
Impact of Fortified Infant Cereals on the Burden of Iron Deficiency Anemia in 6- to 23-Month-Old Indonesian Infants and Young Children: A Health Economic Simulation Model

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
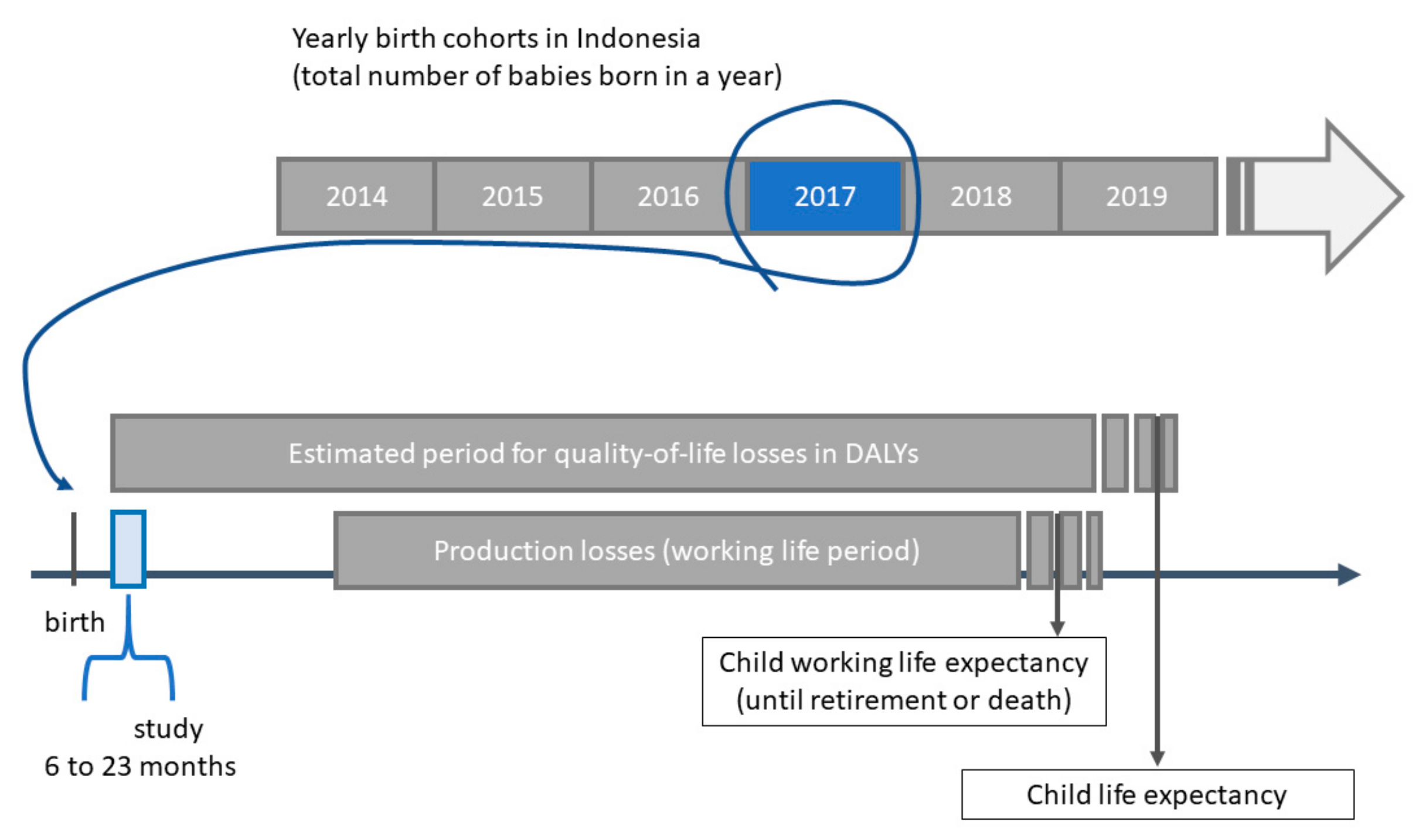
2.1. Data Source and Study Population
2.2. Estimating the Burden of IDA and the Effect of Fortified Infant Cereals
2.3. Costs of the Health Consequences of IDA
2.4. Sensitivity Analysis
3. Results
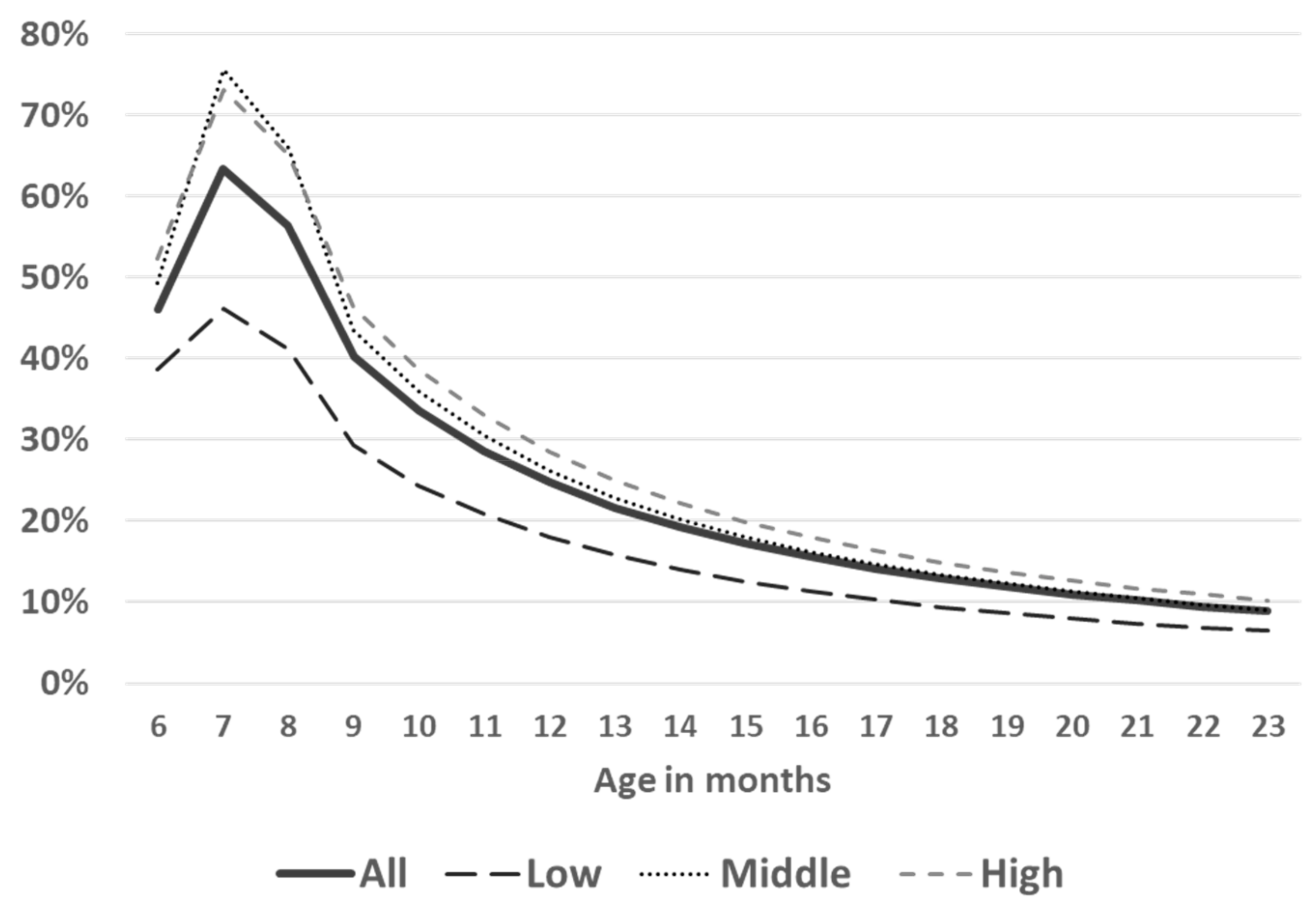
3.1. Baseline Hb Levels and Prevalence of IDA in the Study Sample
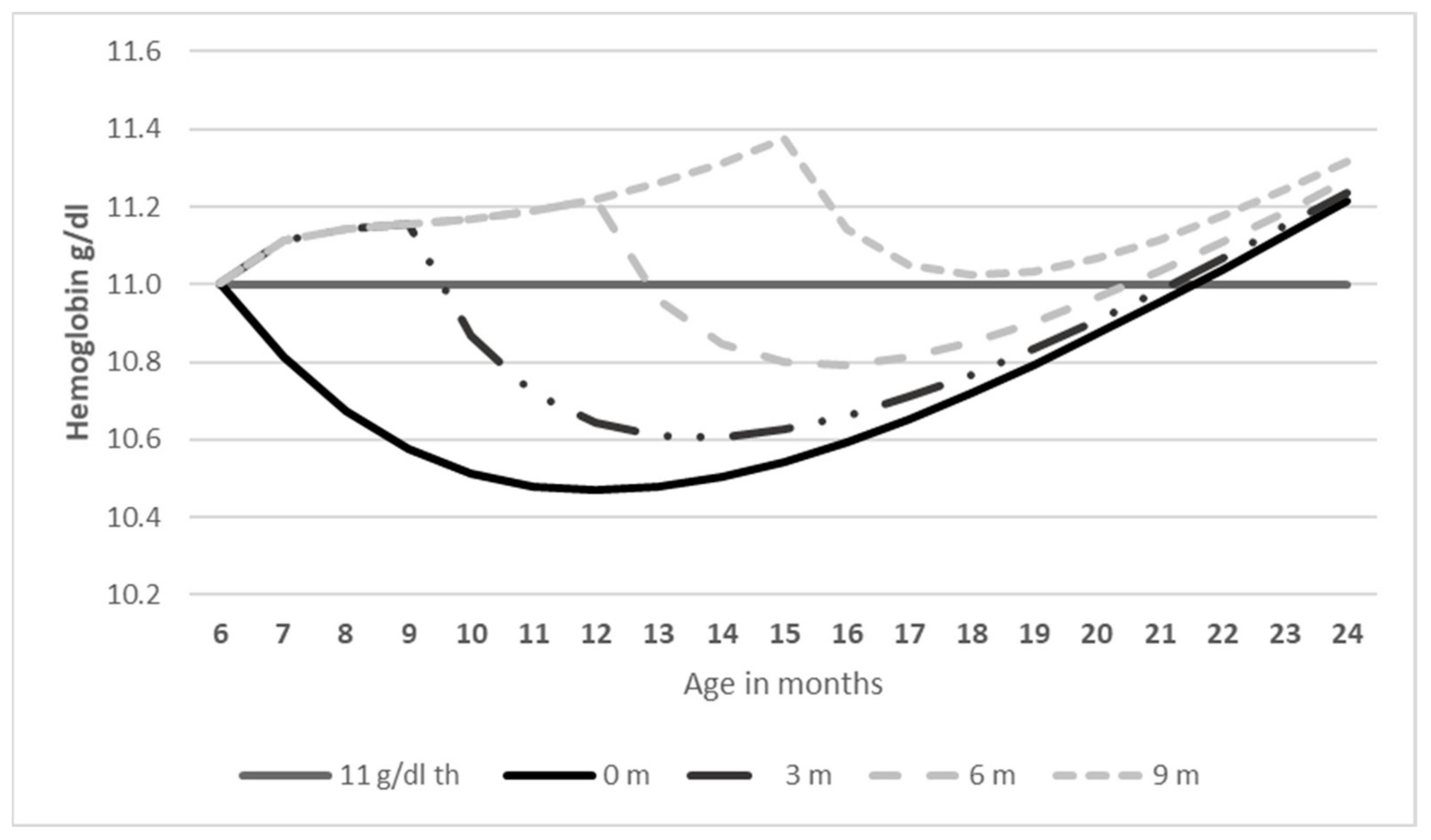
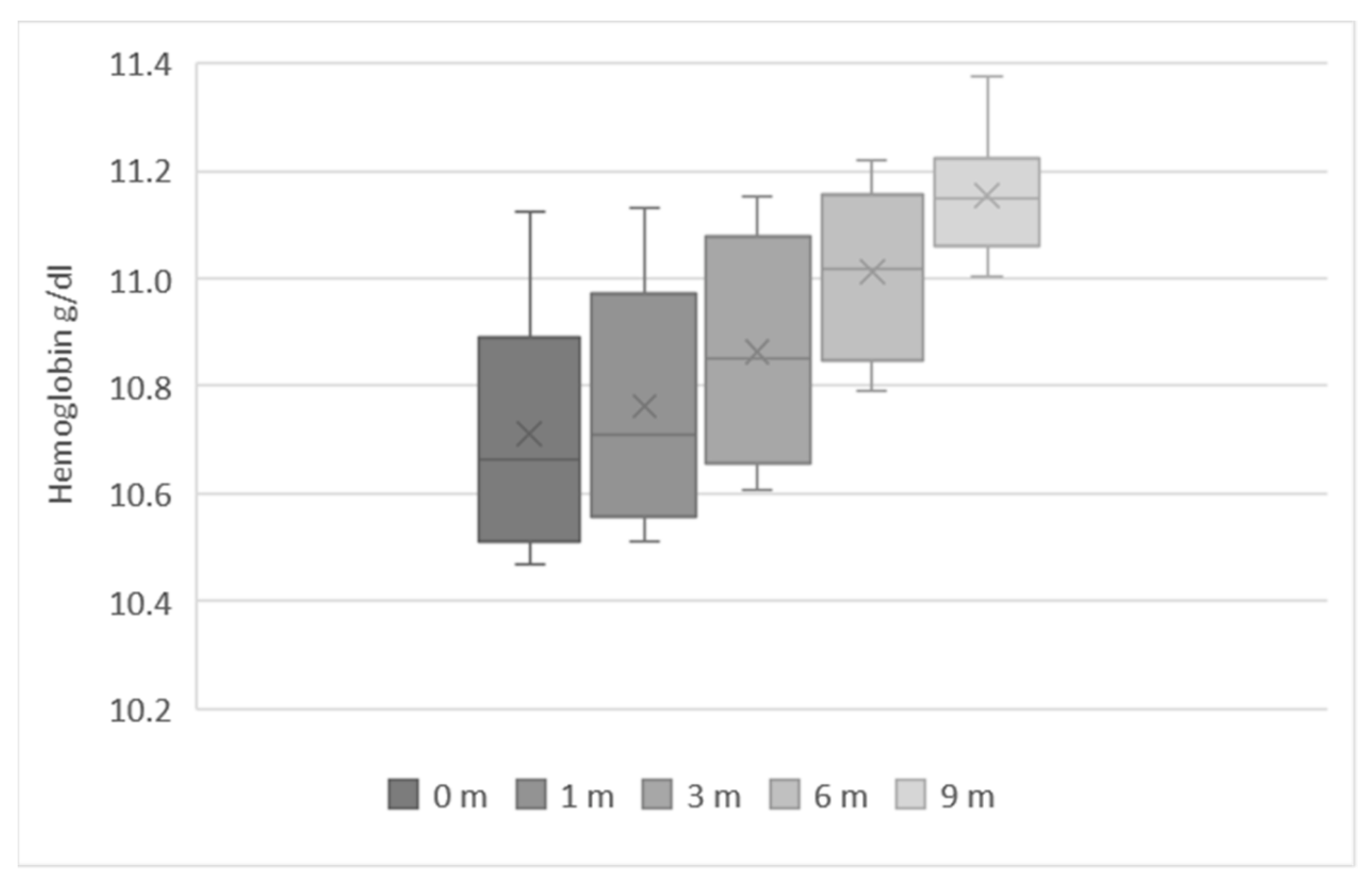
3.2. Estimated Level and Duration of Consumption of Fortified Infant Cereals in 6 to 23-Month-Old Indonesian Children
3.3. Increasing the Consumption of Fortified Infant Cereals: Effects on IDA
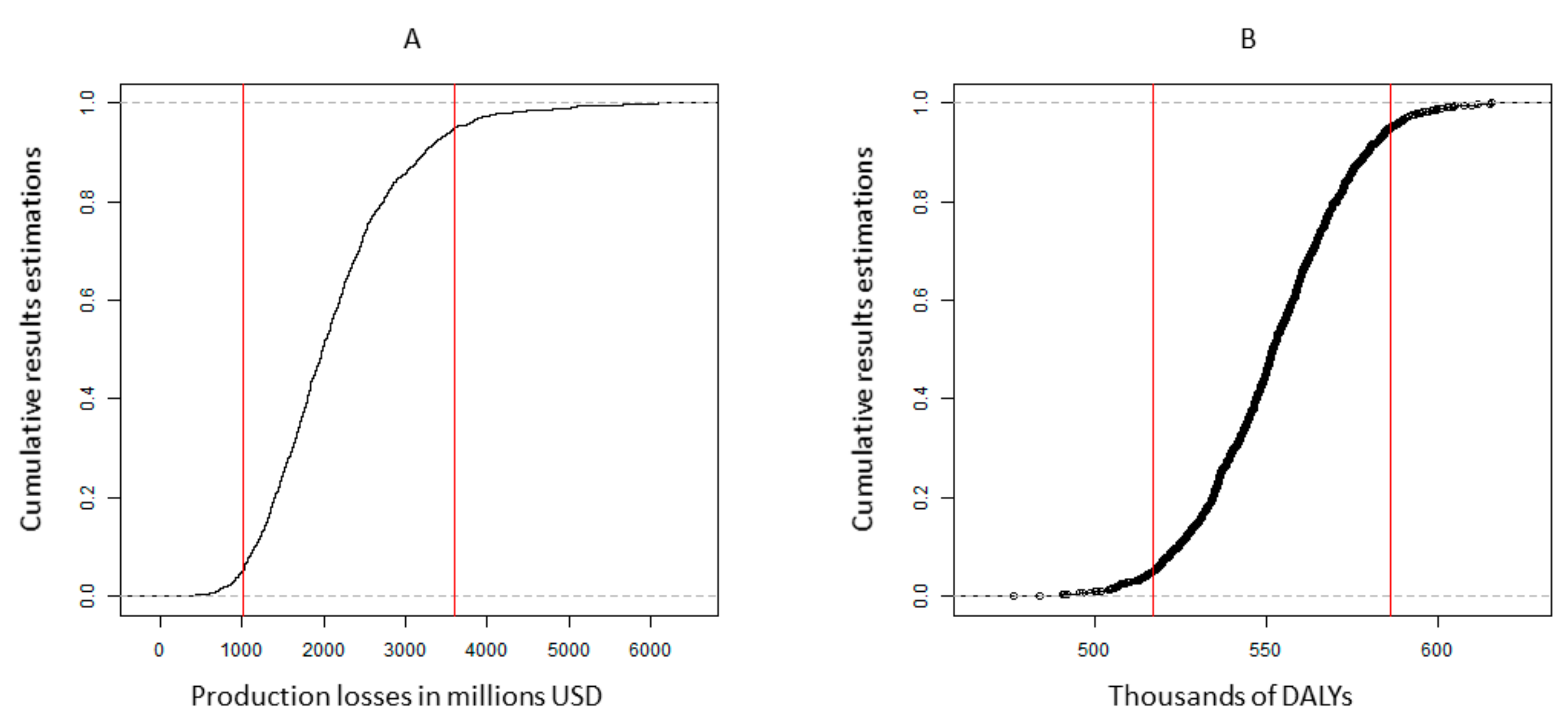
3.4. Probabilistic Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Additional Information on the Model Estimation

Appendix B. Model Parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Baseline Values | 95% CI | Distribution | References |
|---|---|---|---|---|
| Share of anemia due to IDA in preschool age children | 64% | (0.57:0.70) | Beta | Kassebaum, et al. [11] |
| Health consequences of IDA | ||||
| Relative risk of mortality | 2.19 | (1.68:3.36) | Lognormal | Brabin, et al. [46] |
| IQ loss due to IDA (points) | 9 | (5.1:13.4) | Gamma | Lozoff, et al. [47] |
| Reduced physical activity (tiredness/irritability) | 1 | Murray, et al. [48] |
| Disability Weight | Baseline Values | 95% CI | Distribution | References |
|---|---|---|---|---|
| Anemia mild | 0.005 | (0.002:0.023) | Beta | Wieser et al. Murray et al. [31,48] |
| Anemia moderate | 0.058 | (0.038:0.086) | Beta | |
| Anemia severe | 0.164 | (0.112:0.228) | Beta | |
| Intellectual disability mild | 0.031 | (0.018:0.049) | Beta | |
| Intellectual disability moderate | 0.08 | (0.053:0.114) | Beta |
| Parameters | Baseline Values | 95% CI | Distribution | References |
|---|---|---|---|---|
| Life expectancy (years) | 71.1 | (68.8:73.4) | Gamma | World Bank [49] |
| Working life begins (years) | 17 | (14.5:19.1) | Gamma | World Bank [49] |
| Working life ends (years) | 65 | (60.6:71.4) | Gamma | World Bank [49] |
| Labor force participation % | 55 | (0.497:0.571) | Beta | World Bank [49] |
| Projected income growth % | 3.5 | (0.039:0.031) | Normal | World Bank [49] |
| Interest rate % | 3 | (0.034:0.026) | Normal | Smith [50] |
| Mean monthly wage in USD | 255 | (215:283) | Gamma | World Bank [49] |
