- Bakirci, N.; Kalaca, S.; Francis, H.; Fletcher, A.M.; Pickering, C.A.C.; Tumerdem, N.; Cali, S.; Oldham, L.; Niven, R. Natural History and Risk Factors of Early Respiratory Responses to Exposure to Cotton Dust in Newly Exposed Workers. J. Occup. Environ. Med. 2007, 49, 853–861. [Google Scholar] [CrossRef]
- Bakirci, N.; Sayiner, A.; Sacaklioglu, F.; Bayindir, U. Across-shift lung function variation in cottonseed oil workers. Occup. Med. 2006, 56, 365–370. [Google Scholar] [CrossRef] [Green Version]
- Fell, A.K.M.; Notø, H.; Skogstad, M.; Nordby, K.-C.; Eduard, W.; Svendsen, M.V.; Øvstebø, R.; Trøseid, A.M.S.; Kongerud, J. A cross-shift study of lung function, exhaled nitric oxide and inflammatory markers in blood in Norwegian cement production workers. Occup. Environ. Med. 2011, 68, 799–805. [Google Scholar] [CrossRef]
- Ulfvarson, U.; Alexandersson, R. Reduction in adverse effect on pulmonary function after exposure to filtered diesel exhaust. Am. J. Ind. Med. 1990, 17, 341–347. [Google Scholar] [CrossRef]
- Hao, Y.; Zhang, G.; Han, B.; Xu, X.; Feng, N.; Li, Y.; Wang, W.; Kan, H.; Bai, Z.; Zhu, Y.; et al. Prospective evaluation of respiratory health benefits from reduced exposure to airborne particulate matter. Int. J. Environ. Health Res. 2017, 27, 126–135. [Google Scholar] [CrossRef]
- Mirabelli, M.C.; Golan, R.; Greenwald, R.; Raysoni, A.U.; Holguin, F.; Kewada, P.; Winquist, A.; Flanders, W.D.; Sarnat, J.A. Modification of Traffic-related Respiratory Response by Asthma Control in a Population of Car Commuters. Epidemiology 2015, 26, 546–555. [Google Scholar] [CrossRef] [Green Version]
- Zuurbier, M.; Hoek, G.; Oldenwening, M.; Meliefste, K.; Hazel, P.V.D.; Brunekreef, B. Respiratory Effects of Commuters’ Exposure to Air Pollution in Traffic. Epidemiology 2011, 22, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Baccarelli, A.A.; Zheng, Y.; Zhang, X.; Chang, D.; Liu, L.; Wolf, K.R.; Zhang, Z.; McCracken, J.P.; Díaz, A.; Bertazzi, P.A.; et al. Air pollution exposure and lung function in highly exposed subjects in Beijing, China: A repeated-measure study. Part. Fibre Toxicol. 2014, 11, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cakmak, S.; Dales, R.; Kauri, L.; Mahmud, M.; Van Ryswyk, K.; Vanos, J.; Liu, L.; Kumarathasan, P.; Thomson, E.; Vincent, R.; et al. Metal composition of fine particulate air pollution and acute changes in cardiorespiratory physiology. Environ. Pollut. 2014, 189, 208–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girardot, S.P.; Ryan, P.B.; Smith, S.M.; Davis, W.T.; Hamilton, C.B.; Obenour, R.A.; Renfro, J.R.; Tromatore, K.A.; Reed, G.D. Ozone and PM 2.5 Exposure and Acute Pulmonary Health Effects: A Study of Hikers in theGreat Smoky Mountains National Park. Environ. Health Perspect. 2006, 114, 1044–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.-W.; Qian, Z.; Bloom, M.S.; Nelson, E.J.; Liu, E.; Han, B.; Zhang, N.; Liu, Y.; Ma, H.; Chen, D.-H.; et al. A panel study of airborne particulate matter concentration and impaired cardiopulmonary function in young adults by two different exposure measurement. Atmos. Environ. 2018, 180, 103–109. [Google Scholar] [CrossRef]
