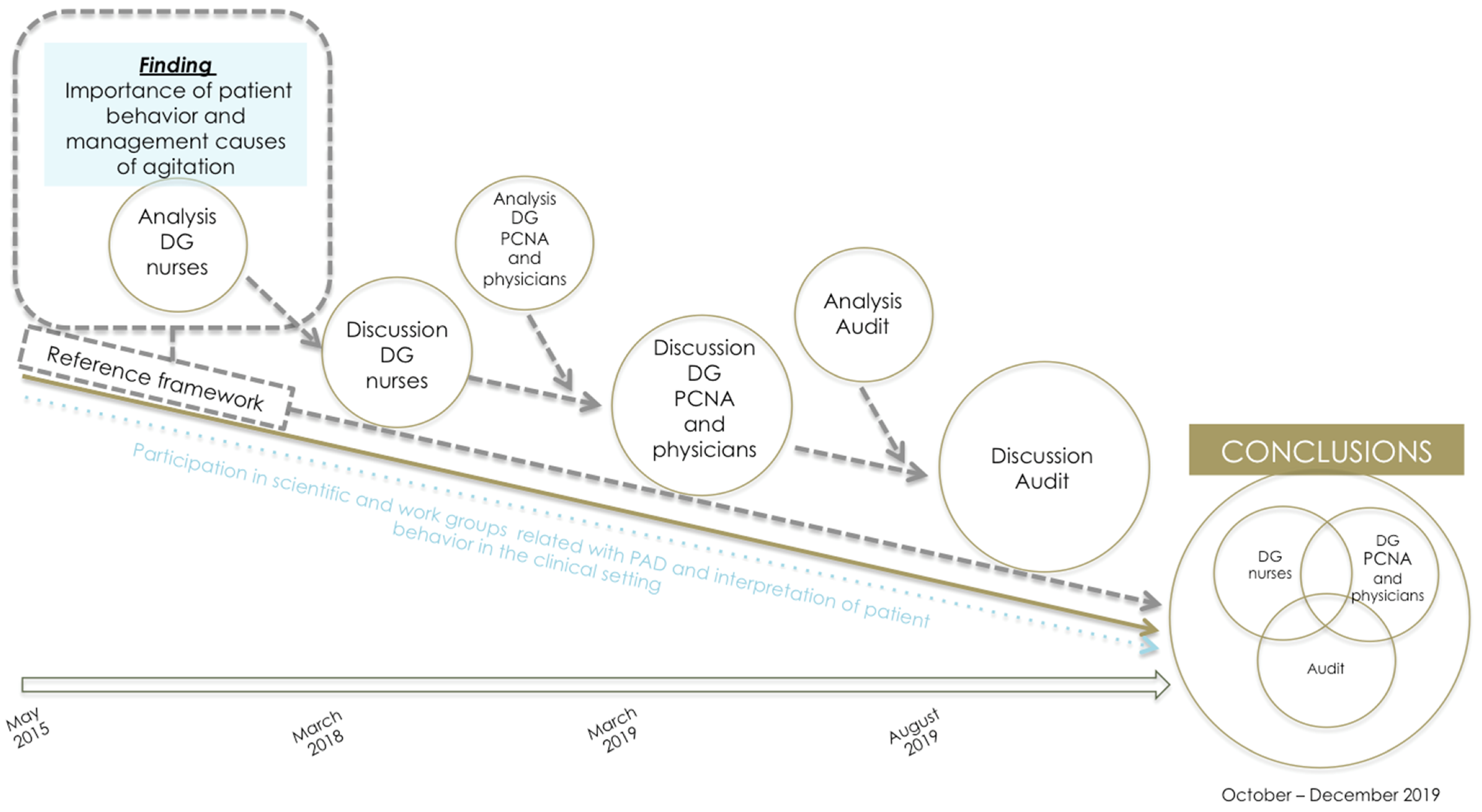
As a consequence of this cumulative and progressive integration of the findings of the different study components across the research process, a description of the results displays aspects that are at once explanatory and comparative. In light of the latter, we considered it opportune to merge the Results and Discussion sections by way of providing an internal dialogue between the contributions of the different components of the multimethod study, and a contrast with other external evidence.
4.1. Characteristics of the Clinical Context
In order to contextualize the findings on the decision-making process surrounding PR use as well as the factors that modulate this process, we propose to begin by setting out some of the results of the clinical audit that convey the reality of PR use at the 17 ICUs where the study was undertaken.
With respect to the characteristics of the ICU and in reference to the level of health care complexity, it should be noted that the mean nurse:patient ratio was 1:2 (range 1:1.25 to 1:3.62). Furthermore, it is likewise important to note that only 41.18% of the ICUs had a specific PR-management protocol, with specific training having been given at two of these units (
Table 6 and
Table 7).
A total of 1070 patients were observed, and of these, 194 had some type of PR, amounting to a median prevalence of PR use of the four observation periods of 19.11% (min: 0%–max: 44.44%)), with wide variability in both the overall group of patients and in those with ETT (
Table 7). These data are within the range of PR use found in other studies. While papers from the United Kingdom and Scandinavian countries report a prevalence of close on 0%, the equivalent figures were 76% in Canada, 39% in the USA, 43% in Italy, just under 23% in Holland, and 15.6 to 43.9% in Spain [
1,
21,
27,
90,
91,
92]. Our data indicate a prevalence of 42.10% (min: 0%–max: 76.92%) in patients with ETT. Studies undertaken in France, Japan, Jordan, and Canada report prevalence as high as 76.9% of patients with ETT [
5,
25,
27,
28,
47,
86,
93].
The most common PR location was on both upper extremities (85%). The most frequent adverse effects were edema in the area of application (39.65%), and increased agitation-disorientation-delirium (20.35%).
In accordance with the prevalence of PR use, ICUs were classified into compliers/non-compliers with the standard (prevalence of 15% or less). Of the 17 ICUs, five (29.41%) met the standard (
Table 7).
