
Impact of the COVID-19 Pandemic on Adolescents’ Sexual and Reproductive Health in Low- and Middle-Income Countries

 , , ,
, , ,  , , ,
, , , 
Abstract
:1. Introduction
- What is known from the literature about the impact of COVID-19 on SRH of adolescents in LMICs?
- What interventions have been designed and implemented to promote SRH and access to SRH services for adolescents in LMICs during the COVID-19 pandemic?
- How can future studies overcome research gaps and inform programs and policies that meet the SRH care needs of adolescents in the context of the pandemic?
2. Methods
2.1. Data Sources and Search Strategy
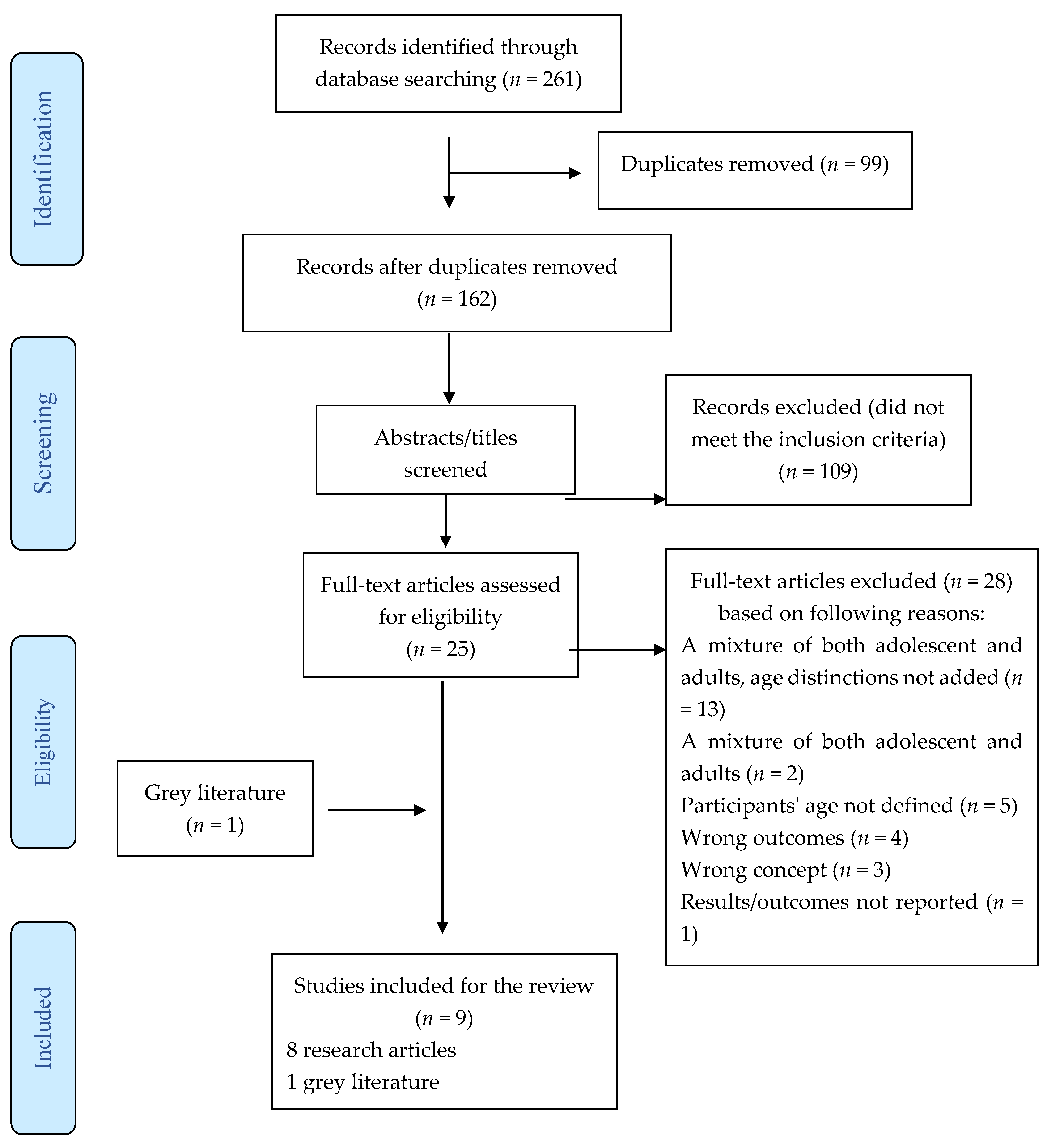
2.2. Study Selection
2.3. Data Extraction
3. Results
3.1. Limited Access to Sexual and Reproductive Health Services during COVID-19
3.2. School Closure and Increased Rates of Early Marriages
3.3. Sexual or Intimate Partner Violence during COVID-19
3.4. Disruption in Maternity Care
3.5. Adolescents’ Involvement in Risky or Exploitative Work
3.6. Interventions to Improve Sexual and Reproductive Health Services during COVID-19
3.7. Policy Development Related to Adolescent Sexual and Reproductive Health
4. Discussion
4.1. Low Socioeconomic Status and Early or Unwanted Pregnancies
4.2. Impact of Pandemic on Affordability and Accessibility of Menstrual Products
4.3. Domestic/Intimate Partner Violence during the Pandemic
4.4. Limited In-Person Services Experience
4.5. Role of School in Promoting SRH
4.6. Preparedness for Future Crises
4.7. Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bauer, A.; Garman, E.; McDaid, D.; Avendano, M.; Hessel, P.; Díaz, Y.; Araya, R.; Lund, C.; Malvasi, P.; Matijasevich, A.; et al. Integrating youth mental health into cash transfer programmes in response to the COVID-19 crisis in low-income and middle-income countries. Lancet Psychiatry 2021, 8, 340–346. [Google Scholar] [CrossRef]
