
Sick Leave and Intention to Quit the Job among Nursing Staff in German Hospitals during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
1.1. Predictors and Correlates for Sick Leave and Turnover among Nurses
1.2. Focus of the Present Study
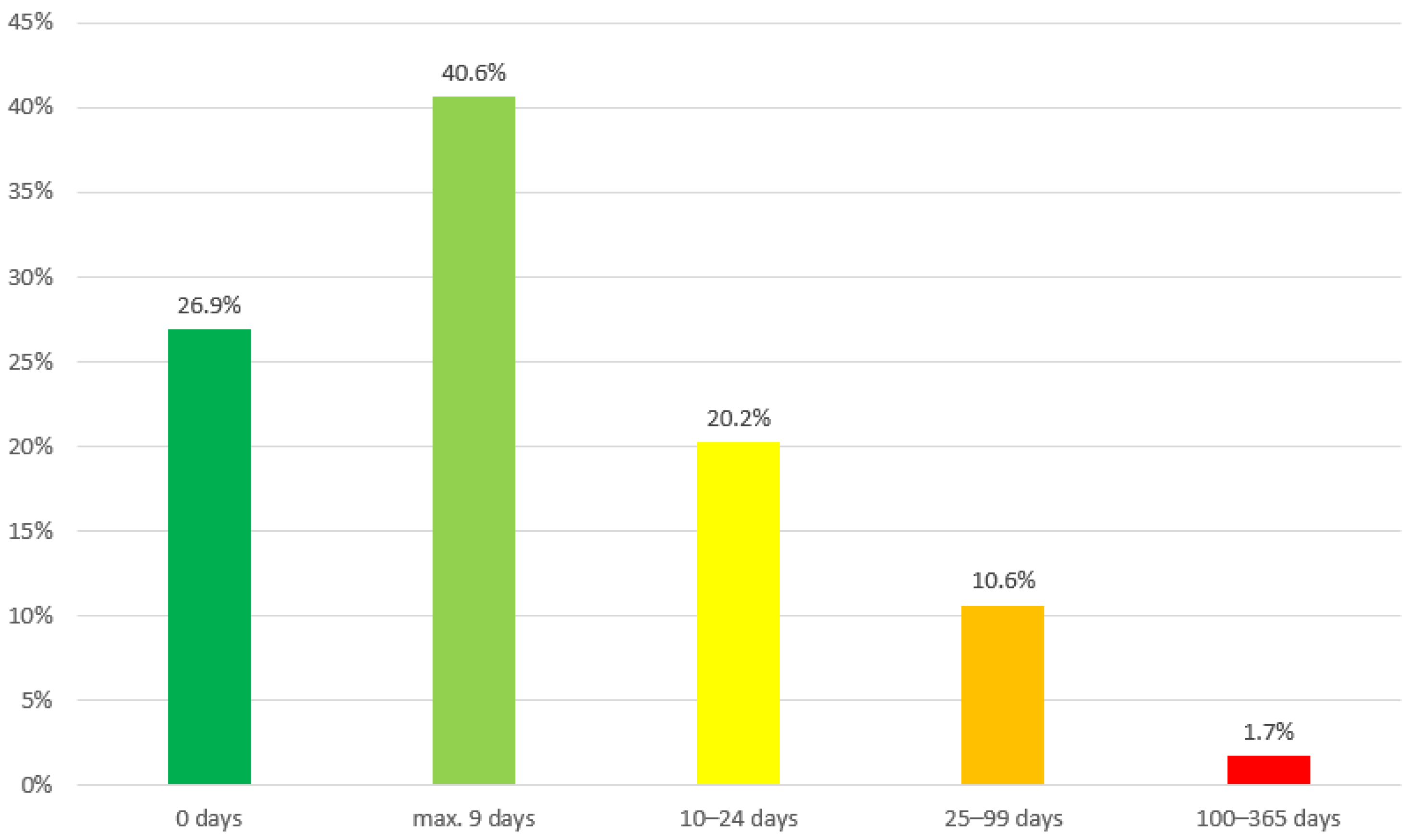
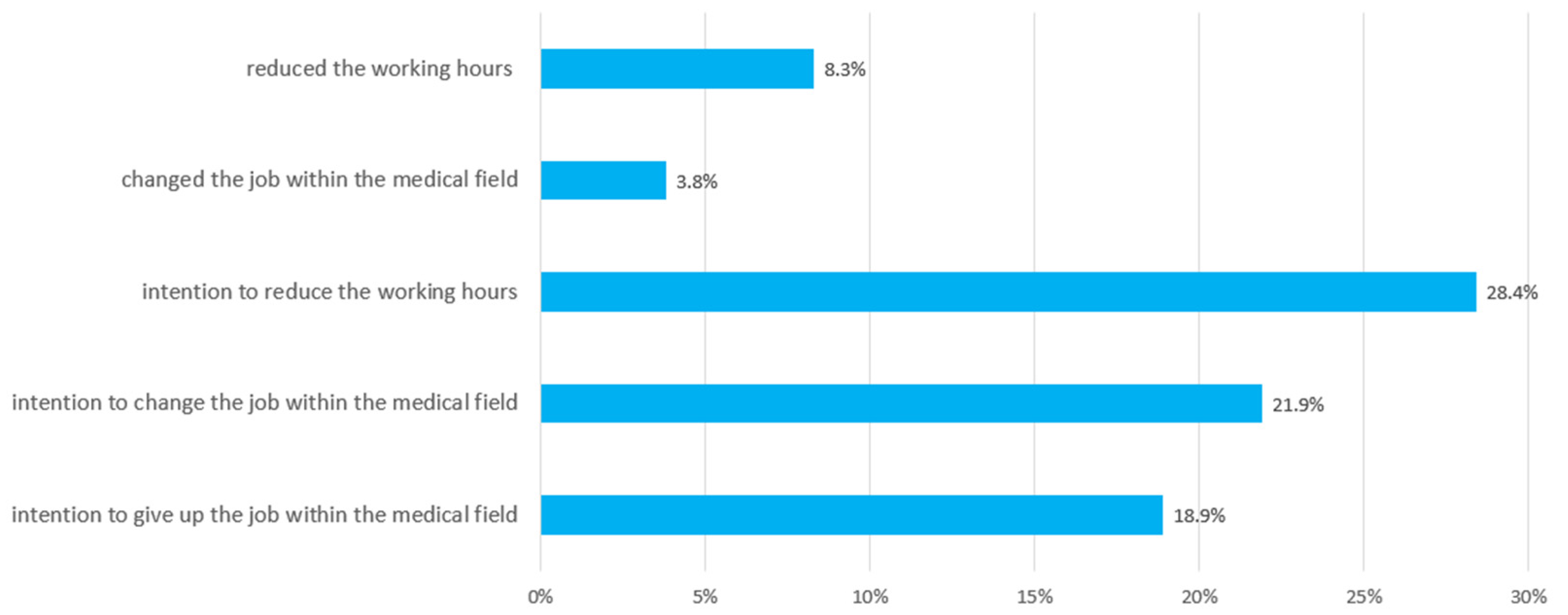
- What is the reported number of sick leave days and the reported intention to leave the job?
- Which sociodemographic, occupational, COVID-19 related, work related and (mental) health related factors are associated with days of sick leave and intention to leave the job among nurses?
2. Materials and Methods
2.1. Data Collection
2.2. Measures
2.2.1. Days of Sick Leave and Turnover Intention
2.2.2. Work-Related Variables
2.2.3. COVID-19 Related Variables
2.2.4. Mental Health Variables and Exhaustion
2.2.5. Sociodemographic and Occupational Variables
2.2.6. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Frequency of Sick Leave and Turnover Intention
3.3. Predictors of Sick Leave and Turnover Intention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gesundheitsberichterstattung des Bundes (Federal Health Reporting). 2021. Available online: https://www.gbe-bund.de/gbe/pkg_isgbe5.prc_menu_olap?p_uid=gast&p_aid=8360653&p_sprache=D&p_help=2&p_indnr=96&p_indsp=&p_ityp=H&p_fid= (accessed on 4 January 2022).
