
A Single-Day Training for Managers Reduces Cognitive Stigma Regarding Mental Health Problems: A Randomized Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Training
2.3. Questionnaires
2.4. Data Sample
2.5. Design & Data Analysis
3. Results
3.1. Descriptives
3.2. Quantitative Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harvey, S.B.; Henderson, M.; Lelliott, P.; Hotopf, M. Mental health and employment: Much work still to be done. Br. J. Psychiatry 2009, 194, 201–203. [Google Scholar] [CrossRef] [Green Version]
- Petrie, K.; Joyce, S.; Tan, L.; Henderson, M.; Johnson, A.; Nguyen, H.; Modini, M.; Groth, M.; Glozier, N.; Harvey, S.B. A framework to create more mentally healthy workplaces: A viewpoint. Aust. N. Z. J. Psychiatry 2018, 52, 15–23. [Google Scholar] [CrossRef]
- Falkai, P. Bedeutung psychischer Erkrankungen für das Gesundheitssystem in Deutschland. Drug Res. 2017, 67 (Suppl. S1), S3–S4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smit, H.; Cuijpers, P.; Oostenbrink, J.; Batelaan, N.; de Graaf, R.; Beekman, A.J. Costs of Nine Common Mental Disorders: Implications for Curative and Preventive Psychiatry. J. Ment. Health Policy Econ. 2006, 9, 193–200. [Google Scholar] [PubMed]
- Jacobi, F.; Höfler, M.; Strehle, J.; Mack, S.; Gerschler, A.; Scholl, L.; Busch, M.A.; Maske, U.; Hapke, U.; Gaebel, W.; et al. Psychische Störungen in der Allgemeinbevölkerung: Studie zur Gesundheit Erwachsener in Deutschland und ihr Zusatzmodul Psychische Gesundheit (DEGS1-MH). Nervenarzt 2014, 85, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Bundespsychotherapeutenkammer. BPtK-Studie zur Arbeits- und Erwerbsunfähigkeit: Psychische Erkrankungen und Gesundheitsbedingte Frühverrentung. Available online: https://www.bptk.de/wp-content/uploads/2019/01/20140128_BPtK-Studie_Arbeits-und_Erwerbsunfaehigkeit-2013.pdf (accessed on 8 January 2022).
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, D.A.; McLaughlin, T.J.; Rogers, W.H.; Chang, H.; Lapitsky, L.; Lerner, D. Job performance deficits due to depression. Am. J. Psychiatry 2006, 163, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Lerner, D.; Henke, R.M. What does research tell us about depression, job performance, and work productivity? J. Occup. Environ. Med. 2008, 50, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.B.; Glozier, N.; Henderson, M.; Allaway, S.; Litchfield, P.; Holland-Elliott, K.; Hotopf, M. Depression and work performance: An ecological study using web-based screening. Occup. Med. 2011, 61, 209–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.S.; Beck, A.L.; Berglund, P.; McKenas, D.K.; Pronk, N.P.; Simon, G.E.; Kessler, R.C. Effects of major depression on moment-in-time work performance. Am. J. Psychiatry 2004, 161, 1885–1891. [Google Scholar] [CrossRef] [PubMed]
- Evans-Lacko, S.; Knapp, M. Global patterns of workplace productivity for people with depression: Absenteeism and presenteeism costs across eight diverse countries. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1525–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Siegrist, J. Effort-reward imbalance at work and health. In Historical and Current Perspectives on Stress and Health; Research in Occupational Stress and Well-Being; Emerald Group Publishing Limited: Bingley, Great Britain, 2002; pp. 261–291. [Google Scholar] [CrossRef]