- Riley, T.; Sully, E.; Ahmed, Z.; Biddlecom, A. Estimates of the Potential Impact of the COVID-19 Pandemic on Sexual and Reproductive Health in Low- and Middle-Income Countries. Int. Perspect. Sex. Reprod. Health 2020, 46, 73–76. [Google Scholar] [CrossRef]
- World Bank. Classifying Countries by Income. Available online: https://datatopics.worldbank.org/world-development-indicators/stories/the-classification-of-countries-by-income.html (accessed on 19 November 2021).
- Desrosiers, A.; Betancourt, T.; Kergoat, Y.; Servilli, C.; Say, L.; Kobeissi, L. A systematic review of sexual and reproductive health interventions for young people in humanitarian and lower-and-middle-income country settings. BMC Public Health 2020, 20, 666. [Google Scholar] [CrossRef]
- Nanda, P.; Tandon, S.; Khanna, A. Virtual and essential-adolescent SRHR in the time of COVID-19. Sex. Reprod. Health Matters 2020, 28, 81–84. [Google Scholar] [CrossRef]
- Lindberg, L.D.; Bell, D.L.; Kantor, L.M. The sexual and reproductive health of adolescents and young adults during the COVID-19 pandemic. Perspect. Sex. Reprod. Health 2020, 52, 75–79. [Google Scholar] [CrossRef]
- Ahmed, Z.; Guttmacher Institute. Covid-19 Could Have Devastating Effects on Adolescents’ Sexual and reproductive Health and Rights. Available online: https://www.guttmacher.org/print/article/2020/06/covid-19-could-have-devastating-effects-adolescents-sexual-and-reproductive-health (accessed on 20 February 2021).
- Partnership for Maternal, Newborn & Child Health. Sexual and Reproductive Health and Rights during COVID-19. Available online: https://www.who.int/pmnch/covid-19/toolkits/adolescent/srhr/en/ (accessed on 20 February 2021).
