
Relationships between Cognitive Functioning and Powered Mobility Device Use: A Scoping Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Registration
2.2. Data Sources and Searches
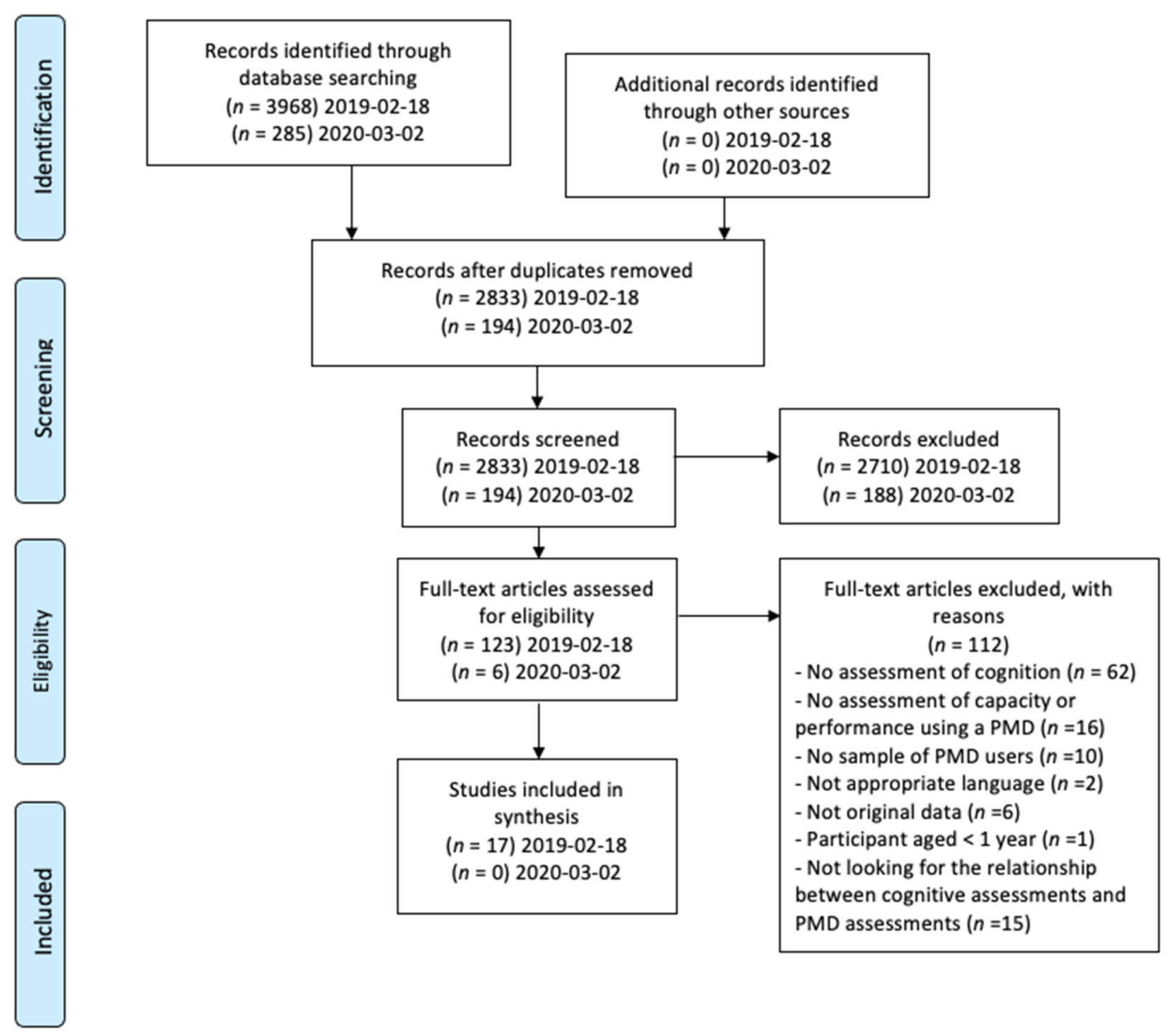
2.3. Study Selection
2.4. Appraisal of the Methodological Quality of Included Studies
2.5. Data Extraction and Synthesis
3. Results
3.1. Studies Looking for Predictive or Correlational Associations between PMD Mobility and Cognitive Outcomes (n = 4)
3.1.1. Children
3.1.2. Adults
3.1.3. Older Adults
3.2. Studies Exploring the Effects of a PMD Provision or Training on PMD Mobility and Cognitive Outcomes (n = 13)
3.2.1. Studies in Children
3.2.2. Studies in Adults
3.2.3. Studies in Older Adults
4. Discussion
4.1. Studies Looking for the Predictive or Correlational Associations between PMD Mobility and Cognitive Outcomes
4.2. Studies Exploring the Effects of a PMD Provision or Training on PMD Mobility and Cognitive Outcomes
4.3. Implications
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fasciglione, M. Article 20 [Personal Mobility]. In The United Nations Convention on the Rights of Persons with Disabilities; Della Fina, V., Cera, R., Palmisano, G., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 375–385. ISBN 978-3-319-43788-0. [Google Scholar]
- Brandt, Å.; Iwarsson, S.; Ståhle, A. Older People’s Use of Powered Wheelchairs for Activity and Participation. J. Rehabil. Med. 2004, 36, 70–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, D.M. Americans with Disabilities: 2014; US Census Bureau: Suitland-Silver Hill, ML, USA, 2018; pp. 70–152.
