
Cigarette Smoking in Response to COVID-19: Examining Co-Morbid Medical Conditions and Risk Perceptions

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. COVID-19 Risk Perceptions
3.3. COVID-19 Pandemic and Cigarette Smoking Changes
4. Discussion
4.1. Limitations
4.2. Future Directions/Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19): Symptoms of Coronavirus 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 1 April 2021).
- Bonaccorsi, G.; Pierri, F.; Cinelli, M.; Flori, A.; Galeazzi, A.; Porcelli, F.; Schmidt, A.L.; Valensise, C.M.; Scala, A.; Quattrociocchi, W.; et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 15530–15535. [Google Scholar] [CrossRef] [PubMed]
- Codagnone, C.; Bogliacino, F.; Gómez, C.; Charris, R.; Montealegre, F.; Liva, G.; Lupiáñez-Villanueva, F.; Folkvord, F.; Veltri, G.A. Assessing concerns for the economic consequence of the COVID-19 response and mental health problems associated with economic vulnerability and negative economic shock in Italy, Spain, and the United Kingdom. PLoS ONE 2020, 15, e0240876. [Google Scholar]
- Keeter, S. A Third of Americans Experienced High Levels of Psychological Distress during the Coronavirus Outbreak. Available online: https://www.pewresearch.org/fact-tank/2020/05/07/a-third-of-americans-experienced-high-levels-of-psychological-distress-during-the-coronavirus-outbreak/ (accessed on 1 April 2021).
- Kochhar, R. Unemployment Rose Higher in Three Months of COVID-19 Than It Did in Two Years of the Great Recession. 2020. Available online: https://www.pewresearch.org/fact-tank/2020/06/11/unemployment-rose-higher-in-three-months-of-covid-19-than-it-did-in-two-years-of-the-great-recession/ (accessed on 1 April 2021).
- Parker, K.; Minkin, R.; Bennett, J. Economic Fallout from COVID-19 Continues to Hit Lower-Income Americans the Hardest. Coronavirus Disease (COVID-19) 2020. Available online: https://www.pewsocialtrends.org/2020/09/24/economic-fallout-from-covid-19-continues-to-hit-lower-income-americans-the-hardest/ (accessed on 1 April 2021).
- Eisenberg, S.L.; Eisenberg, M.J. Smoking Cessation During the COVID-19 Epidemic. Nicotine Tob. Res. 2020, 22, 1664–1665. [Google Scholar] [CrossRef]
- Farsalinos, K.; Barbouni, A.; Niaura, R. Systematic review of the prevalence of current smoking among hospitalized COVID-19 patients in China: Could nicotine be a therapeutic option? Reply. Intern. Emerg. Med. 2021, 16, 235–236. [Google Scholar] [CrossRef]
- Karanasos, A.; Aznaouridis, K.; Latsios, G.; Synetos, A.; Plitaria, S.; Tousoulis, D.; Toutouzas, K. Impact of Smoking Status on Disease Severity and Mortality of Hospitalized Patients with COVID-19 Infection: A Systematic Review and Meta-analysis. Nicotine Tob. Res. 2020, 22, 1657–1659. [Google Scholar] [CrossRef]
- Patanavanich, R.; Glantz, S.A. Smoking is associated with worse outcomes of COVID-19 particularly among younger adults: A systematic review and meta-analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Lian, N.; Deng, Y.; Lin, S. The impact of COPD and smoking history on the severity of COVID-19: A systemic review and meta-analysis. J. Med. Virol. 2020, 92, 1915–1921. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Ruiz, C.A.; Lopez-Padilla, D.; Alonso-Arroyo, A.; Aleixandre-Benavent, R.; Solano-Reina, S.; de Granda-Orive, J.I. COVID-19 and Smoking: A Systematic Review and Meta-Analysis of the Evidence. Arch. Bronconeumol. 2021, 57, 21–34. [Google Scholar] [PubMed]