- United Nations Funds for Population Activities. Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-based Violence, Female Genital Mutilation and Child Marriage. Available online: https://www.unfpa.org/sites/default/files/resource-pdf/COVID-19_impact_brief_for_UNFPA_24_April_2020_1.pdf (accessed on 20 February 2021).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. “PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation”. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melbourne, V.H.I. Covidence Systematic Review Software. Available online: www.covidence.org (accessed on 5 February 2021).
- Banati, P.; Jones, N.; Youssef, S. Intersecting vulnerabilities: The impacts of COVID-19 on the psycho-emotional lives of young people in low- and middle-income countries. Eur. J. Dev. Res. 2020, 32, 1613–1638. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.; Wilson, K.; Badia, J.; Agot, K.; Neary, J.; Njuguna, I.; Kibugi, J.; Healy, E.; Beima-Sofie, K.; John-Stewart, G.; et al. The psychosocial effects of the COVID-19 pandemic on youth living with HIV in western Kenya. AIDS Behav. 2021, 25, 68–72. [Google Scholar] [CrossRef]
- Eboi, A.A.; Awan Ismail, N.A.H. New Media Strategies’ Model for Sexual Reproductive Health & Rights Campaigns among Young People in Informal Settlements: Mitigating the Challenges. Eur. J. Mol. Clin. Med. 2020, 7, 1455–1473. [Google Scholar]
- Muhaidat, N.; Fram, K.; Thekrallah, F.; Qatawneh, A.; Al-Btoush, A.A. Pregnancy during COVID-19 outbreak: The impact of lockdown in a middle-income country on antenatal healthcare and wellbeing. Int. J. Women’s Health 2020, 12, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Bellerose, M.; Diaw, M.; Pinchoff, J.; Kangwana, B.; Austrian, K. Pre-pandemic influences on Kenyan girls’ transitions to adulthood during COVID-19. Girlhood Stud. 2020, 13, 133–150. [Google Scholar] [CrossRef]
- Siedner, M.J.; Kraemer, J.D.; Meyer, M.J.; Harling, G.; Mngomezulu, T.; Gabela, P.; Dlamini, S.; Gareta, D.; Majozi, N.; Ngwenya, N.; et al. Access to primary healthcare during lockdown measures for COVID-19 in rural South Africa: An interrupted time series analysis. BMJ Open 2020, 10, e043763. [Google Scholar] [CrossRef]
- Herran, K.; Palacios, I. Evaluating and improving upon Ecuador’s adolescent pregnancy prevention policies in an Era of increased urgency. Ann. Glob. Health 2020, 86, 1–3. [Google Scholar] [CrossRef]
- Dourado, I.; Magno, L.; Soares, F.; Massa, P.; Nunn, A.; Dalal, S.; Grangeiro, A. Adapting to the COVID-19 pandemic: Continuing HIV prevention services for adolescents through telemonitoring, Brazil. AIDS Behav. 2020, 24, 1994–1999. [Google Scholar] [CrossRef]
- United Nations Population Funds. Not on Pause: Responding to the Sexual and Reproductive Health Needs of Adolescents in the Context of the Covid-19 Crisis. Available online: https://www.unfpa.org/sites/default/files/resource-pdf/Not_on_Pause.pdf (accessed on 25 March 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 19, 1–12. [Google Scholar]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.W.; Haines, J. The impact of COVID-19 on health behavior, stress, financial and food security among middle to high income Canadian families with young children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef]
- Morgan, A.; Boxall, H. Social isolation, time spent at home, financial stress and domestic violence during the COVID-19 pandemic. Trends Issues Crime Crim. Justice 2020, 609, 1–18. [Google Scholar]
- Thayer, Z.M.; Gildner, T.E. COVID-19-related financial stress associated with higher likelihood of depression among pregnant women living in the United States. Am. J. Hum. Biol. 2021, 33, e23508. [Google Scholar] [CrossRef]
- Nalwadda, G.; Mirembe, F.; Byamugisha, J.; Faxelid, E. Persistent high fertility in Uganda: Young people recount obstacles and enabling factors to use of contraceptives. BMC Public Health 2010, 10, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, K.; Jewkes, R. Blood Blockages and Scolding Nurses: Barriers to Adolescent Contraceptive Use in South Africa. Reprod. Health Matters 2006, 14, 109–118. [Google Scholar] [CrossRef]
- Plan International. Periods in a Pandemic Menstrual Hygiene Management in the Time of COVID-19. Available online: https://plan-international.org/publications/periods-in-a-pandemic#:~:text=Periods%20don’t%20stop%20during,human%20rights%2C%20health%20and%20dignity (accessed on 20 June 2021).