- Smith, E.M.; Giesbrecht, E.M.; Mortenson, W.B.; Miller, W.C. Prevalence of Wheelchair and Scooter Use among Community-Dwelling Canadians. Phys. Ther. 2016, 96, 1135–1142. [Google Scholar] [CrossRef] [Green Version]
- GOV.UK. National Wheelchair Data Collection. Available online: https://www.england.nhs.uk/statistics/2019/07/30/national-wheelchair-q1-201920/ (accessed on 9 August 2021).
- Sund, T.; Iwarsson, S.; Anttila, H.; Brandt, Å. Effectiveness of Powered Mobility Devices in Enabling Community Mobility-Related Participation: A Prospective Study among People with Mobility Restrictions. PM&R 2015, 7, 859–870. [Google Scholar] [CrossRef]
- Jones, M.A.; McEwen, I.R.; Neas, B.R. Effects of Power Wheelchairs on the Development and Function of Young Children with Severe Motor Impairments. Pediatric Phys. Ther. 2012, 24, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Bottos, M.; Bolcati, C.; Sciuto, L.; Ruggeri, C.; Feliciangeli, A. Powered Wheelchairs and Independence in Young Children with Tetraplegia. Dev. Med. Child Neurol. 2001, 43, 769. [Google Scholar] [CrossRef]
- Nilsson, L.M.; Eklund, M. Driving to Learn: Powered Wheelchair Training for Those with Cognitive Disabilities. Int. J. Ther. Rehabil. 2006, 13, 517–527. [Google Scholar] [CrossRef]
- Maywald, A.; Stanley, M. Prescribing Mobility Scooters in Australia: Occupational Therapists’ Narratives. Aust. Occup. Ther. J. 2015, 62, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Mortenson, W.B.; Clarke, L.H.; Best, K. Prescribers’ Experiences with Powered Mobility Prescription among Older Adults. Am. J. Occup. Ther. 2013, 67, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mockler, S.R.; McEwen, I.R.; Jones, M.A. Retrospective Analysis of Predictors of Proficient Power Mobility in Young Children With Severe Motor Impairments. Arch. Phys. Med. Rehabil. 2017, 98, 2034–2041. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; Version 1.0.; World Health Organization: Geneva, Switzerland, 2001; ISBN 978-92-4-056020-8. [Google Scholar]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, M.J.; Booth, A. A Typology of Reviews: An Analysis of 14 Review Types and Associated Methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Pellichero, A.; Kenyon, L.K.; Best, K.L.; Sorita, É.; Lamontagne, M.-E.; Lavoie, M.D.; Routhier, F. Influence of Cognitive Functioning on Powered Mobility Device Use: Protocol for a Systematic Review. JMIR Res. Protoc. 2020, 9, e16534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) Version 2018 for Information Professionals and Researchers. EFI 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Butler, C.; Okamoto, G.A.; McKay, T.M. Motorized Wheelchair Driving by Disabled Children. Arch. Phys. Med. Rehabil. 1984, 65, 95–97. [Google Scholar] [PubMed]
- Furumasu, J.; Guerette, P.; Tefft, D. Relevance of the Pediatric Powered Wheelchair Screening Test for Children with Cerebral Palsy. Dev. Med. Child. Neurol. 2004, 46, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.A.; McEwen, I.R.; Hansen, L. Use of Power Mobility for a Young Child with Spinal Muscular Atrophy. Phys. Ther. 2003, 83, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Kenyon, L.K.; Farris, J.P.; Gallagher, C.; Hammond, L.; Webster, L.M.; Aldrich, N.J. Power Mobility Training for Young Children with Multiple, Severe Impairments: A Case Series. Phys. Occup. Ther. Pediatrics 2017, 37, 19–34. [Google Scholar] [CrossRef]
- Kenyon, L.K.; Farris, J.P.; Aldrich, N.J.; Rhodes, S. Does Power Mobility Training Impact a Child’s Mastery Motivation and Spectrum of EEG Activity? An Exploratory Project. Disabil. Rehabil. Assist. Technol. 2018, 13, 665–673. [Google Scholar] [CrossRef]