- Seyda, S.; Köppen, R.; Hickmann, H. Pflegeberufe Besonders vom Fachkräftemangel Betroffen (Nursing Professions Particularly Affected by Shortage of Skilled Workers); Kompetenzzentrum Fachkräftesicherung (KOFA) KOMPAKT: Cologne, Germany, 2021. [Google Scholar]
- Radtke, R. Prognostizierter Bedarf an Stationären und Ambulanten Pflegekräften* in Deutschland bis zum Jahr 2035 (Projected demand for inpatient and outpatient nursing staff in Germany up to 2035). 2020. Available online: https://de.statista.com/statistik/daten/studie/172651/umfrage/bedarf-an-pflegekraeften-2025/ (accessed on 4 January 2022).
- Lagerström, M.; Hansson, T.; Hagberg, M. Work-related low-back problems in nursing. Scand. J. Work. Environ. Health 1998, 24, 449–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brusini, A. Low back pain among nurses in Italy: A review. G. Ital. Med. Lav. Ergon. 2021, 43, 369–372. [Google Scholar] [PubMed]
- Alharbi, J.; Jackson, D.; Usher, K. The potential for COVID-19 to contribute to compassion fatigue in critical care nurses. J. Clin. Nurs. 2020, 29, 2762–2764. [Google Scholar] [CrossRef]
- Salmond, E.; Salmond, S.; Ames, M.; Kamienski, M.; Holly, C. Experiences of compassion fatigue in direct care nurses: A qualitative systematic review. JBI Database Syst. Rev. Implement Rep. 2019, 17, 682–753. [Google Scholar] [CrossRef] [PubMed]
- Robert-Koch-Institut. COVID-19: Fallzahlen in Deutschland und weltweit. (COVID-19: Case Numbers in Germany and Worldwide). 2022. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Fallzahlen.html/ (accessed on 4 January 2022).