| Impact of IQ losses on wages % | 8 | (0.05:0.01) | Beta | Psacharopoulos [51] |
| Intergenerational income correlation | 0.55 | (0.50:0.59) | Beta | Black, Solon [52,53] |
| Parameter | Value | 95% CI | Reference |
|---|---|---|---|
| Recommended nutrient intakes (RNIs) and fortification | |||
| RNI iron 6–23M in mg/day | 7.2–11 | WHO/FAO [54] | |
| Iron (mg) per serving in fortified infant cereals | 5 | Nestle | |
| Increase in hemoglobin due to additional iron intake | |||
| Δ Hb g/L in from fortified infant cereals 3 months one serving | Based on Eichler K et al. [18] | ||
| Δ Hb g/L in from fortified infant cereals 3 months two servings | |||
| Δ Hb g/L in from fortified infant cereals 3 months three servings |
References
- Petry, N.; Olofin, I.; Hurrell, R.F.; Boy, E.; Wirth, J.P.; Moursi, M.; Angel, M.D.; Rohner, F. The Proportion of Anemia Associated with Iron Deficiency in Low, Medium, and High Human Development Index Countries: A Systematic Analysis of National Surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). The Global Prevalence of Anemia in 2011; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Cappellini, M.D.; Musallam, K.M.; Taher, A.T. Iron deficiency anaemia revisited. J. Intern. Med. 2020, 287, 153–170. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.M.; Leon, J.S.; Suchdev, P.S. Identification, prevention and treatment of iron deficiency during the first 1000 days. Nutrients 2014, 6, 4093–4114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandjaja, S.; Budiman, B.; Harahap, H.; Ernawati, F.; Soekatri, M.; Widodo, Y.; Sumedi, E.; Rustan, E.; Sofia, G.; Syarief, S.N.; et al. Food consumption and nutritional and biochemical status of 0·5-12-year-old Indonesian children: The SEANUTS study. Br. J. Nutr. 2013, 110, S11–S20. [Google Scholar] [CrossRef] [Green Version]
- Burke, R.M.; Rebolledo, P.A.; Aceituno, A.M.; Revollo, R.; Iñiguez, V.; Klein, M.; Drews-Botsch, C.; Leon, J.S.; Suchdev, P.S. Effect of infant feeding practices on iron status in a cohort study of Bolivian infants. BMC Pediatr. 2018, 18, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; Pelaez, C.; et al. Appropriate age range for introduction of complementary feeding into an infant’s diet. EFSA J. 2019, 17, e05780. [Google Scholar]
- Dewey, K.G. Nutrition, growth, and complementary feeding of the breastfed infant. Ped. Clin. North Am. 2001, 48, 87–104. [Google Scholar] [CrossRef]
