
Data-Enhancement Strategies in Weather-Related Health Studies

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Proposed Strategies
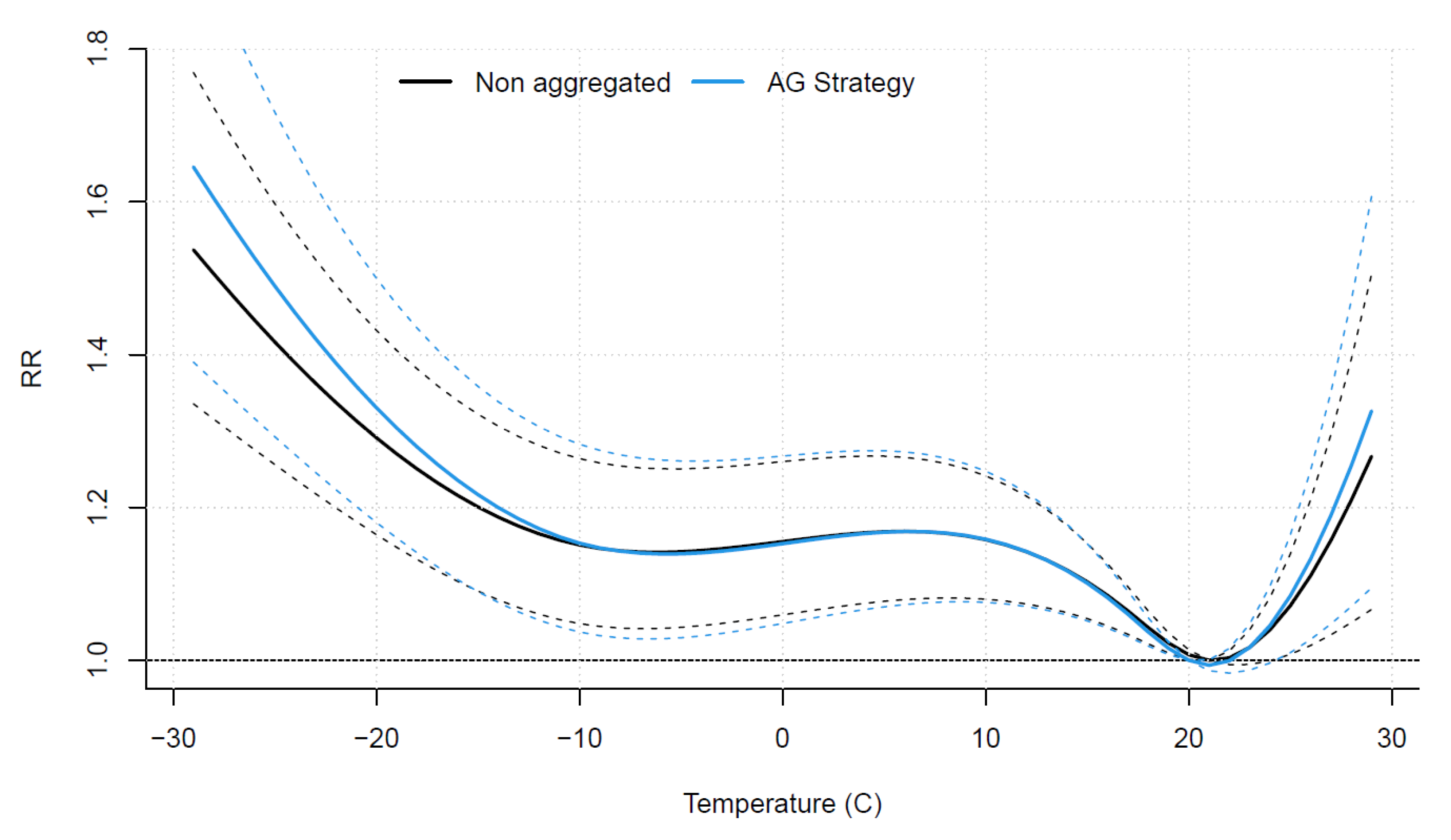
2.2.1. AG Strategy: Aggregating the Health Response
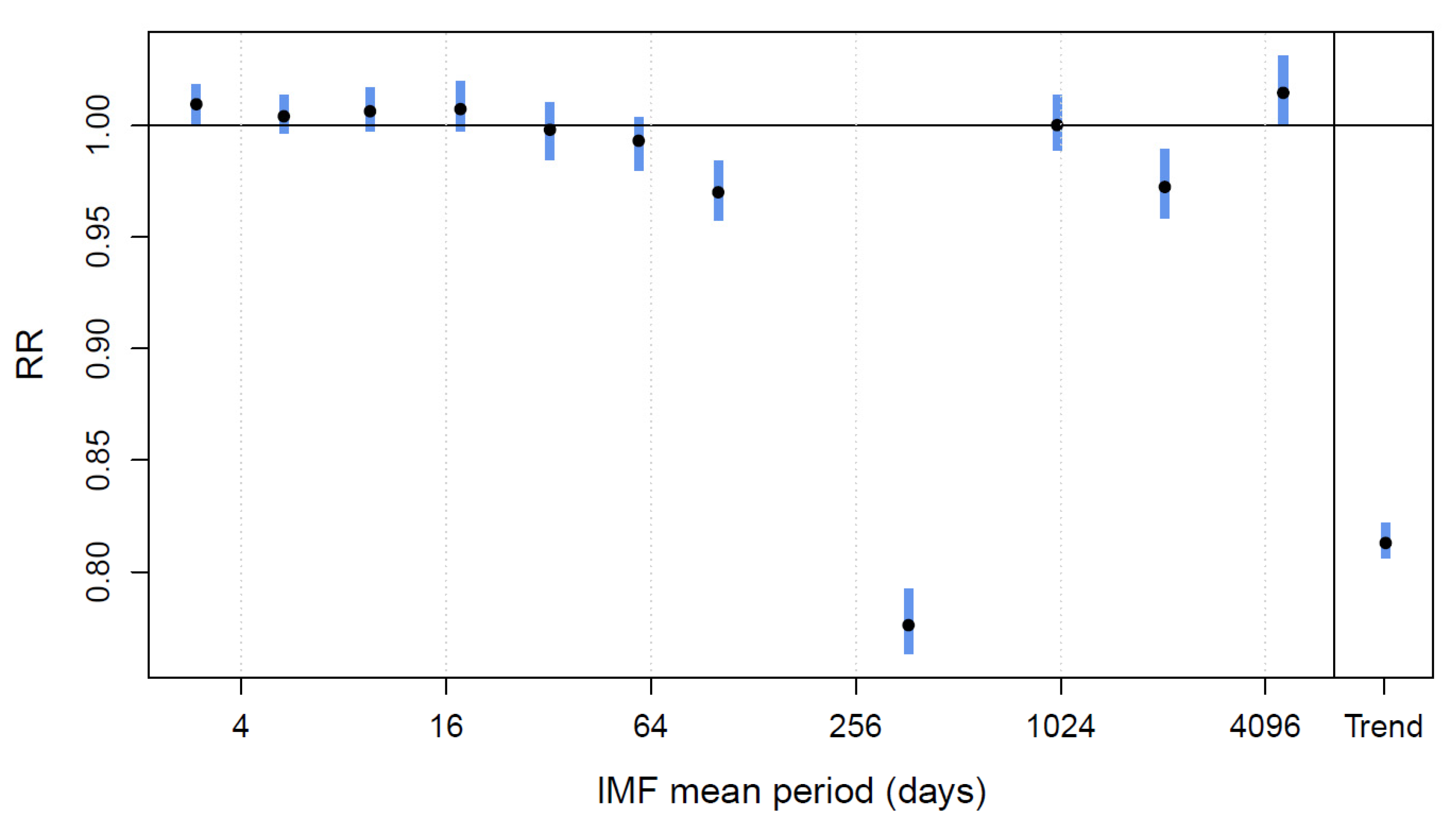
2.2.2. EMDR Strategy: Empirical Mode Decomposition Regression
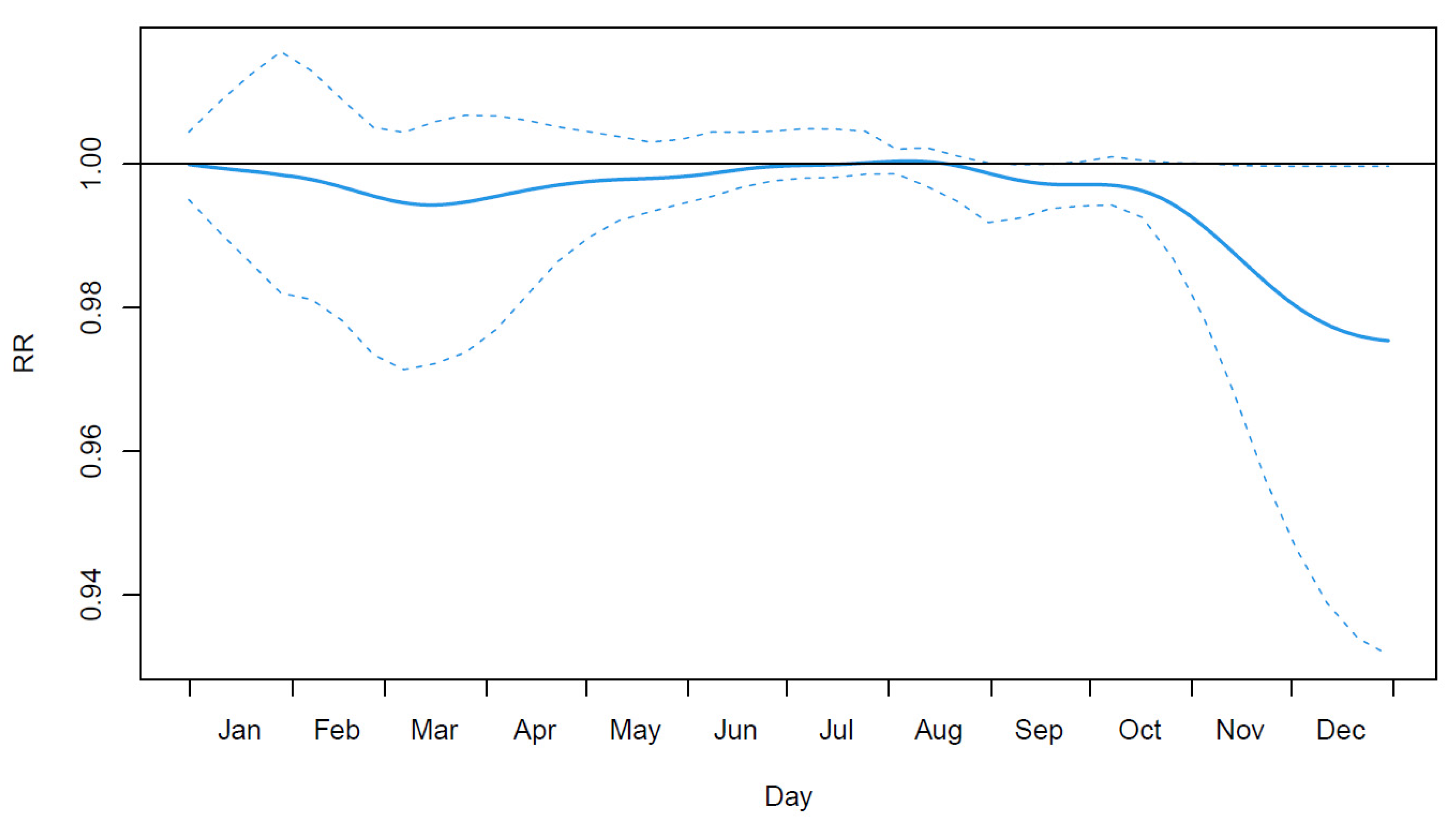
2.2.3. FY Strategy: Annual Variations through Functional Regression
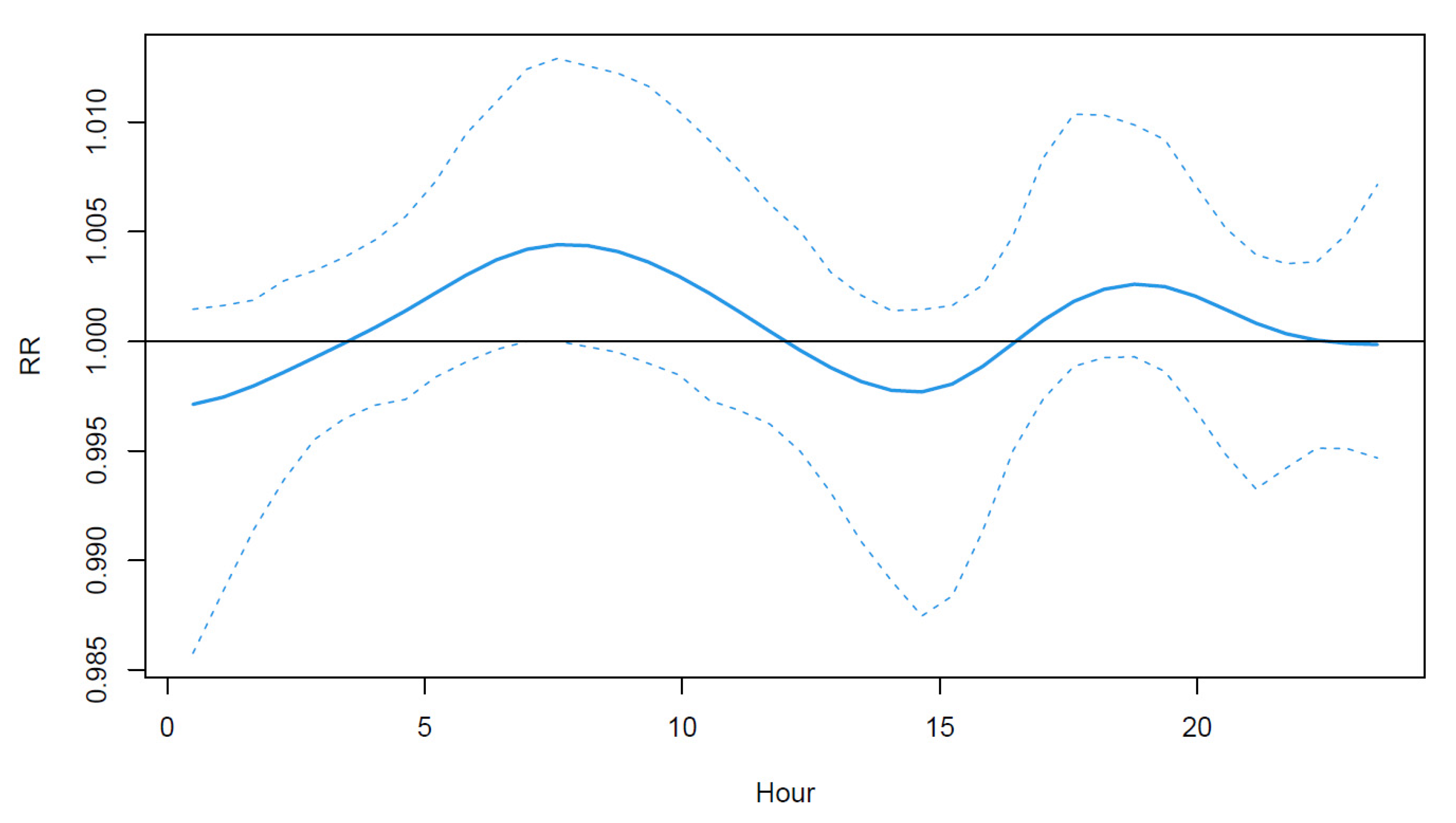
2.2.4. FD Strategy: Intraday Variation through Functional Regression
2.2.5. Numerical Comparison
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Belanger, D.; Abdous, B.; Valois, P.; Gosselin, P.; Sidi, E.A.L. A Multilevel Analysis to Explain Self-Reported Adverse Health Effects and Adaptation to Urban Heat: A Cross-Sectional Survey in the Deprived Areas of 9 Canadian Cities. BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.M.; Gu, S.H.; Bi, P.; Yang, J.; Liu, Q.Y. Heat Waves and Morbidity: Current Knowledge and Further Direction-A Comprehensive Literature Review. Int. J. Environ. Res. Public Health 2015, 12, 5256–5283. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.Y.; Guo, Y.M.; FitzGerald, G.; Aitken, P.; Tippett, V.; Chen, D.; Wang, X.M.; Tong, S.L. The Impacts of Heatwaves on Mortality Differ with Different Study Periods: A Multi-City Time Series Investigation. PLoS ONE 2015, 10, e0134233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keatinge, W.R. Winter Mortality and Its Causes. Int. J. Circumpolar Health 2002, 61, 292–299. [Google Scholar] [CrossRef]
- Kinney, P.L.; Schwartz, J.; Pascal, M.; Petkova, E.; Le Tertre, A.; Medina, S.; Vautard, R. Winter Season Mortality: Will Climate Warming Bring Benefits? Environ. Res. Lett. 2015, 10, 064016. [Google Scholar] [CrossRef] [PubMed]