- Dragano, N.; Siegrist, J.; Nyberg, S.T.; Lunau, T.; Fransson, E.I.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Erbel, R.; et al. Effort-Reward Imbalance at Work and Incident Coronary Heart Disease: A Multicohort Study of 90,164 Individuals. Epidemiology 2017, 28, 619–626. [Google Scholar] [CrossRef]
- Siegrist, J.; Li, J. Work Stress and Altered Biomarkers: A Synthesis of Findings Based on the Effort-Reward Imbalance Model. Int. J. Environ. Res. Public Health 2017, 14, 1373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Vegchel, N.; de Jonge, J.; Bosma, H.; Schaufeli, W. Reviewing the effort-reward imbalance model: Drawing up the balance of 45 empirical studies. Soc. Sci. Med. 2005, 60, 1117–1131. [Google Scholar] [CrossRef] [PubMed]
- Franke, F.; Ducki, A.; Felfe, J. Trends in der Psychologischen Führungsforschung: Neue Konzepte, Methoden und Erkenntnisse; Hogrefe: Göttingen, Germany, 2014. [Google Scholar]
- Harms, P.D.; Credé, M.; Tynan, M.; Leon, M.; Jeung, W. Leadership and stress: A meta-analytic review. Leadersh. Q. 2017, 28, 178–194. [Google Scholar] [CrossRef]
- Selart, M.; Johansen, S.T. Ethical Decision Making in Organizations: The Role of Leadership Stress. J. Bus Ethics 2011, 99, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Driskell, J.E.; Salas, E.; Johnston, J. Does stress lead to a loss of team perspective? Group Dyn. Theory Res. Pract. 1999, 3, 291–302. [Google Scholar] [CrossRef]
- Campbell, M.; Baltes, J.I.; Martin, A.; Meddings, K. The stress of leadership. Cent. Creat. Leadersh. 2007, 10, 3–15. [Google Scholar]
- Jones, A.M. Disclosure of Mental Illness in the Workplace: A Literature Review. Am. J. Psychiatr. Rehabil. 2011, 14, 212–229. [Google Scholar] [CrossRef]
- Mintz, J.; Mintz, L.I.; Arruda, M.J.; Hwang, S.S. Treatments of depression and the functional capacity to work. Arch. Gen. Psychiatry 1992, 49, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Schomerus, G.; Angermeyer, M.C. Stigma and its impact on help-seeking for mental disorders: What do we know? Epidemiol. Psychiatr. Sci. 2008, 17, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Angermeyer, M.C.; Dietrich, S. Public beliefs about and attitudes towards people with mental illness: A review of population studies. Acta Psychiatr. Scand. 2006, 113, 163–179. [Google Scholar] [CrossRef] [PubMed]
- Krupa, T.; Kirsh, B.; Cockburn, L.; Gewurtz, R. Understanding the stigma of mental illness in employment. Work 2009, 33, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Sharac, J.; McCrone, P.; Clement, S.; Thornicroft, G. The economic impact of mental health stigma and discrimination: A systematic review. Epidemiol. Psychiatr. Sci. 2010, 19, 223–232. [Google Scholar] [CrossRef]
- Rüsch, N.; Berger, M.; Finzen, A.; Angermeyer, M.C. Das Stigma Psychischer Erkrankungen–Ursachen, Formen und Therapeutische Konsequenzen. 2004. Available online: http://berger-psychische-erkrankungen-klinik-und-therapie.de/ergaenzung_ruesch.pdf (accessed on 8 January 2022).
- Holzinger, A.; Beck, M.; Munk, I.; Weithaas, S.; Angermeyer, M.C. Das Stigma psychischer Krankheit aus der Sicht schizophren und depressiv Erkrankter. Psychiatr. Prax. 2003, 30, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.H.C.; Bathje, G.J.; Kalibatseva, Z.; Sung, D.; Leong, F.T.L.; Collins-Eaglin, J. Stigma, mental health, and counseling service use: A person-centered approach to mental health stigma profiles. Psychol. Serv. 2017, 14, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Clement, S.; Schauman, O.; Graham, T.; Maggioni, F.; Evans-Lacko, S.; Bezborodovs, N.; Morgan, C.; Rüsch, N.; Brown, J.S.L.; Thornicroft, G. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 2015, 45, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Schibalski, J.V.; Müller, M.; Ajdacic-Gross, V.; Vetter, S.; Rodgers, S.; Oexle, N.; Corrigan, P.W.; Rössler, W.; Rüsch, N. Stigma-related stress, shame and avoidant coping reactions among members of the general population with elevated symptom levels. Compr. Psychiatry 2017, 74, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Schomerus, G.; Schwahn, C.; Holzinger, A.; Corrigan, P.W.; Grabe, H.J.; Carta, M.G.; Angermeyer, M.C. Evolution of public attitudes about mental illness: A systematic review and meta-analysis. Acta Psychiatr. Scand. 2012, 125, 440–452. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.J.; Reavley, N.J.; Ross, A.; Too, L.S.; Jorm, A.F. Interventions to reduce stigma towards people with severe mental illness: Systematic review and meta-analysis. J. Psychiatr. Res. 2018, 103, 120–133. [Google Scholar] [CrossRef]
- Thornicroft, G.; Mehta, N.; Clement, S.; Evans-Lacko, S.; Doherty, M.; Rose, D.; Koschorke, M.; Shidhaye, R.; O’Reilly, C.; Henderson, C. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet 2016, 387, 1123–1132. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Druss, B.G.; Perlick, D.A. The Impact of Mental Illness Stigma on Seeking and Participating in Mental Health Care. Psychol. Sci. Public Interest J. Am. Psychol. Soc. 2014, 15, 37–70. [Google Scholar] [CrossRef] [Green Version]
- Carr, W.; Wei, Y.; Kutcher, S.; Heffernan, A. Preparing for the Classroom: Mental Health Knowledge Improvement, Stigma Reduction and Enhanced Help-Seeking Efficacy in Canadian Preservice Teachers. Can. J. Sch. Psychol. 2018, 33, 314–326. [Google Scholar] [CrossRef]
- Gould, M.; Greenberg, N.; Hetherton, J. Stigma and the military: Evaluation of a PTSD psychoeducational program. J. Trauma. Stress 2007, 20, 505–515. [Google Scholar] [CrossRef]
- Hansson, L.; Markström, U. The effectiveness of an anti-stigma intervention in a basic police officer training programme: A controlled study. BMC Psychiatry 2014, 14, 55. [Google Scholar] [CrossRef] [Green Version]
- Dimoff, J.K.; Kelloway, E.K.; Burnstein, M.D. Mental health awareness training (MHAT): The development and evaluation of an intervention for workplace leaders. Int. J. Stress Manag. 2016, 23, 167–189. [Google Scholar] [CrossRef]
- Hamann, J.; Mendel, R.; Reichhart, T.; Rummel-Kluge, C.; Kissling, W. A “Mental-Health-at-the-Workplace” Educational Workshop Reduces Managers’ Stigma Toward Depression. J. Nerv. Ment. Dis. 2016, 204, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Shann, C.; Martin, A.; Chester, A.; Ruddock, S. Effectiveness and application of an online leadership intervention to promote mental health and reduce depression-related stigma in organizations. J. Occup. Health Psychol. 2019, 24, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Gayed, A.; Milligan-Saville, J.S.; Nicholas, J.; Bryan, B.T.; LaMontagne, A.D.; Milner, A.; Madan, I.; Calvo, R.A.; Christensen, H.; Mykletun, A.; et al. Effectiveness of training workplace managers to understand and support the mental health needs of employees: A systematic review and meta-analysis. Occup. Environ. Med. 2018, 75, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Milligan-Saville, J.S.; Tan, L.; Gayed, A.; Barnes, C.; Madan, I.; Dobson, M.; Bryant, R.A.; Christensen, H.; Mykletun, A.; Harvey, S.B. Workplace mental health training for managers and its effect on sick leave in employees: A cluster randomised controlled trial. Lancet Psychiatry 2017, 4, 850–858. [Google Scholar] [CrossRef]