- Krebs, N.F. Food Based Complementary Feeding Strategies for Breastfed Infants: What’s the Evidence that it Matters? Nutr. Today 2014, 49, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Kurniawan, Y.A.; Muslimatun, S.; Achadi, E.L.; Sastroamidjojo, S. Anaemia and iron deficiency anaemia among young adolescent girls from the peri urban coastal area of Indonesia. Asia Pac. J. Clin. Nutr. 2006, 15, 350–356. [Google Scholar]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014, 123, 615–624. [Google Scholar] [CrossRef]
- Fahmida, U.; Santika, O. Development of complementary feeding recommendations for 12-23-month-old children from low and middle socio-economic status in West Java, Indonesia: Contribution of fortified foods towards meeting the nutrient requirement. Br. J. Nutr. 2016, 116, S8–S15. [Google Scholar] [CrossRef] [Green Version]
- Santika, O.; Fahmida, U.; Ferguson, E.L. Development of food-based complementary feeding recommendations for 9- to 11-month-old peri-urban Indonesian infants using linear programming. J. Nutr. 2009, 139, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Bolcato, M.; Russo, M.; Trentino, K.; Isbister, J.; Rodrguez, D.; Aprile, A. Patient blood management: The best approach to transfusion medicine risk management. Transfus. Apher. Sci. 2020, 59, 102779. [Google Scholar] [CrossRef]
- Mannar, V.; Gallego, E.B. Iron fortification: Country level experiences and lessons learned. J. Nutr. 2002, 132, 856S–858S. [Google Scholar] [CrossRef] [Green Version]
- Indonesian Food and Drug Administration (BPOM). Indonesian FDA Regulation no 24 Year 2020 on Monitoring of Food Products for Medical Purposes; BPOM: Jakarta, Indonesia, 2020. [Google Scholar]
- Finn, K.; Callen, C.; Bhatia, J.; Reidy, K.; Bechard, L.J.; Carvalho, R. Importance of Dietary Sources of Iron in Infants and Toddlers: Lessons from the FITS Study. Nutrients 2017, 9, 733. [Google Scholar] [CrossRef] [Green Version]
- Eichler, K.; Wieser, S.; Rüthemann, I.; Brügger, U. Effects of micronutrient fortified milk and cereal food for infants and children: A systematic review. BMC Public Health 2012, 12, 506. [Google Scholar] [CrossRef] [Green Version]
- Nicklas, T.A.; O’Neil, C.E.; Fulgoni, V.L. Nutrient intake, introduction of baby cereals and other complementary foods in the diets of infants and toddlers from birth to 23 months of age. AIMS Public Health 2020, 7, 123–147. [Google Scholar] [CrossRef]