- Reddy, R.K.; Charles, W.N.; Sklavounos, A.; Dutt, A.; Seed, P.T.; Khajuria, A. The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1045–1056. [Google Scholar] [CrossRef]
- Patanavanich, R.; Siripoon, T.; Amponnavarat, S.; Glantz, S.A. Active smokers are at higher risk of COVID-19 death: A systematic review and meta-analysis. Nicotine Tob. Res. 2022. [Google Scholar] [CrossRef]
- Hou, H.; Li, Y.; Zhang, P.; Wu, J.; Shi, L.; Xu, J.; Diao, J.; Wang, Y.; Yang, H. Smoking Is Independently Associated with an Increased Risk for COVID-19 Mortality: A Systematic Review and Meta-analysis Based on Adjusted Effect Estimates. Nicotine Tob. Res. 2021, 23, 1947–1951. [Google Scholar] [CrossRef] [PubMed]
- Barthélémy, H.; Mougenot, E.; Duracinsky, M.; Salmon-Ceron, D.; Bonini, J.; Péretz, F.; Chassany, O.; Carrieri, P. Smoking increases the risk of post-acute COVID-19 syndrome: Results from a French community-based survey. Tob. Induc. Dis. 2022, 20, 59. [Google Scholar] [CrossRef]
- Sarich, P.; Cabasag, C.J.; Liebermann, E.; Vaneckova, P.; Carle, C.; Hughes, S.; Egger, S.; O’Connell, D.L.; Weber, M.F.; da Costa, A.M.; et al. Tobacco smoking changes during the first pre-vaccination phases of the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine 2022, 47, 101375. [Google Scholar] [CrossRef] [PubMed]
- Vanderbruggen, N.; Matthys, F.; Van Laere, S.; Zeeuws, D.; Santermans, L.; Van den Ameele, S.; Crunelle, C.L. Self-Reported Alcohol, Tobacco, and Cannabis Use during COVID-19 Lockdown Measures: Results from a Web-Based Survey. Eur. Addict. Res. 2020, 26, 309–315. [Google Scholar] [CrossRef]
- Yach, D. Tobacco Use Patterns in Five Countries during the COVID-19 Lockdown. Nicotine Tob. Res. 2020, 22, 1671–1672. [Google Scholar] [CrossRef] [PubMed]
- Klemperer, E.M.; West, J.C.; Peasley-Miklus, C.; Villanti, A.C. Change in Tobacco and Electronic Cigarette Use and Motivation to Quit in Response to COVID-19. Nicotine Tob. Res. 2020, 22, 1662–1663. [Google Scholar] [CrossRef]
- Gendall, P.; Hoek, J.; Stanley, J.; Jenkins, M.; Every-Palmer, S. Changes in Tobacco Use during the 2020 COVID-19 Lockdown in New Zealand. Nicotine Tob. Res. 2021, 23, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Keng, S.L.; Stanton, M.V.; Haskins, L.B.; Almenara, C.A.; Ickovics, J.; Jones, A.; Grigsby-Toussaint, D.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; et al. COVID-19 stressors and health behaviors: A multilevel longitudinal study across 86 countries. Prev. Med. Rep. 2022, 27, 101764. [Google Scholar] [CrossRef]
- Bar-Zeev, Y.; Shauly-Aharonov, M.; Neumark, Y.; Hirshoren, N. Changes in Smoking Behavior, Stress, and Sleep Duration among Israeli Hospital Workers during the COVID-19 pandemic: A Cross-Sectional Study. Nicotine Tob. Res. 2022. [Google Scholar] [CrossRef]
- Chagué, F.; Boulin, M.; Eicher, J.C.; Bichat, F.; Saint-Jalmes, M.; Cransac, A.; Soudry, A.; Danchin, N.; Laurent, G.; Cottin, Y.; et al. Smoking in Patients with Chronic Cardiovascular Disease During COVID-19 Lockdown. Front. Cardiovasc. Med. 2022, 9, 845439. [Google Scholar] [CrossRef] [PubMed]