- Boysen, E.; Schiller, B.; Mörtl, K.; Gündel, H.; Hölzer, M. Preliminary Analyses Showed Short-Term Mental Health Improvements after a Single-Day Manager Training. Int. J. Environ. Res. Public Health 2018, 15, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, E.; Schiller, B.; Moertl, K.; Weimer, K.; Eisele, M.; Kauderer, J.; Papenfuss, F.; Guendel, H.; Hoelzer, M. Long-Term Attitude Change After a Single-Day Manager Training Addressing Mental Health at the Workplace. Int. J. Environ. Res. Public Health 2019, 16, 5105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans-Lacko, S.; Little, K.; Meltzer, H.; Rose, D.; Rhydderch, D.; Henderson, C.; Thornicroft, G. Development and psychometric properties of the Mental Health Knowledge Schedule. Can. J. Psychiatry Rev. Can. Psychiatr. 2010, 55, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Link, B.G.; Phelan, J.C.; Bresnahan, M.; Stueve, A.; Pescosolido, B.A. Public conceptions of mental illness: Labels, causes, dangerousness, and social distance. Am. J. Public Health 1999, 89, 1328–1333. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.L. Chronic Schizophrenia; Taylor and Francis: Abingdon, UK, 2013. [Google Scholar]
- Mack, S.; Jacobi, F.; Gerschler, A.; Strehle, J.; Höfler, M.; Busch, M.A.; Maske, U.E.; Hapke, U.; Seiffert, I.; Gaebel, W.; et al. Self-reported utilization of mental health services in the adult German population--evidence for unmet needs? Results of the DEGS1-Mental Health Module (DEGS1-MH). Int. J. Methods Psychiatr. Res. 2014, 23, 289–303. [Google Scholar] [CrossRef]
- Marie, D.; Miles, B. Social distance and perceived dangerousness across four diagnostic categories of mental disorder. Aust. N. Z. J. Psychiatry 2008, 42, 126–133. [Google Scholar] [CrossRef]
- Warttig, S.L.; Forshaw, M.J.; South, J.; White, A.K. New, normative, English-sample data for the Short Form Perceived Stress Scale (PSS-4). J. Health Psychol. 2013, 18, 1617–1628. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived Stress Scale (PSS). J. Health Soc. Behav. 1983. [Google Scholar] [CrossRef]
- Rödel, A.; Siegrist, J.; Hessel, A.; Brähler, E. Fragebogen zur Messung beruflicher Gratifikationskrisen. Z. Für Differ. Diagn. Psychol. 2004, 25, 227–238. [Google Scholar] [CrossRef]
- Mohr, G.; Rigotti, T.; Müller, A. Irritation—Ein Instrument zur Erfassung Psychischer Beanspruchung im Arbeitskontext. Skalen- und Itemparameter aus 15 Studien. Z. Für Arb. Organ. AO 2005, 49, 44–48. [Google Scholar] [CrossRef]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The measurement of effort–reward imbalance at work: European comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Mohr, G.; Müller, A.; Rigotti, T. Normwerte der Skala Irritation: Zwei Dimensionen psychischer Beanspruchung1. Diagnostica 2005, 51, 12–20. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. An Ultra-Brief Screening Scale for Anxiety and Depression: The PHQ–4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, B.; Evans-Lacko, S.; London, J.; Rhydderch, D.; Henderson, C.; Thornicroft, G. Anti-stigma training for medical students: The Education Not Discrimination project. Br. J. Psychiatry Suppl. 2013, 55 (Suppl S55), s89–s94. [Google Scholar] [CrossRef] [Green Version]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69. [Google Scholar] [CrossRef]