- Ziegler, E.E.; Fomon, S.J.; Nelson, S.E.; Jeter, J.M.; Theuer, R.C. Dry cereals fortified with electrolytic iron or ferrous fumarate are equally effective in breast-fed infants. J. Nutr. 2011, 141, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Atkins, L.A.; McNaughton, S.A.; Campbell, K.J.; Szymlek-Gay, E.A. Iron intakes of Australian infants and toddlers: Findings from the Melbourne Infant Feeding, Activity and Nutrition Trial (InFANT) Program. Br. J. Nutr. 2016, 115, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Fotedar, A.; Bhasin, J.S.; Chakravarty, A.; Kulkarni, A.; Bhalla, G.; Anwar, F.; Rao, S. Effectiveness of iron-fortified infant cereals on hemoglobin levels of children aged 12–24 months: A cross-sectional study from New Delhi, India. J. Fam. Med. Prim. Care 2018, 7, 77–80. [Google Scholar]
- Awasthi, S.; Reddy, N.U.; Mitra, M.; Singh, S.; Ganguly, S.; Jankovic, I.; Grathwohl, D.; Cercamondi, C.I.; Ghosh, A. Micronutrient-fortified infant cereal improves Hb status and reduces iron-deficiency anaemia in Indian infants: An effectiveness study. Br. J. Nutr. 2020, 123, 780–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidsson, L.; Sarker, S.A.; Jamil, K.A.; Sultana, S.; Hurrell, R. Regular consumption of a complementary food fortified with ascorbic acid and ferrous fumarate or ferric pyrophosphate is as useful as ferrous sulfate in maintaining hemoglobin concentrations >105 g/L in young Bangladeshi children. Am. J. Clin. Nutr. 2009, 89, 1815–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glinz, D.; Wegmüller, R.; Ouattara, M.; Diakité, V.G.; Aaron, G.J.; Hofer, L.; Zimmermann, M.B.; Adiossan, L.G.; Utzinger, J.; N’goran, E.K.; et al. Iron Fortified Complementary Foods Containing a Mixture of Sodium Iron EDTA with Either Ferrous Fumarate or Ferric Pyrophosphate Reduce Iron Deficiency Anemia in 12- to 36-Month-Old Children in a Malaria Endemic Setting: A Secondary Analysis of a Cluster-Randomized Controlled Trial. Nutrients 2017, 9, 759. [Google Scholar]
- Phu, P.V.; Hoan, N.V.; Salvignol, B.; Treche, S.; Wieringa, F.T.; Khan, N.C.; Tuong, P.D.; Berger, J. Complementary foods fortified with micronutrients prevent iron deficiency and anemia in Vietnamese infants. J. Nutr. 2010, 140, 2241–2247. [Google Scholar]
- Egayanti, Y.; Sri Palupi, N.; Prangdimurti, E. Profile of complementary food consumption during the first year of life based on Indonesian Individual Food Consumption Survey 2014. Mal. J. Nutr. 2018, 24, 53–61. [Google Scholar]
- Strauss, J.; Witoelar, F.; Sikoki, B. The Fifth Wave of the Indonesia Family Life Survey: Overview and Field Report; RAND Corporation: Santa Monica, CA, USA, 2016; Volume 1. [Google Scholar]
