
Fear, Efficacy, and Environmental Health Risk Reporting: Complex Responses to Water Quality Test Results in Low-Income Communities

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
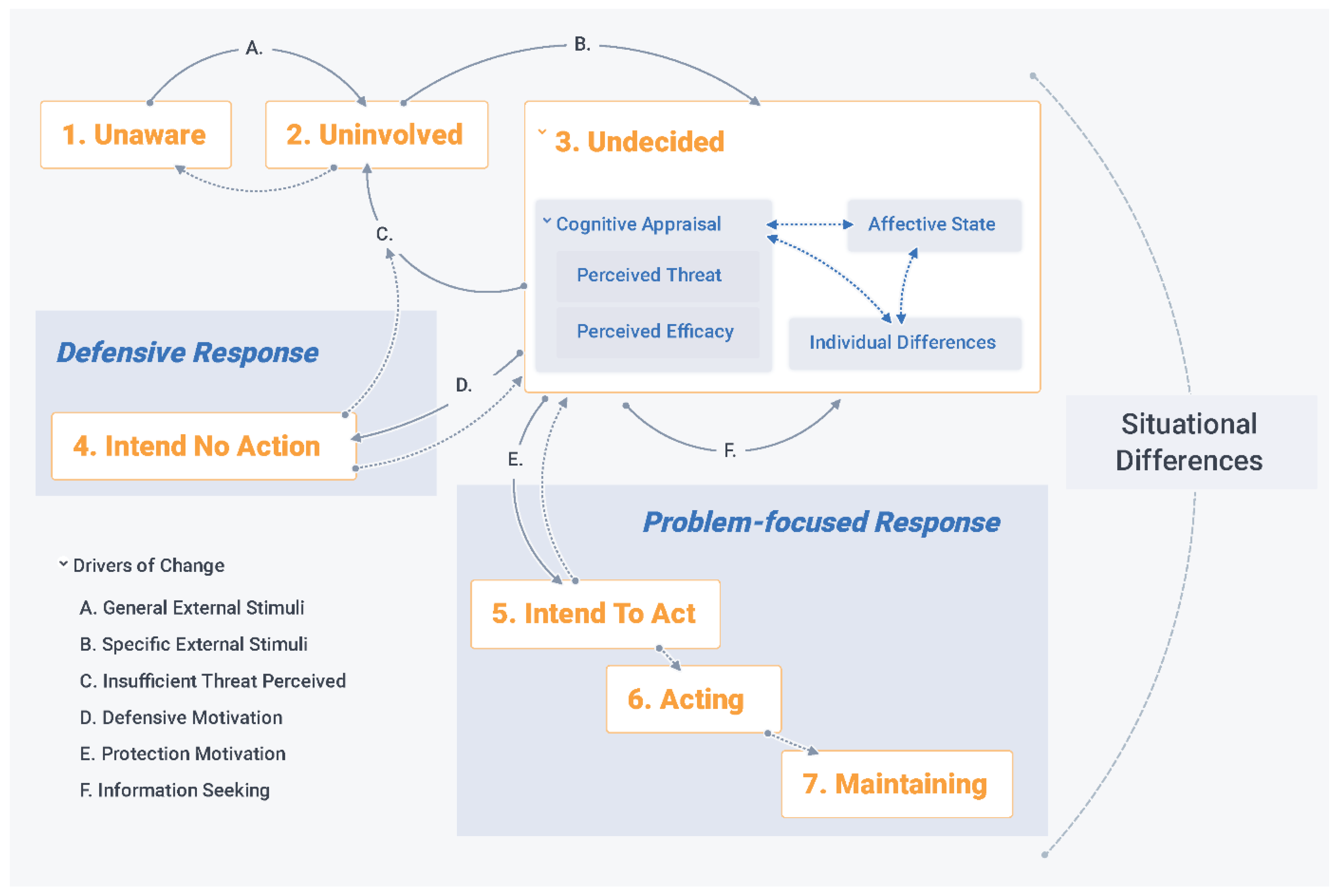
2.1. An Integrated Fear Appeal Framework
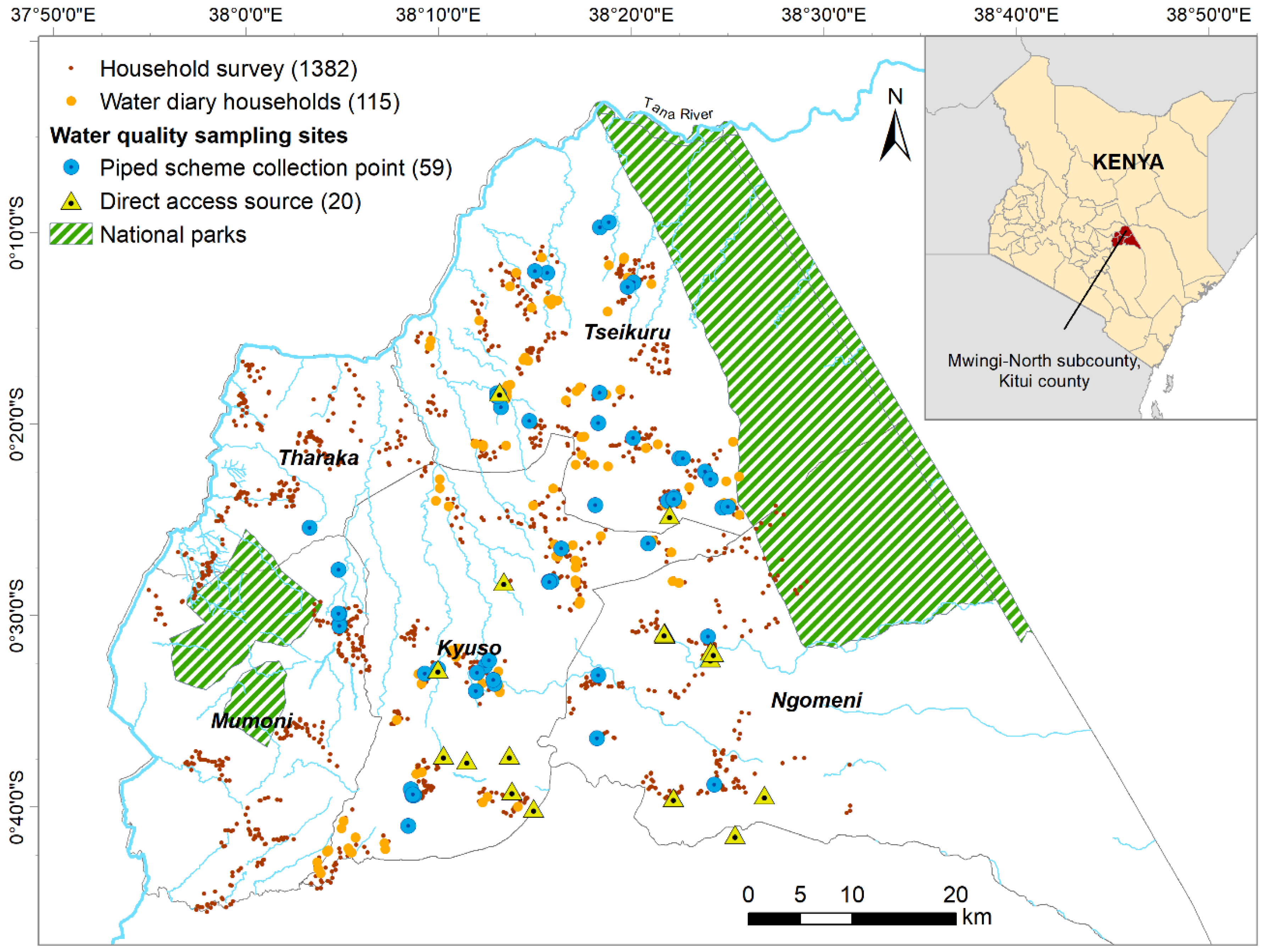
2.2. Study Area
2.3. Mixed-Methods Data Collection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Instrument | Dates | Sample | Description | Execution |
|---|---|---|---|---|
| (1) Cross-sectional household survey | 9–20 March 2018 | A total of 1457 households: 71% household heads, 22% spouses, 6% other relatives. 60% were between 30 and 59 years old and 44% presented as female. | A survey on indicators of multidimensional poverty, including domestic water services, with a subsection on perceptions and decision-making around drinking-water safety. The questionnaire, further method information, and data are available via the UK Data Service ReShare public repository (10.5255/UKDA-SN-854561). | 17 enumerators were locally recruited and trained on data collection, ethics, and code of conduct. Tablets and the Open Data Kit and Enketto mobile survey platforms were used. Quality control checks were executed daily with continuous feedback to enumerators. The final data were checked for consistency and coherence, with incomplete forms excluded. |
| (2) Longitudinal household survey (daily water diaries and bimonthly check-in survey) | August 2018–July 2019 | One hundred fifteen households: completed 5826 diary weeks and 1241 check-in surveys (min 4, max 19, mean 11 surveys each). A total of 78% of participants presented as female and mean age was 45 (SD = 15 years). | Daily diary forms and twice-monthly surveys to capture participants water collection practices. Details of the forms and their development are already published [71]. The twice-monthly surveys asked about perceived changes in water quality, HHWT practices, and illnesses (see questionnaire in Supplementary File S1). | Three enumerators conducted the check-in surveys and collected and digitized the diary forms using tablets and the Ona Systems survey platform. Participants did a pilot week to practice. Data were reviewed bi-monthly by 2 of the authors. Follow-up visits with participants to seek explanations for unusual data were conducted by the enumerators as needed. Mid-week check-in phone calls were implemented to counteract disinterest. |
