
Seroprevalence of SARS-CoV-2 Antibodies in Employees of Three Hospitals of a Secondary Care Hospital Network in Germany and an Associated Fire Brigade: Results of a Repeated Cross-Sectional Surveillance Study Over 1 Year

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Enrolment and Data Management
2.3. SARS-CoV-2 Antibody Testing
2.4. Outcomes
- (i)
- The detection of possible differences among.
- (a)
- HCWs working in high-risk areas with regular contact to COVID-19 positive patients: COVID-19 ward, intensive care unit (ICU), and emergency department.
- (b)
- HCWs working in intermediate-risk areas with contact to COVID-19 negative patients.
- (c)
- Non-HCWs working in low-risk areas with no contact to patients at all (personnel working in administration, kitchen, cleaning service, and others).
- (d)
- Non-HCWs working in the fire brigade with intermediate-risk.
- (ii)
- The description of clinical symptoms 2 months before testing.
- (iii)
- Correlation of the results with the number of COVID-19 positive patients treated, and to the local incidence.
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. Seroprevalence
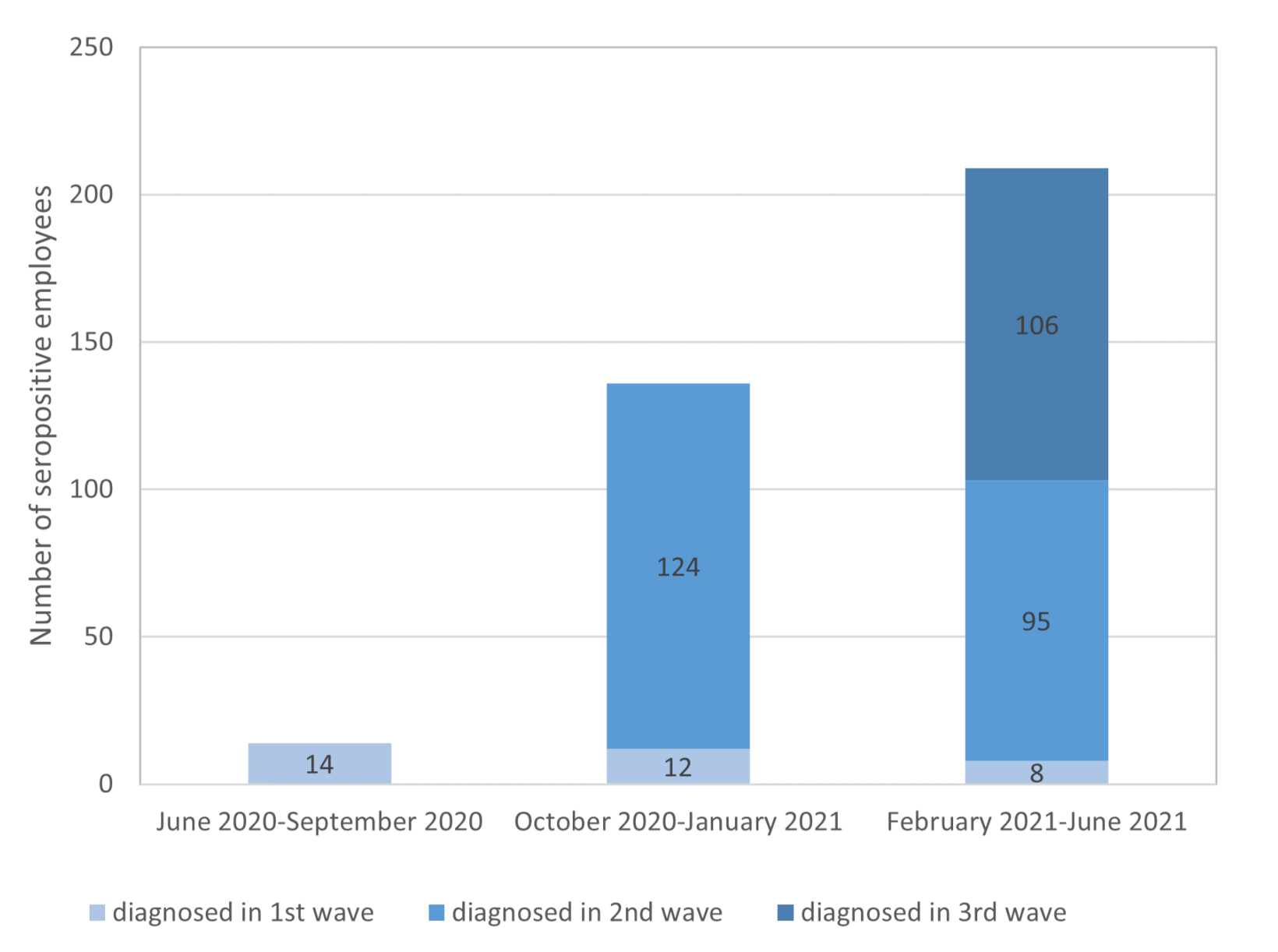
3.2.1. First Observational Period: June–September 2020
3.2.2. Second Observational Period: October 2020–January 2021
3.2.3. Third Observational Period: February–June 2021
3.2.4. Total Seroprevalence within the Year of Observation
3.3. Seroprevalence Associated with Age
3.4. Seroprevalence Associated with Risk at Work
3.4.1. Intermediate-Risk and High-Risk HCWs
3.4.2. Low-Risk and Intermediate-Risk Non-HCWs
3.4.3. Risk According to Profession and Institution
3.5. Clinical Symptoms of Seropositive Employees and Available PCR Results
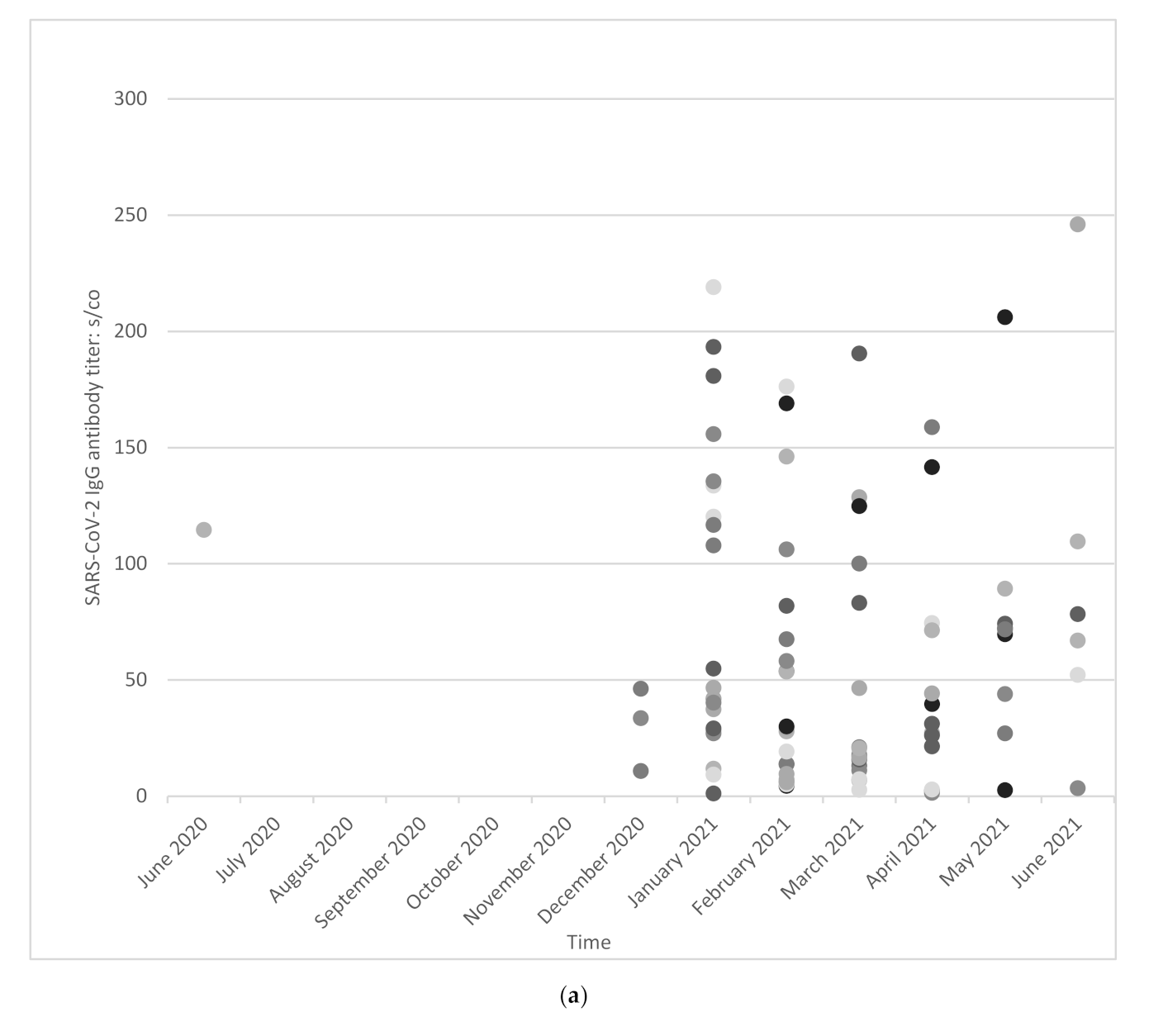
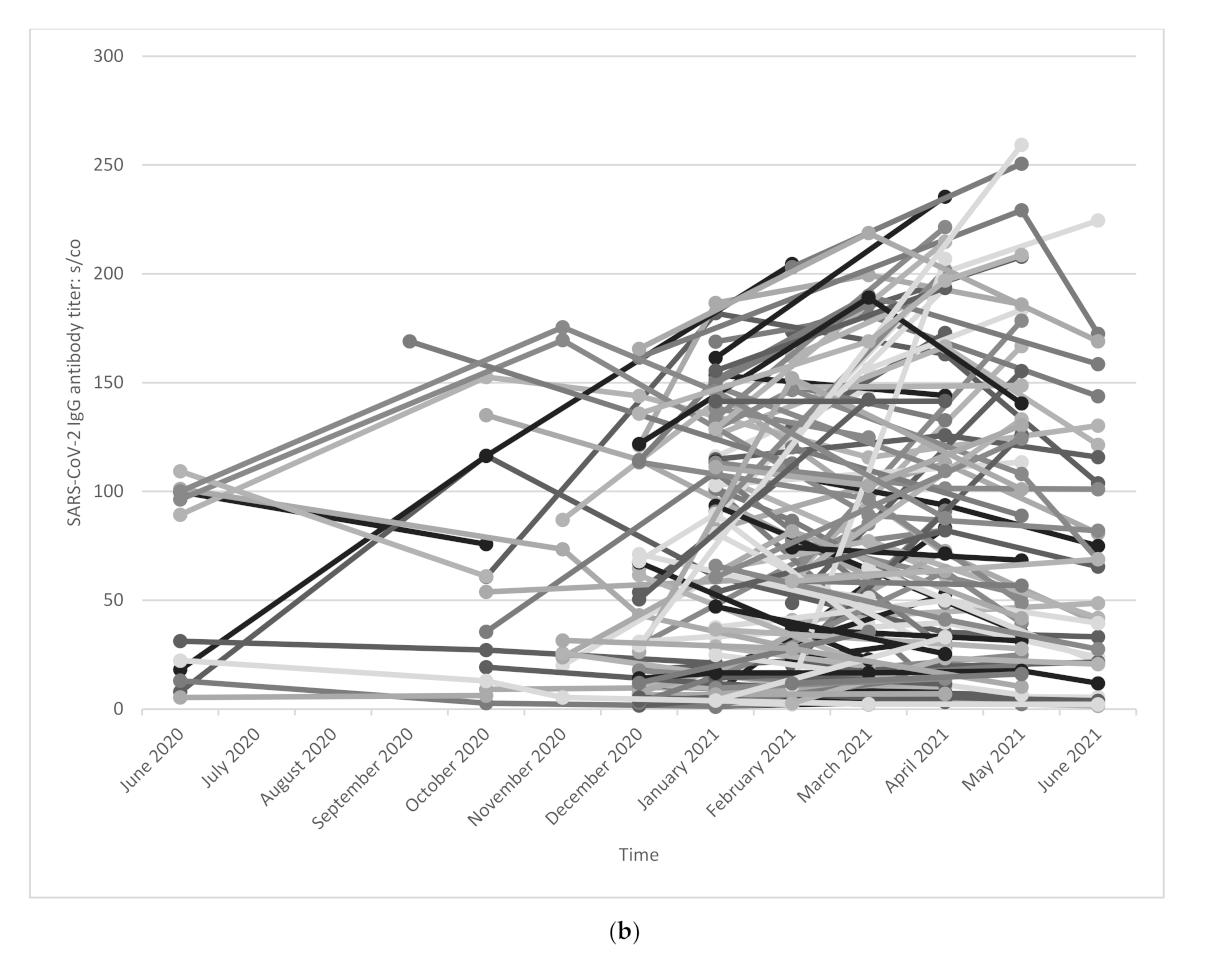
3.6. SARS-CoV-2 IgG Antibody Titer
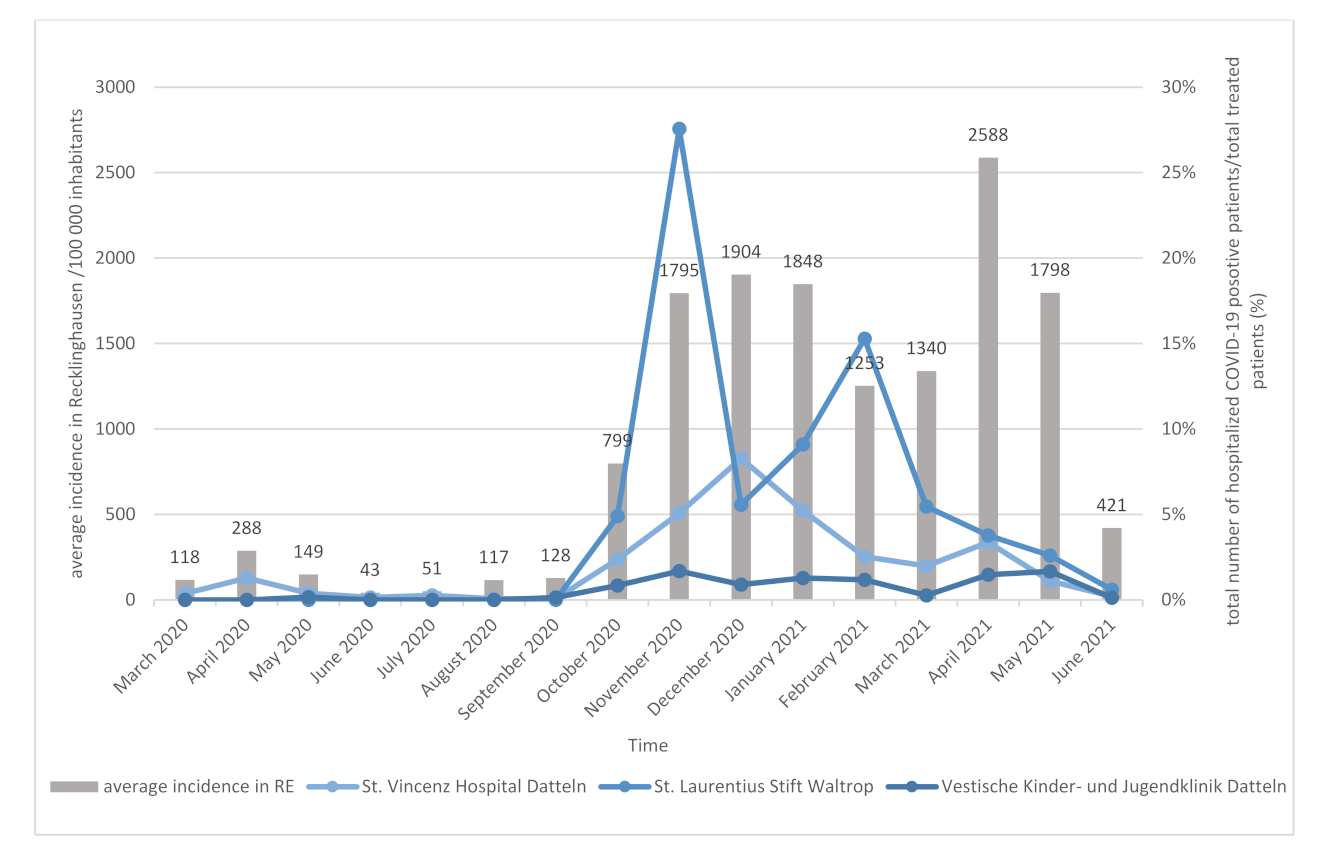
3.7. Seroprevalence with Regard to the Treated COVID-19 Patients and the Epidemiological Context
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Consent for Publication
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Ralph, R.; Lew, J.; Zeng, T.; Francis, M.; Xue, B.; Roux, M.; Toloue Ostadgavahi, A.; Rubino, S.; Dawe, N.J.; Al-Ahdal, M.N.; et al. 2019-nCoV (Wuhan virus), a novel Coronavirus: Human-to-human transmission, travel-related cases, and vaccine readiness. J. Infect. Dev. Ctries. 2020, 14, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, J. COVID-19: A fast evolving pandemic. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 241–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abebe, E.C.; Dejenie, T.A.; Shiferaw, M.Y.; Malik, T. The newly emerged COVID-19 disease: A systemic review. Virol. J. 2020, 17, 96. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019-COVID-19. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of Coronavirus Disease 2019 in China. New Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Pergolizzi, J.V., Jr.; Magnusson, P.; LeQuang, J.A.; Breve, F.; Paladini, A.; Rekatsina, M.; Yeam, C.T.; Imani, F.; Saltelli, G.; Taylor, R., Jr.; et al. The current clinically relevant findings on COVID-19 pandemic. Anesthesiol. Pain Med. 2020, 10, e103819. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and risk factors for Coronavirus infection in health care workers: A living rapid review. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef]
- Khonyongwa, K.; Taori, S.K.; Soares, A.; Desai, N.; Sudhanva, M.; Bernal, W.; Schelenz, S.; Curran, L.A. Incidence and outcomes of healthcare-associated COVID-19 infections: Significance of delayed diagnosis and correlation with staff absence. J. Hosp. Infect. 2020, 106, 663–672. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Impact of personal protective equipment use on health care workers’ physical health during the COVID-19 pandemic: A systematic review and meta-analysis. Am. J. Infect. Control. 2021, 49, 1305–1315. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Ferrante di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 6, CD013652. [Google Scholar] [CrossRef] [PubMed]
- Kayi, I.; Madran, B.; Keske, S.; Karanfil, O.; Arribas, J.R.; Pshenismall es, C.N.; Petrosillo, N.; Gonen, M.; Ergonul, O. The seroprevalence of SARS-CoV-2 antibodies among health care workers before the era of vaccination: A systematic review and meta-analysis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2021, 27, 1242–1249. [Google Scholar] [CrossRef]
- Hossain, A.; Nasrullah, S.M.; Tasnim, Z.; Hasan, M.K.; Hasan, M.M. Seroprevalence of SARS-CoV-2 IgG antibodies among health care workers prior to vaccine administration in Europe, the USA and East Asia: A systematic review and meta-analysis. EClinicalMedicine 2021, 33, 100770. [Google Scholar] [CrossRef] [PubMed]
- Bahrs, C.; Kimmig, A.; Weis, S.; Ankert, J.; Hagel, S.; Maschmann, J.; Stallmach, A.; Steiner, A.; Bauer, M.; Behringer, W.; et al. Prospective surveillance study in a 1,400-bed university hospital: COVID-19 exposure at home was the main risk factor for SARS-CoV-2 point seroprevalence among hospital staff. Transbound. Emerg. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Fill Malfertheiner, S.; Brandstetter, S.; Roth, S.; Harner, S.; Buntrock-Dopke, H.; Toncheva, A.A.; Borchers, N.; Gruber, R.; Ambrosch, A.; Kabesch, M.; et al. Immune response to SARS-CoV-2 in health care workers following a COVID-19 outbreak: A prospective longitudinal study. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 130, 104575. [Google Scholar] [CrossRef]