- Lynch, A.; Ryu, J.-C.; Agrawal, S.; Galloway, J.C. Power Mobility Training for a 7-Month-Old Infant with Spina Bifida. Pediatric Phys. Ther. 2009, 21, 362–368. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, L.; Nyberg, P. Driving to Learn: A New Concept for Training Children With Profound Cognitive Disabilities in a Powered Wheelchair. Am. J. Occup. Ther. 2003, 57, 229–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tefft, D.; Guerette, P.; Furumasu, J. Cognitive Predictors of Young Children’s Readiness for Powered Mobility. Dev. Med. Child Neurol. 1999, 41, 665–670. [Google Scholar] [CrossRef]
- Benford, F. Use of Powered Mobility for a Young Adult with Profound and Multiple Learning Disabilities: A Practice Analysis. Br. J. Occup. Ther. 2017, 80, 517–520. [Google Scholar] [CrossRef]
- Kenyon, L.K.; Farris, J.; Brockway, K.; Hannum, N.; Proctor, K. Promoting Self-Exploration and Function Through an Individualized Power Mobility Training Program. Pediatric Phys. Ther. 2015, 27, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Massengale, S.; Folden, D.; McConnell, P.; Stratton, L.; Whitehead, V. Effect of Visual Perception, Visual Function, Cognition, and Personality on Power Wheelchair Use in Adults. Assist. Technol. 2005, 17, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Mountain, A.D.; Kirby, R.L.; Smith, C.; Eskes, G.; Thompson, K. Powered Wheelchair Skills Training for Persons with Stroke: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2014, 93, 1031–1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullen, B.; O’Neill, B.; Evans, J.J. Neuropsychological Predictors of Powered Wheelchair Use: A Prospective Follow-up Study. Clin. Rehabil. 2008, 22, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Thornton, H. Can Patients with Unilateral Neglect Following Stroke Drive Electrically Powered Wheelchairs? Br. J. Occup. Ther. 2003, 66, 496–504. [Google Scholar] [CrossRef]
- Mountain, A.D.; Kirby, R.L.; Eskes, G.A.; Smith, C.; Duncan, H.; MacLeod, D.A.; Thompson, K. Ability of People With Stroke to Learn Powered Wheelchair Skills: A Pilot Study. Arch. Phys. Med. Rehabil. 2010, 91, 596–601. [Google Scholar] [CrossRef]
- Mioshi, E.; Dawson, K.; Mitchell, J.; Arnold, R.; Hodges, J.R. The Addenbrooke’s Cognitive Examination Revised (ACE-R): A Brief Cognitive Test Battery for Dementia Screening. Int. J. Geriat. Psychiatry 2006, 21, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.A.; Evans, J.J.; Emslie, H.; Alderman, N.; Burgess, P. The Development of an Ecologically Valid Test for Assessing Patients with a Dysexecutive Syndrome. Neuropsychol. Rehabil. 1998, 8, 213–228. [Google Scholar] [CrossRef]
- Wilson, B.A.; Cockburn, J.; Halligan, P. Behavioural Inattention Test; Thames Valley Test, Co.: Bury St. Edmunds, UK, 1987; ISBN 978-0-9514322-2-8. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Patterson, J. F-A-S Test. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 1024–1026. ISBN 978-0-387-79947-6. [Google Scholar]
- Colarusso, R.; Hammill, D.D. MVPT-3rd: Motor-Free Visual Perception Test; Manual, 3rd ed.; Academic Therapy Publications: Novato, CA, USA, 2003; ISBN 978-1-57128-287-3. [Google Scholar]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Money, J.; Alexander, D.; Walker, H.T. A Standardized Road-Map Test of Direction Sense: Manual; Johns Hopkins Press: Baltimore, ML, USA, 1965. [Google Scholar]
- Nilsson, L.; Eklund, M.; Nyberg, P.; Thulesius, H. Driving to Learn in a Powered Wheelchair: The Process of Learning Joystick Use in People With Profound Cognitive Disabilities. Am. J. Occup. Ther. 2011, 65, 652–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-156504-2. [Google Scholar]