- National Population and Family Planning Board (BKKBN); Statistics Indonesia (BPS); Ministry of Health (Kemenkes); ICF. Indonesia Demographic and Health Survey 2017; BKKBN: Jakarta, Indonesia; BPS: Jakarta, Indonesia; Kemenkes: Jakarta, Indonesia; ICF: Jakarta, Indonesia, 2018. [Google Scholar]
- Wieser, S.; Brunner, B.; Tzogiou, C.; Plessow, R.; Zimmermann, M.B.; Farebrother, J.; Soofi, S.; Bhatti, Z.; Ahmed, I.; Bhutta, Z.A. Societal Costs of Micronutrient Deficiencies in 6- to 59-month-old Children in Pakistan. Food Nutr. Bull. 2017, 38, 485–500. [Google Scholar] [CrossRef] [Green Version]
- Wieser, S.; Plessow, R.; Eichler, K.; Malek, O.; Capanzana, M.V.; Agdeppa, I.; Bruegger, U. Burden of micronutrient deficiencies by socio-economic strata in children aged 6 months to 5 years in the Philippines. BMC Public Health 2013, 13, 1167. [Google Scholar] [CrossRef] [Green Version]
- Ekowati, I.N.; Nestle Indonesia. Internal Summary Sales Report Consumer Research Nestle Indonesia. 2020; unpublished data. [Google Scholar]
- Fahmida, U.; Kolopaking, R.; Santika, O.; Sriani, S.; Umar, J.; Htet, M.K.; Ferguson, E. Effectiveness in improving knowledge, practices, and intakes of “key problem nutrients” of a complementary feeding intervention developed by using linear programming: Experience in Lombok, Indonesia. Am. J. Clin. Nutr. 2015, 101, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.R.; Morris, S.S.; Sachdev, H.P.S.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef]
- Gould, J.F. Complementary Feeding, Micronutrients and Developmental Outcomes of Children. Nestle. Nutr. Inst. Workshop Ser. 2017, 87, 13–28. [Google Scholar]
- Dewey, K.G.; Adu-Afarwuah, S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern. Child Nutr. 2008, 4 (Suppl. 1), 24–85. [Google Scholar] [CrossRef]
- Dewey, K.G.; Brown, K.H. Update on technical issues concerning complementary feeding of young children in developing countries and implications for intervention programs. Food Nutr. Bull. 2003, 24, 5–28. [Google Scholar] [CrossRef] [Green Version]
- Prieto-Patron, A.; Van der Horst, K.; Hutton, Z.V.; Detzel, P. Association between Anaemia in Children 6 to 23 Months Old and Child, Mother, Household and Feeding Indicators. Nutrients 2018, 10, 1269. [Google Scholar] [CrossRef] [Green Version]
- Faber, M.; Kvalsvig, J.D.; Lombard, C.J.; Benadé, A.J. Effect of a fortified maize-meal porridge on anemia, micronutrient status, and motor development of infants. Am. J. Clin. Nutr. 2005, 82, 1032–1039. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, A.; Madanijah, S.; Dwiriani, C.M.; Kolopaking, R. Complementary feeding practices and nutritional status of children 6-23 months old: Formative study in Aceh, Indonesia. Nutr. Res. Pract. 2018, 12, 512–520. [Google Scholar] [CrossRef]