- Barreca, A.I.; Shimshack, J.P. Absolute Humidity, Temperature, and Influenza Mortality: 30 Years of County-Level Evidence from the United States. Am. J. Epidemiol. 2012, 176, S114–S122. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.E.; Dougherty, E.; McArthur, C.; Huang, Q.S.; Baker, M.G. Cold, Dry Air Is Associated with Influenza and Pneumonia Mortality in Auckland, New Zealand. Influenza Other Respir. Viruses 2016, 10, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Vanasse, A.; Cohen, A.; Courteau, J.; Bergeron, P.; Dault, R.; Gosselin, P.; Blais, C.; Bélanger, D.; Rochette, L.; Chebana, F. Association between Floods and Acute Cardiovascular Diseases: A Population-Based Cohort Study Using a Geographic Information System Approach. Int. J. Environ. Res. Public Health 2016, 13, 168. [Google Scholar] [CrossRef] [Green Version]
- Modarres, R.; Ouarda, T.; Vanasse, A.; Orzanco, M.G.; Gosselin, P. Modeling Climate Effects on Hip Fracture Rate by the Multivariate GARCH Model in Montreal Region, Canada. Int. J. Biometeorol. 2014, 58, 921–930. [Google Scholar] [CrossRef]
- Analitis, A.; de’ Donato, F.; Scortichini, M.; Lanki, T.; Basagana, X.; Ballester, F.; Astrom, C.; Paldy, A.; Pascal, M.; Gasparrini, A.; et al. Synergistic Effects of Ambient Temperature and Air Pollution on Health in Europe: Results from the PHASE Project. Int. J. Environ. Res. Public Health 2018, 15, 1856. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Zhu, J. Amplified or Exaggerated Changes in Perceived Temperature Extremes under Global Warming. Clim. Dyn. 2019, 54, 117–127. [Google Scholar] [CrossRef]
- Demain, J.G. Climate Change and the Impact on Respiratory and Allergic Disease: 2018. Curr. Allergy Asthma Rep. 2018, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Ballester, J.; Robine, J.-M.; Herrmann, F.R.; Rodó, X. Long-Term Projections and Acclimatization Scenarios of Temperature-Related Mortality in Europe. Nat. Commun. 