| (3) Household-level semi-structured interviews and participant observation | July–November 2018 | Thirty-five water users: primary fetchers of water (13), and/or primary managers of water within the home (17), and/or household heads (19). A total of 18 presented as female, 6 were single parenting, 5 were physically disabled, and 4 were >60 years old. | Qualitative depth sourced from 35 semi-structured in-depth interviews and 21 participant observation daily journals, exploring the diversity of water perceptions and practices within communities, including which factors influence supply-selection. Further information about the ethnographic approach used for this work is published in [72]. | Two of the co-authors (female University of Nairobi graduate students) lived in the communities to build rapport and interact with community members at homesteads, water supplies, market areas, and during special functions. The fieldwork began with establishing support from community leaders, familiarizing with the location, and conducting informal scoping conversations and observations to adjust the interview guides. Interviews were conducted in Kiswahili and Kikamba, and translated and transcribed in English. |
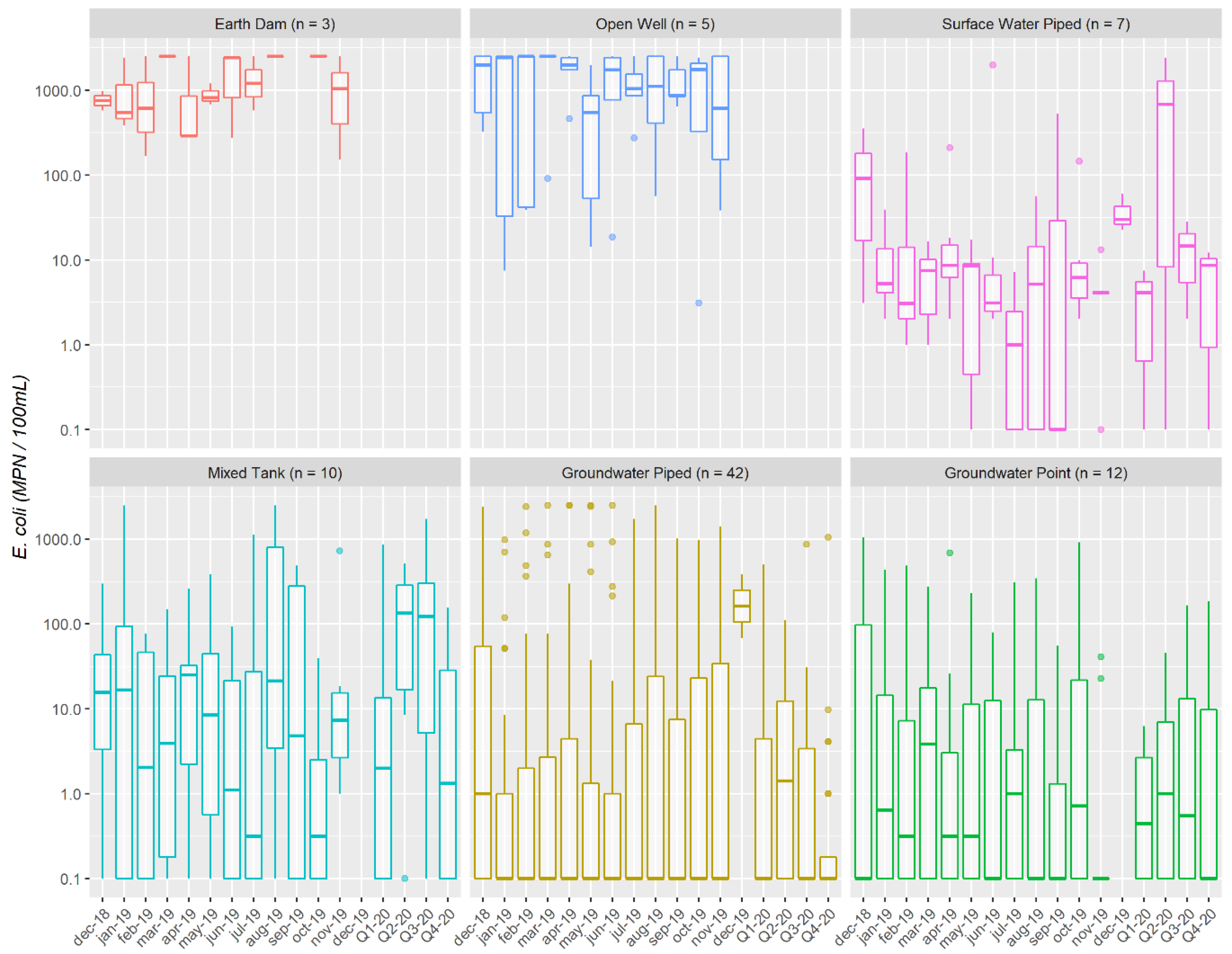
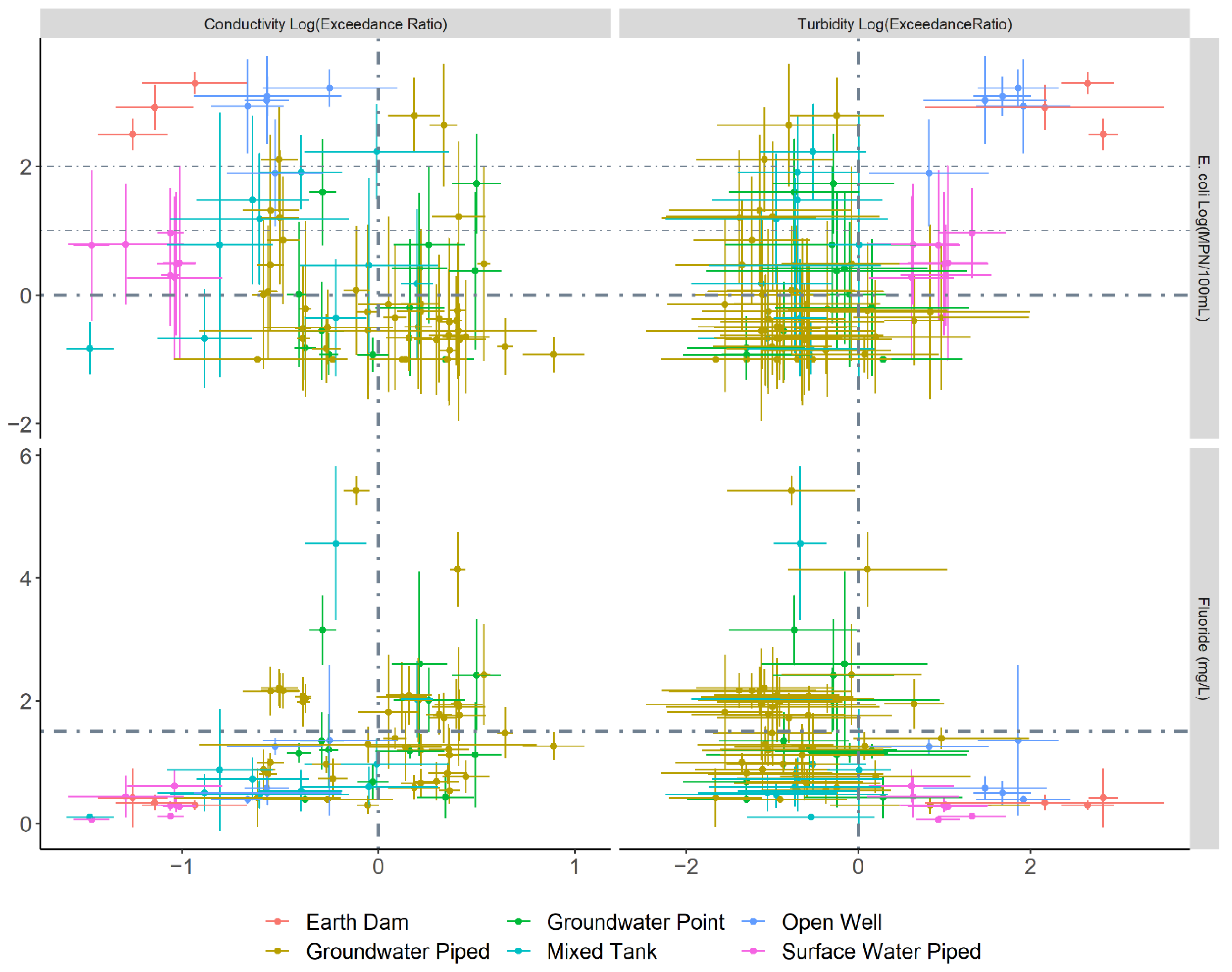
| (4) Water quality monitoring programme | December 2018 –2020 | Seventy-nine water points: 12 handpumps, 52 piped groundwater taps from 25 schemes (including 10 mixed tanks with rainwater collection), 3 earth dams, 5 open wells, and 7 piped surface water taps from 4 schemes. | Monthly sampling and analysis of chemical (pH, conductivity, turbidity, fluoride) and microbial (Escherichia coli and total coliforms) water quality in 2019. Parameters were selected following Kitui water supply project document review and meetings with the County government to identify key contaminants of concern for the area. In 2020, we continued quarterly sampling for 45 of the sites (those which were registered for maintenance services). | Two of the co-authors conducted the monitoring with training and supervision from the first author. On-site testing was conducted using a HACH multimeter (HQ 40D) with a conductivity (CDC40101) probe, and a Hanna turbidimeter (HI93703). pH (PHC10101), fluoride (ISEF12101), and E. coli and total coliforms (IDEXX Quanti-Tray2000 system with Colilert-18 growth medium) were analysed in the lab. Details of the sampling protocol including weekly quality assurance and control steps are in Supplementary File S2. |
| (5) LWM survey series | November 2018–July 2020 | Fifty-two LWMs: 28 CBM committee members, 15 school administrators, 3 health facility officers, and 6 private owners. 