- Kenyon, L.K.; Hostnik, L.; McElroy, R.; Peterson, C.; Farris, J.P. Power Mobility Training Methods for Children: A Systematic Review. Pediatric Phys. Ther. 2018, 30, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Miller, W.C.; Mortenson, W.B.; Mihailidis, A. Feasibility RCT Protocol Evaluating a Powered-Wheelchair Training Program for Older Adults. Can. J. Occup. Ther. 2019, 86, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Mortenson, W.B.; Mihailidis, A.; Miller, W.C. Understanding the Task Demands for Powered Wheelchair Driving: A Think-Aloud Task Analysis. Disabil. Rehabil. Assist. Technol. 2020, 1–8. [Google Scholar] [CrossRef]
- Korkki, S.M.; Richter, F.R.; Jeyarathnarajah, P.; Simons, J.S. Healthy Ageing Reduces the Precision of Episodic Memory Retrieval. Psychol. Aging 2020, 35, 124–142. [Google Scholar] [CrossRef]
- Hoang, I.; Servant, V.; Schneider, M.; Bouteille, A.; Truche, A. Conduire Après Une Lésion Cérébrale Acquise Non Évolutive: Comment Se Ressaisir Des Recommandations HAS Pour Améliorer Les Pratiques Professionnelles et Conseiller Au Mieux Les Patients. In Sécurité Routière: Etat des Lieux et Initiatives Dans le Monde; Archives-Ouvertes: France, 2018; pp. 245–254. [Google Scholar]
- Nilsson, L. Powered Mobility for People with Profound Cognitive Disabilities Leads to Developing Occupational Performance. Br. J. Occup. Ther. 2019, 82, 655–657. [Google Scholar] [CrossRef]
- Campos, J.J.; Anderson, D.I.; Barbu-Roth, M.A.; Hubbard, E.M.; Hertenstein, M.J.; Witherington, D. Travel Broadens the Mind. Infancy 2000, 1, 149–219. [Google Scholar] [CrossRef] [PubMed]
- Toglia, J.P. The Dynamic Interactional Model and the Multicontext Approach. Cognition, Occupation, and Participation across the Lifespan: Neuroscience, Neurorehabilitation, and Models of Intervention in Occupational Therapy; Katz, N., Toglia, J., Eds.; AOTA Press: New York, NY, USA, 2018; ISBN 978-1-56900-479-1. [Google Scholar]
- Chanquoy, L.; Tricot, A.; Sweller, J. La Charge Cognitive: Théorie et Applications; Armand Colin: Paris, France, 2007; ISBN 978-2-200-34724-6. [Google Scholar]
- Raffard, S.; Gely-Nargeot, M.-C.; Capdevielle, D.; Bayard, S.; Boulenger, J.-P. Potentiel d’apprentissage et revalidation cognitive dans la schizophrénie. L’Encéphale 2009, 35, 353–360. [Google Scholar] [CrossRef]
- Heaton, R.K.; Marcotte, T.D.; Mindt, M.R.; Sadek, J.; Moore, D.J.; Bentley, H.; Mccutchan, J.A.; Reicks, C.; Grant, I.; HNRC Group. The Impact of HIV-Associated Neuropsychological Impairment on Everyday Functioning. J. Inter. Neuropsych. Soc. 2004, 10, 317–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellichero, A.; Best, K.L.; Routhier, F.; Viswanathan, P.; Wang, R.H.; Miller, W.C. Blind Spot Sensor Systems for Power Wheelchairs: Obstacle Detection Accuracy, Cognitive Task Load, and Perceived Usefulness among Older Adults. Disabil. Rehabil. Assist. Technol. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.C. Smart Wheelchairs: A Literature Review. J. Rehabil. Res. Dev. 2005, 42, 423. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1st Author, Publication Date | Time of Assessments | Sample Sample Size, Mean Age, (Range), Diagnosis | Intervention | Outcome Measurement (Items) | Results | Level of Evidence MMAT Score |
|---|---|---|---|---|---|---|
| Randomized Controlled Trials (n = 2) | ||||||
| Jones et al., 2012 | Baseline, Post PMD provision and training (12 months) | n = 28 IG, n = 14 21 months (14–30 months) CG, n = 14 22 months (14–30 months) cerebral palsy, diverse myopathy, arthrogryposis, progeria, tetraphocomelia, failure to thrive, myotonic dystrophy, hydrocephalus, Dandy Walker syndrome, Achondroplastic dwarfism | IG
| cognition (a) PEDI (cognitive) (b) Battelle Developmental Inventory (b1) communication (b2) cognitive PMD capacity (a) PEDI (mobility) | cognition (a) p = 0.38 (b) (b1) communication p = 0.42 (b2) cognitive p = 0.38 PMD capacity (a) p = 0.02 * | II 5/5 |