4.2. Awareness and Definition of the Problem: Safety and Prevention of Risk in Relation to PR Use
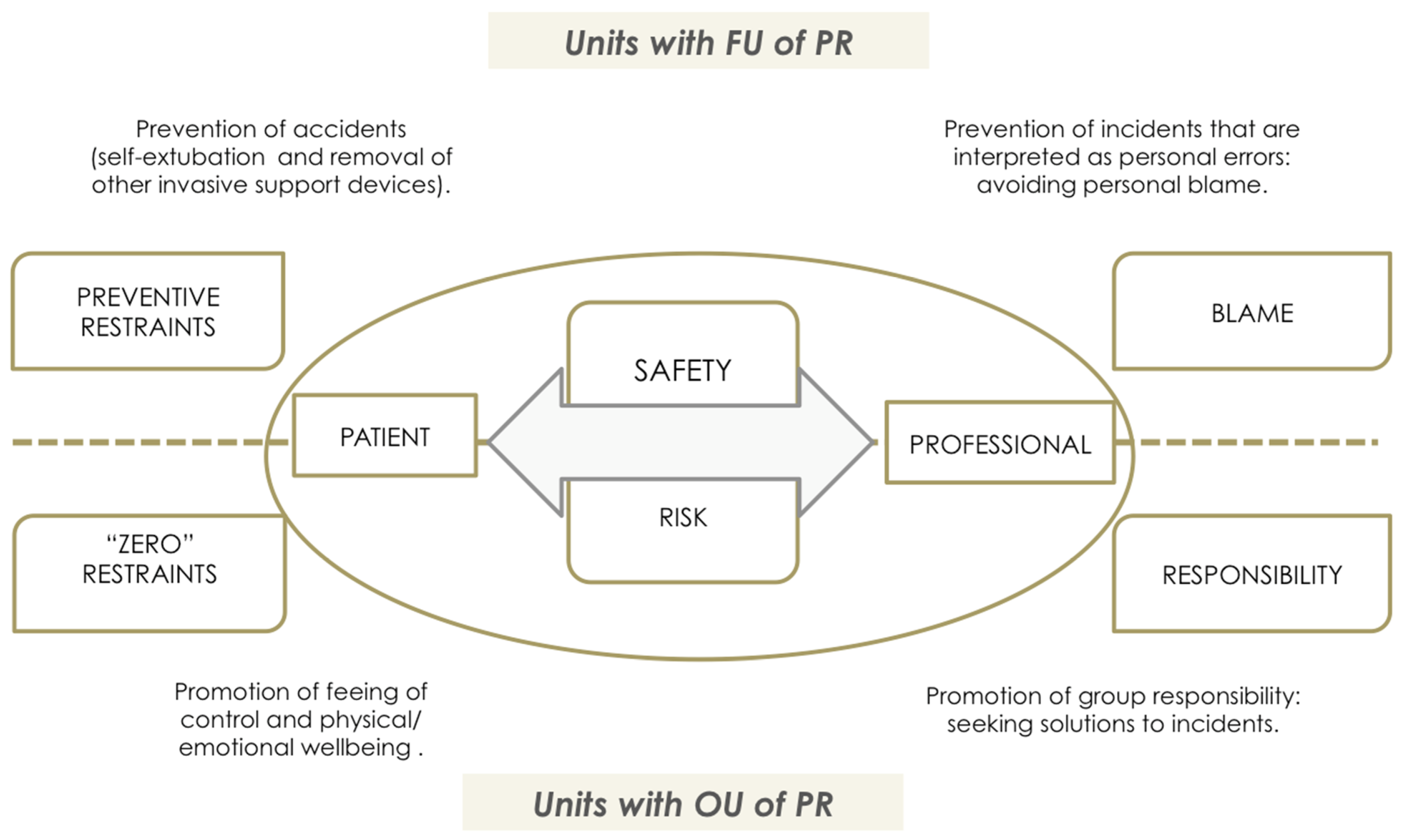
According to the participants’ discourse, the theoretical support underpinning PR use is the concept of safety and risk as perceived by health professionals. The concept of safety is thus envisaged from two perspectives that lie at opposite ends of a single continuum. These are safety in reference to the patient and safety in reference to the health professionals themselves vis-à-vis performance of their designated tasks (
Figure 7).
At an ICU with a FU of PR, the PCNA’s discourse is based on the prevention of risk (essentially risk of self-removal of invasive devices), a standpoint from which they conceptualize this as “preventive restraint”, along with avoidance of “blame” for causing accidents.
“Preventive restraint” refers to routine and systematic (non-individualized) use of PR with the idea of ensuring a patient’s safety. This preventive attitude assumes that all patients admitted to ICU (mainly those from whom sedation is being withdrawn in order to advance toward removal of mechanical ventilation) are exposed to universal risk situations (not considering the particular situation to which the patient is exposed and how they interact with it). This risk of experiencing accidents (such as self-extubations) is attributed to patient behavior such as psychomotor agitation, without taking into account the causes or the magnitude of the consequences of the risk or of the preventive interventions (restraint) themselves.
DG mixed physicians: “A patient who was awake was a little agitated and they already came in to put the wrist straps on him. I said: ‘‘What are you doing? I’m talking to him!’’ ‘‘No, no, it’s in case he becomes agitated”. Many patients, when they arrive back from operating theater, or if you’ve just intubated them, on come the wrist straps”.
In relation with health professional-oriented safety, there is a culture focused on defensive intervention aimed at minimizing any possible incidents that might be attributed to the health professional. “Preventive restraint” thus becomes a defensive shield to prevent incidents whilst one is the person directly in charge of the patient. Similarly, there is a lack of communication within the team, and an absence of individualized assessment or consensus-based protocols.
DG2-Nurses: “I feel that what you say about having the feeling of having your back covered is something that makes us afraid. It’s something that’s obvious, you probably lack the information and training at this level, and this lack of certainty of saying, “if certain things happen in what way could that affect me”, well it’s also something that leads you to say, “listen, first I protect myself, and..”.
This would be in line with some of the results of the clinical audit, which bear out the fact that the PR-application profile fundamentally corresponds to patients with AAs (82.47%) and ETT (68.04%) (
Table 8), with the most frequent indications for use being agitation (61.40%) and attempted self-removal of artificial airways (50.88%).
In contrast to “preventive restraint”, in units with OU of PR, the discourse of physicians, nurses, and PCNA is committed to the promotion of the patient’s well-being and comfort, rejecting protocolized interventions, and using individualized assessment to guide clinical judgment and decision-making. The goal here is PR use in the smallest number of cases, and always with an awareness (justified intervention, taking into account the possible complications arising from their use).
DG PCNA OU: “[…] use restraints as little as possible […] and in full awareness […]. Well... I don’t get the idea of preventive (restraint). That’s to say, if we’re already saying that the fact of applying therapeutic immobilization is a complicated matter, if we apply it preventively...What do we do? Do we restrain everyone before waking them up?”
DG mixed physicians: “See what you’ve done? I told you that you had to have him restrained”, and that starts creating a dynamic […] it’s a question of the overall dynamic of people, that’s to say the feeling of thinking that one shouldn’t do it […] other than in specific cases and specific moments, it has to be a collective thing because if there’s somebody less inclined to do so, how do you put him on the right track with the idea, “See what you’ve done?”
Furthermore, the concept of safety and professional risk is approached from a different perspective. Hence, at an ICU with OU, both physicians and PCNA see the risk of undesirable events as something intrinsic to professional practice, even though resources and advances in knowledge mean that these are less frequent and that safety in the workplace is far greater.
DG mixed physicians: “When it comes to really inevitable risks [...] there are very few; what happens is that, with current state of knowledge, there are things that, as of now, we are unable to prevent, but if you analyze all the factors that influence the famous Emmental cheese with all those holes, if you start covering those holes, there’ll come a day when it’ll be very difficult for those errors and those mistakes to occur”.
Thus, they do not perceive PR use as a means to prevent incidents that might reveal or highlight personal error in professional praxis: what they see instead is that the real solution to the occurrence of undesirable events is a feeling of group responsibility.
DG mixed physicians: “…it’s the fear of feeling guilty, and that they might blame you for something which you think could be a personal error, when really it’s the same old story, we’re going to look for someone to blame and we’re not going to look for solutions and the reasons why things happen […] working together with the whole team and not trying to find scapegoats …but solutions”.
DG-5-Nurses: “Anyway, things have changed a little since safety protocols were established, like now everybody’s more aware that, instead of going around blaming people all the time, looking for someone to blame, it’s necessary to look for a solution to this type of problem. I feel that this whole concept is gradually changing”.
In this context, the concept of safety acquires a more humanistic perspective, focused on the patient’s subjective experience and care from a holistic stance.
DG PCNA OU: [If we were to ask a patient, ‘What does being safe in an ICU mean to you?’, what would he say to us? Think about it]. “Being cared for, […] being accompanied, not feeling isolated. The fact of knowing that he’s being taken care of, monitored, protected. That he’s in the hands of good health professionals […] that he has trust in the professionals”.
With respect to this notion of health care quality and patient safety, in the clinical audit, an inverse correlation was found with overall PR prevalence and PR prevalence in patients with ETT of −43.15% and −52.14%, respectively (
Table 9): in other words, those ICUs that registered better use of restraints in terms of quality displayed a lower prevalence of PR use, both in the overall group of patients and in the subgroup of patients with ETT.
In relation with the above, there is an evident need for a cultural change, a conclusion and at the same time, a demand, that other authors have also contemplated [
2,
8,
38,
94,
95,
96]. In this regard, the principal reason cited by health professionals to justify PR use (i.e., “preservation of patient safety related with life-sustaining devices”) should be modified and shifted toward other meanings of the term “patient safety”, based on an updated reference framework. Conceptualization of the terms “safety/risk” from a biologistic standpoint is predominant in health care models in which PR use is frequent [
5,
38].