- Fahmida, U.; Santika, O.; Kolopaking, R.; Ferguson, E. Complementary feeding recommendations based on locally available foods in Indonesia. Food Nutr. Bull. 2014, 35, S174–S179. [Google Scholar] [CrossRef] [Green Version]
- Kartika, H.H.; Gurnida, D.A.; Primadi, A. Comparison of Hemoglobin level in infants fed with factory made and home made complementary food. Sari Pediatri. 2019, 20, 276–282. [Google Scholar] [CrossRef]
- WHO/UNICEF. Global Strategy for Infant and Young Child Feeding. Geneva. 2003. Available online: https://www.who.int/publications/i/item/9241562218?msclkid=3996d55fc60311ec84d87785d6646b29 (accessed on 20 February 2021).
- Moench-Pfanner, R.; Van Ameringen, M. The Global Alliance for Improved Nutrition (GAIN): A decade of partnerships to increase access to and affordability of nutritious foods for the poor. Food Nutr. Bull. 2012, 33, S373–S380. [Google Scholar] [CrossRef] [Green Version]
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S. How many child deaths can we prevent this year? Lancet 2003, 362, 65–71. [Google Scholar] [CrossRef]
- Brabin, B.J.; Premji, Z.; Verhoeff, F. An analysis of anemia and child mortality. J. Nutr. 2001, 131, 636S–645S, discussion 646S–648S. [Google Scholar] [CrossRef]
- Lozoff, B.; Jimenez, E.; Smith, J.B. Double burden of iron deficiency in infancy and low socioeconomic status: A longitudinal analysis of cognitive test scores to age 19 years. Arch. Pediatr. Adolesc. Med. 2006, 160, 1108–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.J.; Lopez, A.D.; World Health Organization. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; Harvard University Press: Cambridge, MA, USA, 1996. [Google Scholar]
- World Bank, World Development Indicators World Data Bank. 2020. Available online: https://databank.worldbank.org/source/world-development-indicators/preview/on (accessed on 20 July 2020).
- Smith, D.; Gravelle, H. The practice of discounting economic evaluation of health care interventions. In International Journal of Technology Assessment in Health Care; University of York, Centre for Health Economics: York, UK, 2000; pp. 236–243. ISSN 0266-4623. [Google Scholar]
- Psacharopoulos, G.; Patrinos, H.A. Returns to investment in education: A further update. Educ. Econ. 2004, 12, 111–134. [Google Scholar] [CrossRef] [Green Version]
- Black, S.E.; Devereux, P.J. Recent developments in intergenerational mobility. In Handbook of Labor Economics, Vol. 4; O. Ashenfelter, O., Card, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2011; Chapter 16; pp. 1487–1541. [Google Scholar]