- Finkenzeller, T.; Faltlhauser, A.; Dietl, K.H.; Paetzel, C.; Szczypien, N.; Klawonn, F.; Bodmann, K.F.; von Meyer, A. SARS-CoV-2 antibodies in ICU and clinic staff: From Germany’s region with the highest infection rate. Med. Klin. Intensivmed. Und Notf. 2020, 115, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Neumann, M.; Aigner, A.; Rossow, E.; Schwarz, D.; Marschallek, M.; Steinmann, J.; Stucker, R.; Koenigs, I.; Stock, P. Low SARS-CoV-2 seroprevalence but high perception of risk among healthcare workers at children’s hospital before second pandemic wave in Germany. World J. Pediatrics: WJP 2021. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, J.; Vollmer, T.; Fischer, B.; Becher, H.; Becker, A.K.; Sahly, H.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. A prospective sero-epidemiological evaluation of SARS-CoV-2 among health care workers in a German secondary care hospital. Int. J. Infect. Dis. IJID: Off. Publ. Int. Soc. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Larribere, L.; Gordejeva, J.; Kuhnhenn, L.; Kurscheidt, M.; Pobiruchin, M.; Vladimirova, D.; Martin, M.; Roser, M.; Schramm, W.; Martens, U.M.; et al. Assessment of SARS-CoV-2 infection among healthcare workers of a German COVID-19 treatment center. Int. J. Environ. Res. Public Health 2021, 18, 7057. [Google Scholar] [CrossRef]
- Brehm, T.T.; Schwinge, D.; Lampalzer, S.; Schlicker, V.; Kuchen, J.; Thompson, M.; Ullrich, F.; Huber, S.; Schmiedel, S.; Addo, M.M.; et al. Seroprevalence of SARS-CoV-2 antibodies among hospital workers in a German tertiary care center: A sequential follow-up study. Int. J. Hyg. Environ. Health 2021, 232, 113671. [Google Scholar] [CrossRef]
- Korth, J.; Wilde, B.; Dolff, S.; Frisch, J.; Jahn, M.; Krawczyk, A.; Trilling, M.; Schipper, L.; Cordes, S.; Ross, B.; et al. SARS-CoV-2 Seroprevalence in healthcare workers in Germany: A follow-up Study. Int. J. Environ. Res. Public Health 2021, 18, 4540. [Google Scholar] [CrossRef]
- Kindgen-Milles, D.; Brandenburger, T.; Braun, J.F.W.; Cleff, C.; Moussazadeh, K.; Mrosewski, I.; Timm, J.; Wetzchewald, D. Prevalence of SARS-CoV-2 positivity in 516 German intensive care and emergency physicians studied by seroprevalence of antibodies National COVID Survey Germany (NAT-COV-SURV). PLoS ONE 2021, 16, e0248813. [Google Scholar] [CrossRef] [PubMed]
- Behrens, G.M.N.; Cossmann, A.; Stankov, M.V.; Schulte, B.; Streeck, H.; Forster, R.; Bosnjak, B.; Willenzon, S.; Boeck, A.L.; Thu Tran, A.; et al. Strategic anti-SARS-CoV-2 serology testing in a low prevalence setting: The COVID-19 Contact (CoCo) study in healthcare professionals. Infect. Dis. Ther. 2020, 9, 837–849. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.B.; Gruter, L.; Boltzmann, M.; Rollnik, J.D. Prevalence of serum IgG antibodies against SARS-CoV-2 among clinic staff. PLoS ONE 2020, 15, e0235417. [Google Scholar] [CrossRef] [PubMed]
- Epstude, J.; Harsch, I.A. Seroprevalence of COVID-19 antibodies in the cleaning and oncological staff of a municipal clinic. GMS Hyg. Infect. Control. 2020, 15, Doc18. [Google Scholar] [CrossRef]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef]
- Lackermair, K.; William, F.; Grzanna, N.; Lehmann, E.; Fichtner, S.; Kucher, H.B.; Wilhelm, K.; Estner, H. Infection with SARS-CoV-2 in primary care health care workers assessed by antibody testing. Fam. Pract. 2021, 38, 76–79. [Google Scholar] [CrossRef]
