
The Effect of Capacitive and Resistive Electric Transfer Intervention on Delayed-Onset Muscle Soreness Induced by Eccentric Exercise

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
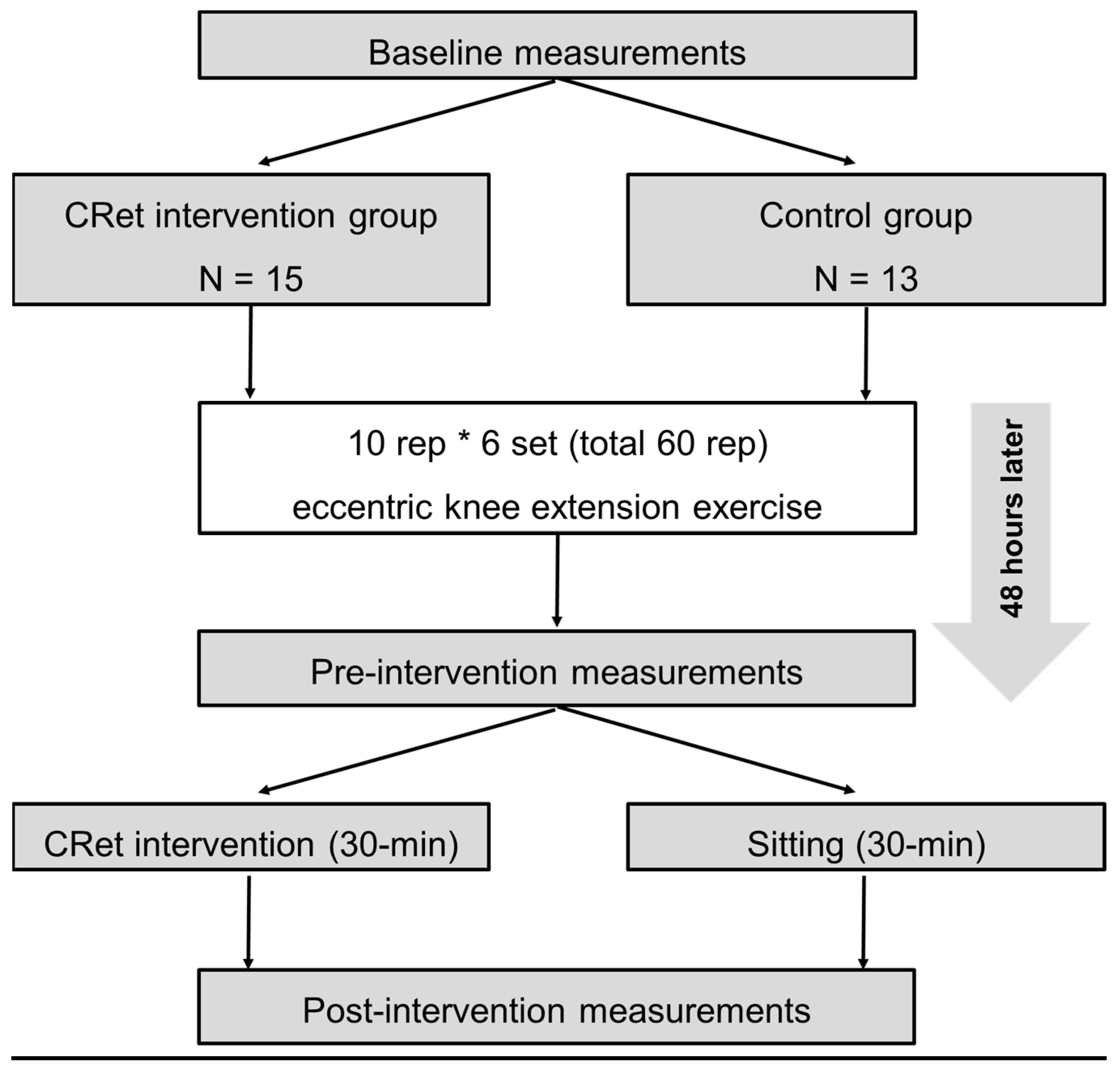
2.2. Experimental Design
2.3. MVC-ISO and MVC-CON
2.4. Knee Flexion ROM
2.5. Muscle Soreness
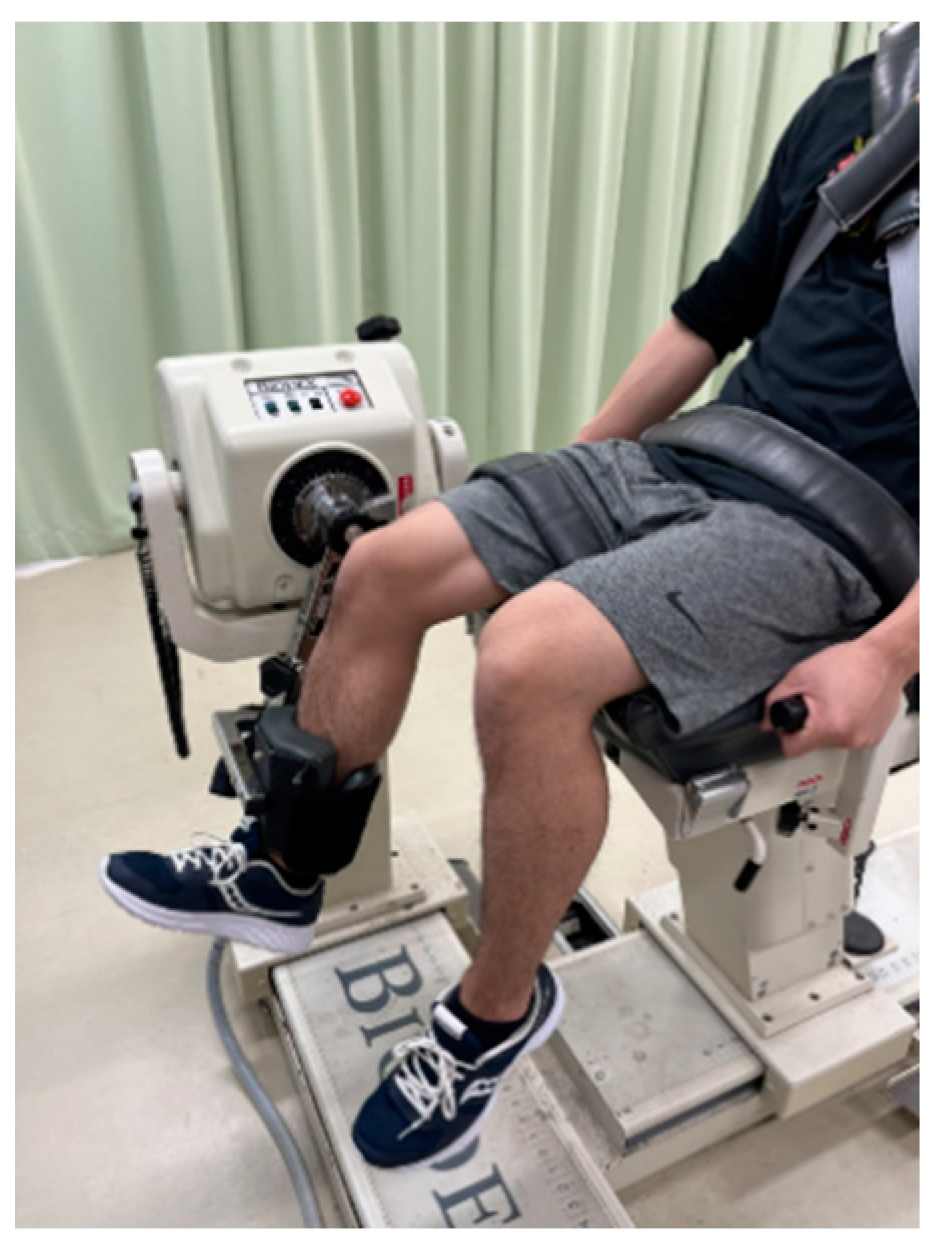
2.6. Eccentric Exercise Task
2.7. CRet Intervention
2.8. Statistical Analysis
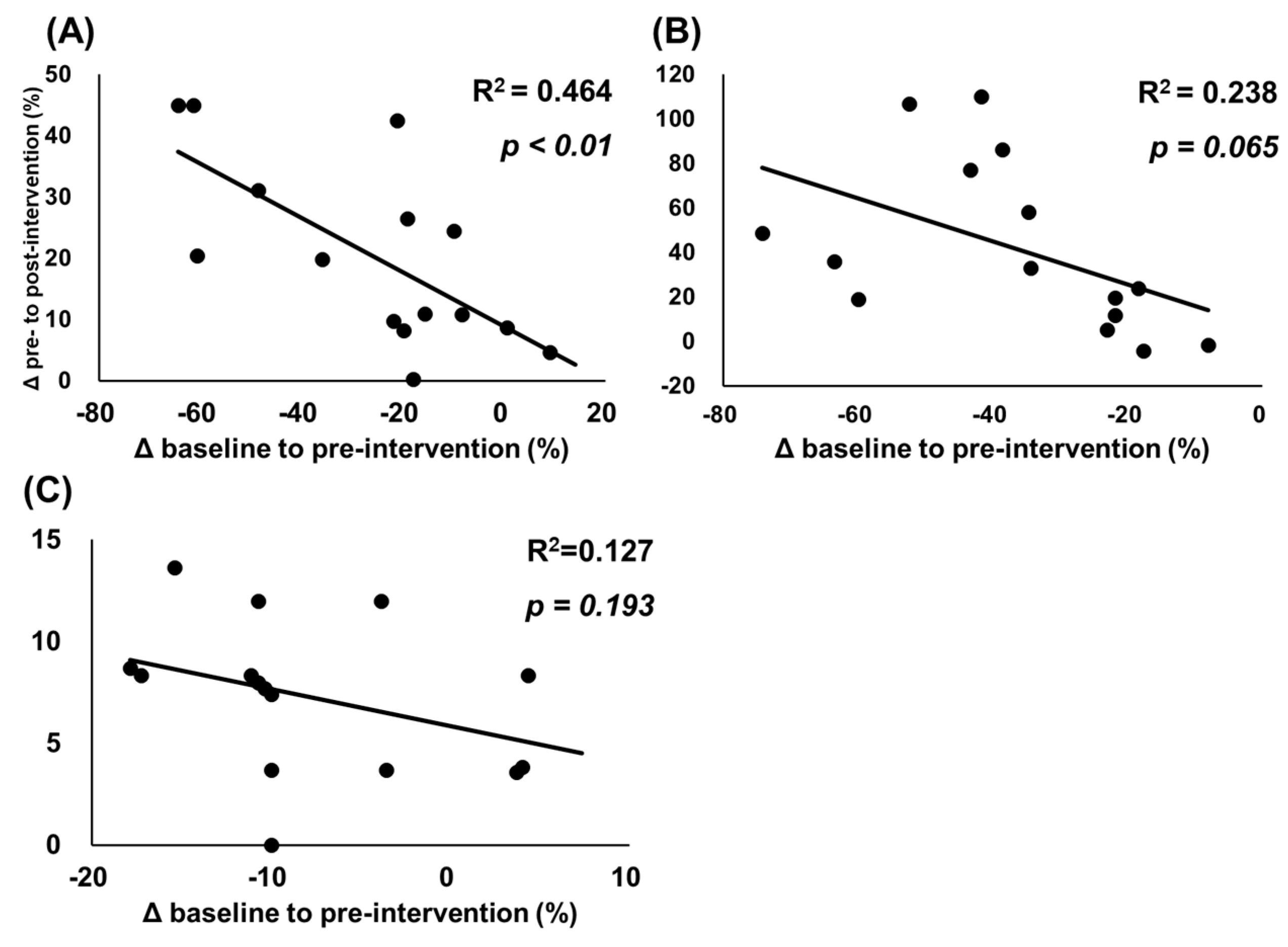
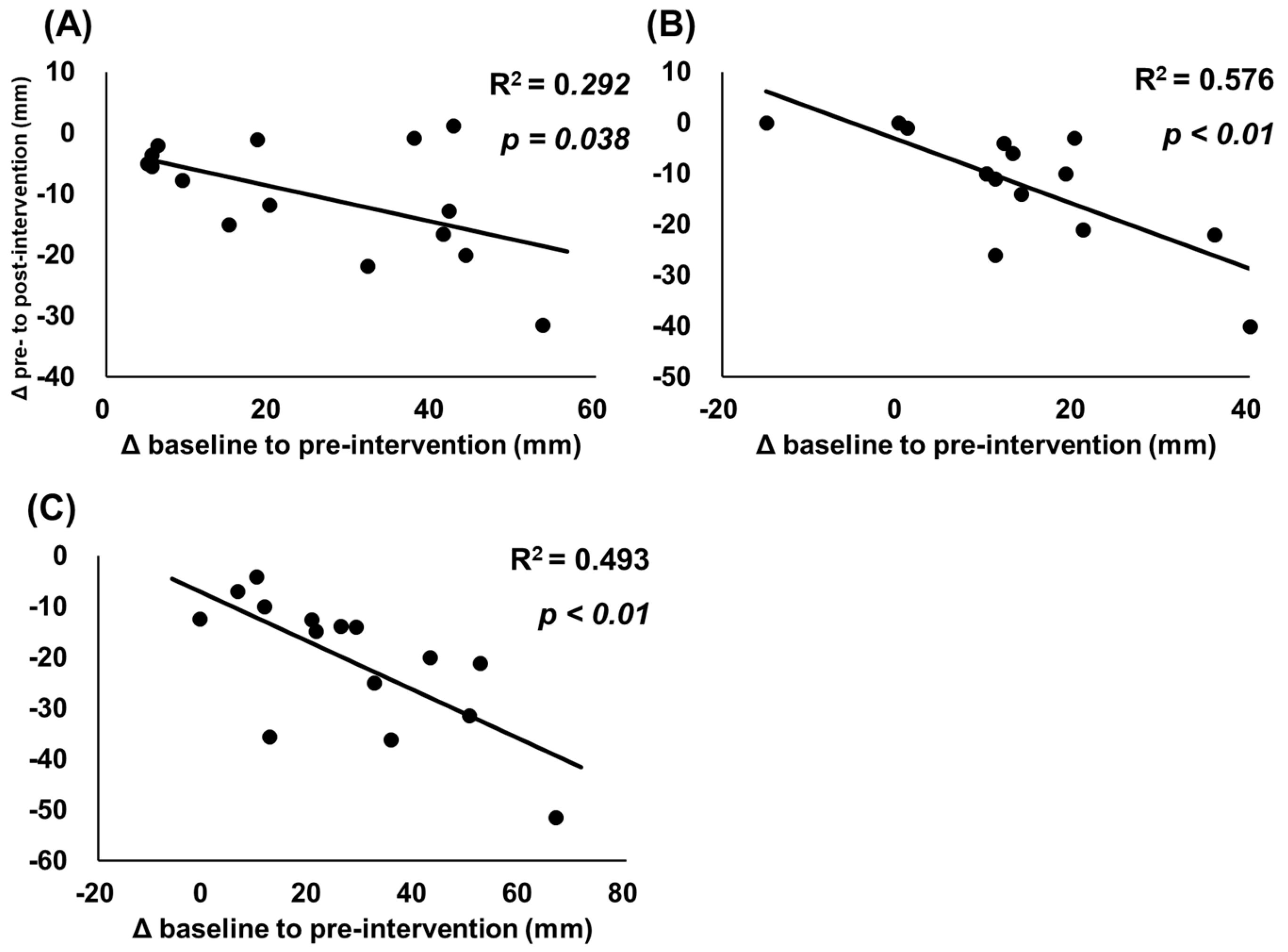
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tseng, W.C.; Nosaka, K.; Tseng, K.W.; Chou, T.Y.; Chen, T.C. Contralateral Effects by Unilateral Eccentric versus Concentric Resistance Training. Med. Sci. Sports Exerc. 2020, 52, 474–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsura, Y.; Takeda, N.; Hara, T.; Takahashi, S.; Nosaka, K. Comparison between eccentric and concentric resistance exercise training without equipment for changes in muscle strength and functional fitness of older adults. Eur. J. Appl. Physiol. 2019, 119, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Chapman, D.; Newton, M.; Sacco, P. Is isometric strength loss immediately after eccentric exercise related to changes in indirect markers of muscle damage? Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2006, 31, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Newton, M.; Sacco, P. Delayed-onset muscle soreness does not reflect the magnitude of eccentric exercise-induced muscle damage. Scand. J. Med. Sci. Sports 2002, 12, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, P.M.; Nosaka, K.; Braun, B. Muscle function after exercise-induced muscle damage and rapid adaptation. Med. Sci. Sports Exerc. 1992, 24, 512–520. [Google Scholar] [CrossRef]
