
The Use of Lean Six Sigma Methodology in the Reduction of Patient Length of Stay Following Anterior Cruciate Ligament Reconstruction Surgery

 , , and
, , and
Abstract
:1. Introduction
1.1. Background
- -
- To reduce the length of stay of ACLR patients by 80% within 9 months of this improvement project start date, thereby improving patient flow and bed occupancy in the hospital.
- -
- To use an LSS approach to reduce any non-value added in the patient’s pathway, while ensuring that this had no negative impact on patient experience of care or post-operative outcomes.
1.2. Lean Six Sigma
2. Methods
2.1. Project Team
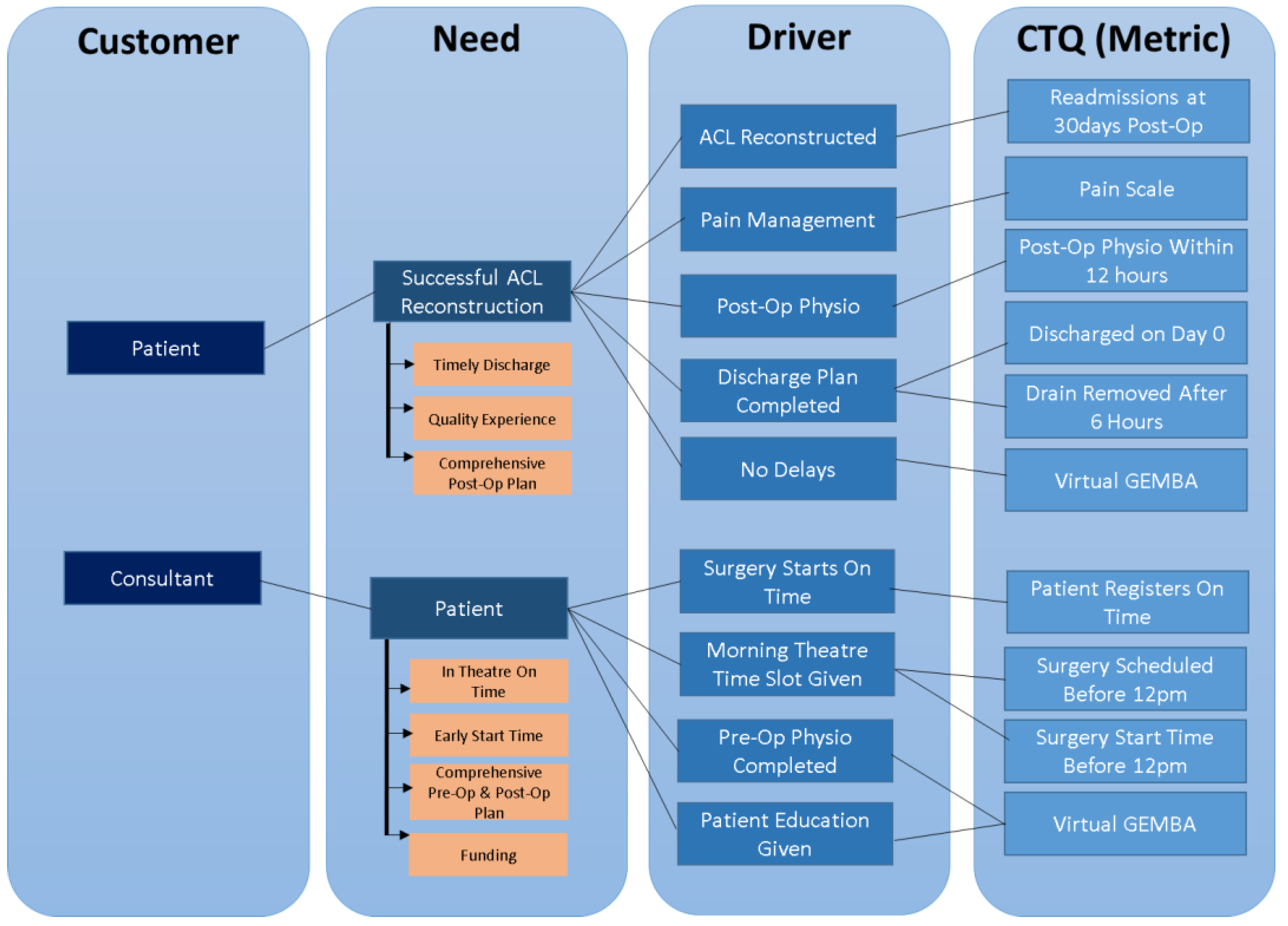
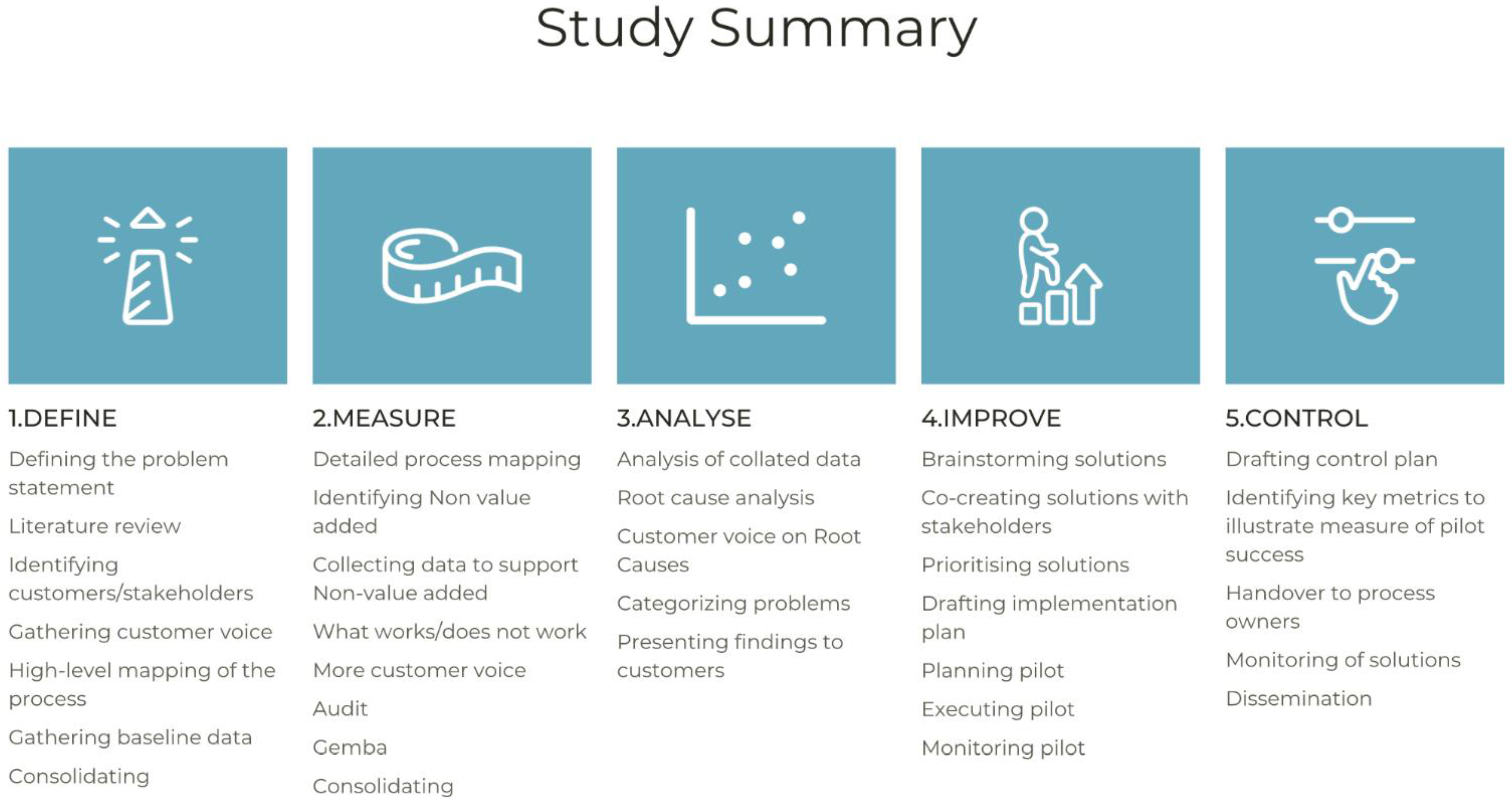
2.2. Define Phase
- Identify the needs of the customer (e.g., patients, staff, and family).