- Gilan, D.; Röthke, N.; Blessin, M.; Kunzler, A.; Stoffers-Winterling, J.; Müssig, M.; Yuen, K.S.L.; Tüscher, O.; Thrul, J.; Kreuter, F.; et al. Psychische Belastungen, Resilienz, Risiko- und protektive Faktoren während der SARS-CoV-2-Pandemie. (Psychological Stress, Resilience, Risk and Protective Factors During the SARS-CoV-2 Pandemic). Dtsch Arztebl. Int. 2020, 117, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Rahme, D.V.; Razzouk, G.N.; Musharrafieh, U.M.; Rahi, A.C.; Akel, M.M. Sickness-related absence among employees at a tertiary care center in Lebanon. Arch. Environ. Occup. Health 2007, 61, 279–284. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Schröder, H.; Wicker, S.; Janssens, U. COVID-19-Pandemie: Pflegende deutlich häufiger krank (COVID-19 pandemic: Carers significantly more often ill). Dtsch Arztebl. Int. 2021, 118, A-1352. [Google Scholar]
- Techniker Krankenkasse. Fehlzeiten bei Pflegekräften Erneut Gestiegen (Absenteeism among Care Workers Increased Again). 2021. Available online: https://www.tk.de/presse/themen/praevention/gesundheitsstudien/steigende-fehlzeiten-bei-pflegekraeften-2111088?tkcm=ab (accessed on 4 January 2022).
- DAK-Krankenstands-Analyse: Krankheitsgeschehen in der Arbeitswelt Während der Pandemie Massiv Verändert (DAK Sickness Absence Analysis: Sickness Incidence in the World of Work Massively Changed during the Pandemic). 2021. Available online: https://www.dak.de/dak/bundesthemen/krankenstand-2020-2424242.html#/ (accessed on 6 January 2022).
- Gesetz über die Zahlung des Arbeitsentgelts an Feiertagen und im Krankheitsfall (Entgeltfortzahlungsgesetz) (Act on the Payment of Remuneration on Public Holidays and in the Event of Sickness; Continued Remuneration Act). Federal Office of Justice. Available online: https://www.gesetze-im-internet.de/entgfg/BJNR106500994.html (accessed on 7 February 2022).
- Jones, C.B. The costs of nurse turnover: Part 1: An economic perspective. J. Nurs. Adm. 2004, 34, 562–570. [Google Scholar] [CrossRef]
- Sherring, S.; Knight, D. An exploration of burnout among city mental health nurses. Br. J. Nurs. 2009, 18, 1234–1240. [Google Scholar] [CrossRef]
- Daouk-Öyry, L.; Anouze, A.L.; Otaki, F.; Dumit, N.Y.; Osman, I. The JOINT model of nurse absenteeism and turnover: A systematic review. Int. J. Nurs. Stud. 2014, 51, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-C.; Chu, C.-I.; Wang, Y.-H.; Lin, L.-C. Turnover factors revisited: A longitudinal study of Taiwan-based staff nurses. Int. J. Nurs. Stud. 2008, 45, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Nyathi, M.; Jooste, K. Working conditions that contribute to absenteeism among nurses in a provincial hospital in the Limpopo Province. Curationis 2008, 31, 28–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellgren, S.F.; Kajermo, K.N.; Ekvall, G.; Tomson, G. Nursing staff turnover at a Swedish university hospital: An exploratory study. J. Clin. Nurs. 2009, 18, 3181–3189. [Google Scholar] [CrossRef]
- Webster, J.; Flint, A.; Courtney, M. A new practice environment measure based on the reality and experiences of nurses working lives. J. Nurs. Manag. 2009, 17, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Josephson, M.; Lindberg, P.; Voss, M.; Alfredsson, L.; Vingård, E. The same factors influence job turnover and long spells of sick leave—A 3-year follow-up of Swedish nurses. Eur. J. Public Health 2008, 18, 380–385. [Google Scholar] [CrossRef] [Green Version]
- Karlowicz, K.A.; Ternus, M.P. Issues influencing psychiatric nurse retention during the first year of employment: A case analysis. J. Nurs. Manag. 2009, 17, 49–58. [Google Scholar] [CrossRef]