- Cleak, M.J.; Eston, R.G. Delayed onset muscle soreness: Mechanisms and management. J. Sports Sci. 1992, 10, 325–341. [Google Scholar] [CrossRef]
- Armstrong, R.B. Mechanisms of exercise-induced delayed onset muscular soreness: A brief review. Med. Sci. Sports Exerc. 1984, 16, 529–538. [Google Scholar] [CrossRef]
- Dupuy, O.; Douzi, W.; Theurot, D.; Bosquet, L.; Dugué, B. An Evidence-Based Approach for Choosing Post-exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front. Physiol. 2018, 9, 403. [Google Scholar] [CrossRef]
- Wang, Y.; Li, S.; Zhang, Y.; Chen, Y.; Yan, F.; Han, L.; Ma, Y. Heat and cold therapy reduce pain in patients with delayed onset muscle soreness: A systematic review and meta-analysis of 32 randomized controlled trials. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2021, 48, 177–187. [Google Scholar] [CrossRef]
- Matsuo, S.; Suzuki, S.; Iwata, M.; Hatano, G.; Nosaka, K. Changes in force and stiffness after static stretching of eccentrically-damaged hamstrings. Eur. J. Appl. Physiol. 2015, 115, 981–991. [Google Scholar] [CrossRef]
- Yahata, K.; Sato, S.; Kiyono, R.; Inaba, K.; Sutoh, S.; Hiraizumi, K.; Nakamura, M. The acute effect of stretching on eccentrically-damaged muscle: Analysis of differences between Hold 339 relax stretching and modified PNF stretching. Jpn. J. Phys. Fit. Sports Med. 2020, 69, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, D.; Nakamura, M.; Ohya, S.; Aoki, T.; Edama, M. The acute effect of stretching on eccentrically-damaged muscle: Analysis of differences 341 between hold-relax and static stretching. Jpn. J. Phys. Fit. Sports Med. 2019, 68, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, M.; Yasaka, K.; Kiyono, R.; Onuma, R.; Yahata, K.; Sato, S.; Konrad, A. The Acute Effect of Foam Rolling on Eccentrically-Induced Muscle Damage. Int. J. Environ. Res. Public Health 2020, 18, 75. [Google Scholar] [CrossRef]