2011, 2, 358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Gasparrini, A.; Li, S.; Sera, F.; Vicedo-Cabrera, A.M.; de Sousa Zanotti Stagliorio Coelho, M.; Saldiva, P.H.N.; Lavigne, E.; Tawatsupa, B.; Punnasiri, K.; et al. Quantifying Excess Deaths Related to Heatwaves under Climate Change Scenarios: A Multicountry Time Series Modelling Study. PLoS Med. 2018, 15, e1002629. [Google Scholar] [CrossRef] [PubMed]
- Ebi, K.L. Greater Understanding Is Needed of Whether Warmer and Shorter Winters Associated with Climate Change Could Reduce Winter Mortality. Environ. Res. Lett. 2015, 10, 111002. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, B.; Sera, F.; Vicedo-Cabrera, A.M.; Abrutzky, R.; Åström, D.O.; Bell, M.L.; Chen, B.-Y.; de Sousa Zanotti Stagliorio Coelho, M.; Patricia Matus, C.; Dang Tran, N.; et al. The Role of Humidity in Associations of High Temperature with Mortality: A Multiauthor, Multicity Study. Environ. Health Perspect. 2019, 127, 097007. [Google Scholar] [CrossRef]
- Schwartz, J.; Samet, J.M.; Patz, J.A. Hospital Admissions for Heart Disease: The Effects of Temperature and Humidity. Epidemiology 2004, 15, 755–761. [Google Scholar] [CrossRef]
- Barreca, A.I. Climate Change, Humidity, and Mortality in the United States. J. Environ. Econ. Manag. 2012, 63, 19–34. [Google Scholar] [CrossRef] [Green Version]
- Vicedo-Cabrera, A.M.; Sera, F.; Guo, Y.; Chung, Y.; Arbuthnott, K.; Tong, S.; Tobias, A.; Lavigne, E.; de Sousa Zanotti Stagliorio Coelho, M.; Hilario Nascimento Saldiva, P.; et al. A Multi-Country Analysis on Potential Adaptive Mechanisms to Cold and Heat in a Changing Climate. Environ. Int. 2018, 111, 239–246. [Google Scholar] [CrossRef]
- Liu, T.; Ma, W. Climate Change and Health: More Research on Adaptation Is Needed. Lancet Planet. Health 2019, 3, e281–e282. [Google Scholar] [CrossRef] [Green Version]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time Series Regression Studies in Environmental Epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Goggins, W.B.; Yang, C.; Hokama, T.; Law, L.S.K.; Chan, E.Y.Y. Using Annual Data to Estimate the Public Health Impact of Extreme Temperatures. Am. J. Epidemiol. 