
Self-Care by Muslim Women during Ramadan Fasting to Protect Nutritional and Cardiovascular Health

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
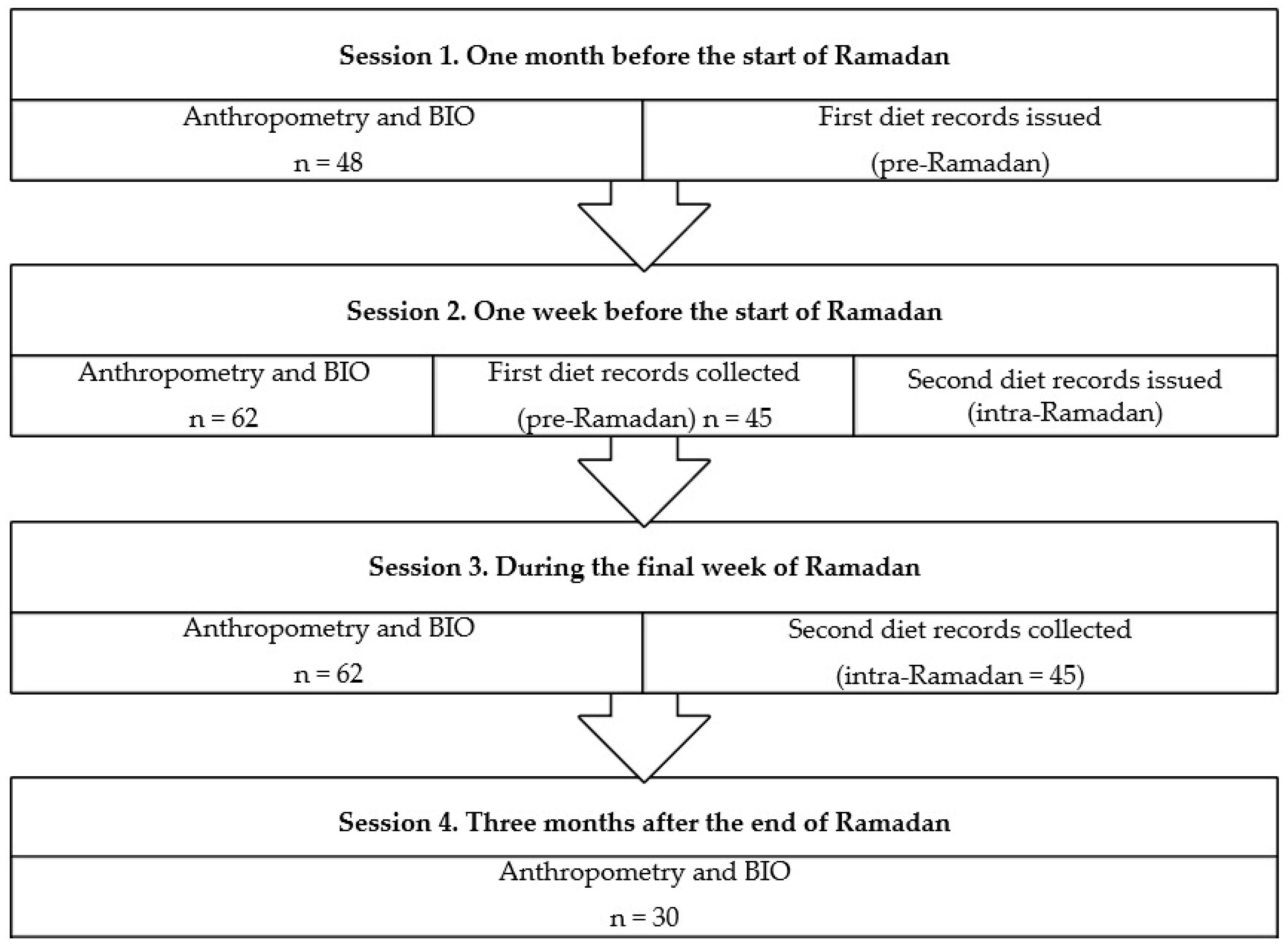
2.1. Study Design and Sampling
2.2. Data Collection
2.3. Anthropometric Evaluation and Body Composition Analysis
2.4. Food Consumption
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Anthropometric Measurements and Bioimpedance
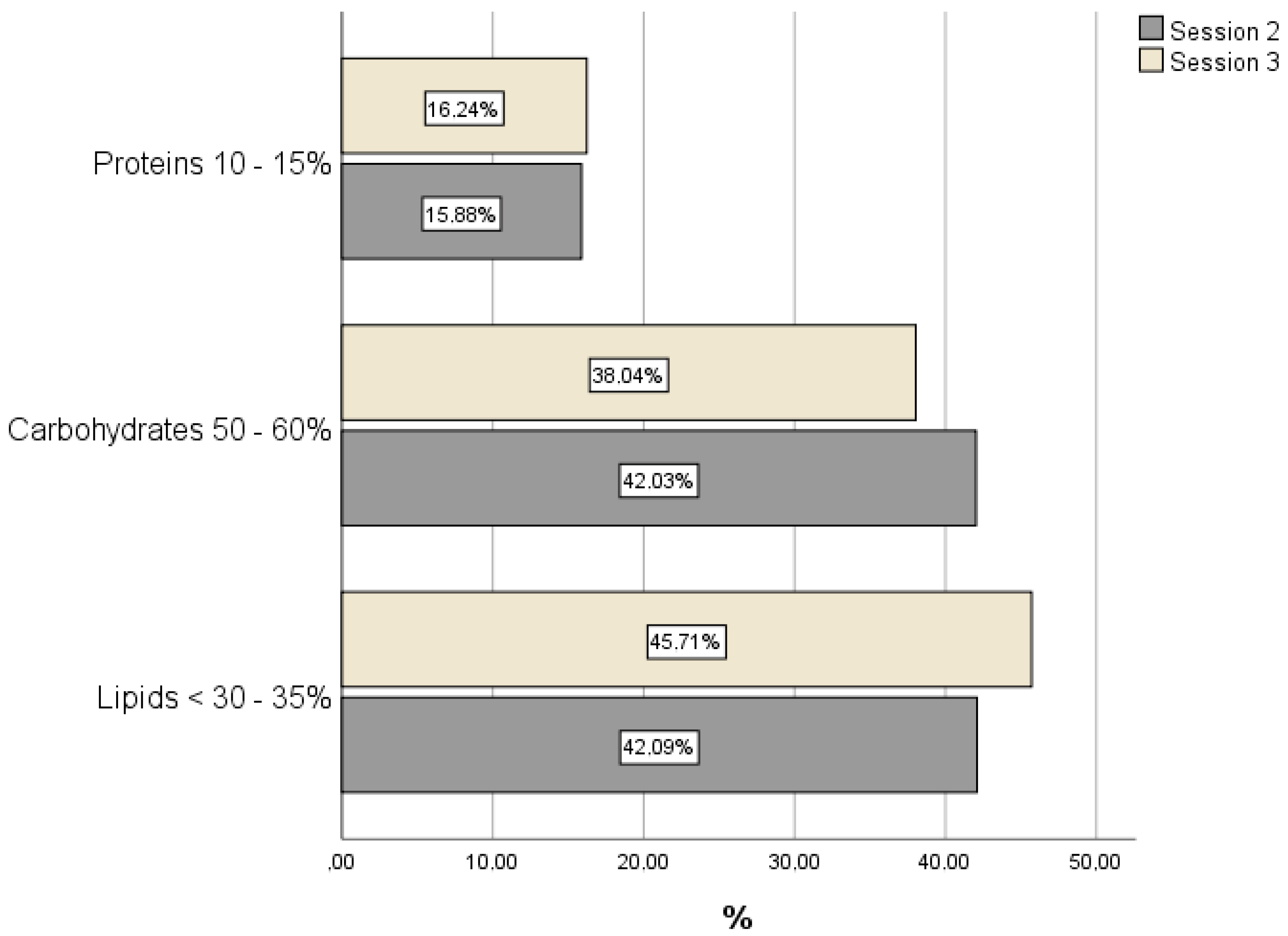
3.3. Dietary Intake: Macronutrients and Micronutrients
3.4. Cardiovascular Risk during Ramadan
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bakan, A.A.; Yildiz, S.; Alkan, A.; Yetis, H.; Kurtcan, S.; Ilhan, M.M. Microstructural Effects of Ramadan Fasting on the Brain: A Diffusion Tensor Imaging Study. Diagn. Interv. Radiol. 2015, 21, 256–261. [Google Scholar] [CrossRef]
- Harder-Lauridsen, N.M.; Rosenberg, A.; Benatti, F.B.; Damm, J.A.; Thomsen, C.; Mortensen, E.L.; Pedersen, B.K.; Krogh-Madsen, R. Ramadan Model of Intermittent Fasting for 28 d Had No Major Effect on Body Composition, Glucose Metabolism, or Cognitive Functions in Healthy Lean Men. Nutrition 2017, 37, 92–103. [Google Scholar] [CrossRef]
- Qasrawi, S.O.; Pandi-Perumal, S.R.; BaHammam, A.S. The Effect of Intermittent Fasting during Ramadan on Sleep, Sleepiness, Cognitive Function, and Circadian Rhythm. Sleep Breath. 2017, 21, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Terrón Caro, T. La Mujer En El Islam. Análisis Desde Una Perspectiva Socioeducativa. El Futur. Del Pasado 2012, 3, 237–254. [Google Scholar] [CrossRef]
- Varela Moreiras, G. Nutritional Problems in Spanish Women; Results from the ANIBES Study. Nutr. Hosp. 2015, 32, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Zomeño, M.D.; Dégano, I.R.; Pérez-Fernández, S.; Goday, A.; Vila, J.; Civeira, F.; Moure, R.; Marrugat, J. Excess Weight in Spain: Current Situation, Projections for 2030, and Estimated Direct Extra Cost for the Spanish Health System. Rev. Esp. Cardiol. (Engl. Ed.) 2019, 72, 916–924. [Google Scholar] [CrossRef]