- Identify what drivers the organisation should have in place to meet these needs.
- Identify the metrics to ensure that this driver is meeting the need.
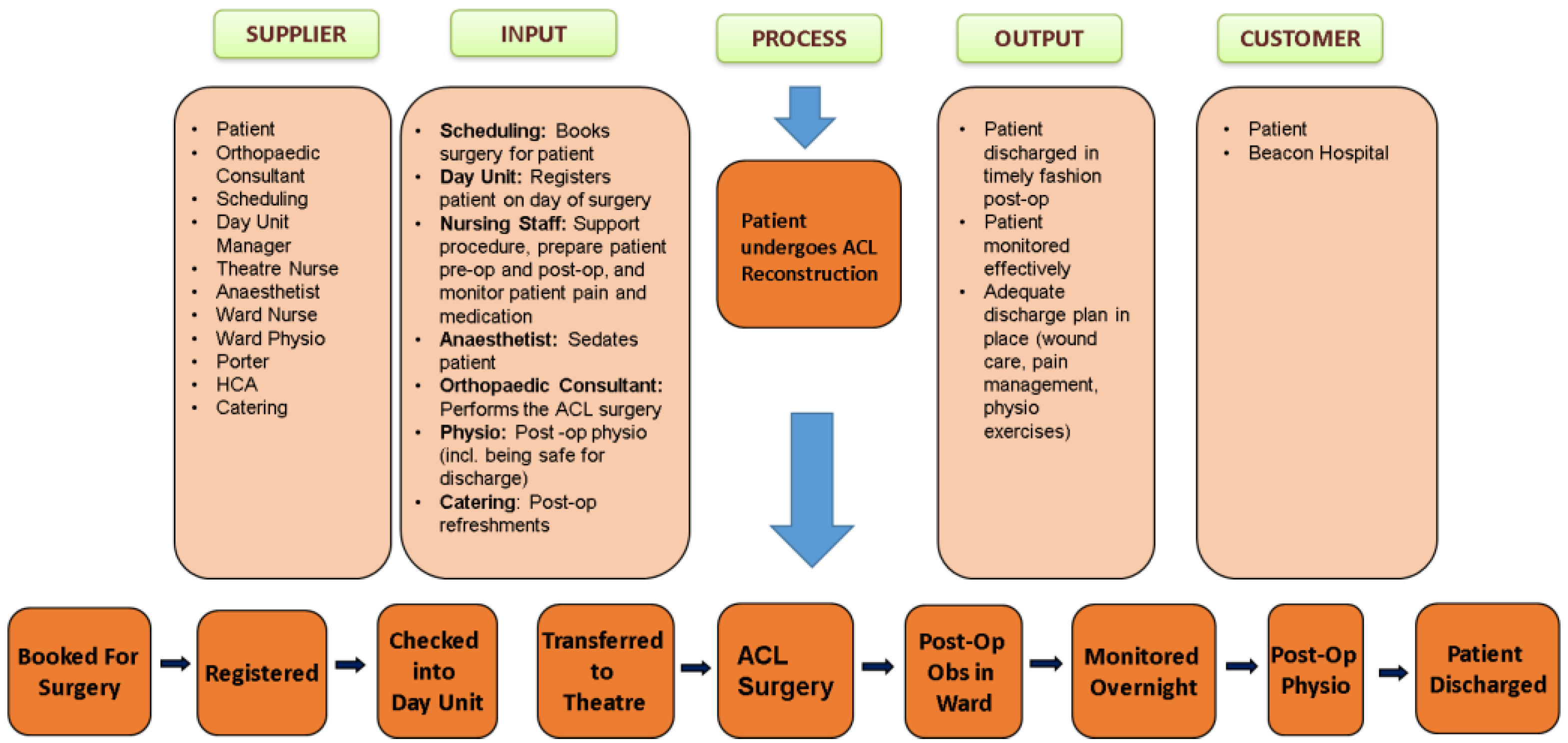
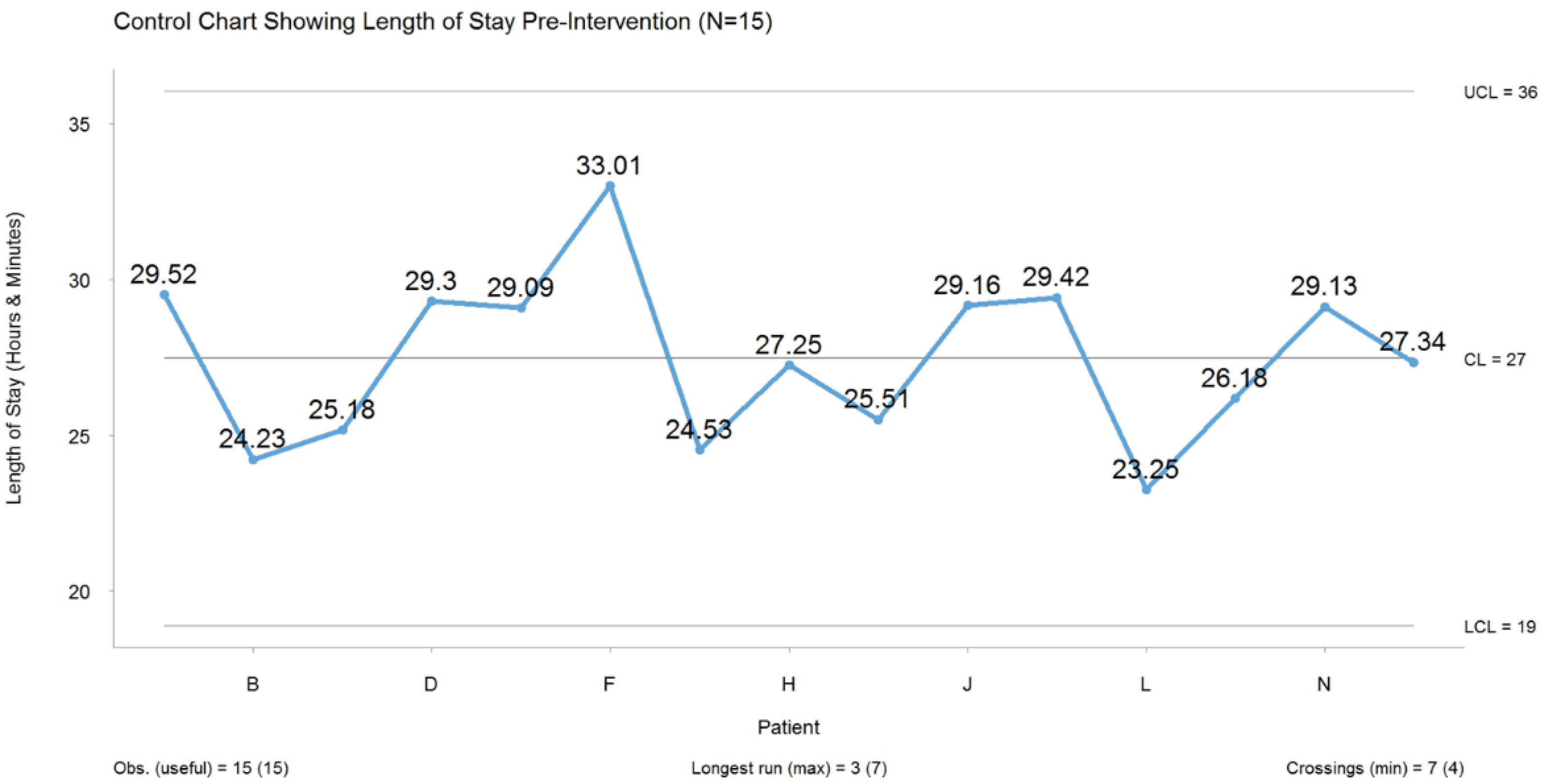
2.3. Measure Phase
- Length of stay from when the patient arrives in the day unit until they are discharged home.