2015, 182, 80–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparrini, A. The Case Time Series Design. Epidemiology 2021, 32, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Dell’Aniello, S.; Suissa, D.; Ernst, P. Friday and Weekend Hospital Stays: Effects on Mortality. Eur. Respir. J. 2014, 44, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Masselot, P.; Chebana, F.; Bélanger, D.; St-Hilaire, A.; Abdous, B.; Gosselin, P.; Ouarda, T.B.M.J. Aggregating the Response in Time Series Regression Models, Applied to Weather-Related Cardiovascular Mortality. Sci. Total Environ. 2018, 628–629, 217–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epanechnikov, V.A. Non-Parametric Estimation of a Multivariate Probability Density. Theory Probab. Its Appl. 1969, 14, 153–158. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed Lag Non-Linear Models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality Risk Attributable to High and Low Ambient Temperature: A Multicountry Observational Study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Rehill, N.; Armstrong, B.; Wilkinson, P. Clarifying Life Lost Due to Cold and Heat: A New Approach Using Annual Time Series. BMJ Open 2015, 5, e005640. [Google Scholar] [CrossRef]
- Hyndman, R.J.; Khandakar, Y. Automatic Time Series Forecasting: The Forecast Package for R. J. Stat. Softw. 2008, 27, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.-C.; Tung, C.C.; Liu, H.H. The Empirical Mode Decomposition and the Hilbert Spectrum for Nonlinear and Non-Stationary Time Series Analysis. Proc. R. Soc. Lond. Ser. A Math. Phys. Eng. Sci. 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Huang, N.E.; Shen, Z.; Long, S.R. A New View of Nonlinear Water Waves: The Hilbert Spectrum1. Annu. Rev. Fluid Mech. 1999, 31, 417–457. [Google Scholar] [CrossRef] [Green Version]