- Romero-Moraleda, B.; González-García, J.; Cuéllar-Rayo, Á.; Balsalobre-Fernández, C.; Muñoz-García, D.; Morencos, E. Effects of Vibration and Non-Vibration Foam Rolling on Recovery after Exercise with Induced Muscle Damage. J. Sports Sci. Med. 2019, 18, 172–180. [Google Scholar]
- Nakamura, M.; Kasahara, K.; Yoshida, R.; Yahata, K.; Sato, S.; Murakami, Y.; Aizawa, K.; Konrad, A. The Effect of Static Compression via Vibration Foam Rolling on Eccentrically Damaged Muscle. Int. J. Environ. Res. Public Health 2022, 19, 1823. [Google Scholar] [CrossRef] [PubMed]
- Kasahara, K.; Yoshida, R.; Yahata, K.; Sato, S.; Murakami, Y.; Aizawa, K.; Konrad, A.; Nakamura, M. Comparison of the Acute Effects of Foam Rolling with High and Low Vibration Frequencies on Eccentrically Damaged Muscle. J. Sports Sci. Med. 2022, 21, 112–119. [Google Scholar] [CrossRef]
- Kato, S.; Saitoh, Y.; Miwa, N. Repressive effects of a capacitive-resistive electric transfer (CRet) hyperthermic apparatus combined with provitamin C on intracellular lipid-droplets formation in adipocytes. Int. J. Hyperth. 2013, 29, 30–37. [Google Scholar] [CrossRef] [PubMed]
- De Sousa-De Sousa, L.; Tebar Sanchez, C.; Maté-Muñoz, J.L.; Hernández-Lougedo, J.; Barba, M.; Lozano-Estevan, M.D.C.; Garnacho-Castaño, M.V.; García-Fernández, P. Application of Capacitive-Resistive Electric Transfer in Physiotherapeutic Clinical Practice and Sports. Int. J. Environ. Res. Public Health 2021, 18, 12446. [Google Scholar] [CrossRef]