- Stordeur, S.; D’Hoore, W.; the NEXT-Study Group. Organizational configuration of hospitals succeeding in attracting and retaining nurses. J. Adv. Nurs. 2007, 57, 45–58. [Google Scholar] [CrossRef] [Green Version]
- Schreuder, J.A.H.; Roelen, C.A.M.; Koopmans, P.C.; Moen, B.E.; Groothoff, J.W. Effort-reward imbalance is associated with the frequency of sickness absence among female hospital nurses: A cross-sectional study. Int. J. Nurs. Stud. 2010, 47, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Ge, J.; He, J.; Liu, Y.; Zhang, J.; Pan, J.; Zhang, X.; Liu, D. Effects of effort-reward imbalance, job satisfaction, and work engagement on self-rated health among healthcare workers. BMC Public Health 2021, 21, 195. [Google Scholar] [CrossRef]
- Nilsson, A.; Denison, E.; Lindberg, P. Life values as predictors of pain, disability and sick leave among Swedish registered nurses: A longitudinal study. BMC Nurs. 2011, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.; Tagaya, A.; Ota, K.; Nagasawa, Y.; Matsuura, R.; Sato, C. Factors affecting turnover of Japanese novice nurses in university hospitals in early and later periods of employment. J. Nurs. Manag. 2010, 18, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Gohar, B.; Larivière, M.; Lightfoot, N.; Wenghofer, E.; Larivière, C.; Nowrouzi-Kia, B. Meta-analysis of nursing-related organizational and psychosocial predictors of sickness absence. Occup. Med. 2020, 70, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Fochsen, G.; Josephson, M.; Hagberg, M.; Toomingas, A.; Lagerström, M. Predictors of leaving nursing care: A longitudinal study among Swedish nursing personnel. Occup. Environ. Med. 2006, 63, 198–201. [Google Scholar] [CrossRef] [Green Version]
- Nikkhah-Farkhani, Z.; Piotrowski, A. Nurses’ turnover intention a comparative study between Iran and Poland. Med. Pr. 2020, 71, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; de Los Santos, J.A.A. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 2021, 29, 395–403. [Google Scholar] [CrossRef]
- Morawa, E.; Schug, C.; Geiser, F.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Hiebel, N.; Borho, A.; Erim, Y. Psychosocial burden and working conditions during the COVID-19 pandemic in Germany: The VOICE survey among 3678 health care workers in hospitals. J. Psychosom. Res. 2021, 144, 110415. [Google Scholar] [CrossRef]
- Schug, C.; Erim, Y.; Geiser, F.; Hiebel, N.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Steudte-Schmiedgen, S.; Borho, A.; et al. Vaccination willingness against COVID-19 among healthcare workers in Germany: Results from a University Medicine Network survey between November 2020 and January 2021. Bundesgesundheitsblatt Gesundh. Gesundh. 2022, 65, 74–85. [Google Scholar] [CrossRef]
- Ilmarinen, J. The work ability index (WAI). Occup. Med. 2007, 57, 160. [Google Scholar] [CrossRef] [Green Version]
- Bundesanstalt für Arbeitsschutz und Arbeitsmedizin (German Federal Institute for Occupational Safety and Health). Work Ability Index (WAI). Modifizierte Kurzversion für die Studie zur Mentalen Gesundheit bei der Arbeit (S-MGA); (Modified Short Version for the Study on Mental Health at Work). 2019. Available online: https://www.baua.de/DE/Themen/Arbeit-und-Gesundheit/Psychische-Gesundheit/Mentale-Gesundheit-und-kognitive-Leistungsfaehigkeit/pdf/WAI-Kurzversion.pdf?__blob=publicationFile&v=2 (accessed on 26 January 2022).