- Herzberg, J.; Vollmer, T.; Fischer, B.; Becher, H.; Becker, A.K.; Sahly, H.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Half-year longitudinal seroprevalence of SARS-CoV-2-antibodies and rule compliance in German hospital employees. Int. J. Environ. Res. Public Health 2021, 18, 10972. [Google Scholar] [CrossRef]
- Perkhofer, L.; Grunke, P.; Gashi-Ymeri, E.; Grunke, T.; Kroschel, J.; Michel, D.; Pensel, E.; Rost, A.; Denkinger, M.; Dallmeier, D.; et al. COVID-19 pandemic-related burden and SARS-CoV-2 prevalence in care facilities. Z. Gerontol. Geriatr. 2021, 54, 463–470. [Google Scholar] [CrossRef]
- Weinberger, T.; Steffen, J.; Osterman, A.; Mueller, T.T.; Muenchhoff, M.; Wratil, P.R.; Graf, A.; Krebs, S.; Quartucci, C.; Spaeth, P.M.; et al. Prospective longitudinal serosurvey of health care workers in the first wave of the SARS-CoV-2 pandemic in a quaternary care hospital in Munich, Germany. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e3055–e3056. [Google Scholar] [CrossRef]
- Epstude, J.; Skiba, M.; Harsch, I.A. Antibody titers and rapid antigen testing in elderly patients with SARS-CoV-2 pneumonia vs. staff of ICU and „COVID-19” wards. GMS Hyg. Infect. Control. 2021, 16, Doc11. [Google Scholar] [CrossRef] [PubMed]
- Reinwald, M.; Deckert, P.M.; Ritter, O.; Andresen, H.; Schreyer, A.G.; Weylandt, K.H.; Dammermann, W.; Luth, S. Prevalence and course of IgA and IgG antibodies against SARS-CoV-2 in healthcare workers during the first wave of the COVID-19 Outbreak in Germany: Interim results from an ongoing observational cohort study. Healthcare 2021, 9, 498. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.; Girl, P.; Ruhnke, M.; Spranger, M.; Kaier, K.; von Buttlar, H.; Dobler, G.; Borde, J.P. SARS-CoV-2 Seroprevalence among health care workers—A voluntary screening study in a regional medical center in southern Germany. Int. J. Environ. Res. Public Health 2021, 18, 3910. [Google Scholar] [CrossRef] [PubMed]
- Kern, P.K.; Weißer, H.; Menzel, T. Erstes Großklinikum umfangreich getestet—Keine relevante Immunität gegen SARS-CoV-2 in Fulda. Klin. Fulda Pressemitt. 2020. [Google Scholar]
- Hoffmann, S.; Schiebel, J.; Hufert, F.; Gremmels, H.D.; Spallek, J. COVID-19 among healthcare workers: A prospective serological-epidemiological cohort study in a standard care hospital in rural Germany. Int. J. Environ. Res. Public Health 2021, 18, 10999. [Google Scholar] [CrossRef]
- Harsch, I.A.; Skiba, M.; Konturek, P.C.; Epstude, J. Prevalence of antibodies against COVID-19 in the staff of a COVID-19 regular ward. GMS Hyg. Infect. Control. 2020, 15, Doc09. [Google Scholar] [CrossRef]