- Number of anterior cruciate ligament procedures performed from April 2019 to October 2019.
- Hospital occupancy, measured monthly from project start in December 2018.
- Pain score, measured hourly.
- Length of time the drain is in situ.
- Thirty-day re-admissions.
- Any delays that occurred were documented.
- Time of post-operative physiotherapy.
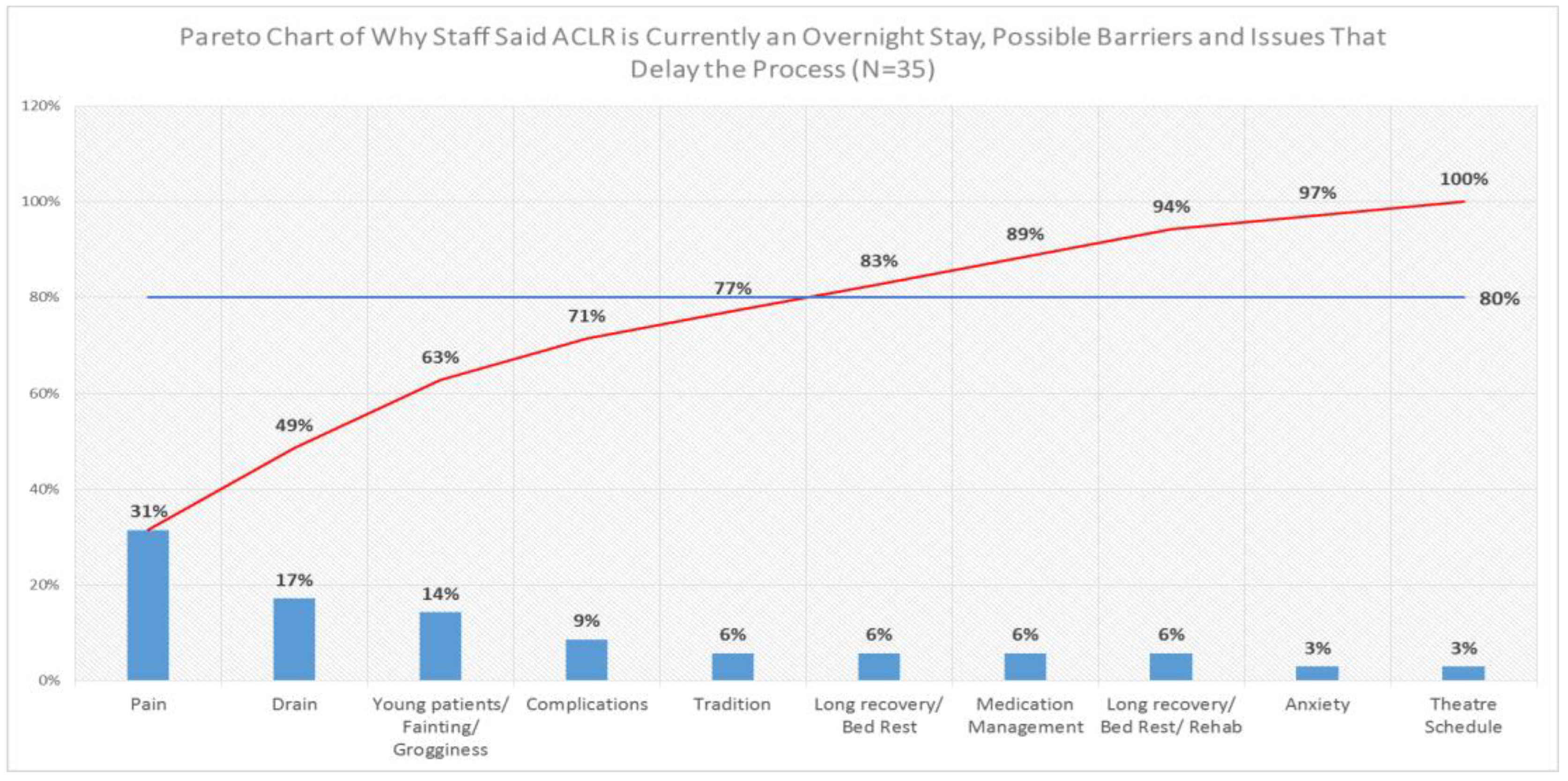
2.4. Analyse Phase
2.5. Improve Phase
- Inform stakeholders of pre-intervention ‘As Is’ situation.
- Discuss with the operating room scheduling team (this is the team that schedules the patient’s slot in theatre after the consultant has booked them in for the surgery) having ACLR patients first on the operative list for surgery.
- Pre-operative physiotherapy to be initiated and consultant to inform the patient of day-case status.
- Patient to be booked by the consultant as normal, but, in this instance, is scheduled as a day-case procedure (as opposed to an overnight stay, provided that the patient meets all inclusion criteria mentioned above).