81% presented as male. The median level of participation in the survey series was 86% (limited primarily by supply functionality and periodic absence of LWMs). | A series of 5 surveys to track LWMs’ reactions to the monitoring results including changes in their perceptions, intentions, and behaviours around drinking-water safety. The surveys were conducted (1) before monitoring, (2) after the first reporting, (3) monthly check-ins, (4) at the end of 2019, (5) mid-2020. Table S1 provides an overview of the integrated fear appeal framework concepts assessed in each survey. The questionnaires are provided in Supplementary File S3. | Two of the co-authors conducted the surveys with training from the first author. They lived and worked in rural Kitui prior to this project and each have >4 years of training and experience in water services. Most of the survey questions were open-ended and responses were summarized in paragraphs on paper forms. Each survey was piloted for a week to refine questions and confirm a common understanding of aims among the research team. Data were digitized and checked for comprehensiveness and consistency weekly, with follow-ups for clarification carried out as needed. |
| (6) LWM semi-structured interviews | July–August 2019 | Thirty-eight LWMs: Repeated attempts were made in July and August to interview all 52 LWMs but 4 school and 13 CBM LWMs were not available, and 1 private LWM declined to be interviewed. | Semi-structured interviews to discuss LWM views on water safety; the utility and drawbacks of monitoring; and options, roles, and responsibilities for managing water quality. Conceptual framework terminology was not used in the interview, which was designed to facilitate relatable discussion focused on the practical and specific rather than abstract concepts (see the interview guide in Supplementary File S4). | The interviews were conducted in English (27) or a blend of Kiswahili and Kikamba (11) by the first author and 2 of the co-authors. We used audio recording and verbatim transcription for all but 2 interviews, for which the interviewees preferred that only written notes be used. During post-interview debriefs and the transcription process, ambiguities were discussed by the interview team and annotations were added to guide later analysis. In 4 cases we contacted the LWMs for further clarification. |
2.4. Data Analysis
3. Results
3.1. Water Quality Results Overview
3.2. Water User Perceptions of Threat and Efficacy
3.3. Household-Level Water Management Choices
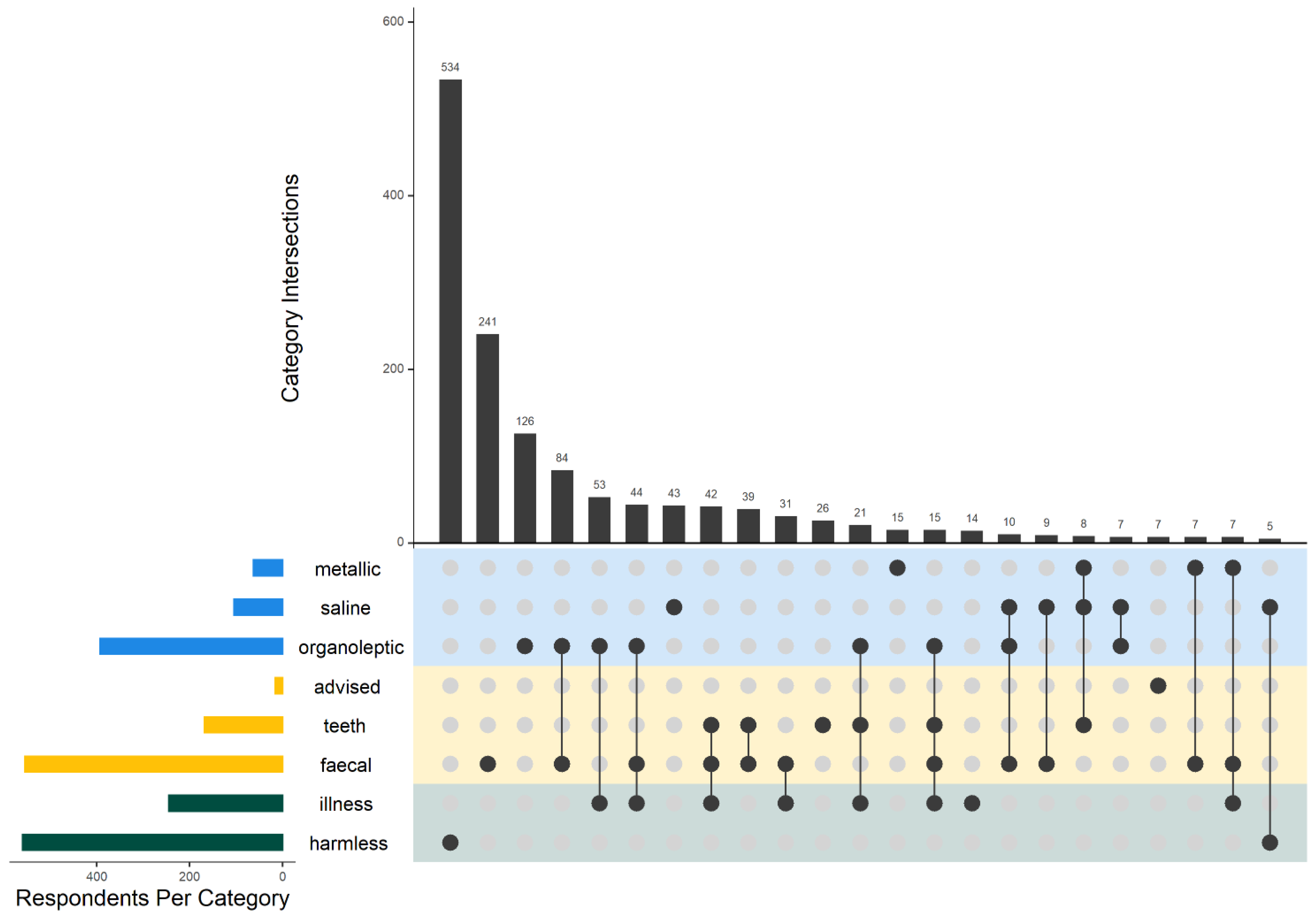
- clean drinking-water was not otherwise available (159 responses from 62 households);
- to avoid previously experienced illness (102 responses from 27 households);
- to kill germs/bacteria (63 from 31) or visible worms and insects (14 from 11);
- to protect a sick person (21 from 14), young child (10 from 3), or visitors (6 from 4);
- because it was advised by a doctor (12 from 6) or NGO (11 from 4);
- to avoid salinity (2 from 2);
- or out of habit (1 from 1).