- Brune, B.; Korth, J.; Fessmann, K.; Stappert, D.; Nohl, A.; Lembeck, T.; Standl, F.; Stang, A.; Dittmer, U.; Witzke, O.; et al. SARS-CoV-2 IgG seroprevalence in personnel of the extraclinical fight against the COVID-19 pandemic. Notf. Rett. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Tomczyk, S.; Honning, A.; Hermes, J.; Grossegesse, M.; Hofmann, N.; Michel, J.; Neumann, M.; Nitsche, A.; Hoppe, B.; Eckmanns, T.; et al. Longitudinal SARS-CoV-2 seroepidemiological investigation among healthcare workers at a tertiary care hospital in Germany. BMC Infect. Dis. 2022, 22, 80. [Google Scholar] [CrossRef]
- Hildebrandt, A.; Hökelekli, O.; Uflacker, L.; Rudolf, H.; Gatermann, S.G. COVID-19: Hotspot hospital?- seroprevalence of SARS-CoV-2 antibodies in hospital employees in a secondary care hospital network in Germany: Intermediate results of a prospective surveillance study. Int. J. Hyg. Environ. Health 2021, 235, 113771. [Google Scholar] [CrossRef]
- R Core Team, R: A Language and Environment for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 18 November 2021).
- RKI. Available online: https://web.archive.org/web/20200424144252/https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Massnahmen_Verdachtsfall_Infografik_Tab.html (accessed on 28 April 2020).
- Gornyk, D.; Harries, M.; Glöckner, S.; Strengert, M.; Kerrinnes, T.; Heise, J.K.; Maaß, H.; Ortmann, J.; Kessel, B.; Kemmling, Y.; et al. SARS-CoV-2 seroprevalence in Germany—a population-based sequential study in seven regions. Dtsch. Arztebl. Int. 2021, 118, 824–831. [Google Scholar] [CrossRef]
- Wachtler, B.; Neuhauser, H.; Haller, S.; Grabka, M.M.; Zinn, S.; Schaade, L.; Hövener, C.; Hoebel, J. The risk of infection with SARS-CoV-2 among healthcare workers during the pandemic—Findings of a nationwide sero-epidemiological study in Germany. Dtsch. Arztebl. Int. 2021, 118, 842–843. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital | Time Period | Number of Employees Tested | SARS-CoV-2 IgG Antibody Rate | Additional Information | Reference |
|---|---|---|---|---|---|
| University Hospital Bonn | First wave | 217 frontline HCWs | 1.86% | [23] | |
| University Hospital Jena | First wave | 660 employees | 1.90% | [14] | |
| University Regensburg | First wave | 166 HCWs | 0.00% | Perinatal center | [15] |
| BDH Clinic Hessisch Oldendorf | First wave | 406 employees | 2.70% | Neurological center | [24] |
| Saalfeld | First wave | 45 employees, 20 HCWs | 1.54% | Cleaning staff, oncological ward | [25] |
| University Hospital Essen | First wave, second wave | March–December 2020 450 HCWs | March–May 2020: 2.2%; June–July 2020: 4.0%; August–December 2020: 5.1% | Classification into high-risk, intermediate-risk and low-risk group | [21,26] |
| Weiden and Tirschenreuth, Bavaria | First wave (July 2020) | 1838/2387 HCWs (77%) | 15.1% HCWs | Region with highest rate of infection | [16] |
| University Hospital Munich | First wave | 151 HCWs | 2.60% | [27] | |
| Altona Children’s hospital Hamburg | First wave | 619 hospital employees | 0.33% | 70.3% of total staff | [17] |