- Verify with scheduling and billing about the change of patient status from an inpatient to a day-case procedure.
- Liaise with ward managers and bed managers as to recovery on the ward as opposed to the day unit.
- Reminder emails with audit attached to be sent to all relevant stakeholders 2 days pre-surgery.
- LSS team rota to be established for the day of surgery to assist staff with data collection.
- Collect the audit form on the morning after discharge, and discuss any issues that may have arisen with the ward manager.
- Analyse audit data.
3. Results
Control Phase
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Granan, L.P.; Forssbald, M.; Lind, M.; Engerbretsen, L. The Scandinavian ACL registries. 2004–2007 baseline epidemiology. Acta Orthop. 2009, 80, 563–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, J.; Martin, S.; Niagara, C.; Singer, G.A. Comparison of outpatient and inpatient anterior cruciate ligament reconstruction surgery. Arthroscopy 1995, 11, 151–156. [Google Scholar] [CrossRef]
- Jameson, S.S.; Dowen, D.; James, P.; Serrano-Pedraza, I.; Reed, M.R.; Deehan, D. Complications following anterior cruciate ligament reconstruction in the English NHS. Knee 2012, 19, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucocq, J.; Khalil, M.; Roberts, L.; Dalgleish, S.; Jariwala, A. Improving day surgery rates of anterior cruciate ligament reconstruction in surgical units not dedicated to performing day surgery: A retrospective observational cohort study. J. Eval. Clin. Pract. 2021, 27, 1321–1325. [Google Scholar] [CrossRef]
- Lutz, C.; Baverel, L.; Colombet, P.; Cournapeau, J.; Potel, J.-F.; Roussignol, X.; Cucurulo, T.; Servien, E. Pain after out-patient vs. in-patient ACL reconstruction: French prospective study of 1076 patients. Orthop. Traumatol. Surg. Res. 2016, 102, 265–270. [Google Scholar] [CrossRef]
- British Association of Day Surgery. Directory of Procedures, 5th ed.; British Association of Day Surgery: London, UK, 2016. [Google Scholar]
- Daly, A.; Teeling, S.P.; Ward, M.; McNamara, M.; Robinson, C. The Use of Lean Six Sigma for Improving Availability of and Access to Emergency Department Data to Facilitate Patient Flow. Int. J. Environ. Res. Public Health 2021, 18, 11030. [Google Scholar] [CrossRef]
- Poksinska, N.B.; Fialkowska-Filipek, M.; Engstrom, J. Does Lean healthcare improve patient satisfaction? A mixed-method investigation into primary care. BMJ 2016, 26, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Namara, M.; Teeling, S.P. Developing a university-accredited Lean Six Sigma curriculum to overcome system blindness. IJQHC 2019, 31, 3–5. [Google Scholar]
- Lawal, A.K.; Rotter, T.; Kinsman, L.; Sari, N.; Harrison, L.; Jeffery, C.; Kutz, M.; Khan, M.F.; Flynn, R. Lean management in health care: Definition, concepts, methodology and effects reported (systematic review protocol). Syst. Rev. 2014, 3, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Tolga, T.M.; Sezen, B.; Antony, J. An overview of six sigma applications in the healthcare industry. Int. J. Health Care Qual. Assur. 2007, 20, 329–340. [Google Scholar] [CrossRef]
- De Souza, L. Trends and approaches in Lean healthcare leadership. Leadersh. Healthc. 2009, 22, 121–139. [Google Scholar] [CrossRef]
- Dinesh, T.A.; Singh, S.; Nair, P.; Remya, T.R. Reducing waiting time in outpatient services of Large University Teaching Hospital—A six Sigma approach. Manag. Health 2013, 17, 31–37. [Google Scholar]
- George, M.L. Lean Six Sigma—Combining Six Sigma Quality with Lean Speed; McGraw-Hill: New York, NY, USA, 2002. [Google Scholar]
- Snee, R.D. Lean Six Sigma—Getting better all the time. Int. J. Lean Six Sigma 2010, 1, 9–29. [Google Scholar] [CrossRef]
- Deblois, S.; Lepanto, L. Lean and Six Sigma in acute care: A systematic review of reviews. Int. J. Health Care Qual. Assur. 2016, 29, 192–208. [Google Scholar] [CrossRef] [PubMed]
- Jiju, A. The Ten Commandments of Lean Six Sigma: A Guide for Practitioners; Emeral Publishing Limited: Bingley, UK, 2019. [Google Scholar]
- Connolly, K.; Teeling, S.P.; Mc Namara, M. Live well after stroke. Int. Pract. Dev. J. 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Improta, G.; Balto, G.; Ricciardi, C.; Russo, M.A.; Santalucia, I.; Triassi, M.; Cesarelli, M. Lean Six Sigma in Healthcare: Fast track surgery for patients undergoing prosthetic hip replacement surgery. TQM J. 2019, 31, 526–540. [Google Scholar] [CrossRef]