- Siegrist, J.; Wege, N.; Pühlhofer, F.; Wahrendorf, M. A short generic measure of work stress in the era of globalization: Effort-reward imbalance. Int. Arch. Occup. Environ. Health 2009, 82, 1005–1013. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Kroenke, K.; Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 2005, 58, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Löwe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt (Federal Statistical Office). Population with migration background—Results of the microcensus 2019—Fachserie 1 Reihe 2.2—2019. 2020. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Publikationen/Downloads-Migration/migrationshintergrund-2010220197004.html (accessed on 28 January 2021).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Baas, J. Gesundheitsreport. Pflegefall Pflegebranche? So Geht’s Deutschlands Pflegekräften. (Health Report. Nursing Case Nursing Sector? This is How Germany’s Care Workers Are Doing.); Techniker-Krankenkasse, Ed.; Techniker Krankenkasse: Hamburg, Germany, 2019. [Google Scholar]
- Tori, K.; Dinh, T.T.H.; Mather, C. Healthcare Professional Presenteeism during a COVID-19 Outbreak in an Australian Rural Healthcare Environment: A Case Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8336. [Google Scholar] [CrossRef]
- Aronsson, G.; Gustafsson, K. Sickness Presenteeism: Prevalence, Attendance-Pressure Factors, and an Outline of a Model for Research. J. Occup. Environ. Med. 2005, 47, 958–966. [Google Scholar] [CrossRef]
- Lo, W.-Y.; Chien, L.-Y.; Hwang, F.-M.; Huang, N.; Chiou, S.-T. From job stress to intention to leave among hospital nurses: A structural equation modelling approach. J. Adv. Nurs. 2018, 74, 677–688. [Google Scholar] [CrossRef]
- Oreg, S.; Vakola, M.; Armenakis, A. Change Recipients’ Reactions to Organizational Change: A 60-Year Review of Quantitative Studies. J. Appl. Behav. Sci. 2011, 47, 461–524. [Google Scholar] [CrossRef]
- Burke, R.J.; Greenglass, E.R. Effects of hospital restructuring on full time and part time nursing staff in Ontario. Int. J. Nurs. Stud. 2000, 37, 163–171. [Google Scholar] [CrossRef]
- Lauchart, M.; Ascher, P.; Kesel, K.; Weber, S.; Grabein, B.; Schneeweiss, B.; Fischer-Truestedt, C.; Schoenberg, M.; Rogler, G.; Borelli, C. Compatibility of Work and Family Life: Survey of Physicians in the Munich Metropolitan Area. Gesundheitswesen 2019, 81, 299–308. [Google Scholar] [CrossRef]
- Rabe, J.E.; Schillok, H.; Merkel, C.; Voss, S.; Coenen, M.; De Bock, F.; von Rüden, U.; Bramesfeld, A.; Jung-Sievers, C. Burden in parents of school-aged children during different phases of the COVID-19 pandemic in Germany: An analysis within the COVID-19 snapshot monitoring (COSMO) study. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 1500–1511. [Google Scholar] [CrossRef]
- Gräske, J.; Forbrig, T.A.; Koppe, L.; Urban, S.; Neumann, F.; Boguth, K. Effort-Reward Imbalance, Ability to Work and the Desire for Career Exits: A Cross-sectional Study of Nurses. Gesundheitswesen 2021. [Google Scholar] [CrossRef]
- Hasselhorn, H.M.; Tackenberg, P.; Peter, R. Effort-reward imbalance among nurses in stable countries and in countries in transition. Int. J. Occup. Environ. Health 2004, 10, 401–408. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Sample N = 757 | Sickness Leave, n (%) (≥10 Days in Last 12 Months) | p-Value, Effect Size | Intention to Leave the Job, n (%) | p-Value, Effect Size | |
|---|---|---|---|---|---|
| Gender, n (%) | 0.239 * (0.043) | 0.247 * (0.042) | |||
| Women | 582 (76.9) | 196 (33.7) | 105 (18.0) | ||
| Men | 173 (22.9) | 50 (28.9) | 38 (22.0) | ||
| Diverse | 2 (0.3) | 0 (0.0) | 0 (0.0) | ||
| Age, years, n (%) | 0.727 (0.042) | 0.010 (0.123) | |||
| 18–30 | 183 (24.2) | 54 (29.5) | 43 (23.5) | ||
| 31–40 | 180 (23.8) | 58 (32.2) | 38 (21.1) | ||
| 41–50 | 158 (20.9) | 52 (32.9) | 34 (21.5) | ||
| >50 | 236 (31.2) | 82 (34.7) | 28 (11.9) | ||