| Hamburg | First wave | 871 employees April 2020 406 employees follow-up in October 2020 | 4.36% 0.74% | Secondary care hospital | [18,28] |
| Heilbronn | First wave | 3067 HCWs | 3.50% | COVID-19 treatment center | [19] |
| Ulm | First wave | 394 HCWs | 0.25% | Residential care home for the elderly | [29] |
| University Medical Center Hamburg-Eppendorf | First wave | 1253 employees including 1026 HCWs | 1.80% | [20] | |
| Munich | First wave | 300 HCWs | 4.67% | Quaternary care hospital | [30] |
| Saalfeld | First wave | 68 HCWs | 0% | ICU and COVID-19 ward | [31] |
| Two university hospitals in Brandenburg | First wave | 1013 HCWs | 2.1–2.2% | Ongoing study | [32] |
| Ortenaukreis | First wave | 198 HCWs | 3.50% | Regional medical center and several outpatient facilities | [33] |
| Fulda | First wave | 1800 HCWs | 1% | [34] | |
| HCWs recruited in all parts of Germany | First wave | 516 HCWs | 3.50% | Intensive care and emergency care unit | [22] |
| Oberspreewald-Lausitz | First wave, second wave (July–December 2020) | 166 HCWs | 13.30% | Standard care hospital | [35] |
| Saalfeld | First wave | 18 employees | 0.00% | Regular ward | [36] |
| Essen | First wave | 732 employees | 1.1% | Professional fire brigade and aid organizations in the city area | [37] |
| Berlin | First wave | 1477 HCWs 1223 HCWs | May/June 2020: 1.2% December 2020: 4.6% | Tertiary care hospital | [38] |
| St. Vincenz Hospital Datteln | First wave, second wave, third wave | 1842 employees including 1411 HCWs | June–September 2020: 1.2% October 2020–January 2021: 13.2% February–June 2021: 29.3% | Employees of three hospitals of a secondary care hospital network and an associated fire brigade | [39], actual data |
| Variable | SARS-CoV-2 Antibodies Total | Statistics | |||
|---|---|---|---|---|---|
| All Employees Without Repeated Testing | OR (95% CI) | p-Value | |||
| All | Not Detectable | Detectable | |||
| n = 1842 | n = 1599 | n = 243 | |||
| Age a | 0.040 | ||||
| 16–25 years | 301 (16.5%) | 251 (15.8%) | 50 (20.7%) | Reference | |
| 26–40 years | 527 (28.8%) | 450 (28.3%) | 77 (31.8%) | 0.86 [0.58; 1.27] | |
| >40 years | 999 (54.7%) | 884 (55.8%) | 115 (47.5%) | 0.65 [0.46; 0.94] | |
| Sex | 0.396 | ||||
| Male | 1503 (81.6%) | 1310 (82.0%) | 193 (79.4%) | Reference | |
| Female | 339 (18.4%) | 289 (18.0%) | 50 (20.6%) | 1.18 [0.83; 1.64] | |
| Hospital/Institution | <0.001 | ||||
| St. Vincenz Hospital Datteln | 858 (46.6%) | 725 (45.3%) | 133 (54.7%) | Reference | |
| St.-Laurentius-Stift Waltrop | 319 (17.3%) | 260 (16.3%) | 59 (24.3%) | 1.24 [0.88; 1.73] | |
| Children’s Hospital Datteln | 522 (28.3%) | 487 (30.5%) | 35 (14.4%) | 0.39 [0.26; 0.57] | |
| Fire brigade | 103 (5.6%) | 90 (5.6%) | 13 (5.4%) | 0.80 [0.41; 1.42] | |
| others | 40 (2.2%) | 37 (2.3%) | 3 (1.2%) | 0.46 [0.11; 1.31] | |
| Profession | 0.7135 | ||||
| Nurse | 927 (50.3%) | 802 (50.2%) | 125 (51.4%) | Reference | |
| Medical doctor | 215 (11.7%) | 187 (11.7%) | 28 (11.5%) | 0.96 [0.61; 1.48] | |