- Jarjour, S.; Jerrett, M.; Westerdahl, D.; De Nazelle, A.; Hanning, C.; Daly, L.; Lipsitt, J.; Balmes, J. Cyclist route choice, traffic-related air pollution, and lung function: A scripted exposure study. Environ. Health 2013, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Kubesch, N.J.; de Nazelle, A.; Westerdahl, D.; Martinez, D.; Carrasco-Turigas, G.; Bouso, L.; Guerra, S.; Nieuwenhuijsen, M.J. Respiratory and inflammatory responses to short-term exposure to traffic-related air pollution with and without moderate physical activity. Occup. Environ. Med. 2015, 72, 284–293. [Google Scholar] [CrossRef]
- Thaller, E.I.; Petronella, S.A.; Hochman, D.; Howard, S.; Chhikara, R.S.; Brooks, E.G. Moderate Increases in Ambient PM2.5 and Ozone Are Associated with Lung Function Decreases in Beach Lifeguards. J. Occup. Environ. Med. 2008, 50, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Vilcassim, M.J.R.; Thurston, G.D.; Chen, L.-C.; Lim, C.C.; Saunders, E.; Yao, Y.; Gordon, T. Exposure to air pollution is associated with adverse cardiopulmonary health effects in international travellers. J. Travel Med. 2019, 26, taz032. [Google Scholar] [CrossRef]
- Wu, S.; Deng, F.; Wang, X.; Wei, H.; Shima, M.; Huang, J.; Lv, H.; Hao, Y.; Zheng, C.; Qin, Y.; et al. Association of lung function in a panel of young healthy adults with various chemical components of ambient fine particulate air pollution in Beijing, China. Atmos. Environ. 2013, 77, 873–884. [Google Scholar] [CrossRef]
- Wu, S.; Deng, F.; Hao, Y.; Shima, M.; Wang, X.; Zheng, C.; Wei, H.; Lv, H.; Lu, X.; Huang, J.; et al. Chemical constituents of fine particulate air pollution and pulmonary function in healthy adults: The Healthy Volunteer Natural Relocation study. J. Hazard. Mater. 2013, 260, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Herbert, F.A.; Hessel, P.A.; Melenka, L.S.; Yoshida, K.; Nakaza, M. Respiratory Consequences of Exposure to Wood Dust and Formaldehyde of Workers Manufacturing Oriented Strand Board. Arch. Environ. Health Int. J. 1994, 49, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.-W.; Lin, Y.-Y.; Wu, T.-C.; Hong, C.-C.; Chan, C.-C.; Lung, S.-C.C. Workplace air quality and lung function among dental laboratory technicians. Am. J. Ind. Med. 2006, 49, 85–92. [Google Scholar] [CrossRef]
- Mandryk, J.; Alwis, K.U.; Hocking, A.D. Work-related symptoms and dose-response relationships for personal exposures and pulmonary function among woodworkers. Am. J. Ind. Med. 1999, 35, 481–490. [Google Scholar] [CrossRef]
- Mandryk, J.; Alwis, K.U.; Hocking, A.D. Effects of personal exposures on pulmonary function and work-related symptoms among sawmill workers. Ann. Occup. Hyg. 2000, 44, 281–289. [Google Scholar] [CrossRef]
- Mitchell, D.C.; Armitage, T.L.; Schenker, M.B.; Bennett, D.H.; Tancredi, D.J.; Langer, C.E.; Reynolds, S.J.; Dooley, G.; Mehaffy, J.; Mitloehner, F.M. Particulate Matter, Endotoxin, and Worker Respiratory Health on Large Californian Dairies. J. Occup. Environ. Med. 2015, 57, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Neghab, M.; Jabari, Z.; Shouroki, F.K. Functional disorders of the lung and symptoms of respiratory disease associated with occupational inhalation exposure to wood dust in Iran. Epidemiol. Health 2018, 40, e2018031. [Google Scholar] [CrossRef]