- Vaamonde, J.G.; Álvarez-Món, M.A. Obesidad y Sobrepeso. Med.-Programa Form. Médica Contin. Acreditado 2020, 13, 767–776. [Google Scholar] [CrossRef]
- Konieczna, J.; Abete, I.; Galmés, A.M.; Babio, N.; Colom, A.; Zulet, M.A.; Estruch, R.; Vidal, J.; Toledo, E.; Díaz-López, A.; et al. Body Adiposity Indicators and Cardiometabolic Risk: Cross-Sectional Analysis in Participants from the PREDIMED-Plus Trial. Clin. Nutr. 2019, 38, 1883–1891. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; Ridder, H. International Standards for Anthropometric Assessment, 3rd ed.; International Society for the Advancement of Kinanthropometry: Lower Hutt, New Zealand, 2011. [Google Scholar]
- World Health Organization. Obesity and Overweight. Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 13 November 2021).
- Aranceta, J.; Majem, L.S. Objetivos Nutricionales Para La Población Española. Span. J. Community Nutr. 2011, 17, 178–199. [Google Scholar]
- FAO/WHO Expert Consultation on Fats and Fatty Acids in Human Nutrition. Interim Summary of Conclusions and Dietary Recommendations on Total Fat & Fatty Acids; World Health Organization: Geneva, Switzerland, 2008; pp. 1–14. [Google Scholar]
- Müller, M.J.; Braun, W.; Enderle, J.; Bosy-Westphal, A. Beyond BMI: Conceptual Issues Related to Overweight and Obese Patients. Obes. Facts 2016, 9, 193–205. [Google Scholar] [CrossRef]
- Memari, A.-H.; Kordi, R.; Panahi, N.; Nikookar, L.R.; Abdollahi, M.; Akbarnejad, A. Effect of Ramadan Fasting on Body Composition and Physical Performance in Female Athletes. Asian J. Sports Med. 2011, 2, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Rohin, M.A.K.; Rozano, N.; Abd Hadi, N.; Mat Nor, M.N.; Abdullah, S.; Dandinasivara Venkateshaiah, M. Anthropometry and Body Composition Status during Ramadan among Higher Institution Learning Centre Staffs with Different Body Weight Status. Sci. World J. 2013, 2013, 308041. [Google Scholar] [CrossRef] [Green Version]
- Nugraha, B.; Riat, A.; Ghashang, S.K.; Eljurnazi, L.; Gutenbrunner, C. A Prospective Clinical Trial of Prolonged Fasting in Healthy Young Males and Females—Effect on Fatigue, Sleepiness, Mood and Body Composition. Nutrients 2020, 12, 2281. [Google Scholar] [CrossRef] [PubMed]