4.3. Needs Assessment: The Clinical Reasoning Underlying the Decision-Making Process
The qualitative findings yielded by examining the experience of ICU nurses showed that in units with FU of PR, the presence of artificial airways or the initiation of the process of weaning patients off mechanical ventilation is used to justify the practice as a way of preventing self-removal of life-sustaining devices, without there being any assessment of the need for their use. Accordingly, PR use could not be attributed to a decision-making process for the management of restraints: a clinical judgment of this nature would not appear to exist.
DG mixed physicians: “See what you’ve done? I told you that you had to have him restrained”, and that starts creating a dynamic that the patient is about to arrive, and the assistant says, “Do I restrain him?” What are you talking about, restrain him? He’s just come in, and you’ve got no idea of how he’s going to behave, he’s hardly in the room and you’re already restraining him. That’s why I say that it’s a question of the overall dynamic of people”.
This would be in line with the results of the clinical audit, which concluded that in 33.68% of cases, PRs are applied as a matter of ICU policy (i.e., without reflexive evaluation of the need for PR use in each case) (
Table 8).
While this reality might differ in an ICU with an OU of PR, where the health professionals acknowledge that such a decision-making process does indeed exist, they nonetheless experience difficulties when it comes to consciously putting it into words.
DG5 OU-nurses: “…in each nurse’s judgment [...]. On what do you base yourselves in order to take the decision? […] if I see, well, that during these mornings the patient is calm, I take advantage of the situation, I unfasten him [...] quietly observing him to see how he reacts […]. I continue to keep an eye on him. [...] Don’t you use anything on which to base your decision, a RASS score, a delirium scale, some element that would enable you to decide? […] If he’s clearly agitated, we restrain him, then there’s no turning back […], in a calm patient who answers you by nodding his head, well I don’t know, you just keep on watching…”.
In this connection, attention should be drawn to the differences found in the influence exerted by interpretation of the patient’s behavior on the indication for PR use or use of tools for assessment and management of the causes of agitation.
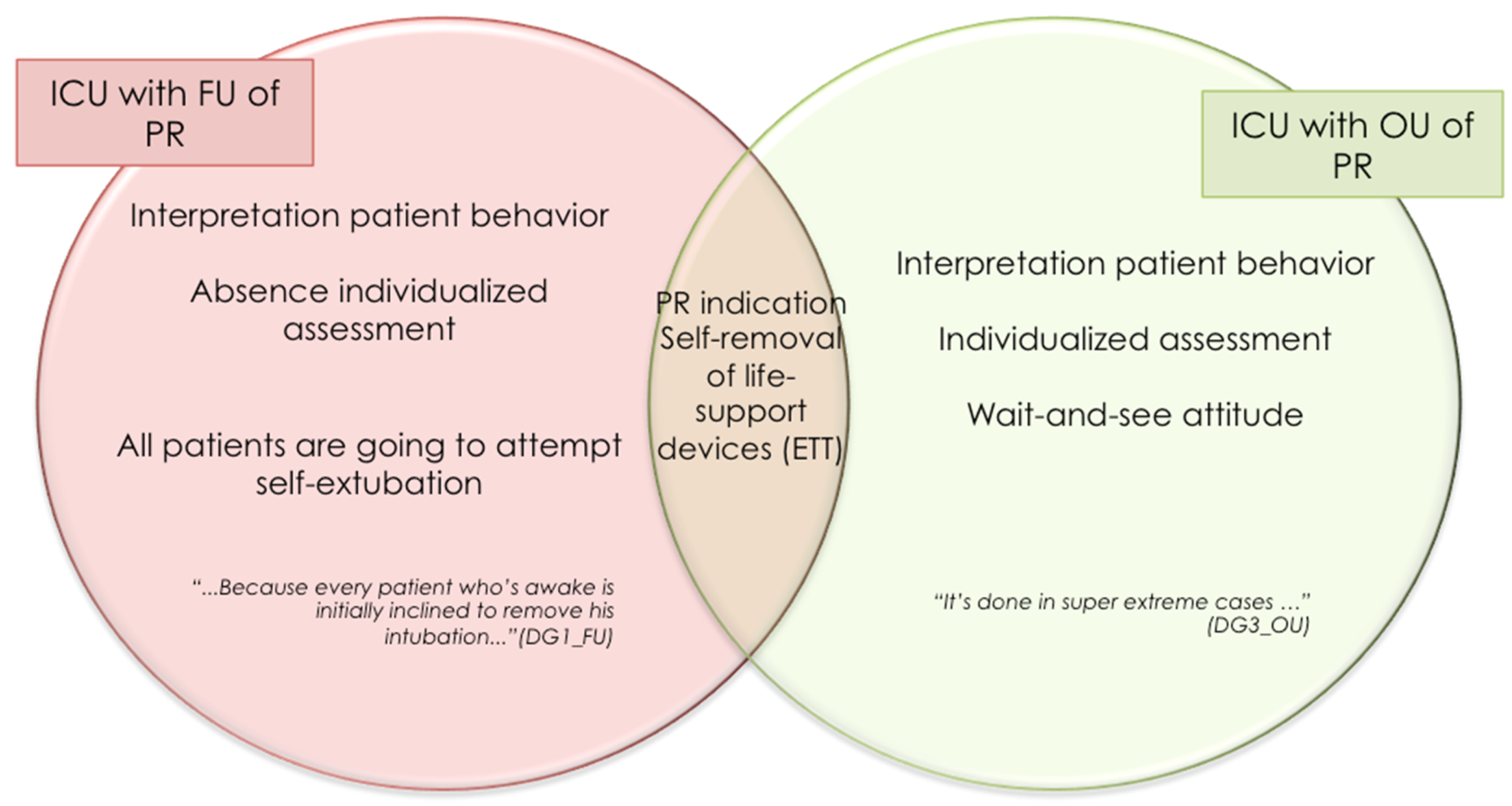
As can be seen in
Figure 8, in both subtypes of ICU, the indication for the use of restraints is the prevention of the self-removal of life-sustaining devices, however, there are differences in the way in which nurses interpret patient behavior. At an ICU with FU of PR, it is assumed that all patients are going to attempt self-extubation. In contrast to this, an ICU with OU of PR adopts a wait-and-see attitude, with the decision to apply or not to apply restraints being taken in accordance with the assessment of each patient.