| Living alone, n (%) | 0.772 (0.11) | 0.377 (0.032) | |||
| Yes | 195 (25.8) | 65 (33.3) | 41 (21.0) | ||
| No | 562 (74.2) | 181 (32.2) | 102 (18.1) | ||
| Children, n (%) | 0.489 (0.025) | 0.388 (0.031) | |||
| Yes | 374 (49.4) | 126 (33.7) | 66 (17.6) | ||
| No | 383 (50.6) | 120 (31.3) | 77 (20.1) | ||
| Migration background, n (%) | 0.780 (0.010) | 0.084 (0.063) | |||
| Yes | 99 (13.1) | 31 (31.3) | 25 (25.3) | ||
| No | 657 (86.8) | 215 (32.7) | 118 (18.0) | ||
| Missing | 1 (0.1) | - | - | ||
| Caring for old, ill or disabled relatives, n (%) | 0.364 (0.033) | 0.580 (0.020) | |||
| Yes | 131 (17.3) | 47 (35.9) | 27 (20.6) | ||
| No | 626 (82.7) | 199 (31.8) | 116 (18.5) | ||
| Work setting, n (%) | 0.518 (0.023) | 0.561 (0.021) | |||
| University hospital | 652 (86.1) | 209 (32.1) | 121 (18.6) | ||
| Non-university hospital | 105 (13.9) | 37 (35.2) | 22 (21.0) | ||
| Disciplines, n (%) | 0.281 (0.091) | 0.290 (0.090) | |||
| Surgical ward | 137 (18.1) | 52 (38.0) | 32 (23.4) | ||
| Conservative discipline | 118 (15.6) | 31 (26.3) | 17 (14.4) | ||
| Mixed surgical and conservative discipline | 93 (12.3) | 35 (37.6) | 13 (14.0) | ||
| Psychiatry/psychosomatics | 100 (13.2) | 31 (31.0) | 20 (20.0) | ||
| Intensive/emergency care | 200 (26.4) | 59 (29.5) | 43 (21.5) | ||
| Other | 109 (14.4) | 38 (34.9) | 18 (16.5) | ||
| Working in patient care, n (%) | 0.632 (0.017) | 0.616 (0.018) | |||
| Yes | 719 (95.0) | 235 (32.7) | 137 (19.1) | ||
| No | 38 (5.0) | 11 (28.9) | 6 (15.8) | ||
| Professional experience in patient care | 0.503 (0.044) | 0.021 (0.104) | |||
| <3 years | 32 (4.2) | 12 (37.5) | 12 (37.5) | ||
| 3–6 years | 103 (13.6) | 29 (28.2) | 21 (20.4) | ||
| >6 years | 584 (77.1) | 194 (33.2) | 104 (17.8) | ||
| Missing | 38 (5.0) | - | - | ||
| Employment | 0.398 (0.031) | 0.638 (0.017) | |||
| Full-time | 442 (58.4) | 149 (33.7) | 81 (18.3) | ||
| Part-time | 315 (41.6) | 97 (30.8) | 62 (19.7) |
| Total Sample N = 757 | Sickness Leave, n (%) (≥10 Days in Last 12 Months) | p-Value, Effect Size | Intention to Leave the Job, n (%) | p-Value, Effect Size | |
|---|---|---|---|---|---|
| Infection with SARS-CoV-2 virus, n (%) | <0.001 (0.265) | 0.017 (0.104) | |||
| Yes | 79 (10.4) | 54 (68.4) | 20 (25.3) | ||
| No | 600 (79.3) | 165 (27.5) | 101 (16.8) | ||
| I do not know | 78 (10.3) | 27 (34.6) | 22 (28.2) | ||
| Contact with infected patients, n (%) | 0.117 (0.057) | 0.010 (0.093) | |||
| Yes | 254 (33.6) | 73 (28.7) | 61 (24.0) | ||
| No | 503 (66.4) | 173 (34.4) | 82 (16.3) | ||
| Contact with contaminated material, n (%) | 0.185 (0.048) | 0.010 (0.094) | |||
| Yes | 224 (29.6) | 65 (29.0) | 55 (24.6) | ||
| No | 533 (70.4) | 181(34.0) | 88 (16.5) | ||
| Risk group due to pre-existing illness, n (%) | <0.001 (0.123) | 0.004 (0.104) | |||
| Yes | 147 (19.4) | 65 (44.2) | 40 (27.2) | ||
| No | 610 (80.6) | 181 (29.7) | 103 (16.9) | ||
| Occupancy rate of the wards, n (%) | 0.441 (0.070) | 0.635 (0.056) | |||
| Strongly below average | 17 (2.2) | 9 (52.9) | 4 (23.5) | ||
| Slightly below average | 52 (6.9) | 18 (34.6) | 9 (17.3) | ||
| Average | 227 (30.0) | 74 (32.6) | 36 (15.9) | ||
| Slightly above average | 235 (31.0) | 76 (32.3) | 48 (20.4) | ||
| Strongly above average | 226 (29.9) | 69 (30.5) | 46 (20.4) | ||
| Change of department due to the pandemic, n (%) | 0.799 (0.009) | <0.001 (0.155) | |||
| Yes | 83 (11.0) | 28 (33.7) | 30 (36.1) | ||
| No | 674 (89.0) | 218 (32.3) | 113 (16.8) | ||
| Presently working in home office, n (%) | 0.957 (0.002) | 0.199 (0.051) | |||
| Yes (exclusively/partly) | 25 (3.3) | 8 (32.0) | 2 (8.0) | ||
| No | 732 (96.7) | 238 (32.5) | 141 (19.3) |