| Care worker | 201 (10.9%) | 168 (10.5%) | 33 (13.6%) | 1.26 [0.82; 1.90] | |
| Cleaning service | 36 (2.0%) | 31 (1.9%) | 5 (2.1%) | 1.06 [0.35; 2.57] | |
| Administration staff | 136 (7.4%) | 124 (7.8%) | 12 (4.9%) | 0.63 [0.32; 1.13] | |
| Fire brigade | 103 (5.6%) | 90 (5.6%) | 13 (5.4%) | 0.94 [0.48; 1.67] | |
| Kitchen | 35 (1.9%) | 31 (1.9%) | 4 (1.7%) | 0.86 [0.25; 2.22] | |
| Therapist | 88 (4.8%) | 75 (4.7%) | 13 (5.4%) | 1.12 [0.58; 2.02] | |
| Other profession | 101 (5.5%) | 91 (5.7%) | 10 (4.1%) | 0.71 [0.34; 1.35] | |
| Risk of COVID-19 infection | <0.001 | ||||
| non-HCW | |||||
| Low-risk-group: working without patient contact | 328 (17.8%) | 292 (18.3%) | 36 (14.8%) | Reference | |
| Intermediate-risk group: fire brigade | 103 (5.6%) | 90 (5.6%) | 13 (5.4%) | 1.18 [0.58; 2.28] | |
| HCW | |||||
| Intermediate-risk group | 1223 (66.4%) | 1071 (67.0%) | 152 (62.6%) | 1.15 [0.79; 1.71] | |
| High-risk group | 188 (10.2%) | 146 (9.1%) | 42 (17.3%) | 2.33 [1.43; 3.81] | |
| Number of symptoms within the last 2 months | <0.001 | ||||
| No symptoms | 1373 (74.5%) | 1246 (77.9%) | 127 (52.3%) | Reference | |
| 1 symptom | 268 (14.5%) | 230 (14.4%) | 38 (15.6%) | 1.62 [1.09; 2.38] | |
| 2 symptoms | 78 (4.2%) | 60 (3.8%) | 18 (7.4%) | 2.96 [1.65; 5.08] | |
| 3 symptoms | 77 (4.2%) | 48 (3.0%) | 29 (11.9%) | 5.93 [3.57; 9.69] | |
| 4 symptoms | 46 (2.5%) | 15 (0.9%) | 31 (12.8%) | 20.1 [10.7; 39.3] | |
| 5 symptoms | |||||
| Clinical symptoms within the last 2 months b | |||||
| Cold-like symptoms | 173 (9.4%) | 126 (7.9%) | 47 (19.3%) | 2.81 [1.93; 4.03] | <0.001 |
| Headache | 179 (9.7%) | 116 (7.3%) | 63 (25.9%) | 4.47 [3.16; 6.29] | <0.001 |
| Fever | 105 (5.7%) | 60 (3.8%) | 45 (18.5%) | 5.82 [3.83; 8.81] | <0.001 |
| Cough | 261 (14.2%) | 205 (12.8%) | 56 (23.0%) | 2.04 [1.45; 2.83] | <0.001 |
| Hoarseness | 17 (0.92%) | 15 (0.94%) | 2 (0.82%) | 0.93 [0.13; 3.37] | 1.000 |
| Taste or smell disorders | 104 (5.7%) | 32 (2.0%) | 72 (29.6%) | 20.5 [13.2; 32.4] | <0.001 |
| Additional information | |||||
| Previous PCR testing c | <0.001 | ||||
| No information | 1169 (63.5%) | 1143 (71.5%) | 26 (10.7%) | Reference | |
| PCR without known result | 38 (2.1%) | 24 (1.5%) | 14 (5.8%) | 25.4 [10.9; 58.2] | |
| Positive | 173 (9.4%) | 4 (0.3%) | 169 (69.5%) | 1715 [620; 8192] | |
| Negative | 462 (25.1%) | 428 (26.8%) | 34 (14.0%) | 3.49 [2.01; 6.13] | |
| Basic Information | St. Vincenz Hospital Datteln | St. Laurentius Stift Waltrop | Vestische Kinder -und Jugendklinik Datteln | Fire Brigade | Other Institutions | Total Number |
|---|---|---|---|---|---|---|
| Beds | 316 | 172 | 244 | n.a. | n.a. | n.a. |
| Employees | 1085 | 375 | 1240 | 104 | n.I. | 2804 |
| Tested employees (%) | 862 (79.4%) | 324 (86.4%) | 528 (42.6%) | 103 (99.04%) | 40/n.I. | 1817 (64.8%) |
| SARS-CoV-2 IgG antibodies tested employees | ||||||
| June 2020 to September 2020: positive/tested (%) | 5/674 (0.7%) | 8/235 (3.4%) | 1/300 (0.3%) | - | 0/32 | 14/1241 (1.13%) |