- UNICEF. Mitigating the Impacts of COVID-19 and Menstrual Health and Hygiene. Available online: https://www.unicef.org/documents/mitigating-impacts-covid-19-menstrual-health-and-hygiene (accessed on 20 June 2021).
- Ebert, C.; Steinert, J.I. Prevalence and risk factors of violence against women and children during COVID-19, Germany. Bull. World Health Organ 2021, 99, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Munir, M.M.; Munir, M.H.; Rubaca, U. The Shadow Pandemic: Violence against Women in Pakistan during COVID-19 Lockdown. J. Int. Women’s Stud. 2021, 22, 229–248. Available online: https://vc.bridgew.edu/jiws/vol22/iss5/15 (accessed on 22 July 2021).
- Usher, K.; Bhullar, N.; Durkin, J.; Gyamfi, N.; Jackson, D. Family violence and COVID-19: Increased vulnerability and reduced options for support. Int. J. Ment. Health Nurs. 2020, 29, 549–552. [Google Scholar] [CrossRef] [Green Version]
- Perez-Vincent, S.M.; Carreras, M.; Gibbons, M.A.; Murphy, T.E.; Rossi, M.A. COVID-19 Lockdowns and Domestic Violence Evidence from Two Studies in Argentina. Inter-American Development Bank. 2020. Available online: https://publications.iadb.org/publications/english/document/COVID-19-Lockdowns-and-Domestic-Violence-Evidence-from-Two-Studies-in-Argentina.pdf (accessed on 22 July 2021).
- Mambo, S.B.; Sikakulya, F.K.; Ssebuufu, R.; Mulumba, Y.; Wasswa, H.; Thompson, K.; Rusatira, J.C.; Bhondoekhan, F.; Kamyuka, L.K.; Akib, S.O.; et al. Sexual and Reproductive Health and Rights Challenges among Ugandan Youth during COVID-19 Pandemic lockdown: An online Cross-Sectional Study. Res. Sq. 2020, 1–18. [Google Scholar] [CrossRef]
- Obasanjo, B.A. Factors associated with limited access to condoms and sources of condoms during the COVID-19 pandemic in South Africa. Arch. Public Health 2021, 79, 1–9. [Google Scholar]
- Antoci, A.; Sabatini, F.; Sodini, M. Online and offline social participation and social poverty traps. Can social networks save human relations? J. Math. Sociol. 2014, 39, 229–256. [Google Scholar] [CrossRef]
- Hall, J.A.; Kearney, M.W.; Xing, C. Two tests of social displacement through social media use. Inf. Commun. Soc. 2019, 22, 1396–1413. [Google Scholar] [CrossRef]
- Akinfaderin-Agarau, F.; Chirtau, M.; Ekponimo, S.; Power, S. Opportunities and limitations for using new media and mobile phones to expand access to sexual and reproductive health information and services for adolescent girls and young women in six Nigerian states. Afr. J. Reprod. Health 2012, 16, 219–230. [Google Scholar]
- Masruroh, S.; Wijaya, M.; Anantanyu, S. The Role of School Prevention Efforts in Early Marriage in the Ponjong District. Adv. Health Sci. Educ. Theory Pract. 2020, 34, 28–32. [Google Scholar]
- Mehra, D.; Sarkar, A.; Sreenath, P.; Behera, J.; Mehra, S. Effectiveness of a community-based intervention to delay early marriage, early pregnancy and improve school retention among adolescents in India. BMC Public Health 2018, 18, 732–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNICEF. 10 Million Additional Girls at Risk of Child Marriage Due to COVID-19. Available online: https://www.unicef.org/press-releases/10-million-additional-girls-risk-child-marriage-due-covid-19 (accessed on 23 June 2021).