- Gupte, H.A.; Mandal, G.; Jagiasi, D. How has the COVID-19 pandemic affected tobacco users in India: Lessons from an ongoing tobacco cessation program. Tob. Prev. Cessat. 2020, 6, 53. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2021, 75, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Giovenco, D.P.; Spillane, T.E.; Maggi, R.M.; Lee, E.Y.; Philbin, M.M. Multi-level drivers of tobacco use and purchasing behaviors during COVID-19 “lockdown”: A qualitative study in the United States. Int. J. Drug Policy 2021, 94, 103175. [Google Scholar] [CrossRef] [PubMed]
- Elling, J.M.; Crutzen, R.; Talhout, R.; De Vries, H. Tobacco smoking and smoking cessation in times of COVID-19. Tob. Prev. Cessat. 2020, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Kalan, M.E.; Ghobadi, H.; Taleb, Z.B.; Adham, D.; Cobb, C.O.; Ward, K.D.; Behaleh, R.; Fazlzadeh, M. COVID-19 and beliefs about tobacco use: An online cross-sectional study in Iran. Environ. Sci. Pollut. Res. Int. 2020, 28, 40346–40354. [Google Scholar] [CrossRef]
- Kowitt, S.D.; Cornacchione Ross, J.; Jarman, K.L.; Kistler, C.E.; Lazard, A.J.; Ranney, L.M.; Sheeran, P.; Thrasher, J.F.; Goldstein, A.O. Tobacco Quit Intentions and Behaviors among Cigar Smokers in the United States in Response to COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5368. [Google Scholar] [CrossRef]
- Tattan-Birch, H.; Perski, O.; Jackson, S.; Shahab, L.; West, R.; Brown, J. COVID-19, smoking, vaping and quitting: A representative population survey in England. Addiction 2021, 116, 1186–1195. [Google Scholar] [CrossRef]
- Auxier, B.; Anderson, M. Social Media Use in 2021; Pew Research Center: Washington, DC, USA, 2021. [Google Scholar]
- Whitaker, C.; Stevelink, S.; Fear, N. The Use of Facebook in Recruiting Participants for Health Research Purposes: A Systematic Review. J. Med. Internet Res. 2017, 19, e290. [Google Scholar] [CrossRef] [Green Version]
- Antoun, C.; Zhang, C.; Conrad, F.G.; Schober, M.F. Comparisons of Online Recruitment Strategies for Convenience Samples: Craigslist, Google AdWords, Facebook, and Amazon Mechanical Turk. Field Methods 2016, 28, 231–246. [Google Scholar] [CrossRef]
- Boas, T.C.; Christenson, D.P.; Glick, D.M. Recruiting large online samples in the United States and India: Facebook, Mechanical Turk, and Qualtrics. Political Sci. Res. Methods 2020, 8, 232–250. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Evidence Used to Update the List of Underlying Medical Conditions That Increase a Person’s Risk of Severe Illness from COVID-19. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/evidence-table.html (accessed on 18 March 2021).
- Parker, M.A.; Agley, J.; Adams, Z.W.; Villanti, A.C. Opioid use, motivation to quit, and treatment status related to COVID-19: A cross-sectional study. BMC Res. Notes 2021, 14, 195. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Rickert, W.; Robinson, J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br. J. Addict. 1989, 84, 791–799. [Google Scholar] [CrossRef]
- U.S. Census Bureau. Quick Facts. 2021. Available online: https://www.census.gov/quickfacts/US (accessed on 15 May 2022).