- Rehman, N.U.; Park, C.; Huang, N.E.; Mandic, D.P. EMD Via MEMD: Multivariate Noise-Aided Computation of Standard EMD. Adv. Adapt. Data Anal. 2013, 5, 1350007. [Google Scholar] [CrossRef] [Green Version]
- Masselot, P.; Chebana, F.; Bélanger, D.; St-Hilaire, A.; Abdous, B.; Gosselin, P.; Ouarda, T.B.M.J. EMD-Regression for Modelling Multi-Scale Relationships, and Application to Weather-Related Cardiovascular Mortality. Sci. Total Environ. 2018, 612, 1018–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.C.; Tsai, S.-J.; Huang, N.E. Decomposing the Association of Completed Suicide with Air Pollution, Weather, and Unemployment Data at Different Time Scales. J. Affect. Disord. 2011, 129, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Ma, S.; Lin, J.-C.; Shia, B.-C. Lasso Regression Based on Empirical Mode Decomposition. Commun. Stat. Simul. Comput. 2016, 45, 1281–1294. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Tobias, A.; Zanobetti, A.; Schwartz, J.D.; Leone, M.; Michelozzi, P.; Kan, H.; et al. Changes in Susceptibility to Heat During the Summer: A Multicountry Analysis. Am. J. Epidemiol. 2016, 183, 1027–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Nordio, F.; Zanobetti, A.; Kinney, P.; Vautard, R.; Schwartz, J. Acclimatization across Space and Time in the Effect of Temperature on Mortality: A Time-Series Analysis. Environ. Health 2014, 13, 89–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, J.O.; Silverman, B.W. Functional Data Analysis, 2nd ed.; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- Masselot, P.; Chebana, F.; Ouarda, T.B.M.J.; Bélanger, D.; St-Hilaire, A.; Gosselin, P. A New Look at Weather-Related Health Impacts through Functional Regression. Sci. Rep. 2018, 8, 15241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfait, N.; Ramsay, J.O. The Historical Functional Linear Model. Can. J. Stat. 2003, 31, 115–128. [Google Scholar] [CrossRef]