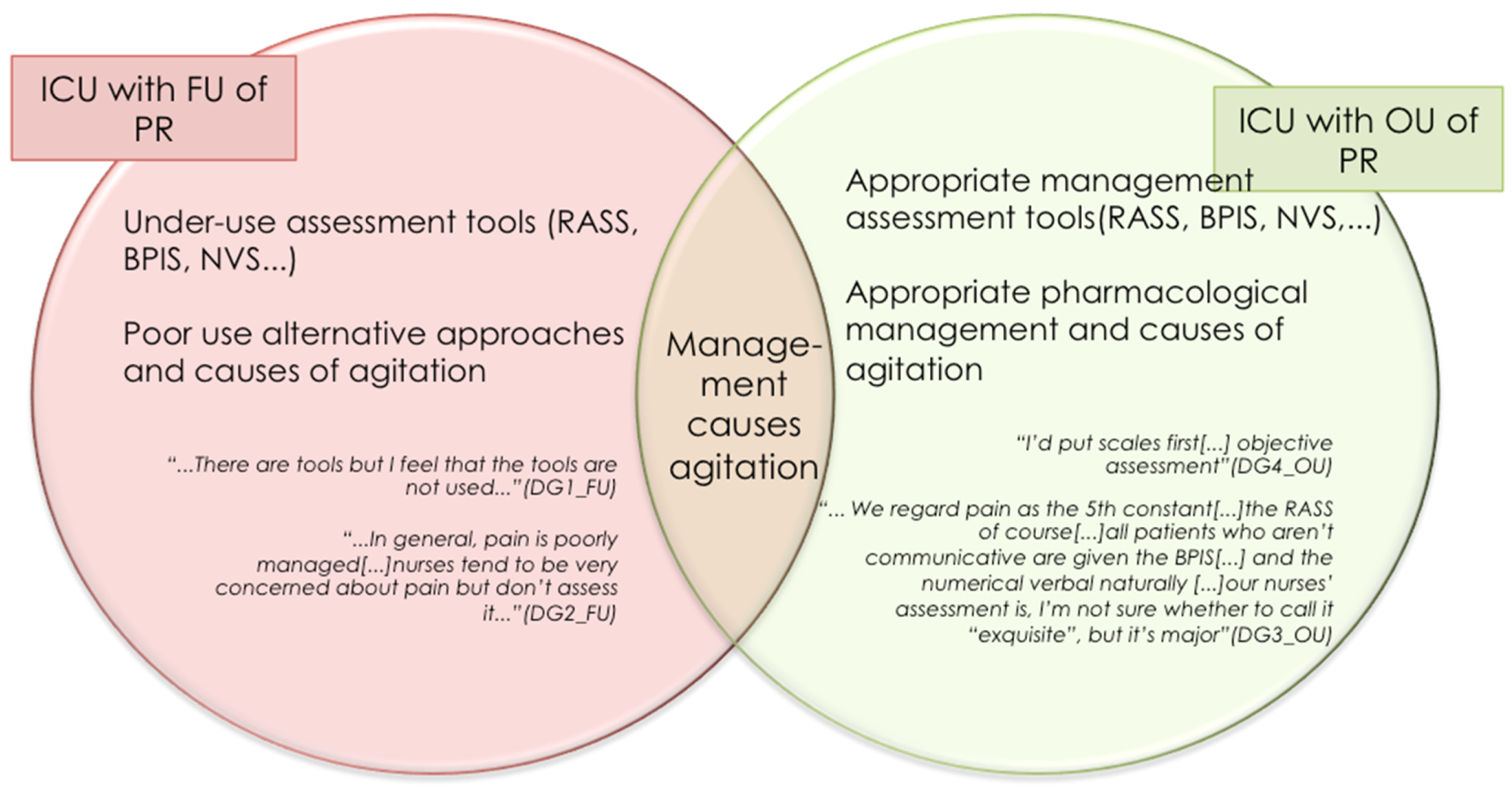
An ICU with OU of PR highlights the importance of the systematic use of validated tools for the assessment of pain, agitation/sedation, and delirium, with the use of these instruments being assumed to determine optimal use of pharmacological tools for the control of agitation. At an ICU with FU of PR, however, there is acknowledgment of the under-use of such tools and mismanagement of some causes of agitation such as pain (see
Figure 9).
With respect to the above, the clinical audit found that, when it came to the monitoring of pain, 64.71% of ICU did so appropriately in communicative patients and 35.29% did so in noncommunicative patients. Whereas 88.24% of ICU monitored sedation in accordance with the guidelines, only 11.76% did so in the case of delirium.
We analyzed the relationship between compliance with the standard and variables of PAD monitoring as well as the use of protocols and training of health professionals (
Table 9). Lower prevalence in the use of restraints was associated with appropriate monitoring of pain in noncommunicative patients (
p < 0.001). With regard to the association with the monitoring of delirium, no conclusions can be drawn, given the negligible number of ICUs that monitored delirium appropriately.
In our results, the most frequent indications for use were agitation, attempted removal of AAs and other devices, which might be related with pain or delirium [
2,
29,
97,
98]. As with other authors, our data indicate that monitoring of pain in noncommunicative patients and delirium are the least reliable elements in the interpretation of patient behavior [
21,
94,
99,
100]. Even so, the association found between appropriate monitoring of pain in noncommunicative patients and low prevalence of PR use is noteworthy, a situation that could be accounted for by better interpretation of patient behavior: a better understanding of pain behaviors in noncommunicative patients (facial muscle tension, frequent movements, increased muscle tone, lack of adaptation to mechanical ventilation, etc.) brings one closer to a better diagnosis and its subsequent treatment, and takes one away from the generic diagnostic label “agitated patient”, under which PR are sometimes applied somewhat unthinkingly. This same result would have been expected in the case of the monitoring of delirium, but the low prevalence of appropriate delirium monitoring in the sample meant that this could not be analyzed. This idea seems to be reinforced by the results such as those published by Pun, Hsieh or Gu, who argued that appropriate detection of both pain (in communicative and noncommunicative patients alike) and delirium would reduce the profiles of agitation and need of PR [
91,
97,
101].
4.4. Other Non-Clinical Elements That Influence Decision-Making about PR Use/Non-Use
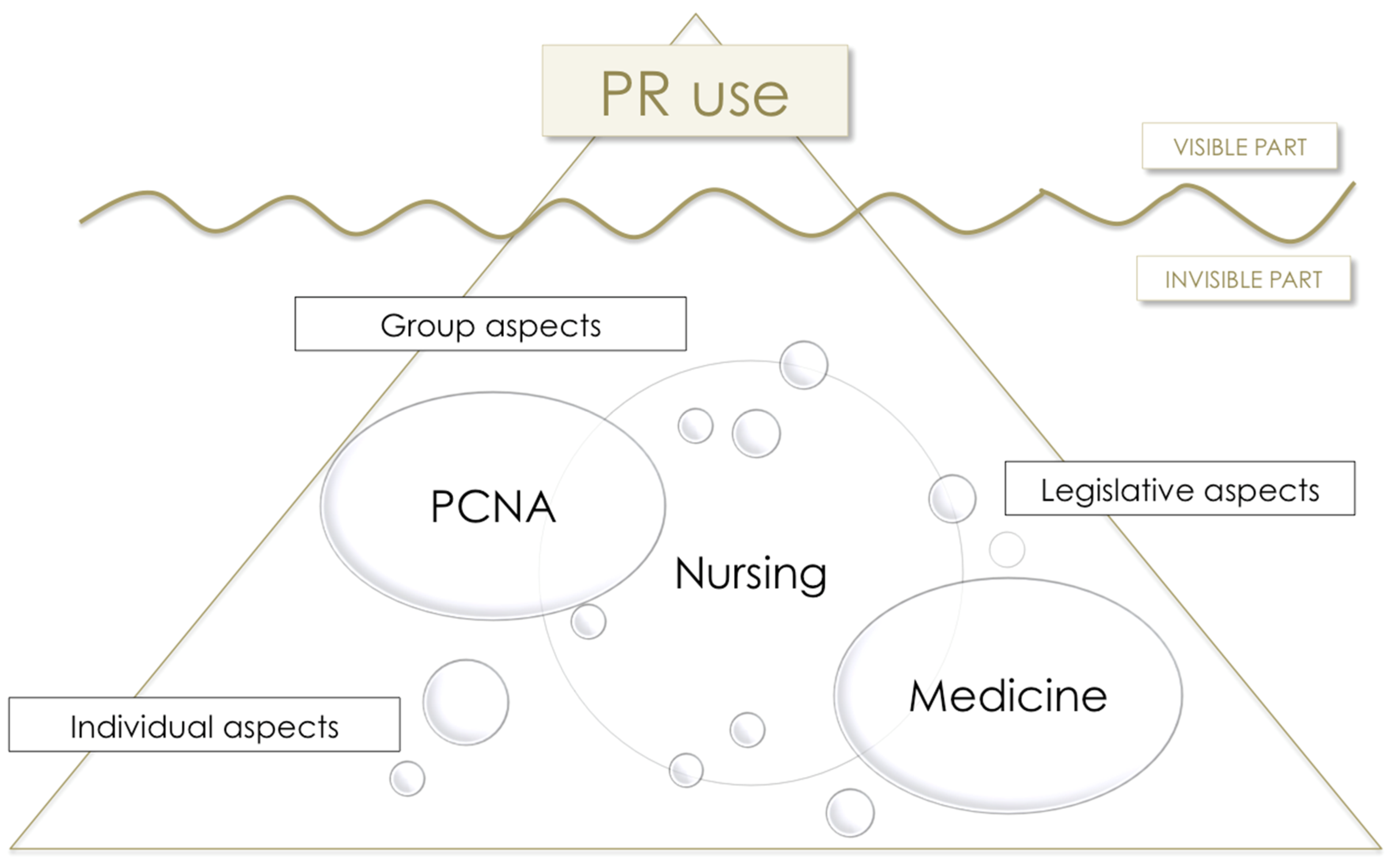
In the participants’ discourse, it was possible to identify a large variety of elements that influence use/non-use of PR and respond to the conceptual framework of the “Iceberg Theory”, the theoretical reference framework adopted as the point of departure.