| Independent Variable Nagelkerkes R2 = 20.0%; Hosmer-Lemeshow test: χ2 = 5.508; df = 8; p = 0.702; 2-Log-Likelihood = 792.672 | ||||||
|---|---|---|---|---|---|---|
| Regression Coefficient | Standard Error | Wald | df | p-Value | OR (95% CI: Minimum–Maximum) | |
| Sociodemographic variables | ||||||
| Gender (Ref. = men) | ||||||
| Women | 0.119 | 0.223 | 0.284 | 1 | 0.594 | 1.126 (0.727–1.743) |
| Age (Ref. = 18–30 years) | ||||||
| 31–40 | 0.374 | 0.330 | 1.291 | 1 | 0.256 | 1.454 (0.762–2.774) |
| 41–50 | 0.459 | 0.365 | 1.578 | 1 | 0.209 | 1.582 (0.773–3.237) |
| >50 | 0.449 | 0.350 | 1.644 | 1 | 0.200 | 1.566 (0.789–3.109) |
| Living alone (Ref. = No) | ||||||
| Yes | −0.017 | 0.223 | 0.006 | 1 | 0.940 | 0.983 (0.636–1.521) |
| Children (Ref. = No) | ||||||
| Yes | 0.046 | 0.219 | 0.045 | 1 | 0.832 | 1.047 (0.682–1.609) |
| Migration background (Ref. = No) | ||||||
| Yes | −0.009 | 0.265 | 0.001 | 1 | 0.974 | 0.991 (0.590–1.665) |
| Caring for old, ill or disabled relatives (Ref. = No) | ||||||
| Yes | 0.071 | 0.238 | 0.088 | 1 | 0.766 | 1.073 (0.673–1.710) |
| Job—related variables | ||||||
| Professional experience in patient care (Ref. = <3 years) | ||||||
| 3–6 | −0.396 | 0.476 | 0.692 | 1 | 0.405 | 0.673 (0.265–1.710) |
| >6 | −0.322 | 0.481 | 0.448 | 1 | 0.503 | 0.725 (0.282–1.861) |
| Employment (Ref. = Full-time) | ||||||
| Part-time | −0.345 | 0.194 | 3.148 | 1 | 0.076 | 0.709 (0.484–1.037) |
| COVID-19—related variables | ||||||
| Infection with SARS-CoV-2 (Ref. = No) | ||||||
| Yes | 1.929 | 0.286 | 45.520 | 1 | <0.001 | 6.883 (3.930–12.055) |
| I don’t know | 0.402 | 0.279 | 2.072 | 1 | 0.150 | 1.495 (0.865–2.583) |
| Contact with infected patients (Ref. = No) | ||||||
| Yes | −0.453 | 0.197 | 5.286 | 1 | 0.021 | 0.635 (0.432–0.935) |
| Risk group due to pre-existing illness (Ref. = No) | ||||||
| Yes | 0.623 | 0.226 | 7.610 | 1 | 0.006 | 1.864 (1.198–2.903) |
| Occupancy rate (Ref. = strongly/slightly below average, average) | ||||||
| Slightly/strongly above average | −0.271 | 0.206 | 1.727 | 1 | 0.189 | 0.763 (0.510–1.142) |
| Change of the department (Ref. = No) | ||||||
| Yes | −0.033 | 0.287 | 0.013 | 1 | 0.909 | 0.968 (0.551–1.699) |
| Symptoms | ||||||
| PHQ-2 * | −0.004 | 0.083 | 0.002 | 1 | 0.962 | 0.996 (0.846–1.173) |
| GAD-2 * | 0.060 | 0.075 | 0.645 | 1 | 0.422 | 1.062 (0.917–1.231) |
| Sleeping disorders # | −0.103 | 0.082 | 1.580 | 1 | 0.209 | 0.902 (0.768–1.059) |
| Exhaustion # | 0.272 | 0.109 | 6.273 | 1 | 0.012 | 1.313 (1.061–1.624) |
| Fear to become infected # | 0.177 | 0.077 | 5.245 | 1 | 0.022 | 1.194 (1.026–1.389) |
| Work—related variables | ||||||
| ERI effort + | −0.099 | 0.058 | 2.903 | 1 | 0.088 | 0.906 (0.809–1.015) |
| ERI reward + | −0.088 | 0.033 | 7.340 | 1 | 0.007 | 0.915 (0.859–0.976) |
| Trust in colleagues # | 0.187 | 0.094 | 3.911 | 1 | 0.048 | 1.205 (1.002–1.451) |
| Higher workload # | −0.023 | 0.076 | 0.095 | 1 | 0.758 | 0.977 (0.842–1.134) |
| Sufficient staff # | −0.201 | 0.097 | 4.321 | 1 | 0.038 | 0.818 (0.676–0.989) |
| Measures of the hospital # | 0.030 | 0.091 | 0.113 | 1 | 0.737 | 1.031 (0.863–1.232) |
| Constant | 0.356 | 0.944 | 0.142 | 1 | 0.706 | 1.428 |
| Independent Variable Nagelkerkes R2 = 30.2%; Hosmer-Lemeshow test: χ2 = 2.698; df = 8; p = 0.952; 2-Log-Likelihood = 546.477 | ||||||
|---|---|---|---|---|---|---|
| Regression Coefficient | Standard Error | Wald | df | p-Value | OR (95% CI: Minimum–Maximum) | |
| Sociodemographic variables | ||||||
| Gender (Ref. = men) | ||||||
| Women | −0.275 | 0.271 | 1.032 | 1 | 0.310 | 0.759 (0.447–1.291) |
| Age (Ref. = 18–30 years) | ||||||
| 31−40 | 0.037 | 0.389 | 0.009 | 1 | 0.924 | 1.038 (0.484–2.225) |