- Yokota, Y.; Sonoda, T.; Tashiro, Y.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Nakayama, Y.; Kawagoe, M.; Shimoura, K.; Tatsumi, M.; et al. Effect of Capacitive and Resistive electric transfer on changes in muscle flexibility and lumbopelvic alignment after fatiguing exercise. J. Phys. Ther. Sci. 2018, 30, 719–725. [Google Scholar] [CrossRef] [Green Version]
- Tashiro, Y.; Hasegawa, S.; Yokota, Y.; Nishiguchi, S.; Fukutani, N.; Shirooka, H.; Tasaka, S.; Matsushita, T.; Matsubara, K.; Nakayama, Y.; et al. Effect of Capacitive and Resistive electric transfer on haemoglobin saturation and tissue temperature. Int. J. Hyperth. 2017, 33, 696–702. [Google Scholar] [CrossRef]
- Bito, T.; Tashiro, Y.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Kawagoe, M.; Sonoda, T.; Nakayama, Y.; Yokota, Y.; Shimoura, K.; et al. Acute effects of capacitive and resistive electric transfer (CRet) on the Achilles tendon. Electromagn. Biol. Med. 2019, 38, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Duñabeitia, I.; Arrieta, H.; Torres-Unda, J.; Gil, J.; Santos-Concejero, J.; Gil, S.M.; Irazusta, J.; Bidaurrazaga-Letona, I. Effects of a capacitive-resistive electric transfer therapy on physiological and biomechanical parameters in recreational runners: A randomized controlled crossover trial. Phys. Ther. Sport 2018, 32, 227–234. [Google Scholar] [CrossRef]
- Coccetta, C.A.; Sale, P.; Ferrara, P.E.; Specchia, A.; Maccauro, G.; Ferriero, G.; Ronconi, G. Effects of capacitive and resistive electric transfer therapy in patients with knee osteoarthritis: A randomized controlled trial. Int. J. Rehabil. Res. 2019, 42, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, Y.; Suzuki, Y.; Nakayama, Y.; Sonoda, T.; Yokota, Y.; Kawagoe, M.; Tsuboyama, T.; Aoyama, T. The effect of Capacitive and