According to studies conducted in settings other than critical patients [
3,
16,
17,
37,
39,
43,
48,
50,
102], health professionals cite the influence of individual, group, and organizational factors.
With respect to the first of these, mention should be made of: fear of physicians’ reaction to self-extubations (“…if he should remove the tube, they’ll kill me…” [DG1-nurses]); health professionals inflexibility when it comes to change (“…because it’s always been done like that…” [DG2]-nurses); and the interpretation put on patients’ behavior (“...attempted suicides […] are restrained from the outset, this is a person who’s tried to commit suicide […] is not of sound mind […] no-one gives it a second thought [...] it’s automatic [...] it’s one of those cases in which…, well, it’s a textbook case…” [DG1-nurses]).
Noteworthy among the group factors are: nurses being blamed for patient-related extubations (“…who’s to blame? The nurse […] your patient has become accidentally extubated... [...] It didn’t happen to the patient in the next bed, the nursing assistant or the doctor, but to you...” [DG1 nurses], “straight away they point the figure at you […] this was your mistake...” [DG2- nurses]); problems of communication between physicians and nurses (“...it depends on the nurse-doctor relationship...” [DG1-nurses], “...they don’t tell you that they’ve lowered the sedation dose...” [DG5-nurses]); pressure from the rest of the members of the group (“...You’ve also got to deal with your colleagues, which goes something like…And you’re not restraining him?’’...” [DG5-nurses]); and mismanagement in the unit of causes of agitation and assessment tools (“…we really do very little to find out what’s causing the agitation...” [DG2-nurses]), “....poor patient sedation ([…] he should be better sedated...” [DG5-nurses]). All of these are matters that could favor the use of restraints.
Finally, insofar as organizational factors are concerned, attention should be drawn to: restriction of family visiting hours (“…the family only spends 20 min here during the morning...” [DG1-nurses]); nurse:patient ratios; the architectural distribution of the ICU (“…it should be an open-plan ward, because then anyone passes through and sees it...” [DG3- nurses]); and allocation of workloads (“…we don’t follow them up because we don’t attend to them continuously...” [DG1-nurses], “... patient distribution, well you have one here and another there […] when it comes to sharing workloads, one of the things that should be borne in mind is patient safety” [DG4-nurses]).
In connection with the organizational factors, though health professionals of both subtypes of units acknowledged the influence of the nurse:patient ratio, it was noteworthy that the ratios were similar in the two subtypes of ICU (i.e., OU and FU). Hence, although this factor is considered relevant by nursing professionals, it may possibly not be quite so decisive in clinical practice [
26,
39,
45]. This hypothesis was explored using the results of the clinical audit by analyzing the possible relationship between optimal PR use, as shown by percentage compliance with the criteria considered, and institutional strategies (use of protocols or educational interventions), prevalence of PR, and nurse:patient ratios (
Table 9). No statistical relationship was found with the existence of a protocol, specific training, or ratios. Along these lines, the literature indicates that there are a number of authors who initially singled out the ratio as a variable associated with increased application of PR. However, other studies have shown wide differences in the use of restraints in countries with the same ratios as the United Kingdom or northern European countries, which not only have an average nurse:patient ratio of 1:1, but which also include figures such as respiratory therapists in their staff rota [
27,
103]. Even so, we agree with Luk et al. and Kandeel and Attia in asserting that, despite the fact that an optimal nurse:patient ratio is more than desirable, the effect on PR prevalence attributed a priori to the ratio may not be all that decisive [
23,
103]. With regard to the profile of ICU staff, aside from nurse:patient ratios, a number of authors have highlighted the importance of ICU skill and training levels when it comes to decision-making about PR use [
5,
104,
105].
4.5. Emotional Responses to Decision-Making about PR Use
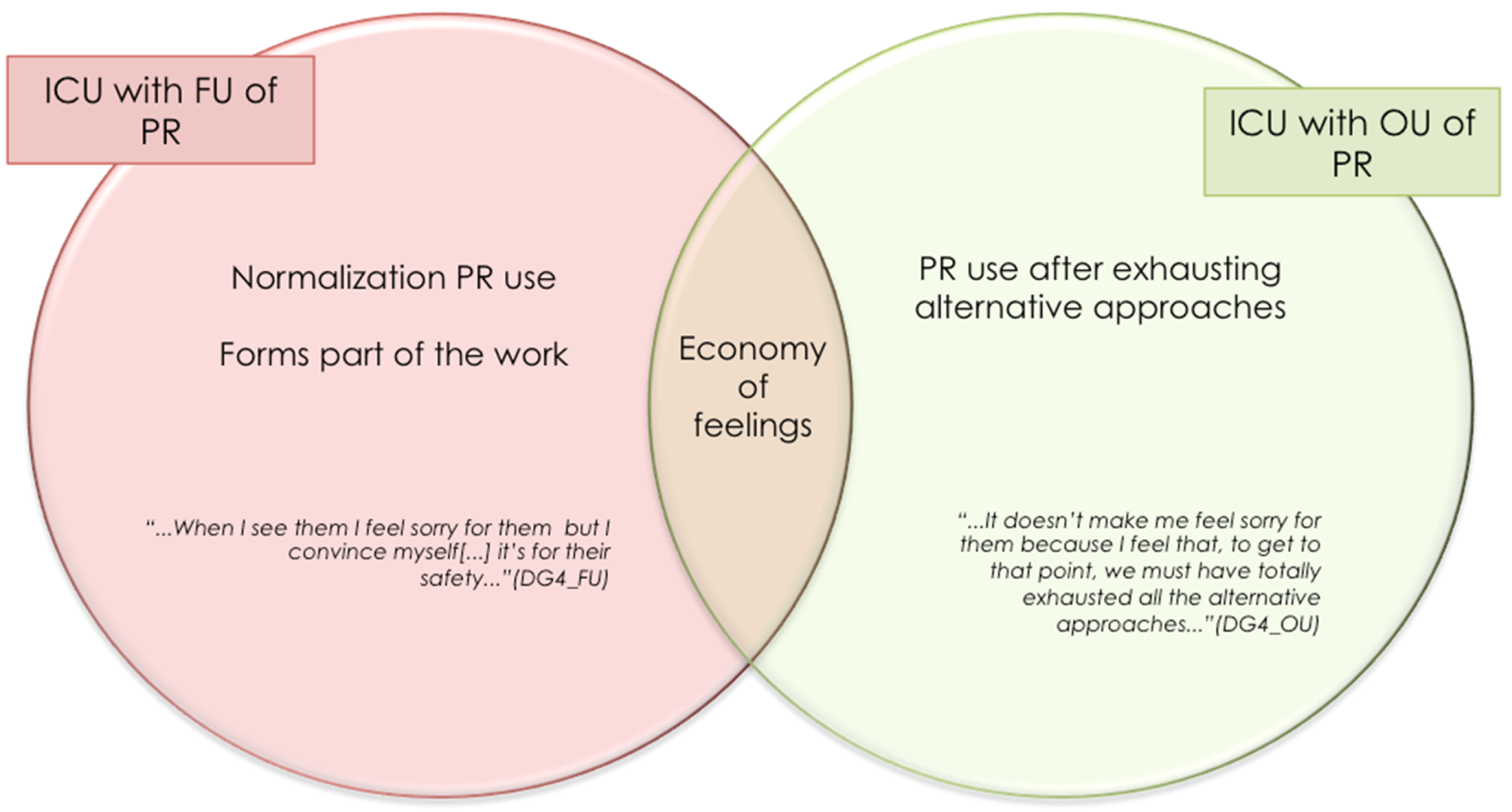
In the discourse of health professionals drawn from ICU with both FU and OU of PR, the subtopic of “economy of feelings” surfaces, in which health professionals voice the absence of feelings generated by managing patients with PR.