3.4. Lay Water Manager Baseline Awareness
3.5. Changes in Perceived Susceptibility
- positive affect display with sustained low susceptibility;
- surprise with increased susceptibility;
- uncertainty with sustained medium susceptibility; and
- disinterest and undetermined affect display with sustained high susceptibility.
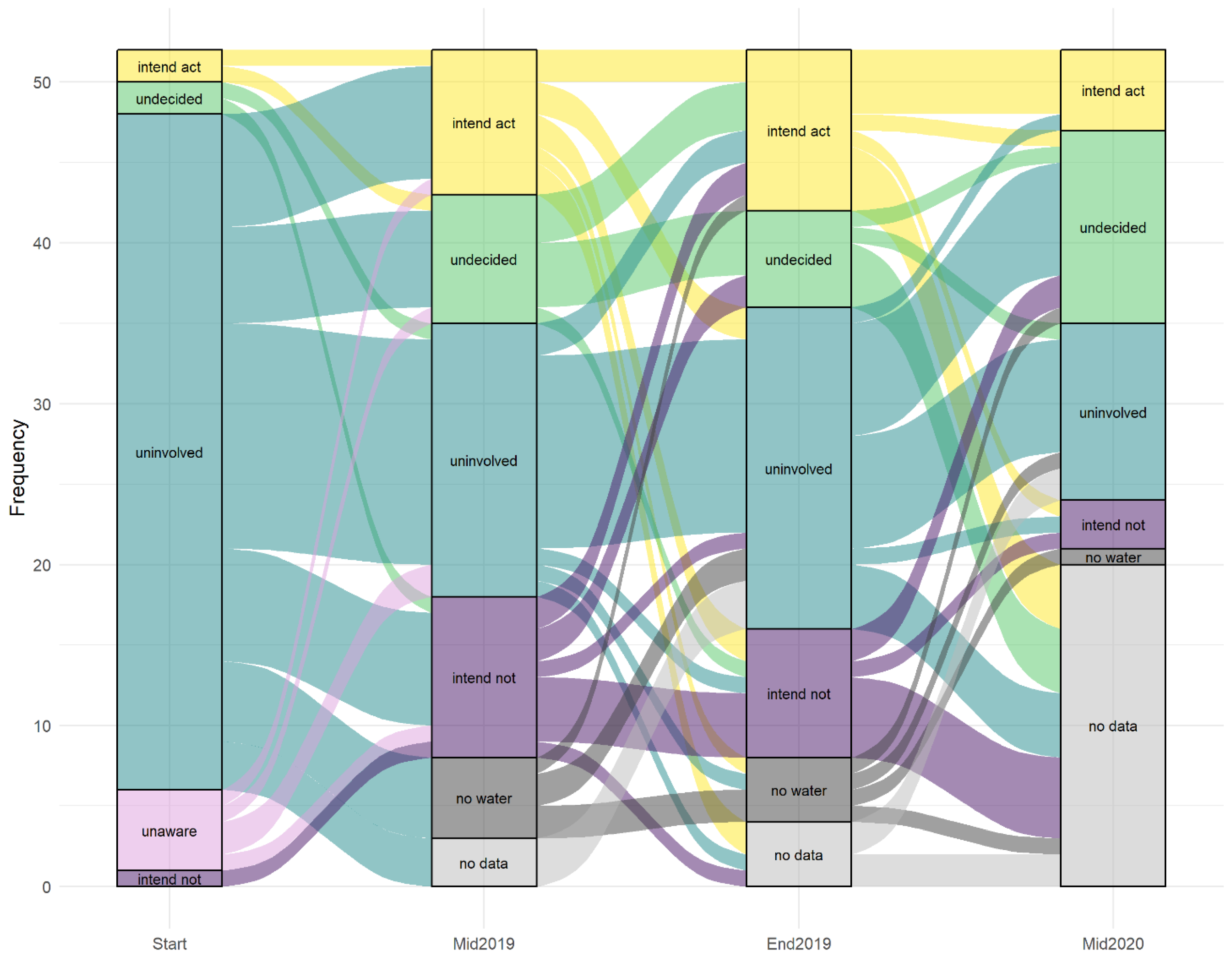
3.6. Evolution of Stages of Change
4. Discussion
4.1. Threat Information Specificity and Framing
4.2. Repeated Messaging and Maintaining the Problem-Focused Response
4.3. Situating Fear Appeals in Context
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tannenbaum, M.B.; Hepler, J.; Zimmerman, R.S.; Saul, L.; Jacobs, S.; Wilson, K.; Albarracin, D. Appealing to fear: A meta-analysis of fear appeal effectiveness and theories. Psychol. Bull. 2015, 141, 1178–1204. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, M.E.; Kincaid, D.L. Social, Cultural and Behavioral Correlates of Household Water Treatment and Storage. In Center Publication HCI 2010-1: Health Communication Insights; Center for Communication Programs, Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2010. [Google Scholar]
- Meadows, D.H. Thinking in Systems: A Primer; Wright, D., Ed.; Earthscan: London, UK, 2008; ISBN 9781844077267. [Google Scholar]
- Dupas, P. What matters (and What Does Not) in households’ decision to invest in malaria prevention? Am. Econ. Rev. 2009, 99, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duflo, E.; Dupas, P.; Kremer, M. Education, HIV, and early fertility: Experimental evidence from Kenya. Am. Econ. Rev. 2015, 105, 2757–2797. [Google Scholar] [CrossRef] [PubMed]
- Hunter, P.D.; Hanley, N.; Czajkowski, M.; Mearns, K.; Tyler, A.N.; Carvalho, L.; Codd, G.A. The effect of risk perception on public preferences and willingness to pay for reductions in the health risks posed by toxic cyanobacterial blooms. Sci. Total Environ. 2012, 426, 32–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, B.; Arana, B.; Mäusezahl, D.; Hubbard, A.; Colford, J.M. Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int. J. Epidemiol. 2009, 38, 1651–1661. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Mendoza, C.; Keswick, B.H.; Chiller, T.M.; Hoekstra, R.M. Difficulties in bringing point-of-use water treatment to scale in rural Guatemala. Am. J. Trop. Med. Hyg. 2008, 78, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Makutsa, P.; Nzaku, K.; Ogutu, P.; Barasa, P.; Ombeki, S.; Mwaki, A.; Quick, R. Challenges in implementing a point-of-use water quality intervention in rural Kenya. Am. J. Public Health 2001, 9, 157. [Google Scholar] [CrossRef]
- Null, C.; Meeks, R.; Miguel, E.; Zwane, A.P. Safe drinking water. Who is willing to pay the price? Int. Initiat. Impact Eval. 2012, Systematic Review 006, 1–36. [Google Scholar]
- World Health Organization; UNICEF Joint Monitoring Programme. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines 2017. Available online: https://www.who.int/mediacentre/news/releases/2017/launch-version-report-jmp-water-sanitation-hygiene.pdf (accessed on 7 December 2021).
- Sutton, S.; Butterworth, J. Self-Supply: Filling the Gaps in Public Water Supply Provision; Practical Action Publishing: Rugby, UK, 2021; ISBN 9781788530439. [Google Scholar]
- IHME. GBD Compare Data Visualisation. Available online: http://www.healthdata.org/data-visualization/gbd-compare (accessed on 17 March 2021).