- Brockhaus, S.; Melcher, M.; Leisch, F.; Greven, S. Boosting Flexible Functional Regression Models with a High Number of Functional Historical Effects. Stat. Comput. 2017, 27, 913–926. [Google Scholar] [CrossRef]
- Bühlmann, P.; Hothorn, T. Boosting Algorithms: Regularization, Prediction and Model Fitting. Stat. Sci. 2007, 22, 477–505. [Google Scholar]
- Arisido, M.W. Functional Measure of Ozone Exposure to Model Short-Term Health Effects. Environmetrics 2016, 27, 306–317. [Google Scholar] [CrossRef]
- Morris, J.S. Functional Regression. Annu. Rev. Stat. Its Appl. 2015, 2, 321–359. [Google Scholar] [CrossRef]
- Brockhaus, S.; Scheipl, F.; Hothorn, T.; Greven, S. The Functional Linear Array Model. Stat. Model. 2015, 15, 279–300. [Google Scholar] [CrossRef] [Green Version]
- Racine, J. Consistent Cross-Validatory Model-Selection for Dependent Data: Hv-Block Cross-Validation. J. Econom. 2000, 99, 39–61. [Google Scholar] [CrossRef]
- Cleveland, W.S.; Devlin, S.J. Locally Weighted Regression: An Approach to Regression Analysis by Local Fitting. J. Am. Stat. Assoc. 1988, 83, 596–610. [Google Scholar] [CrossRef]
- Bustinza, R.; Lebel, G.; Gosselin, P.; Belanger, D.; Chebana, F. Health Impacts of the July 2010 Heat Wave in Quebec, Canada. BMC Public Health 2013, 13, 56. [Google Scholar] [CrossRef] [Green Version]
- Ouarda, T.B.M.J.; Charron, C. Nonstationary Temperature-Duration-Frequency Curves. Sci. Rep. 2018, 8, 15493. [Google Scholar] [CrossRef]
- Sera, F.; Hashizume, M.; Honda, Y.; Lavigne, E.; Schwartz, J.; Zanobetti, A.; Tobias, A.; Iñiguez, C.; Vicedo-Cabrera, A.M.; Blangiardo, M.; et al. Air Conditioning and Heat-Related Mortality: A Multi-Country Longitudinal Study. Epidemiology 2020, 31, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D.; Ebi, K.L.; Forsberg, B. Heatwave Early Warning Systems and Adaptation Advice to Reduce Human Health Consequences of Heatwaves. Int. J. Environ. Res. Public Health 2011, 8, 4623. [Google Scholar] [CrossRef] [Green Version]