- Improta, G.; Balto, G.; Romano, M.; Carpentieri, F.; Bifulco, P.; Russo, M.A.; Rosa, D.; Triassi, M.; Cesarelli, M. Lean Six Sigma: A new approach to the management of patients undergoing prosthetic hip replacement surgery. J Eval. Clin. Pract. 2015, 21, 662–672. [Google Scholar] [CrossRef]
- Mason, S.E.; Nickolay, C.R.; Darzi, A. The use of Lean and Six Sigma methodologies in surgery: A systematic review. Surgeon 2015, 13, 91–100. [Google Scholar] [CrossRef]
- Murphy, C.; Mullen, E.; Hogan, K.; O’Toole, R.; Teeling, S.P. Streamlining an existing hip fracture patient pathway in an acute tertiary adult Irish hospital to improve patient experience and outcomes. Int. J. Qual. Health Care 2019, 31, 45–51. [Google Scholar] [CrossRef]
- Cima, R.R.; Brown, M.J.; Hebl, J.R.; Moore, R.; Rogers, J.C.; Kollengode, A.; Amstutz, G.J.; Weisbrod, C.A.; Narr, B.J.; Deschamps, C. Use of Lean and Six Sigma Methodology to Improve Operating Room Efficiency in a High-Volume Tertiary-Care Academic Medical Center. J. Am. Coll. Surg. 2011, 213, 83–92. [Google Scholar] [CrossRef]
- Brown, R.; Grehan, P.; Brennan, M.; Carter, D.; Brady, A.; Moore, E.; Teeling, S.P.; Ward, M.; Eaton, D. Using Lean Six Sigma to improve rates of day of surgery admission in a national thoracic surgery department. Int, J. Qual. Health Care 2019, 31 (Suppl. 1), 14–21. [Google Scholar] [CrossRef] [PubMed]
- Furter, S. Applying Lean Six Sigma methods to reduce the length of stay in a hospital’s emergency department. Qual. Eng. 2018, 30, 389–404. [Google Scholar] [CrossRef]
- Daly, A.; Wolfe, N.; Teeling, S.P.; Ward, M.; McNamara, M. Redesigning the Process for Scheduling Elective Orthopaedic Surgery: A Combined Lean Six Sigma and Person-Centred Approach. Int. J. Environ. Res. Public Health 2021, 18, 11946. [Google Scholar] [CrossRef] [PubMed]
- Egan, P.; Pierce, A.; Flynn, A.; Teeling, S.P.; Ward, M.; McNamara, M. Releasing Operating Room Nursing Time to Care through the Reduction of Surgical Case Preparation Time: A Lean Six Sigma Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 12098. [Google Scholar] [CrossRef]
- O’ Mahony, L.; McCarthy, K.; O’Donoghue, J.; Teeling, S.P.; Ward, M.; McNamara, M. Using Lean Six Sigma to Redesign the Supply Chain to the Operating Room Department of a Private Hospital to Reduce Associated Costs and Release Nursing Time to Care. Int. J. Environ. Res. Public Health 2021, 18, 11011. [Google Scholar] [CrossRef]
- Teeling, S.P.; Dewing, J.; Baldie, D. A discussion of the synergy and divergence between Lean Six Sigma and person-centred improvement sciences. Int. J. Res. Nurs. 2020, 11, 10–23. [Google Scholar] [CrossRef] [Green Version]
- Teeling, S.P.; Dewing, J.; Baldie, D. A realist inquiry to identify the contributions of Lean Six Sigma to person-centred care and cultures. Int. J. Environ. Res. Public Health 2021, 18, 10427. [Google Scholar] [CrossRef]
- Dempsey, A.; Robinson, C.; Moffatt, N.; Hennessy, T.; Bradshaw, A.; Teeling, S.P.; Ward, M.; McNamara, M. Lean Six Sigma Redesign of a Process for Healthcare Mandatory Education in Basic Life Support—A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 11653. [Google Scholar] [CrossRef]
- Wolfe, N.; Teeling, S.P.; Ward, M.; McNamara, M.; Koshy, L. Operation Note Transformation: The Application of Lean Six Sigma to Improve the Process of Documenting the Operation Note in a Private Hospital Setting. Int. J. Environ. Res. Public Health 2021, 18, 12217. [Google Scholar] [CrossRef]
- Haynes, R.B. Clinical Epidemiology: How to Do Clinical Practice Research; LWW: Philadelphia, PA, USA, 2012. [Google Scholar]
- Thiese, M.S. Observational and interventional study design types; an overview. Biochem. Medica 2014, 24, 199–210. [Google Scholar] [CrossRef]
- Portela, M.C.; Pronovost, P.J.; Woodcock, T.; Carter, P.; Dixon-Woods, M. How to Study Improvement Interventions: A Brief Overview of Possible Study types BMJ. BMJ Qual. Saf. 2015, 24, 325–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teeling, S.P.; Coetzee, H.; Phillips, M.; McKiernan, M.; Ní ShÉ, É.; Igoe, A. Reducing Risk of Development or Exacerbation of Nutritional Deficits by Optimizing Patient Access to Mealtime Assistance. Int. J. Qual. Health Care 2019, 31 (Suppl. 1), 6–13. [Google Scholar] [CrossRef] [PubMed]
- Antony, J.; Bhuller, A.S.; Maneesh Kumar, M.; Kepa Mendibil, K.; Montgomery, D.C. Application of Six Sigma DMAIC methodology in a transactional environment. Int. J. Qual. Reliab. Manag. 2012, 29, 31–53. [Google Scholar] [CrossRef]