- World Health Organization; UNICEF Joint Monitoring Programme. Progress on Household Drinking Water, Sanitation and Hygiene 2000–2017. Special Focus on Inequalities; World Health Organization: New York, NY, USA, 2019. [Google Scholar]
- Prüss-Ustün, A.; Wolf, J.; Bartram, J.; Clasen, T.; Cumming, O.; Freeman, M.C.; Gordon, B.; Hunter, P.R.; Medlicott, K.; Johnston, R. Burden of disease from inadequate water, sanitation and hygiene for selected adverse health outcomes: An updated analysis with a focus on low- and middle-income countries. Int. J. Hyg. Environ. Health 2019, 222, 765–777. [Google Scholar] [CrossRef]
- Katz, T.; Sara, J. Making Rural Water Supply Sustainable: Recommendations from a Global Study; UNDP-World Bank Water and Sanitation Program: Washington, DC, USA, 1997. [Google Scholar]
- Lockwood, H.; Smits, S. Supporting Rural Water Supply: Moving towards a Service Delivery Approach; IRC, Aguaconsult, Practical Action Publishing: Rugby, UK, 2011; ISBN 978-1-85339-729-5. [Google Scholar]
- Harvey, P.A.; Reed, R.A. Community-managed water supplies in Africa: Sustainable or dispensable? Community Dev. J. 2007, 42, 365–378. [Google Scholar] [CrossRef]
- Mugumya, F. Enabling Community-Based Water Management Systems: Governance and Sustainability of Rural Point-water Facilities in Uganda. Ph.D. Thesis, Dublin City University, Dublin, Ireland, 2013. [Google Scholar]
- Fischer, A.; Hope, R.; Manandhar, A.; Hoque, S.; Foster, T.; Hakim, A.; Islam, S.; Bradley, D. Risky responsibilities for rural drinking water institutions: The case of unregulated self-supply in Bangladesh. Glob. Environ. Chang. 2020, 65, 102152. [Google Scholar] [CrossRef]
- Koehler, J.; Rayner, S.; Katuva, J.; Thomson, P.; Hope, R. A cultural theory of drinking water risks, values and institutional change. Glob. Environ. Chang. 2018, 50, 268–277. [Google Scholar] [CrossRef]
- Kelsall, T. Going with the Grain in African Development? Dev. Policy Rev. 2011, 29, s223–s251. [Google Scholar] [CrossRef] [Green Version]
- Bakker, K. Privatizing Water: Governance Failure and the World’s Urban Water Crisis; Cornell University Press: New York, NY, USA, 2010; ISBN 10987654321. [Google Scholar]
- Whaley, L.; Cleaver, F. Can ‘functionality’ save the community management model of rural water supply? Water Resour. Rural Dev. 2017, 9, 56–66. [Google Scholar] [CrossRef]
- Rusca, M.; Schwartz, K. “Going with the grain”: Accommodating local institutions in water governance. Curr. Opin. Environ. Sustain. 2014, 11, 34–38. [Google Scholar] [CrossRef]
- Bartram, J.; Brocklehurst, C.; Fisher, M.B.; Luyendijk, R.; Hossain, R.; Wardlaw, T.; Gordon, B. Global monitoring of water supply and sanitation: History, methods and future challenges. Int. J. Environ. Res. Public Health 2014, 11, 8137–8165. [Google Scholar] [CrossRef] [Green Version]
- Bain, R.; Cronk, R.; Hossain, R.; Bonjour, S.; Onda, K.; Wright, J.; Yang, H.; Slaymaker, T.; Hunter, P.; Pruss-Ustun, A.; et al. Global assessment of exposure to faecal contamination through drinking water based on a systematic review. Trop. Med. Int. Heal. 2014, 19, 917–927. [Google Scholar] [CrossRef] [Green Version]
- Wolf, J.; Bonjour, S.; Prüss-Ustün, A. An exploration of multilevel modeling for estimating access to drinking-water and sanitation. J. Water Health 2013, 11, 64–77. [Google Scholar] [CrossRef]
- Moriarty, P.; Smits, S.; Butterworth, J.; Franceys, R. Trends in rural water supply: Towards a service delivery approach. Water Altern. 2013, 6, 329–349. [Google Scholar]
- Peletz, R.; Kumpel, E.; Bonham, M.; Rahman, Z.; Khush, R. To what extent is drinking water tested in sub-saharan Africa? A comparative analysis of regulated water quality monitoring. Int. J. Environ. Res. Public Health 2016, 13, 275. [Google Scholar] [CrossRef] [Green Version]
- Gerlach, E. Regulating Rural Water Supply Services: A Comparative Review of Existing and Emerging Approaches with a Focus on GIZ Partner Countries; Deutsche Gesellschaft für Internationale Zusammenarbeit: Eschborn, Germany, 2019. [Google Scholar]
- Government of Kenya. The Water Act: No. 43 of 2016; Government of Kenya: Nairobi, Kenya, 2016; Volume 164.
- Water Services Regulatory Board. Guideline for Provision of Water and Sanitation Services in Rural and Underserved Areas in Kenya; Water Services Regulatory Board: Nairobi, Kenya, 2019. [Google Scholar]
- Nowicki, S.; Koehler, J.; Charles, K.J. Including water quality monitoring in rural water services: Why safe water requires challenging the quantity versus quality dichotomy. NPJ Clean Water 2020, 3, 14. [Google Scholar] [CrossRef] [Green Version]
- Bradley, D.J.; Bartram, J. Domestic water and sanitation as water security: Monitoring, concepts and strategy. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20120420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koehler, J.; Thomson, P.; Hope, R. Pump-Priming Payments for Sustainable Water Services in Rural Africa. World Dev. 2015, 74, 397–411. [Google Scholar] [CrossRef] [Green Version]
- MacAllister, D.J.; MacDonald, A.M.; Kebede, S.; Godfrey, S.; Calow, R. Comparative performance of rural water supplies during drought. Nat. Commun. 2020, 11, 1099. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.; Foster, T.; MacDonald, M.C.; Harris, A.R.; Schwab, K.J.; Hadwen, W.L. Addressing how multiple household water sources and uses build water resilience and support sustainable development. NPJ Clean Water 2019, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Balasubramanya, S.; Pfaff, A.; Bennear, L.; Tarozzi, A.; Matin Ahmed, K.; Schoenfeld, A.; van Geen, A. Evolution of household’s responses to the groundwater arsenic crisis in Bangladesh: Information on environmental health risks can have increasing behavioural impact over time. Environ. Dev. Econ. 2014, 19, 631–647. [Google Scholar] [CrossRef] [Green Version]
- Bennear, L.; Tarozzi, A.; Pfaff, A.; Balasubramanya, S.; Matin Ahmed, K.; van Geen, A. Impact of a randomized controlled trial in arsenic risk communication on household water-source choices in Bangladesh. J. Environ. Econ. Manag. 2013, 65, 225–240. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Hamoudi, A.; Jeuland, M.; Turrini, G. Seeing, believing, and behaving: Heterogeneous effects of an information intervention on household water treatment. J. Environ. Econ. Manag. 2017, 86, 141–159. [Google Scholar] [CrossRef]
- Davis, J.; Pickering, A.J.; Rogers, K.; Mamuya, S.; Boehm, A.B. The effects of informational interventions on household water management, hygiene behaviors stored drinking water quality and hand contamination in Peri-Urban Tanzania. Am. J. Trop. Med. Hyg. 2011, 84, 184–191. [Google Scholar] [CrossRef]
- Hamoudi, A.; Jeuland, M.; Lombardo, S.; Patil, S.; Pattanayak, S.K.; Rai, S. The effect of water quality testing on household behavior: Evidence from an experiment in rural India. Am. J. Trop. Med. Hyg. 2012, 87, 18–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leidner, A.J. Estimating the Effectiveness of Health-Risk Communications with Propensity-Score Matching: Application to Arsenic Groundwater Contamination in Four US Locations. J. Environ. Public Health 2014, 2014, 783902. [Google Scholar] [CrossRef]
- Lucas, P.J.; Cabral, C.; Colford, J.M. Dissemination of drinking water contamination data to consumers: A systematic review of impact on consumer behaviors. PLoS ONE 2011, 6, e21098. [Google Scholar] [CrossRef] [PubMed]
- Trent, M.; Dreibelbis, R.; Bir, A.; Tripathi, S.N.; Labhasetwar, P.; Nagarnaik, P.; Loo, A.; Bain, R.; Jeuland, M.; Brown, J. Access to Household Water Quality Information Leads to Safer Water: A Cluster Randomized Controlled Trial in India. Environ. Sci. Technol. 2018, 52, 5319–5329. [Google Scholar] [CrossRef] [PubMed]
- Okyere, C.Y.; Pangaribowo, E.H.; Asante, F.A.; von Braun, J. ZEF-Discussion Papers on Development Policy No. 234: The Impacts of Household Water Quality Testing and Information on Safe Water Behaviors: Evidence from a Randomized Experiment in Ghana; Zentrum für Entwicklungsforschung: Bonn, Germany, 2017. [Google Scholar]