- Chebana, F.; Martel, B.; Gosselin, P.; Giroux, J.-X.; Ouarda, T.B. A General and Flexible Methodology to Define Thresholds for Heat Health Watch and Warning Systems, Applied to the Province of Québec (Canada). Int. J. Biometeorol. 2013, 57, 631–644. [Google Scholar] [CrossRef] [PubMed]
- Cardot, H.; Ferraty, F.; Sarda, P. Functional Linear Model. Stat. Probab. Lett. 1999, 45, 11–22. [Google Scholar] [CrossRef]
- McLean, M.W.; Hooker, G.; Staicu, A.-M.; Scheipl, F.; Ruppert, D. Functional Generalized Additive Models. J. Comput. Graph. Stat. 2014, 23, 249–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Illustration | ||||
|---|---|---|---|---|
| Strategy | Description | Objectives | Health Response | Weather Exposure |
| AG | Aggregated response |
|  |  |
| EMDR | EMD-regression |
|  |  |
| FY | Functional regression at the yearly level |
|  |  |
| FD | Functional regression at the daily level |
|  |  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masselot, P.; Chebana, F.; Ouarda, T.B.M.J.; Bélanger, D.; Gosselin, P. Data-Enhancement Strategies in Weather-Related Health Studies. Int. J. Environ. Res. Public Health 2022, 19, 906. https://doi.org/10.3390/ijerph19020906
Masselot P, Chebana F, Ouarda TBMJ, Bélanger D, Gosselin P. Data-Enhancement Strategies in Weather-Related Health Studies. International Journal of Environmental Research and Public Health. 2022; 19(2):906. https://doi.org/10.3390/ijerph19020906
Chicago/Turabian StyleMasselot, Pierre, Fateh Chebana, Taha B. M. J. Ouarda, Diane Bélanger, and Pierre Gosselin. 2022. "Data-Enhancement Strategies in Weather-Related Health Studies" International Journal of Environmental Research and Public Health 19, no. 2: 906. https://doi.org/10.3390/ijerph19020906