| 41–50 | −0.234 | 0.439 | 0.285 | 1 | 0.593 | 0.791 (0.335–1.869) |
| >50 | −0.668 | 0.442 | 2.291 | 1 | 0.130 | 0.513 (0.216–1.218) |
| Living alone (Ref. = No) | ||||||
| Yes | −0.127 | 0.279 | 0.209 | 1 | 0.648 | 0.880 (0.510–1.520) |
| Children (Ref. = No) | ||||||
| Yes | 0.204 | 0.278 | 0.539 | 1 | 0.463 | 1.226 (0.712–2.113) |
| Migration background (Ref. = No) | ||||||
| Yes | 0.343 | 0.311 | 1.216 | 1 | 0.270 | 1.409 (0.766–2.592) |
| Caring for old, ill or disabled relatives (Ref. = No) | ||||||
| Yes | 0.157 | 0.290 | 0.291 | 1 | 0.589 | 1.170 (0.662–2.066) |
| Job—related variables | ||||||
| Professional experience in patient care (Ref. = <3 years) | ||||||
| 3−6 | −0.583 | 0.531 | 1.207 | 1 | 0.272 | 0.558 (0.197–1.580) |
| >6 | −0.500 | 0.542 | 0.849 | 1 | 0.357 | 0.607 (0.210–1.757) |
| Employment (Ref. = Full-time) | ||||||
| Part-time | 0.633 | 0.244 | 6.763 | 1 | 0.009 | 1.884 (1.169–3.037) |
| COVID-19—related variables | ||||||
| Infection with SARS-CoV-2 (Ref. = No) | ||||||
| Yes | 0.537 | 0.352 | 2.331 | 1 | 0.127 | 1.711 (0.859–3.411) |
| I don’t know | 0.348 | 0.333 | 1.089 | 1 | 0.297 | 1.416 (0.737–2.719) |
| Contact with infected patients (Ref. = No) | ||||||
| Yes | 0.090 | 0.234 | 0.149 | 1 | 0.699 | 1.094 (0.692–1.730) |
| Risk group due to pre-existing illness (Ref. = No) | ||||||
| Yes | 0.519 | 0.276 | 3.538 | 1 | 0.060 | 1.680 (0.978–2.883) |
| Occupancy rate (Ref. = strongly/slightly below average, average) | ||||||
| Slightly/strongly above average | −0.241 | 0.262 | 0.844 | 1 | 0.358 | 0.786 (0.470–1.314) |
| Change of the department (Ref. = No) | ||||||
| Yes | 0.905 | 0.309 | 8.595 | 1 | 0.003 | 2.471 (1.350–4.523) |
| Symptoms | ||||||
| PHQ-2 * | 0.464 | 0.101 | 20.898 | 1 | <0.001 | 1.590 (1.303–1.940) |
| GAD-2 * | 0.029 | 0.086 | 0.118 | 1 | 0.732 | 1.030 (0.870–1.219) |
| Sleeping disorders # | 0.091 | 0.105 | 0.742 | 1 | 0.389 | 1.095 (0.891–1.346) |
| Exhaustion # | −0.233 | 0.149 | 2.447 | 1 | 0.118 | 0.792 (0.592–1.061) |
| Fear to become infected # | 0.141 | 0.093 | 2.295 | 1 | 0.130 | 1.152 (0.959–1.382) |
| Work—related variables | ||||||
| ERI effort + | −0.017 | 0.075 | 0.053 | 1 | 0.819 | 0.983 (0.848–1.139) |
| ERI reward + | −0.163 | 0.043 | 14.658 | 1 | <0.001 | 0.849 (0.781–0.923) |
| Trust in colleagues # | 0.103 | 0.117 | 0.789 | 1 | 0.374 | 1.109 (0.883–1.394) |
| Higher workload # | 0.167 | 0.098 | 2.905 | 1 | 0.088 | 1.181 (0.975–1.431) |
| Sufficient staff # | −0.118 | 0.125 | 0.886 | 1 | 0.347 | 0.889 (0.696–1.136) |
| Measures of the hospital # | −0.042 | 0.112 | 0.139 | 1 | 0.709 | 0.959 (0.770–1.195) |
| Constant | 0.097 | 1.167 | 0.007 | 1 | 0.934 | 1.102 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schug, C.; Geiser, F.; Hiebel, N.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Morawa, E.; Erim, Y. Sick Leave and Intention to Quit the Job among Nursing Staff in German Hospitals during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1947. https://doi.org/10.3390/ijerph19041947
Schug C, Geiser F, Hiebel N, Beschoner P, Jerg-Bretzke L, Albus C, Weidner K, Morawa E, Erim Y. Sick Leave and Intention to Quit the Job among Nursing Staff in German Hospitals during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(4):1947. https://doi.org/10.3390/ijerph19041947
Chicago/Turabian StyleSchug, Caterina, Franziska Geiser, Nina Hiebel, Petra Beschoner, Lucia Jerg-Bretzke, Christian Albus, Kerstin Weidner, Eva Morawa, and Yesim Erim. 2022. "Sick Leave and Intention to Quit the Job among Nursing Staff in German Hospitals during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 4: 1947. https://doi.org/10.3390/ijerph19041947