- Levison, M.M.; Elliott, S.J.; Karanja, D.M.S.; Schuster-Wallace, C.J.; Harrington, D.W. You cannot prevent a disease; you only treat diseases when they occur: Knowledge, attitudes and practices to water-health in a rural Kenyan community. East Afr. J. Public Health 2011, 8, 103–111. [Google Scholar]
- Robinson, D.T.; Schertenleib, A.; Kunwar, B.M.; Shrestha, R.; Bhatta, M.; Marks, S.J. Assessing the impact of a risk-based intervention on piped water quality in rural communities: The case of mid-western Nepal. Int. J. Environ. Res. Public Health 2018, 15, 1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.; Smith, S.W. The effects of fear appeal message repetition on perceived threat, perceived efficacy, and behavioral intention in the extended parallel process model. Health Commun. 2016, 31, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Salmon, C.T. Fear Appeals for Individuals in Different Stages of Change: Intended and Unintended Effects and Implications on Public Health Campaigns. Health Commun. 2006, 20, 91–99. [Google Scholar] [CrossRef]
- Manika, D.; Gregory-Smith, D. Health marketing communications: An integrated conceptual framework of key determinants of health behaviour across the stages of change. J. Mark. Commun. 2017, 23, 22–72. [Google Scholar] [CrossRef]
- Neely, K. Systems Thinking and WASH: Tools and Case Studies for a Sustaintable Water Supply; Neely, K., Ed.; Practical Action Publishing: Rugby, UK, 2019; ISBN 9781780447483. [Google Scholar]
- Witte, K. Putting the fear back into fear appeals: The extended parallel process model. Commun. Monogr. 1992, 59, 329–349. [Google Scholar] [CrossRef]
- Weinstein, N.D.; Sandman, P.M.; Blalock, S.J. The Precaution Adoption Process Model. In Health Behavior and Health Education: Theory, Research and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 123–147. ISBN 9780787996147. [Google Scholar]
- Rogers, R.W. Cognitive and physiological processes in fear appeals and attitude change: A revised theory of protection motivation. In Social Psychophysiology; Cacioppo, J.T., Petty, R.E., Eds.; Guilford: New York, NY, USA, 1983; pp. 153–176. [Google Scholar]
- Leventhal, H. Findings and theory in the study of fear communications. In Advances in Experimental Social Psychology; Berkowitz, L., Ed.; Academic Press: New York, NY, USA, 1970; Volume 5. [Google Scholar]
- Hovland, C.; Janis, I.; Kelly, H. Communication and Persuasion; Yale University Press: New Haven, CT, USA, 1953. [Google Scholar]
- Van’t Riet, J.; Ruiter, R.A.C. Defensive reactions to health-promoting information: An overview and implications for future research. Health Psychol. Rev. 2013, 7, S104–S136. [Google Scholar] [CrossRef]
- Popova, L. The Extended Parallel Process Model: Illuminating the Gaps in Research. Heal. Educ. Behav. 2012, 39, 455–473. [Google Scholar] [CrossRef]
- Roberto, A.J.; Mongeau, P.A.; Liu, Y.; Hashi, E.C. “Fear the Flu, Not the Flu Shot”: A Test of the Extended Parallel Process Model. J. Health Commun. 2019, 24, 829–836. [Google Scholar] [CrossRef]
- Maloney, E.K.; Lapinski, M.K.; Witte, K. Fear appeals and persuasion: A review and update of the extended parallel process model. Soc. Personal. Psychol. Compass 2011, 5, 206–219. [Google Scholar] [CrossRef]
- Weinstein, N.D. The Precaution Adoption Process. Heal. Psychol. 1988, 7, 355–386. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The Transtheoretical Model and Stages of Change. In Health Behavior: Theory, Research and Practice, 5th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015; pp. 125–148. ISBN 9781118629055. [Google Scholar]
- Hovick, S.R.; Bigsby, E.; Wilson, S.R.; Thomas, S. Information Seeking Behaviors and Intentions in Response to Environmental Health Risk Messages: A Test of A Reduced Risk Information Seeking Model. Health Commun. 2021, 36, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Kenya National Bureau of Statistics. 2019 Kenya Population and Housing Census; Government of Kenya: Nairobi, Kenya, 2019; Volume II.
- Kenya National Bureau of Statistics. Basic Report: 2015/16 Kenya Integrated Household Budget Survey (KIHBS); Kenya National Bureau of Statistics: Nairobi, Kenya, 2018.
- World Health Organization; UNICEF Joint Monitoring Programme. WHO UNICEF Joint Monitoring Programme: Household Data. 2021. Available online: https://washdata.org/data/household#!/ (accessed on 7 December 2021).
- Katuva, J.; Hope, R.; Foster, T.; Koehler, J.; Thomson, P. Modelling welfare transitions to prioritise sustainable development interventions in coastal Kenya. Sustainability 2020, 12, 6943. [Google Scholar] [CrossRef]
- WHO. Guidelines for Drinking-Water Quality: Fourth Edition Incorporating the First Addendum, 4th ed.; WHO Press: Geneva, Switzerland, 2017; ISBN 9789241549950. [Google Scholar]
- Hoque, S.F.; Hope, R. The water diary method—Proof-of-concept and policy implications for monitoring water use behaviour in rural Kenya. Water Policy 2018, 20, 725–743. [Google Scholar] [CrossRef]
- Bukachi, S.A.; Omia, D.O.; Musyoka, M.M.; Wambua, F.M.; Peter, M.N.; Korzenevica, M. Exploring water access in rural Kenya: Narratives of social capital, gender inequalities and household water security in Kitui county. Water Int. 2021, 46, 677–696. [Google Scholar] [CrossRef]
- Kassambara, A. Multivariate Analysis II: Practical Guide to Principal Component Methods in R; STHDA, Online; CreateSpace Independent Publishing Platform: Scotts Valley, CA, USA, 2017; ISBN 9781975721138. [Google Scholar]
- Greenacre, M. Contribution biplots. J. Comput. Graph. Stat. 2013, 22, 107–122. [Google Scholar] [CrossRef]
- Conway, J.R.; Lex, A.; Gehlenborg, N. UpSetR: An R package for the visualization of intersecting sets and their properties. Bioinformatics 2017, 33, 2938–2940. [Google Scholar] [CrossRef] [Green Version]
- Thaler, R.; Sunstein, C. Nudge: Improving Decisions about Health, Wealth and Happiness; Penguin Books: London, UK, 2009; ISBN 978-0-141-04001-1. [Google Scholar]
- De França Doria, M. Factors influencing public perception of drinking water quality. Water Policy 2010, 12, 1–19. [Google Scholar] [CrossRef]
- Pickering, A.J.; Null, C.; Winch, P.J.; Mangwadu, G.; Arnold, B.F.; Prendergast, A.J.; Njenga, S.M.; Rahman, M.; Ntozini, R.; Benjamin-Chung, J.; et al. The WASH Benefits and SHINE trials: Interpretation of WASH intervention effects on linear growth and diarrhoea. Lancet Glob. Health 2019, 7, e1139–e1146. [Google Scholar] [CrossRef] [Green Version]
- Libey, A.; Adank, M.; Thomas, E. Who pays for water? Comparing life cycle costs of water services among several low, medium and high-income utilities. World Dev. 2020, 136, 105155. [Google Scholar] [CrossRef]
- Ray, I.; Smith, K.R. Viewpoint towards safe drinking water and clean cooking for all. Lancet Glob. Heal. 2021, 1–5. [Google Scholar] [CrossRef]
- Banerjee, A.V.; Duflo, E. Poor Economics: A Radical Rethinking of the Way to Fight Global Poverty; Public Affairs: New York, NY, USA, 2011; ISBN 978-1-61039-093-4. [Google Scholar]
- Mullainathan, S.; Shafir, E. Scarcity: Why Having too Little Means so Much; Picador: New York, NY, USA, 2013. [Google Scholar]
- Lora-Wainwright, A. Resigned Activism: Living with Pollution in Rural China; The MIT Press: Cambridge, MA, USA, 2017; ISBN 9780262365314. [Google Scholar]
- Roaf, V.; Winkler, I.; Schiessl, M.; Blyberg, A.; Cullet, P.; Fedotova, T.; van den Lande, L.; Martins, P.; Musembi, C.; Neumeyer, H.; et al. Realising the Human Rights to Water and Sanitation: A Handbookby the UN Special Rapporteur Catarina de Albuquerque; UN Special Rapporteur on Water and Sanitation: Geneva, Switzerland, 2014; ISBN 9789892049809. [Google Scholar]
- Helmsing, A.H.J. Decentralisation, enablement, and local governance in low-income countries. Environ. Plan. C Gov. Policy 2002, 20, 317–340. [Google Scholar] [CrossRef]
- Rawls, J. A Theory of Justice; Harvard University Press: London, UK, 1971. [Google Scholar]