- Agoumi, A.; López, M.J.O.; Martínez, F.M.; De La Serrana, H.L.G. Evaluating the Impact of the Ramadan Fasting on the Life Style and Health. Rev. Esp. Nutr. Comunitaria 2014, 20, 137–144. [Google Scholar] [CrossRef]
- Sezen, Y.; Altiparmak, I.; Erkus, M.; Kocarslan, A.; Kaya, Z.; Gunebakmaz, O.; Demirbag, R. Effects of Ramadan Fasting on Body Composition and Arterial Stiffness. J. Pak. Med. Assoc. 2016, 66, 1522–1527. [Google Scholar]
- Fahrial Syam, A.; Suryani Sobur, C.; Abdullah, M.; Makmun, D. Ramadan Fasting Decreases Body Fat but Not Protein Mass. Int. J. Endocrinol. Metab. 2016, 14, e29687. [Google Scholar] [CrossRef] [Green Version]
- Aguilar Shea, A.L.; Muñoz Moreno-Arrones, O.; Palacios Martínez, D.; Vaño-Galván, S. Vitamin D for Daily Practice. Semergen 2020, 46, 406–410. [Google Scholar] [CrossRef]
- Vorland, C.J.; Stremke, E.R.; Moorthi, R.N.; Hill Gallant, K.M. Effects of Excessive Dietary Phosphorus Intake on Bone Health. Curr. Osteoporos. Rep. 2017, 15, 473–482. [Google Scholar] [CrossRef]
- Chen, Q.; Zhang, Y.; Ding, D.; Li, D.; Yang, Y.; Li, Q.; Chen, X.; Hu, G.; Ling, W. Associations between Serum Calcium, Phosphorus and Mortality among Patients with Coronary Heart Disease. Eur. J. Nutr. 2018, 57, 2457–2467. [Google Scholar] [CrossRef]
- Marketou, M.E.; Maragkoudakis, S.; Anastasiou, I.; Nakou, H.; Plataki, M.; Vardas, P.E.; Parthenakis, F.I. Salt-induced Effects on Microvascular Function: A Critical Factor in Hypertension Mediated Organ Damage. J. Clin. Hypertens. 2019, 21, 749–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Evaluación Nutricional de La Dieta Española I. Energía y Macronutrientes. Sobre Datos de la Encuesta Nacional de Ingesta Dietética (ENIDE); Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2011; pp. 1–53.
- Del Pozo, S.; García, V.; Cuadrado, C.; Ruiz, E.; Valero, T.; Ávila, J.; Varela-Moreiras, G. Valoración Nutricional de la Dieta Española de Acuerdo al Panel de Consumo Alimentario; Fundación Española de la Nutrición (FEN): Madrid, Spain, 2012; pp. 1–142. [Google Scholar]