- Slaughter, J.; Koenig, J.Q.; Reinhardt, T.E. Association Between Lung Function and Exposure to Smoke Among Firefighters at Prescribed Burns. J. Occup. Environ. Hyg. 2004, 1, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Shah, D. Healthy worker effect phenomenon. Indian J. Occup. Environ. Med. 2009, 13, 77–79. [Google Scholar] [CrossRef]
- Anthonisen, N.R.; Connett, J.E.; Murray, R.P. Smoking and Lung Function of Lung Health Study Participants after 11 Years. Am. J. Respir. Crit. Care Med. 2002, 166, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yu, L.-Y.; Mu, H.-J.; Xing, L.-Y.; Li, Y.-X.; Pan, G.-W. Shape of concentration-response curves between long-term particulate matter exposure and morbidities of chronic bronchitis: A review of epidemiological evidence. J. Thorac. Dis. 2014, 6, S720–S727. [Google Scholar] [CrossRef]
- Pope, C.A., III; Burnett, R.T.; Krewski, D.; Jerrett, M.; Shi, Y.; Calle, E.E.; Thun, M.J. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke: Shape of the exposure-response relationship. Circulation 2009, 120, 941–948. [Google Scholar] [CrossRef]
- Edginton, S.; O’Sullivan, D.E.; King, W.; Lougheed, M.D. Effect of outdoor particulate air pollution on FEV1 in healthy adults: A systematic review and meta-analysis. Occup. Environ. Med. 2019, 76, 583–591. [Google Scholar] [CrossRef] [Green Version]
- Sin, D.D.; Wu, L.; Man, S.P. The relationship between reduced lung function and cardiovascular mortality: A population-based study and a systematic review of the literature. Chest 2005, 127, 1952–1959. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W.; Beeh, K.M.; Chapman, K.R.; Decramer, M.; Mahler, D.A.; Wedzicha, J.A. Minimal Clinically Important Differences in Pharmacological Trials. Am. J. Respir. Crit. Care Med. 2014, 189, 250–255. [Google Scholar] [CrossRef]
- Moshammer, H.; Panholzer, J.; Ulbing, L.; Udvarhelyi, E.; Ebenbauer, B.; Peter, S. Acute Effects of Air Pollution and Noise from Road Traffic in a Panel of Young Healthy Adults. Int. J. Environ. Res. Public Health 2019, 16, 788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debia, M.; Beaudry, C.; Weichenthal, S.; Tardif, R.; Dufresne, A. Characterization and control of occupational exposure to nanoparticles and ultrafine particles. In André Studies and Research Projects/Report R-777, Montréal, IRSST; IRSST: Montreal, QC, Canada, 2013. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Location | Design | N | Men, % | Age, years | Smokers, % | Exposure Context | Measurement and Exposure Duration | Pollutants and Mean Concentration |
|---|---|---|---|---|---|---|---|---|---|
| Environmental Studies | |||||||||
| Baccarelli et al. (2014) [53] | China | Panel | 120 | 66% | 33 | 39.1 | Traffic-related PM2.5 exposure in truck drivers and office workers | Personal: 8 h | PM2.5: 127 µg/m3 (drivers) and 94 µg/m3 (office workers) |
| Cakmak et al. (2014) [54] | Canada | Crossover | 61 | 46% | 24 | 0 | Near steel plant and college campus | Near Station: 24 h | PM2.5: 12.8 µg/m3 (plant) and 11.5 µg/m3 (campus) |