- Britz, J.J. To know or not to know: A moral reflection on information poverty. J. Inf. Sci. 2004, 30, 192–204. [Google Scholar] [CrossRef]
- Nowicki, S.; DeLaurent, Z.R.; de Villiers, E.P.; Githinji, G.; Charles, K.J. The utility of Escherichia coli as a contamination indicator for rural drinking water: Evidence from whole genome sequencing. PLoS ONE 2021, 16, e0245910. [Google Scholar] [CrossRef]
- Curtis, V.; Dreibelbis, R.; Buxton, H.; Izang, N.; Adekunle, D.; Aunger, R. Behaviour settings theory applied to domestic water use in Nigeria: A new conceptual tool for the study of routine behaviour. Soc. Sci. Med. 2019, 235, 112398. [Google Scholar] [CrossRef]
- Dery, F.; Bisung, E.; Dickin, S.; Dyer, M. Understanding empowerment in water, sanitation, and hygiene (WASH): A scoping review. J. Water Sanit. Hyg. Dev. 2020, 10, 5–15. [Google Scholar] [CrossRef]
- Murray-Johnson, L.; Witte, K.; Liu, W.Y.; Hubbell, A.P.; Sampson, J.; Morrison, K. Addressing cultural orientations in fear appeals: Promoting AIDS-protective behaviors among Mexican immigrant and African American adolescents and American and Taiwanese college students. J. Health Commun. 2001, 6, 335–358. [Google Scholar] [CrossRef]








| Theme | Cases | % Coding Coverage 1 | Description | Example Quote |
|---|---|---|---|---|
| (1) Surface water is especially unsafe | 31 | 4.0 (1.3–8.3) | Participants pointed to the openness and stagnation of water as hazardous, and they linked the threat of disease (speaking of typhoid, amoebiasis, cholera, dysentery, stomach problems and diarrhoea) to inadequate separation of water from livestock, wildlife, latrines, and open defecation, with ‘dirt’ or ‘faeces’ carried into the water by rain (overland flow), on people’s shoes, or on containers and ropes that are used to draw water. | “There are places where people have not dug pit latrines, there are animals that have died and decayed in the bushes, and other bad things. When it rains, then all that dirt is swept by the rainwater and drained in the earth dam. Even now, the rain is not here but whatever dirt was brought before is still in the water source.”—P35F |
| (2) There is a microbial vs. chemical quality trade-off for groundwater | 20 | 1.6 (0.5–4.2) | Participants recognized that groundwater is better protected from faecal contamination but they highlighted that the suitability of many groundwater supplies for drinking and cooking purposes is limited by salinity and bitterness, especially during dry seasons. Participants linked salty water to unquenched thirst, constipation, bloating, and gastrointestinal pain, which one woman described as “slashing your intestines into pieces”. Participants asked about the potential health impacts of salinity on livestock, but they did not discuss chronic health consequences for themselves. | “Water from the boreholes is safe for human consumption since it is well covered and protected from all sources of contamination. However, … it is limited in use due to its saltiness.”—P07M |
| (3) Lack of specific external stimuli limits judgement of water safety | 19 | 1.7 (0.2–5.4) | General knowledge about water contamination is widespread, but none of the participants had received test results for the water supplies that they relied on. Participants discussed the limitations of assessing water quality based on organoleptic properties. On the one hand they may have a bad reaction from drinking water even if it appears clean but, on the other hand, when they become sick they usually cannot be confident of the cause. | “You have to realize that even if the water is dirty, we cannot tell because we don’t have a professional to check its quality or treat it. We just take the water the way it is, even when you get sick you can never tell whether it was the water or something else.”—P06M |
| (4) Water quality threats induce fear for oneself and others | 25 | 1.8 (0.2–3.9) | Participants spoke of prolonged stomach pain and needing to seek medical relief. Death and the contribution of waterborne illness to malnutrition were not directly discussed, but participants said that they fear dirty water and that infants are more susceptible to hygiene-related illness, including from unclean water. This view of heightened susceptibility extended to adults who are already weakened from illness. | “We have a lot of fears because, personally, I have stomach problems and if I take the water without boiling then the problem escalates. I also fear for my children because some of them have similar stomach problems.”—P04F |
| (5) Despite knowledge of threats, poverty constrains safe water practices | 20 | 3.5 (0.3–12.0) | Participants differentiated know-how, will, and capability to act. They discussed access and affordability issues that prevent them from acting on knowledge about water safety practices. They also highlighted the inability of communities to maintain NGO projects without ongoing support, especially in the face of difficult environmental conditions, vandalism, and theft. | “We were trained about the earth dam water and told that it is not clean, but due to our low-income levels and other problems we have here you may find people drinking the earth dam water just the way it is knowing very well it is not good for drinking.”—P35F |
| (6) Gender norms especially limit the self-efficacy of women | 31 | 4.8 (0.7–13.7) | Gender norms within families and the wider community limit opportunities for women to lead and participate in water management committees. Further, many water supplies have flexible payment structures that require users to strike an agreement with the owner or management committee. In most cases, the household head (usually men) makes these agreements, they also decide what portion of household income can be spent on water; consequently, they largely determine supply selection even if other household members (usually women) fetch water and manage its use within the household. | “I cannot say I have anything I do for livelihood, maybe a business or anything. I like the idea and I would very much want to do that, but my husband refuses... And this happens for most women. This really affects us in terms of provision for our children... you will find that [I] am the most knowledgeable person about the needs of the children and the household... Even when they are aware that we know all these, they say it is not possible to allow us to go sell their produce.”—P04F |
| (7) Water source protection is a collective action challenge | 25 | 2.4 (0.4–6.6) | Participants emphasized that self-efficacy is eclipsed by the need for collaboration and leadership from committees or owners in protecting water sources. They discussed examples where protective measures have failed due to lack of cooperation, presenting them as testament to the difficulty of sustaining protective measures despite strong motivation—water quality is only part of the motivation, participants were also concerned about drowning accidents, water shortages, and functionality issues. | “… it is very dirty, people have allowed [livestock] to enter the earth dam and urinate among other things... The thing is if you go and complain, no one listens to you. So, after a while you stop worrying and do what others are doing. If the consequences come, they affect you all.”—P06M |
| (8) Rural isolation limits self-efficacy | 19 | 2.0 (0.4–5.3) | Participants noted the lack of follow through on campaign promises and expressed a sense of isolation both by physical distance and political hierarchy. None of them were positive about their ability to attract or mobilize support from NGOs or the government (neither through the former system of chiefs nor the post-devolution system of village administrators). | “I think we are very deep in the rural areas, I don’t even know how you’ve reached here (chuckles), because nothing ever gets here. People only get to this area when they are in need of votes.”—P29F |
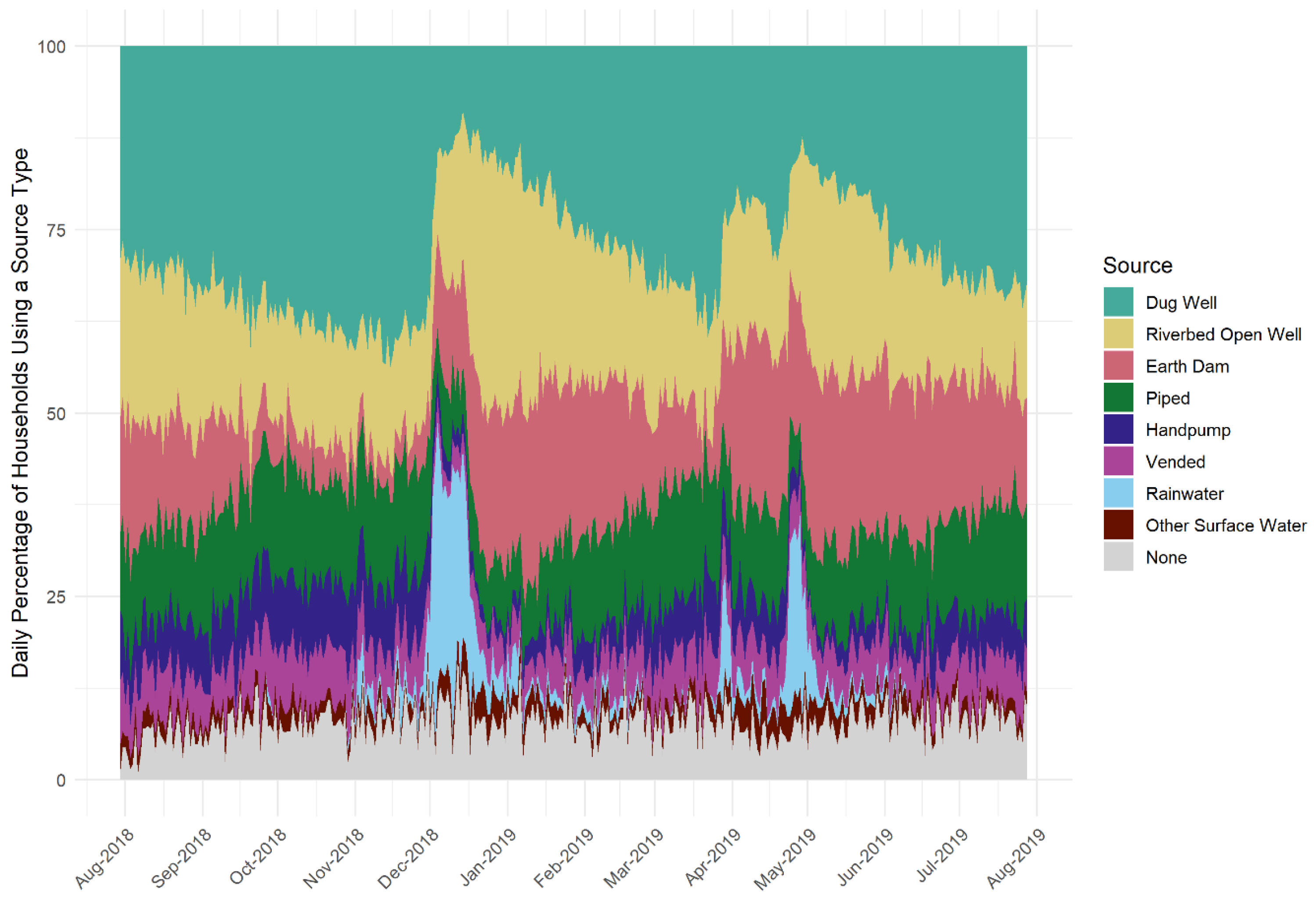