- Solon, G. Cross-country differences in intergenerational earnings mobility. J. Econ. Perspect. 2002, 16, 59–66. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization and Food and Agriculture Organization. Vitamin and Mineral Requirements in Human Nutrition: Report of a Joint FAO/WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]






| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Number of births in 2017 (in thousands) * | 436 | 427 | 418 | 413 | 400 | 376 | 371 | 370 | 357 | 355 |
| Average Hb in g/dL children 6 to 23 mo ** | 10.4 | 10.4 | 10.5 | 10.6 | 10.8 | 10.9 | 11.1 | 11.1 | 11.2 | 11.2 |
| Household income distribution *** | 1.92 | 3.21 | 4.23 | 5.18 | 6.28 | 7.6 | 9.29 | 11.6 | 15.9 | 34.8 |
| Production Losses (Millions of U.S. Dollars) | ||||
| Cognitive impairment | Mortality | Total | ||
| With current level of consumption and fortification | 2005.2 | 4.7 | 2009.9 | |
| Without fortification of infant cereals | 2175.3 | 5.3 | 2180.6 | |
| Difference (%) | 170 (8.5%) | 0.6 (13.4%) | 171 (8.5%) | |
| DALYs (thousands) | ||||
| Impaired physical activity | Cognitive impairment | Mortality | Total | |
| With current level of consumption and fortification | 51.9 | 495.5 | 5.5 | 552.9 |
| Without fortification of infant cereals | 56 | 534.1 | 6.2 | 596 |
| Difference (%) | 4 (7.9%) | 39 (7.8%) | 0.7 (12.9%) | 43 (7.9%) |
| Production Losses (Millions of U.S. Dollars) | ||||
|---|---|---|---|---|
| Cognitive impairment | Mortality | Total | ||
| Current consumption | 2005.2 | 4.7 | 2009.9 | |
| Increased duration of consumption | 1968.7 | 4.6 | 1973 | |
| Difference (%) | 37 (1.8%) | 0.1 (2.8%) | 37 (1.8%) | |
| DALYs (thousands) | ||||
| Impaired physical ability | Cognitive impairment | Mortality | Total | |
| Current consumption | 51.9 | 495.5 | 5.5 | 552.9 |
| Increased duration of consumption | 51 | 487.2 | 5.4 | 543.6 |
| Difference (%) | 0.9 (1.7%) | 8.3 (1.7%) | 0.1 (2.5%) | 9.3 (1.7%) |
| If the Lowest Wealth Tertile Had a Similar Consumption Level as the Middle Tertile | ||||
| Production Losses (Millions of U.S. Dollars) | ||||
| Cognitive impairment | Mortality | Total | ||
| Current consumption | 752.3 | 3.8 | 756.1 | |
| Increased consumption level | 725.1 | 3.4 | 728.6 | |
| Difference (%) | 27.2 (3.6%) | 0.4 (9.7%) | 27.6 (3.6%) | |
| DALYs (in thousands) | ||||
| Impaired physical activity | Cognitive impairment | Mortality | Total | |
| Current consumption | 23.9 | 231 | 4.7 | 259.6 |