| October 2020 to January 2021: positive/tested (%) | 72/395 (18.2%) | 42/231 (18.2%) | 19/356 (5.3%) | 2/46 (4.3%) | 2/7 (28.6%) | 137/1035 (13.2%) |
| February 2021 to June 2021: positive/tested (%) | 116/307 (37.8%) | 48/108 (44.4%) | 32/240 (13.3%) | 11/57 (19.3%) | 2/2 (100%) | 209/714 (29.3%) |
| Altogether | ||||||
| Positive tests/tests | 249/1522 (16.4%) | 123/668 (18.4%) | 68/951 (7.1%) | 13/103 (12.6%) | 4/41 (9.75%) | 457/3285 (13.9%) |
| Positive employees/tested employees (%) (counting all only once in each wave) | 193/1376 (14.0%) | 98/574 (17.1%) | 52/896 (5.8%) | 13/103 (12.6%) | 4/41 (9.75%) | 360/2990 (12.0%) |
| Positive employees/tested employees (%) (counting each employee only once at all) | 133/858 (15.5%) | 59/319 (18.5%) | 35/522 (6.7%) | 13/103 (12.6%) | 3/40 (7.5%) | 243/1842 (13.2%) |
| vaccinated employees/tested employees (February 2021 to June 2021) | 155/307 (50.5%) | 43/108 (39.8%) | 158/240 (65.8%) | 22/57 (38.6%) | 1/2 (50%) | |
| COVID-19 patients | ||||||
| Hospitalised patients | 380 | 106 | 66 | n.a. | n.a. | |
| Patients on intensive care unit | 36 | n.a. | 4 | n.a. | n.a. | |
| Patients died | 48 | 0 | 0 | n.a. | n.a. | |
| Outpatients | 82 | n.a. | 5 * | n.a. | n.a. | |
| SARS-CoV-2 infection in employees | ||||||
| PCR positive | 137 | 63 | 41 | n.I. | n.I. | |
| PCR positive, IgG positive | 133 | 59 | 35 | n.I. | n.I. | |
| PCR positive, IgG antibodies negative | 4 | 4 | n.I. | n.I. | n.I. | |
| PCR positive, IgG not tested | 28 | 12 | n.I. | n.I. | n.I. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hildebrandt, A.; Hökelekli, O.; Uflacker, L.; Rudolf, H.; Paulussen, M.; Gatermann, S.G. Seroprevalence of SARS-CoV-2 Antibodies in Employees of Three Hospitals of a Secondary Care Hospital Network in Germany and an Associated Fire Brigade: Results of a Repeated Cross-Sectional Surveillance Study Over 1 Year. Int. J. Environ. Res. Public Health 2022, 19, 2402. https://doi.org/10.3390/ijerph19042402
Hildebrandt A, Hökelekli O, Uflacker L, Rudolf H, Paulussen M, Gatermann SG. Seroprevalence of SARS-CoV-2 Antibodies in Employees of Three Hospitals of a Secondary Care Hospital Network in Germany and an Associated Fire Brigade: Results of a Repeated Cross-Sectional Surveillance Study Over 1 Year. International Journal of Environmental Research and Public Health. 2022; 19(4):2402. https://doi.org/10.3390/ijerph19042402
Chicago/Turabian StyleHildebrandt, Anke, Oktay Hökelekli, Lutz Uflacker, Henrik Rudolf, Michael Paulussen, and Sören G. Gatermann. 2022. "Seroprevalence of SARS-CoV-2 Antibodies in Employees of Three Hospitals of a Secondary Care Hospital Network in Germany and an Associated Fire Brigade: Results of a Repeated Cross-Sectional Surveillance Study Over 1 Year" International Journal of Environmental Research and Public Health 19, no. 4: 2402. https://doi.org/10.3390/ijerph19042402