| * Cole et al. (2018) [23] | Canada | Crossover | 38 | 74% | 29 | 0 | Cycling in downtown (D) and residential (R) areas | Quasi-personal: 1 h | PM2.5: 6 µg/m3 (D) and 4.7 µg/m3 (R) |
| Dales et al. (2013) [28] | Canada | Crossover | 61 | 75% | 24 | 0 | Exposure near steel plant and college campus | Near Station: 24 h | PM2.5: 12.8 µg/m3 (plant) and 11.5 µg/m3 (campus) |
| † Girardot et al. (2006) [55] | USA | Panel | 354 | 43% | 43 | 0 | Exposure while hiking in a mountain | Near Station: 5 h | PM2.5: 15 µg/m3 |
| * Hao et al. (2017) [49] | China | Panel | 42 | 62% | 55 | 0 | Daily exposures to particles | Personal: 24 h | PM2.5: 146.5 µg/m3 |
| * Hu et al. (2018) [56] | China | Panel | 28 | 43% | 20.6 | 0 | Same day exposure to particles | Personal: 8 h | PM2.5: 65.1 µg/m3 |
| † Huang et al. (2016) [29] | China | Crossover | 40 | 42% | 24 | 0 | Exposure in a transport hub and park | Personal: 2 h | PM2.5: 162 µg/m3 (transport hub) and 53 µg/m3 (park) |
| Jarjour et al. (2013) [57] | USA | Crossover | 73 | 73% | 32 | 0 | Cycling on low traffic (LT) and high traffic (HT) routes | Personal: 2 h | PM2.5: 45 µg/m3 (LT) and 44 µg/m3 (HT) |
| Kubesch et al. (2015) [58] | Spain | Crossover | 28 | 46% | 34 | 0 | Exposure to high and low TRAP in combination with physical exercise | Quasi-Personal: 2 h | PM2.5: 30 µg/m3 (LT) and 80.1 µg/m3 (HT) |
| Liu et al. (2018) [27] | Taiwan | Panel | 100 | 50% | 46 | 0 | Daily exposure to particles | Central Station: 24 h | PM2.5: 25.6 µg/m3 |
| * Matt et al. (2016) [24] | Spain | Crossover | 30 | 50% | 36 | 0 | Exposure in high traffic (HT) and low traffic (LT) roads while performing physical activity | Near Station: 2 h | PM2.5: 39 µg/m3 (LT) and 82 µg/m3 (HT) |
| Mirabelli et al. (2015) [50] | USA | Crossover | 21 | 62% | 35 | 0 | Exposure while commuting | Quasi-Personal: 2 h | PM2.5: 28.8 µg/m3 |
| † Mirowsky et al. (2015) [30] | USA | Crossover | 23 | 48% | 25 | 0 | Walking near traffic routes | Quasi-Personal: 2 h | PM2.5: 20 µg/m3; PM10: 26 µg/m3 |
| † Thaller et al. (2008) [59] | USA | Panel | 142 | 79% | 19 | 27 | Beach guards exposed to ambient PM2.5 | Central Station: 8 h | PM2.5: 10.7 µg/m3 |
| * Vilcassim et al. (2019) [60] | USA | Panel | 34 | 32% | 27 | 0 | Exposure in different cities while travelling by plane | Central Station: 24 h | PM2.5: From 8.7 µg/m3 (New York) to 105 µg/m3 (East Asia) |
| * Weichenthal et al. (2011) [25] | Canada | Crossover | 42 | 67% | 35 | 0 | Cycling indoors, low traffic (LT) and high traffic routes (HT) | Quasi-Personal: 1 h | PM2.5: 2 µg/m3 (Indoor), 8.1 µg/m3 (LT) and 44 µg/m3 (HT) |
| † Wu et al. (2013 a) [61] | China | Panel | 40 | 100% | 20 | 0 | Exposure in suburban and urban areas | Central Station: 24 h | PM2.5: 75.2 µg/m3 (Suburban), 56.6 µg/m3 (Urban 1) and 48.8 µg/m3 (Urban 2) |
| † Wu et al. (2013 b) [62] | China | Panel | 21 | 100% | 20 | 0 | Exposure in suburban and urban areas | Central Station: 24 h | PM2.5: 75.2 µg/m3 (Suburban), 56.6 µg/m3 (Urban 1) and 48.8 µg/m3 (Urban 2) |
| † Zuurbier et al. (2011) [51] | Netherlands | Crossover | 34 | 70% | 42 | 0 | Commuting by bus, car, and by bike | Quasi-Personal: 2 h | PM2.5: 58 µg/m3 (vehicles) and 65.2 µg/m3 (bike) |