- Kröll, C.; Doebler, P.; Nüesch, S. Meta-analytic evidence of the effectiveness of stress management at work. Eur. J. Work. Organ. Psychol. 2017, 26, 677–693. [Google Scholar] [CrossRef]
- Holman, D. Stress Management Interventions: Improving Subjective Psychological Well-Being in the Workplace; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Nabe-Nielsen, K.; Persson, R.; Nielsen, K.; Olsen, O.; Carneiro, I.G.; Garde, A.H. Perspectives on Randomization and Readiness for Change in a Workplace Intervention Study. In Derailed Organizational Interventions for Stress and Well-Being: Confessions of Failure and Solutions for Success; Karanika-Murray, M., Biron, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 201–208. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intervention Group (n = 30) | Control Group (n = 40) | p | |
|---|---|---|---|
| Age M (SD) | 48.17 (8.17) | 47.68 (9.25) | 0.818 |
| Male gender n (%) | 29 (96.7%) | 37 (92.5%) | 0.457 |
| Underage children M (SD) | 0.97 (1.07) | 1.24 (1.02) | 0.286 |
| High school diploma or comparable% | 60.0% | 57.5.% | 0.834 |
| Company site | 14/16 | 21/18 | 0.554 |
| Position 1 | 0.902 | ||
| A n (%) | 5 (16.7%) | 6 (15.0%) | ns. |
| B n (%) | 13 (43.3%) | 19 (47.5%) | ns. |
| C n (%) | 5 (16.7%) | 7 (17.5%) | ns. |
| D n (%) | 7 (23.3%) | 8 (20.0%) | ns. |
| MDNT1 (IQR) | MDNT2 (IQR) | U | p | |||
|---|---|---|---|---|---|---|
| IG | WG | IG | WG | |||
| ERI-Effort 1 | 15.00 (14.00;18.00) | 16.00 (14.25;19.00) | 17.00 (14.00;20.00) | 16.00 (14.00;19.75) | 459.00 | 0.183 |
| ERI-Reward 2 | 48.00 (39.00;43.00) | 50.00 (39.50;54.00) | 45.00 (33.75;53.00) | 51.00 (40.00;53.00) | 478.50 | 0.389 |
| PHQ-4 3 | 1.00 (0.00;2.00) | 1.50 (1.00;3.00) | 1.00 (0.00;3.00) | 1.50 (0.25;3.00) | 545.00 | 0.382 |
| SoDi 4 | 0.80 (0.40;1.55) | 0.80 (0.20;1.50) | 0.80 (0.40;1.20) | 0.80 (0.40;1.55) | 524.50 | 0.365 |
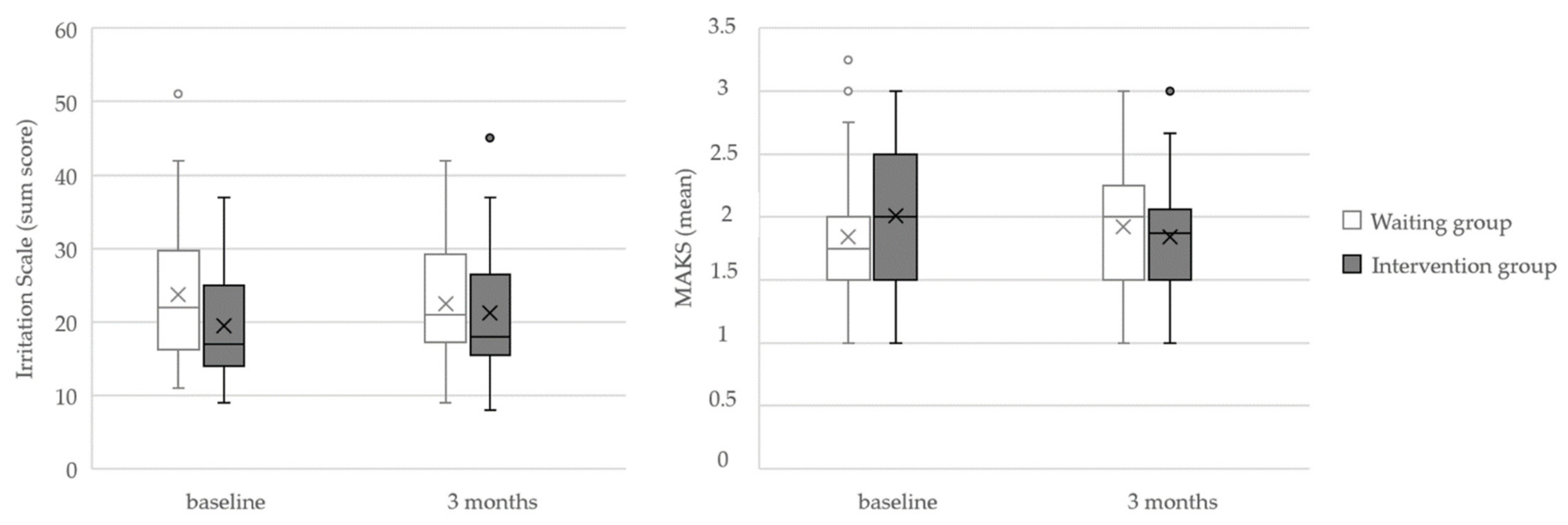
| MAKS 5 | 2.00 (1.50;2.31) | 1.75 (1.50; 1.75) | 1.75 (1.50;2.25) | 2.00 (1.50;2.25) | 417.00 | 0.040 * |
| PSS 6 | 3.00 (2.00;5.00) | 4.00 (3.00;6.00) | 4.00 (2.00;6.00) | 4.00 (3.00;6.00) | 439.00 | 0.051 |
| IS-8 7 | 17.50 (14.00;24.00) | 22.00 (16.50;29.50) | 20.00 (16.00;28.50) | 21.00 (17.25;30.00) | 371.50 | 0.011 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gast, M.; Lehmann, J.; Schwarz, E.; Hirning, C.; Hoelzer, M.; Guendel, H.; Balint, E.M. A Single-Day Training for Managers Reduces Cognitive Stigma Regarding Mental Health Problems: A Randomized Trial. Int. J. Environ. Res. Public Health 2022, 19, 4139. https://doi.org/10.3390/ijerph19074139
Gast M, Lehmann J, Schwarz E, Hirning C, Hoelzer M, Guendel H, Balint EM. A Single-Day Training for Managers Reduces Cognitive Stigma Regarding Mental Health Problems: A Randomized Trial. International Journal of Environmental Research and Public Health. 2022; 19(7):4139. https://doi.org/10.3390/ijerph19074139
Chicago/Turabian StyleGast, Michael, Janina Lehmann, Elena Schwarz, Christian Hirning, Michael Hoelzer, Harald Guendel, and Elisabeth Maria Balint. 2022. "A Single-Day Training for Managers Reduces Cognitive Stigma Regarding Mental Health Problems: A Randomized Trial" International Journal of Environmental Research and Public Health 19, no. 7: 4139. https://doi.org/10.3390/ijerph19074139