- Cornelius, M.E.; Wang, T.W.; Jamal, A.; Loretan, C.G.; Neff, L.J. Tobacco Product Use Among Adults—United States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Kale, D.; Herbec, A.; Perski, O.; Jackson, S.E.; Brown, J.; Shahab, L. Associations between vaping and COVID-19: Cross-sectional findings from the HEBECO study. Drug Alcohol Depend. 2021, 221, 108590. [Google Scholar] [CrossRef] [PubMed]
- Streck, J.M.; Kalkhoran, S.; Bearnot, B.; Gupta, P.S.; Kalagher, K.M.; Regan, S.; Wakeman, S.; Rigotti, N.A. Perceived risk, attitudes, and behavior of cigarette smokers and nicotine vapers receiving buprenorphine treatment for opioid use disorder during the COVID-19 pandemic. Drug Alcohol Depend. 2021, 218, 108438. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, N.A.; Chang, Y.; Regan, S.; Lee, S.; Kelley, J.H.; Davis, E.; Levy, D.E.; Singer, D.E.; Tindle, H.A. Cigarette Smoking and Risk Perceptions During the COVID-19 Pandemic Reported by Recently Hospitalized Participants in a Smoking Cessation Trial. J. Gen. Intern. Med. 2021, 36, 3786–3793. [Google Scholar] [CrossRef]
- Nyman, A.L.; Spears, C.A.; Churchill, V.; Do, V.V.; Henderson, K.C.; Massey, Z.B.; Reynolds, R.M.; Huang, J. Associations between COVID-19 risk perceptions and smoking and quitting behavior among U.S. adults. Addict. Behav. Rep. 2021, 14, 100394. [Google Scholar] [CrossRef]
- Fatollahi, J.J.; Bentley, S.; Doran, N.; Brody, A.L. Changes in Tobacco Use Patterns among Veterans in San Diego during the Recent Peak of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11923. [Google Scholar] [CrossRef]
- Carreras, G.; Lugo, A.; Stival, C.; Amerio, A.; Odone, A.; Pacifici, R.; Gallus, S.; Gorini, G. Impact of COVID-19 lockdown on smoking consumption in a large representative sample of Italian adults. Tob. Control 2021. [Google Scholar] [CrossRef]
- Gaffney, A.; Himmelstein, D.U.; Woolhandler, S. Smoking Prevalence during the COVID-19 Pandemic in the United States. Ann. Am. Thorac. Soc. 2022, 19, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Bou Malhab, S.; Sacre, H.; Salameh, P. Smoking and COVID-19: A Scoping Review. Tob. Use Insights 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Slopen, N.; Kontos, E.Z.; Ryff, C.D.; Ayanian, J.Z.; Albert, M.A.; Williams, D.R. Psychosocial stress and cigarette smoking persistence, cessation, and relapse over 9-10 years: A prospective study of middle-aged adults in the United States. Cancer Causes Control 2013, 24, 1849–1863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buneviciene, I.; Bunevicius, R.; Bagdonas, S.; Bunevicius, A. The impact of pre-existing conditions and perceived health status on mental health during the COVID-19 pandemic. J. Public Health 2022, 44, e88–e95. [Google Scholar] [CrossRef]