- The World Bank. Educating Girls, Ending Child Marriage. Available online: https://www.worldbank.org/en/news/immersive-story/2017/08/22/educating-girls-ending-child-marriage (accessed on 23 June 2021).
- Chaabane, S.; Doraiswamy, S.; Chaabna, K.; Mamtani, R.; Cheema, S. The impact of COVID-19 school closure on child and adolescent health: A rapid systematic review. Children 2021, 8, 415. [Google Scholar] [CrossRef] [PubMed]
- Affoum, N.; Recavarren, I.S. Child Marriage: The Unspoken Consequence of COVID-19. World Bank Blogs. Available online: https://blogs.worldbank.org/developmenttalk/child-marriage-unspoken-consequence-covid-19 (accessed on 23 June 2021).
- Mmeje, O.O.; Coleman, J.S.; Chang, T. Unintended consequences of the COVID-19 pandemic on the sexual and reproductive health of youth. J Adolesc. Health 2020, 67, 326–327. [Google Scholar] [CrossRef] [PubMed]
- Hailemariam, S.; Gutema, L.; Agegnehu, W.; Derese, M. Challenges Faced by Female Out-of-School Adolescents in Accessing and Utilizing Sexual and Reproductive Health Service: A Qualitative Exploratory Study in Southwest, Ethiopia. J. Prim. Care Community Health 2021, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.C.; Bulu, S.; Harris, J.; Humphreys, D.; Malverus, J.; Gray, N.J. “These issues aren’t talked about at home”: A qualitative study of the sexual and reproductive health information preferences of adolescents in Vanuatu. BMC Public Health 2014, 14, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Laghi, F.; Liga, F.; Pompili, S. Adolescents who binge eat and drink: The role of emotion regulation. J. Addict. Dis. 2018, 37, 77–86. [Google Scholar] [CrossRef] [PubMed]
- McCoy, S.S.; Dimler, L.M.; Samuels, D.V.; Natsuaki, M.N. Adolescent susceptibility to deviant peer pressure: Does gender matter? Adolesc. Res. Rev. 2019, 4, 59–71. [Google Scholar] [CrossRef] [Green Version]
- Lunt, A.; Llewellyn, C.; Bayley, J.; Nadarzynski, T. Sexual healthcare professionals’ views on the rapid provision of remote services at the beginning of COVID-19 pandemic: A mixed-methods study. Int. J. STD AIDS 2021, 32, 1138–1148. [Google Scholar] [CrossRef]


{kind=link}
| Author/s and Year of Publication | Setting and Country | Aim of Study | Study Design | Target Population | Intervention | Outcomes of Study |
|---|---|---|---|---|---|---|
| [14] | Settings: Urban, rural, and refugee camps. Multinational: Ethiopia, Cote d’Ivoire, and Lebanon | To mitigate the psycho-emotional toll of the pandemic and promote resilience among adolescents in some of the most difficult places in the world to be a young person. | Qualitative studies | Adolescents Age: 10–19 n = 568 | No intervention |
|
| [15] | Settings: Urban Country: Kenya | To assess the psychosocial effects of COVID-19 within an ongoing cohort study of Adolescents Living with HIV. | Qualitative study | Adolescents and youth Age: 10–24 10–14 (n = 152), 15–19 (n = 188), 20–24 (n = 146) | No intervention |
|
| [16] | Country: Kenya | Three objectives: a. To document the likely challenges that can impede the implementation of a new media strategies model to disseminate SRHR messages to young people in media campaigns. b. To understand how media managers would mitigate the challenges that may interfere with using new media strategies model to disseminate SRHR messages in media campaigns to young people. c. To probe stakeholder perspectives on the possibility and acceptability of adapting a new media strategies model to pass SRHR messages to young people in media campaigns. | Qualitative study | Stakeholders (media managers, policymakers, healthcare professionals, teachers, parents, and youth) Age of youth = 15–24 Age of other participants = NR Total n = 54 | The use of new media platform for sex education. Example Twitter, Facebook, WhatsApp. NGO created platforms for the youth. |