- Fernando, H.; Zibellini, J.; Harris, R.; Seimon, R.; Sainsbury, A. Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghirad, B.; Motaghipisheh, S.; Kolahdooz, F.; Zahedi, M.; Haghdoost, A. Islamic Fasting and Weight Loss: A Systematic Review and Meta-Analysis. Public Health Nutr. 2014, 17, 396–406. [Google Scholar] [CrossRef] [Green Version]
- Mazidi, M.; Rezaie, P.; Chaudhri, O.; Nematy, M. The Effect of Ramadan Fasting on Cardiovascular Risk Factors and Anthropometrics Parameters: A Systematic Review. Pak. J. Med. Sci. 2015, 31, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Elffers, T.W.; de Mutsert, R.; Lamb, H.J.; de Roos, A.; Willems van Dijk, K.; Rosendaal, F.R.; Jukema, J.W.; Trompet, S. Body Fat Distribution, in Particular Visceral Fat, Is Associated with Cardiometabolic Risk Factors in Obese Women. PLoS ONE 2017, 12, e0185403. [Google Scholar] [CrossRef] [Green Version]
- Silveira, E.A.; Noll, P.R.E.S.; Mohammadifard, N.; Rodrigues, A.P.S.; Sarrafzadegan, N.; de Oliveira, C. Which Diets Are Effective in Reducing Cardiovascular and Cancer Risk in Women with Obesity? An Integrative Review. Nutrients 2021, 13, 3504. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Liu, C.; Liu, X.; Pan, X.; Li, X.; Tian, L.; Sun, J.; Yang, S.; Zhao, R.; An, N.; et al. Effect of Epidemic Intermittent Fasting on Cardiometabolic Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Nutr. 2021, 8, 669325. [Google Scholar] [CrossRef] [PubMed]
- Greer, R.C.; Marklund, M.; Anderson, C.A.M.; Cobb, L.K.; Dalcin, A.T.; Henry, M.; Appel, L.J. Potassium-Enriched Salt Substitutes as a Means to Lower Blood Pressure. Hypertension 2020, 75, 266–274. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E. The Role of the Mediterranean Diet on Weight Loss and Obesity-Related Diseases. Rev. Endocr. Metab. Disord. 2020, 21, 315–327. [Google Scholar] [CrossRef]
- Kahan, D. Prevalence and Correlates of Adult Overweight in the Muslim World: Analysis of 46 Countries. Clin. Obes. 2015, 5, 87–98. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Mean ± SD |
|---|---|