Resistive electric transfer on non-specific chronic low back pain. Electromagn. Biol. Med. 2020, 39, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Wachi, M.; Jiroumaru, T.; Satonaka, A.; Ikeya, M.; Oka, Y.; Fujikawa, T. Effect of electromyographic activity using capacitive and resistive electric transfer on non-specific chronic low back pain: A double-blind randomized clinical trial. Electromagn. Biol. Med. 2022, 41, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, R.; Ronconi, G.; Ferrara, P.E.; Salgovic, L.; Vercelli, S.; Solaro, C.; Ferriero, G. Capacitive and resistive electric transfer therapy in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2020, 43, 291–298. [Google Scholar] [CrossRef]
- Chen, T.C.; Nosaka, K.; Sacco, P. Intensity of eccentric exercise, shift of optimum angle, and the magnitude of repeated-bout effect. J. Appl. Physiol. 2007, 102, 992–999. [Google Scholar] [CrossRef]
- Chen, T.C.; Lin, K.Y.; Chen, H.L.; Lin, M.J.; Nosaka, K. Comparison in eccentric exercise-induced muscle damage among four limb muscles. Eur. J. Appl. Physiol. 2011, 111, 211–223. [Google Scholar] [CrossRef]
- Mavropalias, G.; Koeda, T.; Barley, O.R.; Poon, W.C.K.; Fisher, A.J.; Blazevich, A.J.; Nosaka, K. Comparison between high- and low-intensity eccentric cycling of equal mechanical work for muscle damage and the repeated bout effect. Eur. J. Appl. Physiol. 2020, 120, 1015–1025. [Google Scholar] [CrossRef]
- Cohen, J. (Ed.) Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Hillsdale, MI, USA, 1988. [Google Scholar]
- Akiyama, K.; Akagi, R.; Hirayama, K.; Hirose, N.; Takahashi, H.; Fukubayshi, T. Shear Modulus of the Lower Leg Muscles in Patients with Medial Tibial Stress Syndrome. Ultrasound Med. Biol. 2016, 42, 1779–1783. [Google Scholar] [CrossRef]