- Li, L.; Borland, R.; O’Connor, R.J.; Fong, G.T.; McNeill, A.; Driezen, P.; Cummings, M.K. The association between smokers’ self-reported health problems and quitting: Findings from the ITC Four Country Smoking and Vaping Wave 1 Survey. Tob. Prev. Cessat. 2019, 5, 49. [Google Scholar] [CrossRef]
- Li, L.; Borland, R.; Cummings, K.M.; McNeill, A.; Heckman, B.W.; Fong, G.T.; O’Connor, R.J.; Driezen, P. Are health conditions and concerns about health effects of smoking predictive of quitting? Findings from the ITC 4CV Survey (2016–2018). Tob. Prev. Cessat. 2020, 6, 60. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Quitting smoking among adults—United States, 2001–2010. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 1513–1519. [Google Scholar]
- Donze, J.; Ruffieux, C.; Cornuz, J. Determinants of smoking and cessation in older women. Age Ageing 2007, 36, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Shahab, L.; Jarvis, M.J.; Britton, J.; West, R. Prevalence, diagnosis and relation to tobacco dependence of chronic obstructive pulmonary disease in a nationally representative population sample. Thorax 2006, 61, 1043–1047. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Ruiz, C.A.; Masa, F.; Miravitlles, M.; Gabriel, R.; Viejo, J.L.; Villasante, C.; Sobradillo, V.; IBERPOC Study Investigators. Smoking characteristics: Differences in attitudes and dependence between healthy smokers and smokers with COPD. Chest 2001, 119, 1365–1370. [Google Scholar] [CrossRef] [Green Version]
- Vogel, E.A.; Henriksen, L.; Schleicher, N.C.; Prochaska, J.J. Perceived Susceptibility to and Seriousness of COVID-19: Associations of Risk Perceptions with Changes in Smoking Behavior. Int. J. Environ. Res. Public Health 2021, 18, 7621. [Google Scholar] [CrossRef] [PubMed]
- Brandl, C.; Zimmermann, M.E.; Günther, F.; Dietl, A.; Küchenhoff, H.; Loss, J.; Stark, K.J.; Heid, I.M. Changes in healthcare seeking and lifestyle in old aged individuals during COVID-19 lockdown in Germany: The population-based AugUR study. BMC Geriatr. 2022, 22, 34. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.; Rafferty, H.; Suen, L.W.; Vijayaraghavan, M. System-Level Quality Improvement Initiatives for Tobacco Use in a Safety-Net Health System during the COVID-19 Pandemic. J. Prim. Care Community Health 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Whaley, C.M.; Pera, M.F.; Cantor, J.; Chang, J.; Velasco, J.; Hagg, H.K.; Sood, N.; Bravata, D.M. Changes in Health Services Use among Commercially Insured US Populations during the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2024984. [Google Scholar] [CrossRef]