| Age | 33.6 ± 12.7 |
| Number of children (n) | 1 ± 1.5 |
| Age at first Ramadan | 12.3 ± 1.8 |
| Marital status * | |
| Single | 35 (56.5) |
| Married | 21 (33.9) |
| Widowed | 2 (3.2) |
| Divorced | 4 (6.5) |
| Education * | |
| No formal education | 8 (12.9) |
| Basic or elementary | 23 (37.1) |
| Secondary | 16 (25.8) |
| Higher education | 15 (24.2) |
| Self-perception of present weight * | |
| Low | 4 (6.5) |
| Normal | 37 (59.7) |
| Overweight | 19 (30.6) |
| Obese | 2 (3.2) |
| Unknown | 1 (1.6) |
| Variables | Session 1 | Session 2 | Session 3 | Session 4 | p * | p ** |
|---|---|---|---|---|---|---|
| Weight (kg) | 67.3 ± 12.6 | 67.2 ± 14.1 | 66.1 ± 14.0 | 68.3 ± 13.5 | 0.894 | <0.001 |
| BMI (kg/m2) | 26.8 ± 6.4 | 26.3 ± 5.8 | 25.8 ± 5.6 | 26.4 ± 5.5 | 0.865 | <0.001 |
| Normoweight | 24 (50.0) | 29 (46.8) | 29 (46.8) | 14 (46.7) | ||
| Overweight | 9 (18.8) | 18 (29.0) | 21 (33.9) | 9 (30.0) | ||
| Obesity | 15 (31.2) | 15 (24.2) | 12 (19.3) | 7 (23.3) | ||
| Waist CF (cm) | 90.1 ± 11.9 | 90.1 ± 12.4 | 89.4 ± 12.4 | 90.3 ± 12.7 | 0.987 | 0.106 |
| Hip CF (cm) | 100.0 ± 12.5 | 99.0 ± 12.7 | 98.1 ± 12.7 | 100.0 ± 13.1 | 0.850 | 0.008 |
| W/Hp | 0.9 ± 0.0 | 0.9 ± 0.0 | 0.9 ± 0.0 | 0.9 ± 0.0 | 0.361 | 0.633 |
| W/Ht | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.967 | 0.104 |
| % Fat mass | 32.6 ± 9.0 | 32.1 ± 9.4 | 31.4 ± 9.5 | 33.2 ± 9.4 | 0.822 | <0.001 |
| Fat mass (kg) | 23.0 ± 9.8 | 22.8 ± 10.7 | 22.0 ± 10.5 | 23.7 ± 10.3 | 0.886 | <0.001 |
| Lean mass (kg) | 44.4 ± 3.9 | 44.7 ± 4.1 | 44.3 ± 4.05 | 44.6 ± 4.0 | 0.989 | 0.259 |
| Muscle mass (kg) | 42.1 ± 3.6 | 42.2 ± 3.9 | 42.0 ± 3.8 | 42.3 ± 3.8 | 0.991 | 0.286 |
| Total water (kg) | 31.3 ± 3.1 | 31.3 ± 3.4 | 31.1 ± 3.3 | 31.4 ± 3.3 | 0.980 | 0.182 |
| % Water | 47.4 ± 5.8 | 47.7 ± 6.0 | 47.6 ± 6.2 | 47.0 ± 6.0 | 0.960 | 0.897 |
| Visceral fat | 5.1 ± 4.0 | 5.0 ± 4.0 | 4.8 ± 3.8 | 5.1 ± 3.7 | 0.985 | 0.002 |
| Bone mass (kg) | 2.3 ± 0.2 | 2.3 ± 0.2 | 2.2 ± 0.2 | 2.3 ± 0.2 | 0.967 | 0.088 |
| Variables | Session 2 | Session 3 | p | Session 2 | Session 3 | p |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Median | Median | |||