DG1-nurses: “...I don’t feel anything, good or bad...”,
DG4-OU-nurses: “...it’s part of your work, which you may or may not like to a certain extent [...] I don’t go home feeling any the worse…”.
In line with the “economy of feelings”, related concepts emerge such as “nurse’s helplessness”, which appears as a stance with respect to problem-solving and decision-making so that nurses find themselves propelled toward the application of restraints when they perceive that they have been left without tools for managing the patient or have lost motivation and/or confidence in themselves and the resources at their disposal. In the same way, as postulated by the theory of learned helplessness (Seligman and Maier, 1967) [
106], nurses, on seeing that their attempts to avoid PR use tend to fail systematically, allow themselves to be swayed by the dynamic of the unit
(“...applying restraints is also not the solution, that’s something we all understand, but what happens is that…” [DG3-nurses], “…it’s disagreeable, I also don’t like restraining them [...], but...” [DG5-nurses]).
Although “economy of feelings” is envisaged in both subtypes of ICU, significant differences can be seen in the cause of this emotional blunting in the face of an extreme measure such as physical restraint: at an ICU with FU, normalization of PR use could account for the suppression/minimization of feelings; at an ICU with OU of PR, however, this blunting of feelings might be related to the fact that restraints are only used when all alternative approaches have failed (
Figure 10).
While the “economy of feelings” referred to above might initially prove somewhat surprising, it is nevertheless in line with the data in the literature [
16,
43,
107] on other spheres in which health professionals report an absence of feelings on considering the use of restraints as forming part of their work (normalization of PR use) [
48]. Similarly, feelings of helplessness might justify the use of restraints as a nursing response in the face of the many problems that lie outside their professional scope [
48,
106,
108]. Inappropriate management, the elements cited as modulators of PR use, and the simultaneous demand for safety, may place health professionals in a predicament that they seek to resolve by using restraints.
4.6. The Emergence of a New Paradigm for Guiding the Decision-Making Process: “Zero Restraints”
The idea of working under a “zero-restraints” paradigm appears naturally and credibly in the discourse between PCNA from ICU with OU of PR and physicians.
DG mixed physicians: “When is it going to be of interest to us? Well, when everyone admits that what’s being done is not altogether right; perhaps we won’t get to 0% restraint use, but we can bring it down for sure […] there has to be some kind of aim or plan”.
DG-5 Nurses: “I believe we can restrain less because I’ve experienced it. Of course, the fact is I’ve seen it, so zero restraints, and I mean zero, zero, because I don’t know whether you’d need to restrain the patient in some specific case, but what I am sure of is that you can use restraints a lot less because truth is I’ve been there. And at the start, it was like “wow”. And when you see that you really could do it, when we made the break and continued with the same routine of making less use of restraints, well yes, there were people who removed the tube, but it wasn’t like we had a whole lot of extubations, more than before”.
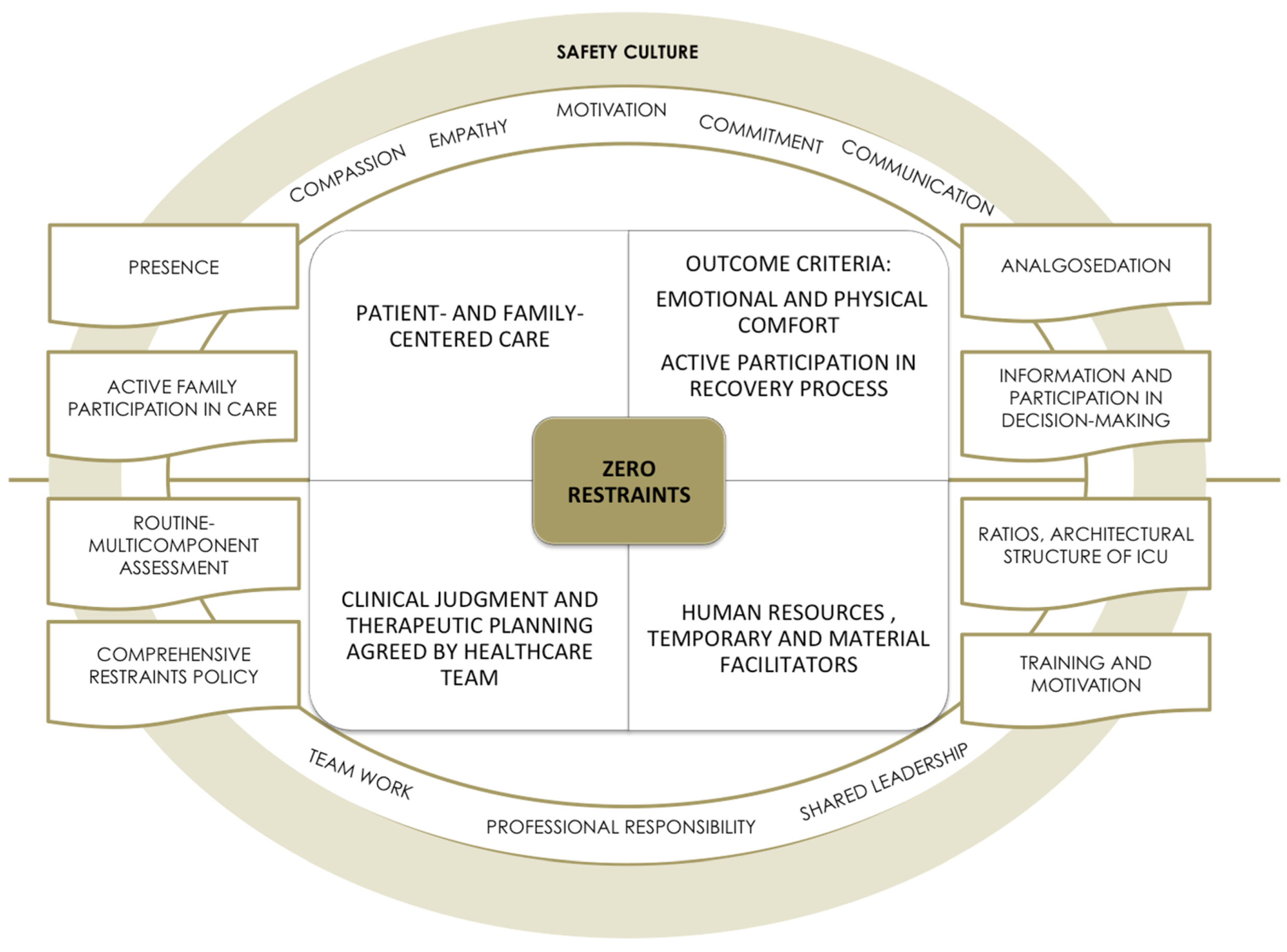
This approach is based on the following four premises: patient- and family-centered care; well-being-comfort and self-determination as outcome criteria; clinical judgment and planning of consensus-based interdisciplinary health care interventions; and the provision of adequate human and material resources (
Table 10).