| Mountain et al., 2014 | Baseline, Post training | n = 17 IG, n = 9 58.7 years (n.r.) CG, n = 8 49.0 years (n.r.) stroke | IG
| cognition (baseline) (a) MoCA, (b) Behavioural Inattention Test, (c) Praxis PMD capacity (a) WST (baseline and follow up) | cognition (baseline) (a) p = 0.027 * (b) p = 0.533 (c) p = 0.619 PMD capacity (a) baseline p = 0.924 follow-up p = 0.006 * | II 4/5 |
| Pre-Post Studies (n = 3) | ||||||
| Bottos et al., 2001 | Baseline, Post PMD provision | n = 29 6.3 years (3–8) tetraplegia | Provision of a PMD (6 to 8 months) | cognition (a) IQ (performance) (b) IQ (verbal) capacity (a) Powered mobility program evaluation | cognition (a) no significant change (b) no significant change capacity (a) p < 0.01 * | III 4/5 |
| Cullen et al., 2008 | Pre-post study | n = 81 65.6 (29–96) diverse diagnosis (e.g., arthritis, multiple sclerosis, stroke, Parkinson disease…) | 1-month PMD provision | cognition (a) IQ (b) Addenbrooke’s Cognitive Examination-R (naming and comprehension) (c) RBANS (verbal memory, visual memory, visual perception) (d) F-A-S Test (e) Behavioural Inattention Test (line bisection) (f) BADS (key search subtest) (g) Depression Anxiety Stress Scale-21 (h) Visual Object and Space perception Battery (screening test, position discrimination, cube analysis) (i) Road Map Test of Direction Sense test PMD capacity (a) self-rated power wheelchair use questionnaire: (level of functional powerchair use (less frequent = use < 3 days per week and <2 activities; for outdoor use < 2 outdoor activities) PMD performance (a) Functional Evaluation in a Wheelchair | cognition/capacity More frequent indoor power wheelchair use was predicted by better score on: - index of overall impairment (zβ = −0.495, p = 0.021 *) - verbal memory (zβ = 0.614, p < 0.001 *), More frequent outdoor power wheelchair use was predicted by betterscore on delayed story recall (zβ = 0.610, p = 0.001 *) PMD performance (a) median score = 89% | |
| Furumasu et al., 2004 | Pre-post study | n = 50 n.r. (21 months—6 years 11 months) n = 26 triplegic or tetraplegic cerebral palsy, n = 24 orthopedic or neuromuscular disabilities | Powered mobility program: motivational play and exploration six sessions 1 h 1 month period | cognition (a) PPWST (problem solving, spatial relations) (b) Symbolic Representation Scale PMD capacity (a) Powered mobility program evaluation | cognition/capacity (a) both factors in the PPWST (problem-solving and spatial relations) were significant: 82.4% of the variance for basic driving skills; 74.1% of the variance for overall driving skills. (b) Symbolic Representation Scale scores increased the predictive power to 87.1% for basic skills and 80.7% for overall mobility. | |
| Mountain et al., 2010 | Baseline, Post training | n = 10 67.1 years (41–87) stroke neglect group n = 6 non-neglect group n = 4 the Sunny Brook Neglect Battery was used to determine neglect and non-neglect group | Neglect group
| cognition (baseline only) (a) Neurobehavioral Cognitive Status Examination (b) Sunny Brook Neglect Battery (c) Visual Scanning Tests (d) 22 clock drawing PMD capacity (a) WST | cognition (baseline only) (a) M = 86.9% (SD 11.6) (b) M = 14.5 (SD 20.3) (c) M = 43.8% (SD 42.7) (d) M = 12.6 (SD 2.2) PMD capacity (a) overall group: p = 0.002 * neglect group: p = 0.740 non-neglect group: data not shown no significant difference in the extend of improvement between the neglect and non-neglect group (p = 0.749) | III 4/5 |
| Cross Sectional Study Design (n = 3) | ||||||
| Butler et al., 1984 | 1 data collection time | n = 13 31.3 months (20–37) paraplegia, cerebral palsy, arthrogryposis congenita, osteogenesis imperfecta, spinal muscular atrophy, four-extremity limb deficiency, hypotonic quadriplegia | PMD training:
| cognition (a) Development profile II PMD capacity (a) cumulative hours to learn the 7 skills (b) days to learn the 7 skills | cognition (a) 12 children scored in the normal range 1 had higher level of intellectual functioning PMD capacity (a) M = 34.4 cumulative hours (b) M= 16.3 days | III 2/5 |
| Massengale et al., 2005 | Cross-sectional | n = 62 40.4 years (18–72) diverse diagnosis (e.g., spinal cord injury, cerebral palsy, post-polio syndrome, stroke, traumatic brain injury…) | n.a. | cognition (a) MVPT-R (b) TONI-3rd (c) WAIS-R (comprehension/picture completion/digit span) PMD capacity (a) Power Mobility Road Test (performance score and time to complete) (b) Power Wheelchair Screening Form | correlations between cognition and PMRT performance score (a) r = 0.591, p = 0.000 * (b) r = 0.392, p = 0.003 * (c) comprehension: r = 0.297, p = 0.026 */picturcompletion r = 0.418, p = 0.001 */digit span: r = 0.315, p = 0.018 * correlations between cognition and time required to complete the PMRT (a) r = −0.707, p = 0.000 * (b) r = −0.324, p = 0.012 * (c) comprehension: r = −0.306, p = 0.019 */picture completion r = −0.418, p = 0.001 */digit span: r = −0.258, p = 0.048 * | |
| Tefft et al., 1998 | Cross-sectional | n = 26 n.r 20–36 months diverse diagnosis (e.g., arthrogryposis, congenital myopathy, quadriplegia, polio syndrome, spina bifida…) | Wheelchair mobility training program 6 sessions of 1 h | Cognition (a) PPWST (object permanence, problem solving, spatial relations) Capacity and performance (a) Powered mobility program evaluation | Cognition/capacity/performance spatial relations and problem solving were significant and accounted for 57% of the variance in Powered mobility program evaluation scores (R2 = 0.57, F = 14.37, p < 0.0001 *) | |
| Single Subject Research Design (n = 2) | ||||||
| Dawson et al., 2003 | A baseline B intervention A baseline B post | n = 2 p1: 67 years old p2: 70 years old stroke, unilateral neglect | PMD training:
| cognition (a) Behavioural Inattention Test (b) Star cancellation test (c) Baking tray task PMD capacity (a) number of left collisions recorded (b) time taken negotiating an obstacle | cognition Participant 1: (a) continued to demonstrate unilateral neglect (b) performed within the normal limit, no significant change comparing the 3 phases (c) trend for rightward spatial bias to normal limit, significant change between phase A1 and B1 p = 0.005 * Participant 2: (a) continued to demonstrate unilateral neglect (b) performed consistently below the normal limits, minimal significant change between phase A2 and B2 p = 0.043 * (c) rightward spatial bias was consistently seen PMD capacity Participant 1: (a) significant reduction in the left collisions p = 0.04 * (b) significant reduction in the time taken to complete the obstacle course p = 0.003 * Participant 2: (a) significant reduction in the left collisions p < 0.0001 * (b) significant reduction in the time taken to complete the obstacle course p = 0.0015 * | IV 3/5 |
| Kenyon et al., 2018 | A baseline B intervention A baseline B intervention 6 weeks follow-up | n = 1 3 years 2 months spastic quadriplegic, cerebral palsy, cortical visual impairment micro cephalic seizure disorder | Individualized PMD training:
| cognition (a) Dimension of Mastery Questionnaire (b) PEDI-CAT (cognitive) PMD capacity (a) Wheelchair Skills Checklist (b) Assessment of Learning Power mobility (c) PEDI-CAT (mobility) | cognition (a) baseline 1: 3.36 (0.32) intervention 1: 3.84 (0.23) baseline 2: 3.84 (0.23) intervention 2: 3.58 (0.17) (b) intervention 1: 51 (1.59) intervention 2: 50 (1.75) follow-up: 51 (1.52) PMD capacity (a) intervention 1: 1/7 skills intervention 2: 5/7 skills follow-up: 5/7 skills (b) intervention 1: phase 2 (curious novice) intervention 2: phase 4 (advanced beginner follow-up: phase 5 (sophisticated beginner) (c) intervention 1: 38 (4.41) intervention 2: 47 (1.65) * follow-up: 49 (1.43) * * Standard error measure exceeded in the mobility domain | IV 4/5 |