| (9) Supply selection is influenced by multiple dynamic factors | 35 | 11.0 (4.0–28.8) | Water supply selection varies in response to rainfall, distance, queuing, security, labour, monetary cost, livestock needs, personal relationships, functionality, and quality. Groundwater salinity limits alternatives to unprotected water supplies and is, therefore, a key constraint on collecting safer water. Further, distance and cost are even firmer constraints on choice than preference of different water qualities. Payment structure is also important: where people can borrow, pay with food, or offset monetary payments by providing labour for the maintenance of a water point, they can more consistently access a preferred supply. Supplies that require upfront payment in cash without exception are more challenging. | “When it gets very dry, the water gets saltier, but when it rains well, the salt is reduced—though not all the times... [In the dry season], people have to buy fresh water from the market kiosks which amounts to being very expensive for some of the community members... Unless one buys water from the salt-less wells, which are very few like three wells in this area.”—P11F |
| (10) Problem-focused water safety measures are employed intermittently | 20 | 1.5 (0.3–3.0) | Boiling, adding chlorine disinfectant, filtering water, or buying bottled water is done intermittently in response to specific stimuli including advice from doctors, to provide for new infants, or to protect people who are already ill. The key reason for not consistently maintaining measures to protect against water quality threats is that time, energy, and money must be put towards problem-focused responses to many different threats, some of which are more immediately severe than waterborne diseases. | “When a person fetches water and takes it home, most of them use it without doing anything to it not even treating it or even boiling it; but when they are told they have amoeba or typhoid, they start boiling the water or even use Water-Guard to treat the water.”—P13M |
| (11) Resources must be balanced for problemfocused responses to multiple threats | 29 | 2.7 (0.3–7.3) | In adopting problem-focused behaviour, participants balanced water quality threats against many others including attacks from people, hyenas, snakes, and majini (spirits) when walking to fetch water; thirst and fatigue from inadequate water access; unreliable rainfall and crops; flooding; falls into wells or reservoirs; chest problems from cooking fires; and communicable diseases including HIV. Participants also worried about keeping children in school. For girls, this intersected with concerns about gender-based disempowerment, sexual assault, early pregnancy, and abusive marriages. For boys, it intersected concerns about drug and alcohol abuse. | “People are having problems finding money to buy water. At the same time, they are also scared of selling their food to leave the children with nothing to eat. The fear is also because no one is sure that it will even rain.”—P30F |
| (12) Cognitive reappraisal, particularly resignation, is a common defensive response | 25 | 1.9 (0.3–6.4) | Participants framed their circumstances as uncontrollable; they were resigned to “use patience” and “persevere with the situation at hand”. One participant linked feeling a heavy burden to using resignation to “try navigate the challenges”. Other forms of cognitive re-appraisal were also expressed including religiosity (circumstances are in God’s hands), downward comparison (unsafe water is better than no water), self-exemption (the hazard is real, but I am not susceptible), and humour as reframing. | “For lack of alternative a woman can even start having labour pains when she is on her way from the water point... Some even suffer backaches up to now. But then how can we help them? This is how the world is.”—P20F |
| No. | Description | Main Cases | Secondary Cases | Intentions 1 | Actions 1 | Efficacy Gap 2 | Defensive Responses 1 |
|---|---|---|---|---|---|---|---|
| 1 | Reporting does not motivate formation of intentions. This pattern is associated with positive affect displays in response to sustained low perceived susceptibility (consistent absence of E. coli when the water was in regular use). | 7 | 0 | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–2) |
| 2 | Reporting prompts intention to act proactively (based on potential future threat but not current threat) or intentions to act are extended to other supplies. Despite E. coli negative results, accompanying information and/or prior test results prompt intention to act and information seeking (specifically, requesting test results from nearby alternative supplies for comparison). This pattern is associated with positive affect displays in response to low perceived susceptibility, but it is unclear what separates uninvolved LWMs (pattern 1) from those who extrapolate threat information and are motivated to engage with water safety measures despite E. coli-negative test results. | 7 | 10 | 2 (1–3) | 1 (0–2) | 1 (0–2) | 0 (0–2) |
| 3 | Reporting of a reduction in E. coli concentration relative to a previous test result prompts reversion from intention to act to uninvolved. This pattern is associated with positive affect displays in response to reduced perceived susceptibility relative to a previous report. | 8 | 14 | 2.5 (0–3) | 1 (0–2) | 1 (0–3) | 0 (0–2) |
| 4 | Sustained threat prompts initial variable engagement that evolves to uninvolved. This pattern is associated with regular concentrated E. coli contamination and the highest expected efficacy gaps, meaning the difference between the number of intentions voiced and the number of actions taken was largest for these LWMs. Defensive processing was most common for these LWMs, presumably supporting their return to the uninvolved stage, wherein they no longer consider adopting control measures. | 7 | 0 | 4 (1–5) | 1 (0–2) | 2 (1–4) | 3 (2–4) |
| 5 | Variable threat prompts long-term engagement with LWMs moving between indecision, intentions to act, and intentions to not act. This pattern is associated with changing perceptions of susceptibility and partial efficacy (actions do not fully control the threat). Defensive processing is indicated but respondents continue to acknowledge and want to address the threat. Respondents looked to test results for confirmation of the impact of their actions. | 16 | 5 | 3.5 (1–5) | 3 (1–4) | 1 (0–1) | 2 (0–4) |
| 6 | Sustained threat prompts sustained intention to act. This pattern is associated with regular concentrated E. coli contamination and is differentiated by higher self-efficacy with LWMs having know-how and ongoing resourcing to implement consistent chlorine disinfection (with support from NGOs in four out of the seven cases). | 7 | 1 | 3 (2–8) | 2 (2–5) | 1 (0–4) | 1 (0–3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowicki, S.; Bukachi, S.A.; Hoque, S.F.; Katuva, J.; Musyoka, M.M.; Sammy, M.M.; Mwaniki, M.; Omia, D.O.; Wambua, F.; Charles, K.J. Fear, Efficacy, and Environmental Health Risk Reporting: Complex Responses to Water Quality Test Results in Low-Income Communities. Int. J. Environ. Res. Public Health 2022, 19, 597. https://doi.org/10.3390/ijerph19010597
Nowicki S, Bukachi SA, Hoque SF, Katuva J, Musyoka MM, Sammy MM, Mwaniki M, Omia DO, Wambua F, Charles KJ. Fear, Efficacy, and Environmental Health Risk Reporting: Complex Responses to Water Quality Test Results in Low-Income Communities. International Journal of Environmental Research and Public Health. 2022; 19(1):597. https://doi.org/10.3390/ijerph19010597
Chicago/Turabian StyleNowicki, Saskia, Salome A. Bukachi, Sonia F. Hoque, Jacob Katuva, Mercy M. Musyoka, Mary M. Sammy, Martin Mwaniki, Dalmas O. Omia, Faith Wambua, and Katrina J. Charles. 2022. "Fear, Efficacy, and Environmental Health Risk Reporting: Complex Responses to Water Quality Test Results in Low-Income Communities" International Journal of Environmental Research and Public Health 19, no. 1: 597. https://doi.org/10.3390/ijerph19010597