- Nakamura, M.; Sato, S.; Hiraizumi, K.; Kiyono, R.; Fukaya, T.; Nishishita, S. Effects of static stretching programs performed at different volume-equated weekly frequencies on passive properties of muscle-tendon unit. J. Biomech. 2020, 103, 109670. [Google Scholar] [CrossRef] [PubMed]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology; Prentice Hall Paerson: London, UK, 2007. [Google Scholar]
- McGowan, C.J.; Pyne, D.B.; Thompson, K.G.; Rattray, B. Warm-Up Strategies for Sport and Exercise: Mechanisms and Applications. Sports Med. 2015, 45, 1523–1546. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D. Warm up I: Potential mechanisms and the effects of passive warm up on exercise performance. Sports Med. 2003, 33, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Kramer, J.F. Ultrasound: Evaluation of its mechanical and thermal effects. Arch. Phys. Med. Rehabil. 1984, 65, 223–227. [Google Scholar] [PubMed]
- Lehmann, J.F.; Brunner, G.D.; Stow, R.W. Pain threshold measurements after therapeutic application of ultrasound, microwaves and infrared. Arch. Phys. Med. Rehabil. 1958, 39, 560–565. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | Pre-Intervention | Post-Intervention | Interaction Effect | ||
|---|---|---|---|---|---|
| MVC-ISO (Nm) | CRet group | 154.3 ± 23.1 | 112.1 ± 34.1 * | 132.0 ± 34.8 # | F = 5.44, p < 0.01 |
| Control group | 162.1 ± 22.9 | 98.8 ± 43.7 * | 100.0 ± 34.5 * | ηp2 = 0.179 | |
| MVC-CON (Nm) | CRet group | 164.9 ± 26.7 | 103.6 ± 34.5 * | 141.5 ± 44.7 # | F = 4.70, p = 0.014 |
| Control group | 154.0 ± 19.8 | 82.3 ± 34.3 * | 91.8 ± 34.7 *,# | ηp2 = 0.158 | |
| Knee flexion ROM (°) | CRet group | 138.0 ± 9.6 | 126.7 ± 8.3 * | 135.7 ± 6.3 # | F = 4.21, p = 0.02 |