|
| [17] | Country: Jordan | To evaluate the impact of the lockdown circumstances in Jordan on antenatal care services and health circumstances of pregnant women during this period. | Qualitative study (cross-sectional study) | Pregnant women (15 years and above) Total n = 944 15–19 years (n = 4) 20–24 years (n = 146) 25 years and above (n = 794) | No intervention |
|
| [18] | Settings: Urban and rural Country: Kenya | To explore the pre-pandemic characteristics that may either protect girls from negative outcomes during the pandemic response or put them at higher risk. | Quantitative study | Adolescent girls Age: 10–14 years (n = 206) Age: 15–19 (n = 650) | No intervention |
|
| [19] | Setting: Health center (urban) Country: South Africa | To assess the impact of the lockdown orders in response to the COVID-19 epidemic in South Africa on access to basic healthcare services. | Quantitative: Interrupted time series analysis | Adolescents 6–19 years of age (n = 4460) 20–45 years accounted for 48% (n = 22 231) | No intervention |
|
| [20] | Country: Ecuador | To evaluate and learn from prior health policy in strategizing more effective adolescent pregnancy prevention legislation. | Descriptive paper (Policy analysis/discussion | Adolescents Age: 15–19 years n = NR | No intervention |
|
| [21] | Setting: UrbanCountry: Brazil | To describe the strategies adopted by PrEP1519 sites of Salvador and São Paulo to continue to provide HIV and SRH services during quarantine periods to contain the COVID-19 pandemic. | Follow-up program | Adolescent men sleeping with men (MSM) and transgender women (TGW) Age: 15–19. n = 484 |
|
|
| [22] | Global | To continue responding to the sexual and reproductive health needs of adolescents in the context of the COVID-19 crisis. | Technical brief (grey literature) | Adolescents 10–19 years n = NR |
| Policy implementation for:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meherali, S.; Adewale, B.; Ali, S.; Kennedy, M.; Salami, B.; Richter, S.; Okeke-Ihejirika, P.E.; Ali, P.; da Silva, K.L.; Adjorlolo, S.; et al. Impact of the COVID-19 Pandemic on Adolescents’ Sexual and Reproductive Health in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2021, 18, 13221. https://doi.org/10.3390/ijerph182413221
Meherali S, Adewale B, Ali S, Kennedy M, Salami B, Richter S, Okeke-Ihejirika PE, Ali P, da Silva KL, Adjorlolo S, et al. Impact of the COVID-19 Pandemic on Adolescents’ Sexual and Reproductive Health in Low- and Middle-Income Countries. International Journal of Environmental Research and Public Health. 2021; 18(24):13221. https://doi.org/10.3390/ijerph182413221
Chicago/Turabian StyleMeherali, Salima, Bisi Adewale, Sonam Ali, Megan Kennedy, Bukola (Oladunni) Salami, Solina Richter, Phil E. Okeke-Ihejirika, Parveen Ali, Kênia Lara da Silva, Samuel Adjorlolo, and et al. 2021. "Impact of the COVID-19 Pandemic on Adolescents’ Sexual and Reproductive Health in Low- and Middle-Income Countries" International Journal of Environmental Research and Public Health 18, no. 24: 13221. https://doi.org/10.3390/ijerph182413221