| Energy (kcal) | 2292.8 ± 1576.0 | 3044 ± 1951.6 | 0.002 | 1880 | 2409.2 | 0.002 |
| Carbohydrates (g) | 240.9 ± 157.2 | 289.6 ± 127.2 | 0.002 | 224.0 | 257.0 | 0.002 |
| Protein (g) | 91.0 ± 63.42 | 123.3 ± 89.5 | 0.002 | 71.6 | 97.8 | 0.002 |
| Lipids (g) | 107.2 ± 93.1 | 154.7 ± 135.8 | 0.008 | 77.5 | 110.0 | 0.008 |
| SFA (g) | 31.3 ± 23.40 | 38.8 ± 24.76 | 0.075 | 25.7 | 31.6 | 0.075 |
| MFA (g) | 52.0 ± 51.16 | 80.6 ± 91.02 | 0.028 | 36.2 | 50.8 | 0.028 |
| PFA (g) | 14.0 ± 13.43 | 22.5 ± 14.73 | <0.001 | 10.0 | 19.7 | <0.001 |
| Cholesterol (mg) | 504.8 ± 969.01 | 658.3 ± 584.0 | <0.001 | 247.0 | 548.0 | <0.001 |
| Trans-fatty acids | 1.1 ± 1.2 | 1.6 ± 0.8 | 0.002 | 0.93 | 17,921.0 | 0.002 |
| Vitamin B2 (mg) | 2.4 ± 2.1 | 2.5 ± 1.9 | 0.223 | 1.8 | 1.9 | 0.223 |
| Niacin (mg) | 19.6 ± 16.4 | 27.5 ± 22.3 | 0.048 | 15.5 | 23.1 | 0.048 |
| Vitamin B6 (mg) | 2.7 ± 2.1 | 4.2 ± 3.3 | 0.001 | 1.9 | 3.1 | 0.001 |
| Folic acid (µg) | 317.1 ± 263.7 | 545.0 ± 593.73 | <0.001 | 243.0 | 358.0 | <0.001 |
| Vitamin D (µg) | 7.3 ± 10.9 | 5.4 ± 5.5 | 0.843 | 3.2 | 3.2 | 0.843 |
| Vitamin E (mg) | 11.6 ± 9.3 | 16.4 ± 14.5 | 0.012 | 8.8 | 11.0 | 0.012 |
| Iron (mg) | 18.8 ± 15.2 | 26.5 ± 18.7 | 0.001 | 12.9 | 20.2 | 0.001 |
| Iodine (µg) | 98.6 ± 81.2 | 130.0 ± 105.2 | 0.025 | 75.5 | 96.9 | 0.025 |
| Calcium (mg) | 928.2 ± 813.6 | 1017.3 ± 624.5 | 0.200 | 748.0 | 829.0 | 0.200 |
| Magnesium (mg) | 300.3 ± 165.9 | 449.3 ± 293.4 | <0.001 | 260.0 | 359,0 | <0.001 |
| Sodium (mg) | 2239.2 ± 1949.1 | 3162.1 ± 6386.7 | 0.731 | 1684.0 | 1864.0 | 0.731 |
| Potassium (mg) | 3189.1 ± 1657.8 | 5800.4 ± 4829.2 | <0.001 | 2795.0 | 4377.0 | <0.001 |
| Phosphorus (mg) | 1501.3 ± 1059.8 | 2049.5 ± 1273.6 | 0.001 | 1259.0 | 1642.0 | 0.001 |
| Vegetable fibre (g) | 23.2 ± 15.8 | 43.8 ± 32.0 | <0.001 | 19.7 | 34.5 | <0.001 |
| Variable | n | % | OR | 95% CI | OR a | 95% CI |
|---|---|---|---|---|---|---|
| Waist circumference (cm) | ||||||
| Normal | 19 | 48.7 | 1 | |||
| Elevated | 43 | 50.6 | 1.08 | 0.50; 2.30 | 1.11 | 0.46; 2.67 |
| W/Hp | ||||||
| Normal | 4 | 40.0 | 1 | |||