- Scala, A.; Ponsiglione, A.M.; Loperto, I.; Vecchia, A.D.; Borcelli, A.; Russo, G.; Triassi, M.; Improta, G. Lean Six Sigma Approach for Reducing Length of Stay for Patients with Femur Fracture in a University Hospital. Int. J. Environ. Res. Public Health 2021, 18, 2843. [Google Scholar] [CrossRef] [PubMed]
- George, A. Application of Six Sigma DMAIC Methodology to Reduce Medication Errors in a Major Trauma Care Centre in India. Indian J. Pharm. Pract. 2018, 11, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Mahesh, B.P.; Soragaon, B.; Annigeri, A.R. Reduction of patient Wait Time at a Multi-Specialty Hospital Using DMAIC Methodology and Factor Analysis. Int. J. Eng. Technol. 2018, 7, 309–312. [Google Scholar]
- Improta, G.; Balato, G.; Romano, M.; Ponsiglione, A.M.; Raiola, E.; Russo, M.A.; Curraco, P.; Santillo, L.C.; Cesarelli, M. Improving Performances of the Knee Replacement Surgery Process by applying DMAIC Principles. J. Eval. Clin. Pract. 2017, 23, 1401–1407. [Google Scholar] [CrossRef]
- Ward, M.E.; Daly, A.; McNamara, M.; Garvey, S.; Teeling, S.P. A Case Study of a Whole System Approach to Improvement in an Acute Hospital Setting. Int. J. Environ. Res. Public Health 2022, 19, 1246. [Google Scholar] [CrossRef]
- Reid, D.B. From lean modules to a lean mindset. Ind. Syst. Eng. Work 2019, 51, 28–33. [Google Scholar]
- Taghizadegan, S. Mastering Lean Six Sigma: Advanced Black Belt Concepts; Momentum Press: New York, NY, USA, 2013. [Google Scholar]
- Elias, A.A. Stakeholder analysis for Lean Six Sigma project management. Int. J. Lean Six Sigma 2016, 7, 394–405. [Google Scholar] [CrossRef]
- McCormack, B.; Borg, M.; Cardiff, S.; Dewing, J.; Jacobs, G.; Janes, N.; Karlsson, B.; McCance, T.; Mekki, T.; Porock, D.; et al. Person-centeredness—The ‘state’ of the art. Int. Pract. Dev. J. 2015, 5, 1–15. [Google Scholar]
- Found, P.; Harrison, R. Understanding the lean voice of the customer. Int. J. Lean Six Sigma 2012, 3, 251–267. [Google Scholar] [CrossRef]
- Donegan, D.; Teeling, S.P.; McNamara, M.; McAweeney, E.; McGrory, L.; Mooney, R. Calling time on the ‘dance of the blind reflex’: How collaborative working reduced older persons’ length of stay in acute care and increased home discharge. Int. Pract. J. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Carli, F.; Zavorsky, G.S. Optimizing functional exercise capacity in the elderly surgical population. Curr. Opin. Clin. Nutr. Metab. Care. 2005, 8, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.W.G.; Smith, C.; Ilo, K.; Beavs, S.; Terry, L.; Ali, F.; Chandrasenan, J. Dedicated peri-operative pathway improved day-case discharge rate for anterior cruciate ligament reconstructions. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 639–644. [Google Scholar] [CrossRef]
- Moyer, R.; Ikert, K.; Long, K.; Marsh, J. The value of preoperative exercise and education for patients undergoing total hip and knee arthroplasty: A systematic review and meta-analysis. J. Bone Jt. Surg. Rev. 2017, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Ditmyer, M.M.; Tropp, R.; Pifer, M. Prehabilitation in preparation for orthopaedic surgery. Orthop. Nurs. 2002, 21, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Laureani, A.; Brady, M.; Anthony, J. Applications of lean six sigma in an Irish hospital. Leadersh. Health Serv. 2013, 26, 322–337. [Google Scholar] [CrossRef] [Green Version]
- Palmer, B. Making Change Work: Practical Tools for Over-Coming Human Resistance to Change; ASQ Quality Press: Milwaukee, WI, USA, 2003; Volume 1–104. [Google Scholar]
- Stamatis, D.H. Essentials for the Improvement of Healthcare Using Lean & Six Sigma; ProQuest (Firm) & Books 24x7, I; Productivity Press: New York, NY, USA, 2011. [Google Scholar]
- Williams, S.J. Improving Healthcare Operations: The Application of Lean, Agile, and Legality in Care Pathway Design; Palgrave Macmillan: Cham, Switzerland, 2017; Volume 1–136. [Google Scholar]
- George, M.L.; Rowlands, D.; Price, M.; Maxey, J. The Lean Six Sigma Pocket Toolbook; McGraw-Hill: New York, NY, USA, 2005. [Google Scholar]
- Radnor, Z.J.; Holweg, M.; Waring, J. Lean in healthcare: The unfilled promise? Soc. Sci. Med. 2012, 74, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Radziwill, N. Leading and managing the Lean management Process. Qual. Manag. J. 2013, 20, 61–62. [Google Scholar] [CrossRef]
- Cookson, D.; Read, C.; Mukherjee, P.; Cooke, M. Improving the quality of emergency department care by removing waste using lean value stream mapping. Int. J. Clin. Leadersh. 2011, 17, 25–30. [Google Scholar]