| Occupational Studies | |||||||||
| * Altin et al. (2002) [44] | Turkey | Cross-shift | 223 | 78% | 27 | 67 | Occupational exposure to cotton dust | Personal: 8 h | PM4: 413 µg/m3 |
| * Bakirci et al. (2006) [46] | Turkey | Cross-shift | 66 | 100% | NA | 79 | Occupational exposure to cotton dust | Quasi-Personal: 8 h | PM4: 1050 µg/m3 (delinting), 1870 µg/m3 (hulling) and 610 µg/m3 (baling) |
| * Bakirci et al. (2007) [45] | Turkey | Cross-shift | 157 | 20% | 52 | 31.2 | Occupational exposure to cotton dust | Personal: 8 h | PM4: 2390 µg/m3 |
| * Fell et al. (2011) [47] | Norway | Cross-shift | 70 | 92% | 41 | 41 | Occupational exposure to cement dust | Personal: 8 h | PM4: 300 µg/m3 |
| * Gaughan et al. (2014) [33] | USA | Cross-shift | 17 | 94% | 26 | 0 | Firefighters exposed to particles | Personal: 12 h | PM4: 490 µg/m3 |
| * Herbert et al. (1994) [63] | Canada | Cross-shift | 99 | NA | 35 | 27.9 | Occupational exposure to wood dust | Quasi-Personal: 6 h | PM4: 270 µg/m3 |
| Hu et al. (2006) [64] | Taiwan | Panel | 45 | 66% | 30 | 31.3 | Exposure in dental laboratories | Personal: 8 h | PM2.5: 107 µg/m3 |
| Mandryk et al. (1999) [65] | Australia | Cross-shift | 198 | 100% | 37 | 33 | Occupational exposure to wood dust | Personal: 8 h | PM4: 2170 µg/m3 (sawmill) and 1700 µg/m3 (joinery) |
| Mandryk et al. (2000) [66] | Australia | Cross-shift | 127 | 100% | 36 | 47.1 | Occupational exposure to wood dust | Personal: 8 h | PM4: 2260 µg/m3 (green mill) and 1460 µg/m3 (dry mill) |
| Mitchell et al. (2015) [67] | USA | Cross-shift | 205 | 100% | 34 | 24.4 | Dairy workers exposed to particles | Personal: 9.2 h | PM2.5: 35 µg/m3 (Workers) and 19.6 µg/m3 (Controls) |
| Neghab et al. (2018) [68] | Iran | Cross-shift | 200 | 100% | 37 | 41 | Occupational exposure to wood dust | Personal: 8 h | PM4: 6760 µg/m3 |
| * Slaughter et al. (2004) [69] | USA | Cross-shift | 65 | 80% | 29 | 16.9 | Firefighters exposed to particles | Personal: 8 h | PM4: 880 µg/m3 |
| * Ulfvarson and Alexandersson (1990) [48] | Sweden | Cross-shift | 24 | 100% | 35 | 0 | Exposure to diesel exhaust | Quasi-Personal: 8 h | PM4: 240 µg/m3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Silveira Fleck, A.; Sadoine, M.L.; Buteau, S.; Suarthana, E.; Debia, M.; Smargiassi, A. Environmental and Occupational Short-Term Exposure to Airborne Particles and FEV1 and FVC in Healthy Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10571. https://doi.org/10.3390/ijerph182010571
da Silveira Fleck A, Sadoine ML, Buteau S, Suarthana E, Debia M, Smargiassi A. Environmental and Occupational Short-Term Exposure to Airborne Particles and FEV1 and FVC in Healthy Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(20):10571. https://doi.org/10.3390/ijerph182010571
Chicago/Turabian Styleda Silveira Fleck, Alan, Margaux L. Sadoine, Stéphane Buteau, Eva Suarthana, Maximilien Debia, and Audrey Smargiassi. 2021. "Environmental and Occupational Short-Term Exposure to Airborne Particles and FEV1 and FVC in Healthy Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 20: 10571. https://doi.org/10.3390/ijerph182010571