Regarding the patient as the subject of care implies taking patient safety as the axis of care, placing clinicians in the role of advocacy, with this being construed as a role of preserving the patients’ safety and defending their rights and interests [
109]. From this standpoint, achievement of a subjective feeling of well-being and comfort is seen as a priority. Some key elements to facilitate such well-being are linked to the presence of a figure that would serve as a reference and effective support. In these participants’ discourse, this figure is represented by the nurse, though the family is seen as being able to contribute to the administration of emotional care with the appropriate support of nurses.
DG mixed physicians: “And then there’s another factor […] all these non-pharmacological and non-healthcare measures, such as family accompaniment for instance, that’s to say, many patients are much calmer if they have a person, a relative at their side, who helps them when they come round, to focus and, to…, that’s been demonstrated, there are many non-pharmacological actions that depend on the family or relatives, who help a lot to maintain these situations”.
DG-5 Nurses: “I think that another measure you were talking about before to try and reduce the number of restraints would be to also increase visits, I feel that this would also be a possible measure. What we ourselves do in the case of some patients is to increase visits for family relatives. Patients are much better off with their family”.
Furthermore, correct analgosedation is essential to place patients in the best condition to maintain their self-control and consciously participate in their recovery process. Providing the patient and family with information about clinical status and training in care are indispensable for making decisions and participating in caregiving, thereby achieving a feeling of control and self-esteem.
DG mixed physicians: “[…] until a few year ago, it was thought that the intensive-care patient had to be sedated and not […] he has to be wide awake, collaborating and in no pain, and if you succeed in this, ok the intubation will cause a little discomfort, but well […]”.
DG PCNA OU: “[…] if instead of applying therapeutic immobilization […] and a member of the family came in and sat there […] holding the man’s hand, the fact is he was quiet the whole afternoon […] there was no need to restrain him or anything”.
None of this is possible, however, without a consensus-based interdisciplinary approach based on in-depth knowledge of the patient and joint decision-making. A routine multicomponent assessment that envisaged PAD monitoring, the risk factors for its implementation, and the pertinence of the continuity of invasive devices, would be crucial in such a decision-making process. This integral and integrated interdisciplinary approach is reflected in the proposal of a “comprehensive restraints policy” and would imply the drawing up of joint-action protocols. In such a context, interpersonal communication (oral and written-recorded) is fundamental, as is formal regulation of the prescription of PR, which, being ambiguous, generates invisibility and a dilution of responsibilities.
DG PCNA OU: “[…] we’re all colleagues. […] I’ve never had a problem with nurses when I’ve told them my opinion, but talking about it, you know? Not pejoratively, always ‘‘no, it’s just that the nurse’’, no, we also have our part”.
DG mixed physicians: “[…] just as a nurse will say ‘‘listen, we’ve got blood sugar levels rising to 250 mg/dL, open me a line of insulin’’, she should tell you, ‘‘listen, look, with this patient there’s no way of keeping him calm, he scares me’’, and we assess it together […] it’s about expressing a joint problem. […] we’re not at the bedside 24 h a day […] its left to the nursing staff, nurses are competent, and many things that you’re not going to see in the 10 min you spend there on your rounds every shift or hour […] it’s very curious how even nursing assistants. […]. Maybe it’s a little about bringing the key element […] cohesion […] into the team, most of the problems begin right there, in the lack of a common goal and communication”.
With respect to human and material resources, different factors were identified that would foster the promotion of restraint-free ICUs (
Table 10). Examples of these are: an adequate nurse:patient ratio that would allow for nursing proximity and bedside presence; pharmacological resources for elective analgosedation; and team training in aspects of assessment and psycho-socio-emotional interventions.
Finally, attention should be drawn to a key guiding factor cited in the health professionals’ discourses, namely, motivation. The motivation required here is the kind that would impel the team toward a change in organizational and health care culture, something that would imply, first, becoming fully aware of how one was working and what the aim of one’s work was, and second, planning a transition strategy endowed with resources that would favor a harmonious and integrating process based on communication, team work, shared leadership, and compassionate, empathetic, and committed care.
DG mixed physicians: “Right, and no-one stops to think that maybe patients shouldn’t be restrained, and maybe we’re doing the wrong thing […] it’s also very difficult to break the… […] I see it as a problem that’s being trivialized and is something cultural, so it has to be changed [...] This has to be re-addressed as a non-trivial, non-routine measure, something that’s exceptional”.
DG-3 Nurses: “flexible positioning (is necessary). We’re dealing with persons and this isn’t a mathematical science: 2 + 2. There are many variables. Training and positioning (bearing in mind that everything’s relative, approximate and provisional)”.
All these elements, highlighted as crucial to progress toward the “zero-restraints” work paradigm in ICU, are shown in
Figure 11 below.
4.7. Joint Decision-Making: Overlapping Roles and Shared Responsibility in the Prescription of PR Use
Returning to the basic premises, by virtue of which patient safety would be construed as a collective responsibility, and decisions (the issuing of clinical opinions and treatment planning) would be based on consensus reached by health care teams, these give rise to the need to think about the prescription of PR use.
The findings show that physicians admit to trusting in the nurses’ judgment, considering them to have in-depth knowledge of the patients and their needs when it comes to guiding decision-making in the management of analgosedation and implementation of pharmacological measures (under nurse-driven protocols) as well as non-pharmacological measures. Furthermore, nurses are regarded by physicians and PCNA as the figure that centralizes information and serves as the manager of patient needs by coordinating therapeutic interventions. Furthermore, the nurse is acknowledged as being the professional carrying front-line responsibility for ensuring patient safety (with this being construed as a basic need or functional pattern). In this respect, their judgment, far from being questioned, is trusted and relied upon.
DG mixed physicians: “If a nurse tells me that she’s going to apply restraints to a patient, even though I may not agree, I trust her judgment”.
DG mixed physicians: “It’s just that I have doubts about the world of prescription because, for example, restraints are considered something that should be prescribed by a doctor, it’s the sort of thing they say, but on the other hand, restraints, at least in my hospital, have always been regarded as coming under the heading of safety, let’s say, and safety is part and parcel of nursing, so there’s never been any challenge or argument about who had to prescribe, and it’s always been the nurses who’ve done it on their own account. They can report it, there isn’t any kind of secretiveness, it’s simply that they’ve viewed it as their initiative, no-one’s ever mentioned it…”.
Notwithstanding the above, nurses demand support in decision-making, in that there are variables that influence and determine patient well-being and safety, and which depend on aspects of clinical and pharmacological management that come within the physicians’ scope of competence. The findings revealed opposing points of view, with feelings of empowerment on the one hand and vulnerability on the other.
DG Nurse-FU: “In my unit, for instance, they’re never prescribed […] that’s surprising when physical restraints should actually be prescribed. And as I feel unsure, well you’re scared that one of these days something’s going to happen and you’re going have to face the music”.
DG Nurse-FU: “It seems to me that there‘s no reason why restraints should come within the sphere of doctors, but (prescription) is a way of protecting ourselves legally and drawing up protocols […] I feel that what’s lacking is training in the management of restraints, PR use protocols that are really for the safety of the patient”.
What also emerges from the nurses’ discourse is the concept of “moral suffering” in relation to decision-making about the application of PR [
5,
41,
110]. They refer to the fact that their use must be agreed upon and never imposed by physicians, alluding to the fact that this sometimes entails a moral dilemma for them (i.e., those who apply the measure but do not agree with the appropriateness of its prescription).