- O’Driscoll, S.W.; Kumar, A.; Salter, R.B. The effect of continuous passive motion on the clearance of a haemarthrosis from a synovial joint. An experimental investigation in the rabbit. Clin. Orthop. Relat. Res. 1983, 176, 305–311. [Google Scholar]
- Drehob, P.; Stover, B.H.; Koo, D. On the Road to a Stronger Public Health Workforce: Visual Tools to Address Complex Challenges. Am. J. Prev. Med. 2014, 47 (Suppl. 3), 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beynnon, B.D.; Johnson, R.J.; Abate, J.A.; Fleming, B.C.; Nichols, C.E. Treatment of Anterior Cruciate Ligament Injuries, Part 2. Am. J. Sports Med. 2005, 33, 1751–1767. [Google Scholar] [CrossRef]
- Smith, I.; Cooke, T.; Jackson, L.; Fitzpatrick, R. Rising to the challenge of achieving day surgery targets. Anaesthesia 2006, 61, 1191–1199. [Google Scholar] [CrossRef]
- Krywulak, S.A.; Mohtadi, N.G.; Russell, M.L.; Sasyniuk, T.M. Patient satisfaction with inpatient versus outpatient reconstruction of the anterior cruciate ligament: A randomized clinical trial. Can. J. Surg. 2005, 48, 201–205. [Google Scholar]
- Clayton, R.A.; Court-Brown, C.M. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury 2008, 39, 1338–1344. [Google Scholar] [CrossRef]
- Khan, T.; Jackson, W.F.; Beard, D.J.; Martin, A.; Ahmad, M.; Spacie, R.; Jones, R.; Howes, S.; Barker, K.; Price, A.J. The use of standard operating procedures in day-case anterior cruciate ligament reconstruction. Knee 2012, 19, 464–468. [Google Scholar] [CrossRef]
- Lefevre, N.; Bohu, Y.; De Pamphilis, O.; Klouche, S.; Devaux, C.; Herman, S. Outpatient surgery feasibility in anterior cruciate ligament reconstruction: A prospective comparative assessment. Orthop. Traumatol. Surg. Res. 2014, 100, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Johns, W.L.; Walley, K.C.; Hammoud, S.; Gonzalez, T.A.; Ciccotti, M.G.; Patel, N.K. Tranexamic Acid in Anterior Cruciate Ligament Reconstruction. A Systematic Review and Meta-analysis. AJSM 2021, 49, 4030–4041. [Google Scholar] [CrossRef]
- West, M.A.; Lyubovnikova, J. Illusions of team working in health care. J Health Organ. Manag. 2013, 27, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Manley, K.; O’Keefe, H.; Jackson, C.; Pearce, J.; Smith, S. A Shared Purpose Framework to Deliver Person-Centred, Safe and Effective Care: Organizational Transformation Using Practice Development Methodology. Int. Pract. Dev. J. 2014, 4, 1–31. [Google Scholar] [CrossRef]
- Honda, A.C.; Bernardo, V.Z.; Gerolamo, M.C.; Davis, M.M. How lean Six Sigma principles Improve Hospital Performance. Qual. Manag. J. 2018, 25, 70–82. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistical Test | Pre-Intervention | Post-Intervention |
|---|---|---|
| Average Length of Stay | ||
| Shapiro–Wilk Normality Test | 0.6 | 0.2 |
| Mean LOS | 27.7 | 12.3 |
| Median LOS | 27.6 | 11.7 |
| SD LOS | 2.6 | 1.7 |
| Welch Two Sample t-Test | 6.197 × 10−16 *** | |
| Average Pain Score | ||
| Mean Pain After Surgery | 4 | 0 |
| SD Pain After Surgery | 2.4 | 1.9 |
| Mean Pain At discharge | 2.5 | 3 |
| SD Pain At Discharge | 1.4 | 2.1 |
| Welch Two Sample t-Test (after surgery) | 0.18 | |
| Welch Two Sample t-Test (at discharge) | 0.65 | |
| Average Length of Time Drain In Situ | ||
| Mean Drain | 21.9 | 7.4 |
| Median Drain | 21.7 | 7.3 |
| SD Drain | 2.8 | 1.3 |
| Welch Two Sample t-Test | 1.062 × 10−6 *** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moffatt, S.; Garry, C.; McCann, H.; Teeling, S.P.; Ward, M.; McNamara, M. The Use of Lean Six Sigma Methodology in the Reduction of Patient Length of Stay Following Anterior Cruciate Ligament Reconstruction Surgery. Int. J. Environ. Res. Public Health 2022, 19, 1588. https://doi.org/10.3390/ijerph19031588
Moffatt S, Garry C, McCann H, Teeling SP, Ward M, McNamara M. The Use of Lean Six Sigma Methodology in the Reduction of Patient Length of Stay Following Anterior Cruciate Ligament Reconstruction Surgery. International Journal of Environmental Research and Public Health. 2022; 19(3):1588. https://doi.org/10.3390/ijerph19031588
Chicago/Turabian StyleMoffatt, Sinead, Catherine Garry, Hannah McCann, Sean Paul Teeling, Marie Ward, and Martin McNamara. 2022. "The Use of Lean Six Sigma Methodology in the Reduction of Patient Length of Stay Following Anterior Cruciate Ligament Reconstruction Surgery" International Journal of Environmental Research and Public Health 19, no. 3: 1588. https://doi.org/10.3390/ijerph19031588