| Case(s) Report (n = 5) | ||||||
| Benford et al., 2017 | 7 data collection time | n = 1 23 years old male spastic quadriplegic epilepsy profound and multiple learning disabilities | Driving to learn develop understanding of cause effect 23 weeks 31 sessions (during 30 to 45 min) | cognition (a) qualitative data (mood and fatigue) PMD capacity (a) Assessment of Learning Power mobility (a1) attention related to PMD use (a2) understanding related to PMD use (a3) expression emotions related to PMD use (a4) activity and movement | cognition (a) “fatigue impacted performance” “his mood generally improve over the period that he participated in sessions” PMD capacity (a1) pre: 3/post: 5 (a2) pre: 3/post: 5 (a3) pre: 3/post: 5 (a4) pre: 3/post: 5 | IV 2/5 |
| Jones et al., 2003 | pretest 1 (beginning) pretest 2 (3 months) postest (6 months) | 20 months old type II spinal muscular atrophy | intervention based on motor learning principles 6 weeks | cognition (a) PEDI (cognitive) (b) Battelle Developmental Inventory (b1) adaptive (b2) communication (b3) cognitive PMD capacity (a) PEDI (mobility) | cognition (a) positive trend (b) (b1) normal development (b2) positive trend (b3) age-equivalent scores increased greater than the period PMD capacity (a) positive trend | IV 4/5 |
| Kenyon et al., 2015 | pre post | n = 1 18 years old spastic quadriplegic cerebral palsy cortical visual impairment | PMD training
| cognition (a) Power mobility screen (cognition: judgement and abstraction) PMD capacity (b) Power mobility screen (motor scale) | cognition (a) pre: 9/21 post: 19/21 PMD capacity (b) pre: 16/30 post: 24/30 | IV 4/5 |
| Kenyon et al., 2017 | case series baseline post | n = 3 n.a. P1:1 year 5 months P2: 2 years 5 months P3: 3 years 5 months cerebral palsy | PMD training:
| cognition (a) PEDI-CAT (cognitive) (b) Dimension of Mastery Questionnaire (cognitive persistence) PMD capacity (a) PEDI-CAT (mobility) (b) Assessment of Learning Power mobility | cognition scales score (SE) (a) P1: pre: 40(3.3)/post: 46(2.3) * P2: pre: 477(2.0)/post: 50(1.8) * P3: pre: 58(1.1)/post: 59(1.1) * (b) P1: stable pre-post (bellow the norm) P2: increase pre-post (bellow the norm) P3: stable pre-post (bellow the norm) PMD capacity (a) P1: pre: 41(3.7)/post: 43(3.2) P2: pre: 34(5.6)/post: 46(3.3) * P3: pre: 41(3.8)/post: 49(2.8) * (b) P1: pre: novice/post: advanced beginner P2: pre: novice/post: beginner P3:pre: level advanced-beginner/post: competent | IV 4/5 |
| Lynch et al., 2009 | case report | n = 1 7-month-old cerebral palsy | Infant-friendly training
| cognition (a) Balley III (a1) cognition (a2) language reception (a3) language expression PMD mobility: (a) joystick activations (b) path length (meters) (c) total path length (meters) (d) percent directed driving success | cognition (a) (a1) pre:7/post:49 (a2) pre:11/post: 16 (a3) pre: 9/post: 14 PMD mobility: (a) positive trend and stable (b) small positive trend (c) positive trend (d) 0 during the first training month/then positive trend | |
| Nilsson et al., 2003 | case report baseline and 12 months follow-up | n = 2 n.a. P1: 5 years old P2: 4 years old profound cognitive disabilities, visual and motor impairment | intensive PMD training:
After 4 months the training was transferred to the children’s homes. | video-recordings: facial expressions, body movement, vocalizations, and reaction to interaction field notes: new and special reaction to behaviors in-depth interviews: how parents and assistants experienced the training and the children’s changing behaviors over time | P1: 1st session: “moving in circles”; “unable to place her hand on the joystick unaided”; “did not display any intention of doing so” follow-up: “after a great effort and with obvious intention, she was able to carry out self-initiated driving” P2: 1st session: “hand-over-hand driving”; “no sign of understanding that he could initiate the driving” follow-up: “able to keep the joystick in driving position”; “fluctuated between guided driving, unintentional driving, and driving after release of guidance”, “occasionally he managed to perform self-initiated driving” | |
| Outcome Measures’ Name | Used In | Outcome Measure Brief Description | Specific Cognitive Function, Evaluated in Included Study, Classified According to the ICF |
|---|---|---|---|
| Addenbrooke’s Cognitive Examination (ACE-R) [34] | Cullen et al., (2008) |
| reception of spoken language (d16700), expression of spoken language (d16710) |
| Behavioural Assessment of the Dysexecutive Syndrome (key search subtest) (BADS) [35] | Cullen et al., (2008) |
| problem solving (b1646) |
| Behavioural Inattention Test [36] | Cullen et al., (2008) |
| visuospatial perception (b1565) |
| Depression Anxiety Stress Scale-21 (DASS-21) [37] | Cullen et al., (2008) |
| psychic stability (b1263) |
| F-A-S test [38] | Cullen et al., (2008) |
| expression of spoken language (d16710) |
| Motor Free Visual Perception Test-Revises (MVPT-R) [39] | Massengale et al., (2005) |
| visuospatial perception (b1565) |
| Pediatric Powered Wheelchair Screening Test (PPWST) [26] | Furumasu et al., (2004) and Tefft et al., (1999) |
| visuospatial perception (b1565), organization and planning (b1641) problem solving (b1646) |
| Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) [40] | Cullen et al., (2008) |
| short term memory (b1440), long term memory (b1441), attention functions (b140), visuospatial perception (b1565), mental function of language (b167) |
| Road Map Test of Direction Sense test [41] | Cullen et al., (2008) |
| cognitive function orientation to place (b1141), cognitive flexibility (b1643) |
| Symbolic Representation Scale [20] | Furumasu et al., (2004) |
| integrative language functions (b1672) |
| Test Of Nonverbal Intelligence—3rd edition (TONI-3rd) (Brown et al., 1996) | Massengale et al., (2005) |
| abstraction (b1640), problem solving (b1646), intellectual function (b117) |
| Visual Object and Space perception Battery (VOSP) (Lezak et al., 2004) | Cullen et al., (2008) |
| visuospatial perception (b1565) |
| Wechsler Adults Intelligence Scale—Revised (WAIS-R) (Matarazzo, 1996) | Massengale et al., (2005) |
| sustaining attention (b1400), short term memory (b1440), judgement (b1645) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellichero, A.; Kenyon, L.K.; Best, K.L.; Lamontagne, M.-E.; Lavoie, M.D.; Sorita, É.; Routhier, F. Relationships between Cognitive Functioning and Powered Mobility Device Use: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 12467. https://doi.org/10.3390/ijerph182312467
Pellichero A, Kenyon LK, Best KL, Lamontagne M-E, Lavoie MD, Sorita É, Routhier F. Relationships between Cognitive Functioning and Powered Mobility Device Use: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(23):12467. https://doi.org/10.3390/ijerph182312467
Chicago/Turabian StylePellichero, Alice, Lisa K. Kenyon, Krista L. Best, Marie-Eve Lamontagne, Marie Denise Lavoie, Éric Sorita, and François Routhier. 2021. "Relationships between Cognitive Functioning and Powered Mobility Device Use: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 23: 12467. https://doi.org/10.3390/ijerph182312467