| Control group | 143.2 ± 8.5 | 136.8 ± 10.9 * | 138.3 ± 10.8 * | ηp2 = 0.144 | |
| Muscle soreness | |||||
| At contraction (mm) | CRet group | 2.2 ± 5.4 | 27.4 ± 15.3 | 17.2 ± 13.4 | F = 1.69, p = 0.195 |
| Control group | 4.9 ± 4.2 | 24.4 ± 12.8 | 23.0 ± 11.5 | ηp2 = 0.063 | |
| At stretching (mm) | CRet group | 25.9 ± 9.1 | 39.4 ± 15.1 | 27.5 ± 13.0 | F = 1.86, p = 0.17 |
| Control group | 34.8 ± 25.0 | 49.8 ± 25.2 | 44.3 ± 26.6 | ηp2 = 0.069 | |
| At palpation (mm) | CRet group | 14.7 ± 10.3 | 45.7 ± 17.3 * | 21.5 ± 14.6 # | F = 5.71, p < 0.01 |
| Control group | 14.7 ± 10.3 | 45.7 ± 17.3 * | 40.4 ± 11.7 * | ηp2 = 0.186 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, M.; Sato, S.; Kiyono, R.; Yahata, K.; Yoshida, R.; Kasahara, K.; Konrad, A. The Effect of Capacitive and Resistive Electric Transfer Intervention on Delayed-Onset Muscle Soreness Induced by Eccentric Exercise. Int. J. Environ. Res. Public Health 2022, 19, 5723. https://doi.org/10.3390/ijerph19095723
Nakamura M, Sato S, Kiyono R, Yahata K, Yoshida R, Kasahara K, Konrad A. The Effect of Capacitive and Resistive Electric Transfer Intervention on Delayed-Onset Muscle Soreness Induced by Eccentric Exercise. International Journal of Environmental Research and Public Health. 2022; 19(9):5723. https://doi.org/10.3390/ijerph19095723
Chicago/Turabian StyleNakamura, Masatoshi, Shigeru Sato, Ryosuke Kiyono, Kaoru Yahata, Riku Yoshida, Kazuki Kasahara, and Andreas Konrad. 2022. "The Effect of Capacitive and Resistive Electric Transfer Intervention on Delayed-Onset Muscle Soreness Induced by Eccentric Exercise" International Journal of Environmental Research and Public Health 19, no. 9: 5723. https://doi.org/10.3390/ijerph19095723