DG Nurse FU: “But I’d like to explain to you that there are sure to be other measures to take and not just restraints, that a doctor can’t force you to restrain a person, because in that case, let him come down and do it himself. […] No, no, force me, no; force, no […] No, but maybe if he was the one who had to restrain the patient, then he might not be so ready to tell you to apply the restraints […] Yes obviously it’s really easy to delegate the job of applying a restraint or whatever, and that’s exactly why they don’t want to talk about it, because what they really do is delegate the job to somebody else, and that’s the person who actually applies the restraints”.
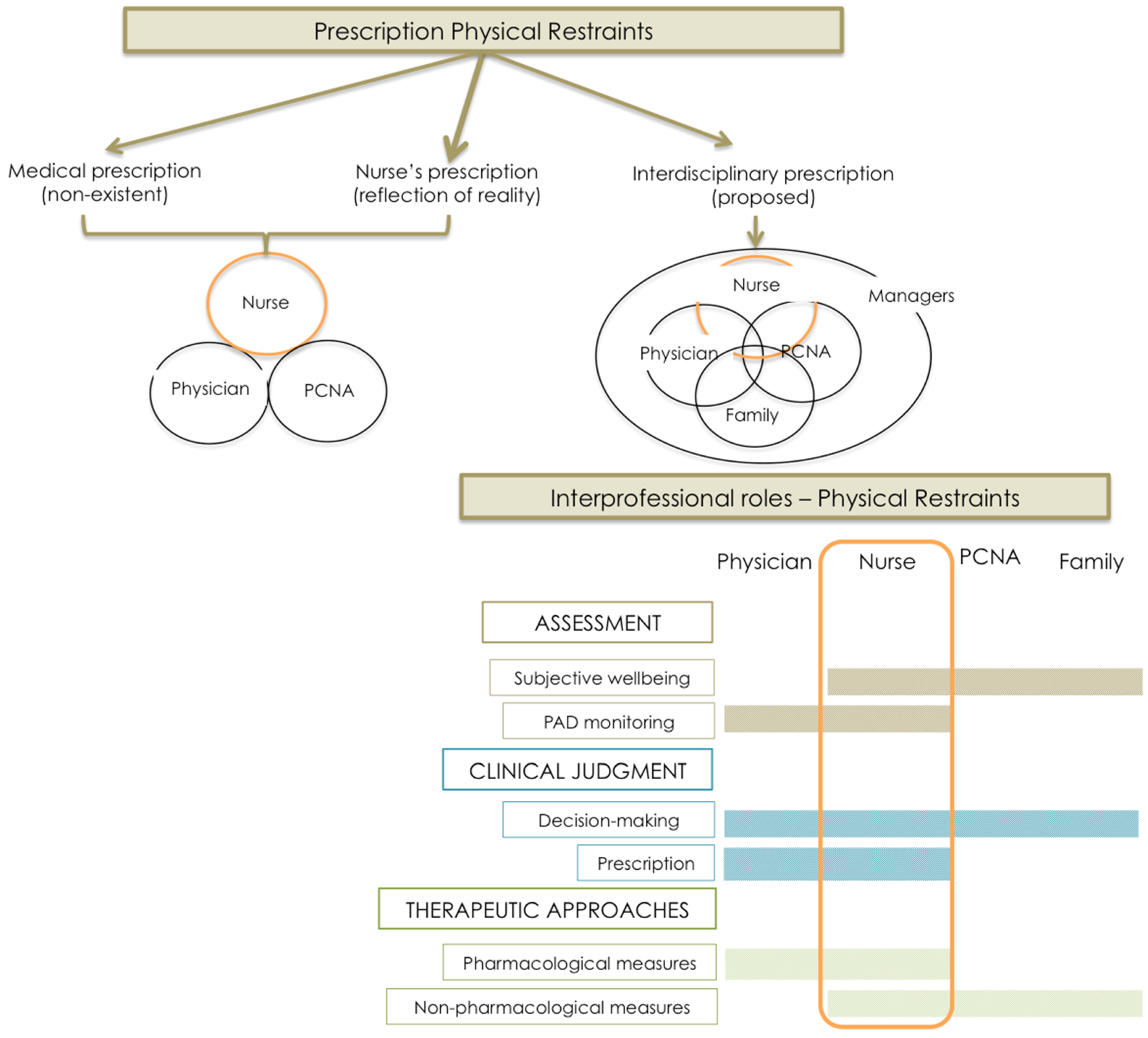
The current PR prescribing scenario at ICU around Spain seems to consist of the “nonexistence of medical prescription”, and the routinization and what one might call the “invisibilization” of decision-making [
5,
8]. In the participants’ discourse, however, the mere fact of airing and sharing points of view enables the possibility of joint prescribing to be raised as the ideal strategy for correct management of PR, acknowledging that it is a therapeutic measure that must be regarded as exceptional and, as a result, its prescription assessed with meticulousness, taking the views of the various members of the health care team into account. This proposal can be seen in
Figure 12, which shows the distribution and overlapping of tasks and responsibilities in the inter-disciplinary approach to a common goal. This same approach is taken in Belgium where, even though the local nurses are legally entitled to prescribe PR, the Belgians provide that the decision should always be made jointly by the health care team as a matter of shared responsibility [
111], something they describe as the “
interpersonal network as a forum for decision-making”.
DG mixed physicians: “[Prescription] really is something that we’ve left in the hands of the nursing staff and we pretty much try not to become involved […] Has it got to be a medical prescription? Well, I feel it ought to be a joint or delegated prescription. Seeing as it’s the nurse who’s at the bedside 24 h a day, or the nursing assistants. They should be the ones participating in this prescription, just as they participate in many other aspects of care. At present, it’s not like that, so in difficult situations they also look for support in the fact that there is or isn’t a medical prescription. Well, an agreement will have to be reached, it’ll have to be reviewed”.
DG mixed physicians: “This has to be re-addressed as a non-trivial, non-routine measure, something that’s exceptional, and that’s imbued with this exceptional nature because of its indications and joint prescription”.
As has already been noted, on discussing the process of taking judicious and consensus-based decisions, anxiety, agitation, and rest-sleep feature prominently as fundamental pillars of pain assessment. Integrated multidimensional information leads to planning of health care interventions at a pharmacological and non-pharmacological level, which in turn implies impeccable coordination among the various professional figures. Having come thus far, it is necessary to introduce another actor with a say in matters and operational capacity, namely, the family, which may exert a major influence. Taking Haines’ contributions [
112] as a reference, the family’s participation can be viewed as passing gradually from a transactional to a transitional phase and eventually becoming transformational, in other words, a progressive improvement in the dialogue between clinicians and the family. Hence, such a transformational participation would reach a maximum and translate as a true dialogue between clinicians and family as the result of a continuous interaction, which would guide decision-making, and ultimately lead to the design and implementation of pluralist decision-making models [
113]. These models should evolve from the family-centered health care model toward a “family engagement” model (with the family empowered and actively included in decision-making from a stance of commitment), where the role of the family unit would become proactive and its needs would be met in line with its values [
114].
In addition, the role of mid- and high-level managers should also be kept in mind. With regard to the latter, health care professionals highlight the passivity of managers with respect to PR use [
5]. These results seem to be in line with the lack of involvement of managers (nurses as well as physicians and PCNA) detected in the discourse.
DG1-nurses: “...the truth is, it’s always been done, everyone knows it, but no-one cares… It’s something that’s always there… and when I say no-one cares, I mean no-one… neither physicians, nor us, nor even my boss, who’s never given it a second thought”.
DG2-nurses: “...when there’s an extubation and they ask you if the patient was restrained… the physicians and the supervisor come to ask you why he wasn’t restrained…”
Institutional positioning and involvement could be crucial in achieving changes in clinical practice, with the introduction of policies and strategic lines that would generate a culture of restraint-free care and provide the structural resources (material and human) and necessary knowledge to implement it [
40].




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}