| Elevated | 58 | 50.9 | 1.55 | 0.42; 5.80 | 1.62 | 0.41; 6.41 |
| Fat mass (%) | ||||||
| Normal | 19 | 48.7 | 1 | |||
| Elevated | 43 | 50.6 | 1.08 | 0.50; 2.30 | 1.08 | 0.50; 2.37 |
| Visceral fat | ||||||
| Normal | 41 | 48.2 | 1 | |||
| Elevated | 21 | 53.8 | 1.25 | 0.59; 2.68 | 1.61 | 0.53; 4.89 |
| Sodium (mg) | ||||||
| Normal | 31 | 44.9 | 1 | |||
| Elevated | 31 | 56.4 | 1.58 | 0.78; 3.23 | 1.59 | 0.78; 3.24 |
| Potassium (mg) | ||||||
| Normal | 31 | 42.5 | 1 | |||
| Elevated | 31 | 60.8 | 2.10 * | 1.01; 4.35 | 2.14 * | 1.02; 4.47 |
| Saturated fatty acids (g) | ||||||
| Normal | 5 | 71.4 | 1 | |||
| Elevated | 57 | 48.7 | 0.38 | 0.07; 2.04 | 0.37 | 0.07; 2.03 |
| Monounsaturated fatty acids (g) | ||||||
| Normal | 29 | 65.9 | 1 | |||
| Elevated | 33 | 41.3 | 0.36 * | 0.17; 0.78 | 0.36 * | 0.17; 0.78 |
| Polyunsaturated fatty acids (g) | ||||||
| Normal | 0 | 0 | ||||
| Elevated | 62 | 50.0 | ||||
| Total cholesterol (mg) | ||||||
| Normal | 28 | 80.0 | 1 | |||
| Elevated | 34 | 38.2 | 0.16 ** | 0.06; 0.39 | 0.15 ** | 0.06; 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Bueno, M.; Fernández-Aparicio, Á.; González-Jiménez, E.; Montero-Alonso, M.Á.; Schmidt-RioValle, J. Self-Care by Muslim Women during Ramadan Fasting to Protect Nutritional and Cardiovascular Health. Int. J. Environ. Res. Public Health 2021, 18, 12393. https://doi.org/10.3390/ijerph182312393
López-Bueno M, Fernández-Aparicio Á, González-Jiménez E, Montero-Alonso MÁ, Schmidt-RioValle J. Self-Care by Muslim Women during Ramadan Fasting to Protect Nutritional and Cardiovascular Health. International Journal of Environmental Research and Public Health. 2021; 18(23):12393. https://doi.org/10.3390/ijerph182312393
Chicago/Turabian StyleLópez-Bueno, Marta, Ángel Fernández-Aparicio, Emilio González-Jiménez, Miguel Ángel Montero-Alonso, and Jacqueline Schmidt-RioValle. 2021. "Self-Care by Muslim Women during Ramadan Fasting to Protect Nutritional and Cardiovascular Health" International Journal of Environmental Research and Public Health 18, no. 23: 12393. https://doi.org/10.3390/ijerph182312393