| Increased consumption level | 23 | 222 | 4.2 | 249.2 |
| Difference (%) | 0.9 (3.9%) | 9 (3.9%) | 0.5 (10.0%) | 10 (4.0%) |
| If the lowest wealth tertile had a similar consumption level as the middle tertile and increased duration of consumption | ||||
| Production losses (millions of U.S. dollars) | ||||
| Cognitive impairment | Mortality | Total | ||
| Current consumption | 752.3 | 3.8 | 756.1 | |
| Increased consumption level and duration | 719.4 | 3.4 | 722.8 | |
| Difference (%) | 32.9 (4.4%) | 0.4 (11.5%) | 33.3 (4.4%) | |
| DALYs (in thousands) | ||||
| Impaired physical ability | Cognitive impairment | Mortality | Total | |
| Current consumption | 23.9 | 231 | 4.7 | 259.6 |
| Increased consumption level and duration | 22.8 | 220.2 | 4.1 | 247.1 |
| Difference (%) | 1.1 (4.7%) | 10.8 (4.7%) | 0.6 (11.8%) | 12.5 (4.8%) |
| Production Losses (Millions of U.S. Dollars) | ||||
|---|---|---|---|---|
| Cognitive impairment | Mortality | Total | ||
| Current consumption | 2 005.2 | 4.7 | 2 009.9 | |
| Two servings per day | 1 844.5 | 4.1 | 1 848.7 | |
| Difference (%) | 161 (8.0%) | 1 (11.7%) | 161 (8.0%) | |
| DALYs (in thousands) | ||||
| Impaired physical ability | Cognitive impairment | Mortality | Total | |
| Current consumption | 51.9 | 495.5 | 5.5 | 552.9 |
| Two servings per day | 48.1 | 458.9 | 4.9 | 511.9 |
| Difference (%) | 3.8 (7.4%) | 36.6 (7.4%) | 0.6 (11.4%) | 41 (7.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prieto-Patron, A.; Detzel, P.; Ramayulis, R.; Sudikno; Irene; Wibowo, Y. Impact of Fortified Infant Cereals on the Burden of Iron Deficiency Anemia in 6- to 23-Month-Old Indonesian Infants and Young Children: A Health Economic Simulation Model. Int. J. Environ. Res. Public Health 2022, 19, 5416. https://doi.org/10.3390/ijerph19095416
Prieto-Patron A, Detzel P, Ramayulis R, Sudikno, Irene, Wibowo Y. Impact of Fortified Infant Cereals on the Burden of Iron Deficiency Anemia in 6- to 23-Month-Old Indonesian Infants and Young Children: A Health Economic Simulation Model. International Journal of Environmental Research and Public Health. 2022; 19(9):5416. https://doi.org/10.3390/ijerph19095416
Chicago/Turabian StylePrieto-Patron, Alberto, Patrick Detzel, Rita Ramayulis, Sudikno, Irene, and Yulianti Wibowo. 2022. "Impact of Fortified Infant Cereals on the Burden of Iron Deficiency Anemia in 6- to 23-Month-Old Indonesian Infants and Young Children: A Health Economic Simulation Model" International Journal of Environmental Research and Public Health 19, no. 9: 5416. https://doi.org/10.3390/ijerph19095416