- Buchbinder, M.; Wilbur, R.; Zuskov, D.; McLean, S.; Sleath, B. Teachable moments and missed opportunities for smoking cessation counseling in a hospital emergency department: A mixed-methods study of patient-provider communication. BMC Health Serv. Res. 2014, 14, 651. [Google Scholar] [CrossRef] [Green Version]
- Grummon, A.H.; Hall, M.G.; Mitchell, C.G.; Pulido, M.; Sheldon, J.M.; Noar, S.M.; Ribisl, K.M.; Brewer, N.T. Reactions to messages about smoking, vaping and COVID-19: Two national experiments. Tob. Control 2020, 31, 402–410. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Categories | N | % |
|---|---|---|---|
| Race | American Indian/Native Alaskan | 8 | 2.8 |
| Asian | 5 | 1.7 | |
| Black | 52 | 18.2 | |
| More than 1 race | 4 | 1.4 | |
| Native Hawaiian/Pacific Islander | 6 | 2.1 | |
| White | 210 | 73.4 | |
| Not reported/unknown | 1 | 0.3 | |
| Ethnicity | Hispanic or Latino | 40 | 14 |
| Not Hispanic or Latino | 243 | 85 | |
| Not reported/unknown | 3 | 1 | |
| Gender | Female | 154 | 53.8 |
| Male | 128 | 44.8 | |
| Non-binary | 1 | 0.3 | |
| Transgender | 2 | 0.7 | |
| Not reported/unknown | 1 | 0.3 | |
| Age | 18–30 | 76 | 26.6 |
| 31–40 | 56 | 19.6 | |
| 41–50 | 50 | 17.5 | |
| 51–60 | 62 | 21.7 | |
| 61 and older | 41 | 14.3 | |
| Not reported/unknown | 1 | 0.3 | |
| Cigarettes per day | 10 or less | 120 | 42 |
| 11–20 | 100 | 35 | |
| 21–30 | 46 | 16.1 | |
| 31 or more | 17 | 5.9 | |
| Not reported/unknown | 3 | 1 | |
| Co-morbid Medical Condition | Any | 148 | 51.7 |
| Cancer | 12 | 4.2 | |
| Cardiovascular Disease | 23 | 8 | |
| Compromised Immune Function | 14 | 4.9 | |
| Diabetes | 30 | 10.5 | |
| Kidney Disease | 12 | 4.2 | |
| Liver Disease | 6 | 2.1 | |
| Lung Disease | 74 | 25.9 | |
| Obesity | 49 | 17.1 | |
| Know someone who had COVID-19 | No | 112 | 39.2 |
| Yes | 173 | 60.5 | |
| Not reported/unknown | 1 | 0.3 |
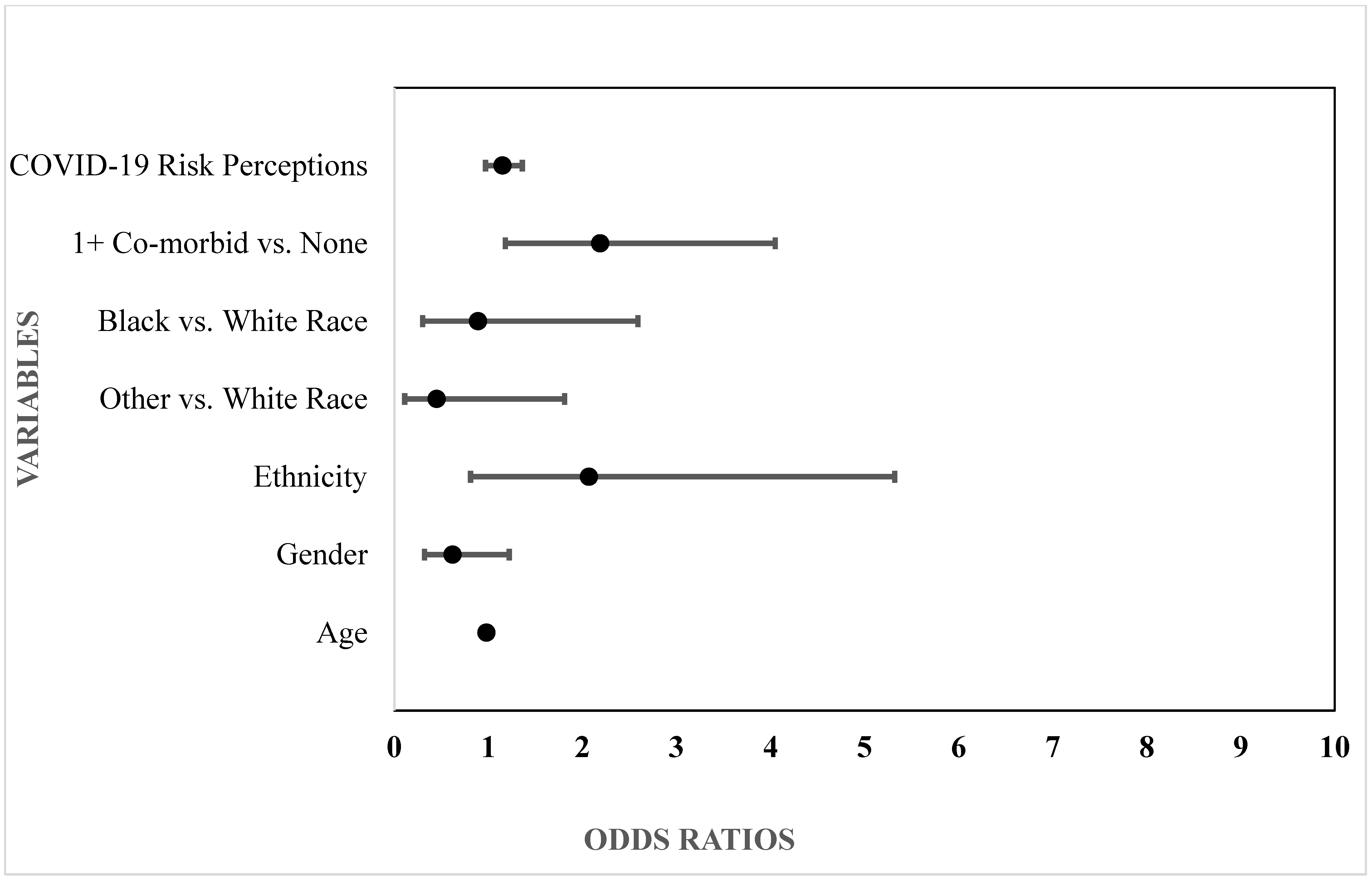
| Variables | Smoking Decreased | Smoking Increased | ||||||
|---|---|---|---|---|---|---|---|---|
| B (SE) | OR (95% CI) | Test Statistic Wald (df) | p | B (SE) | OR (95% CI) | Test Statistic Wald (df) | p | |
| COVID-19 Risk Perceptions | 0.32 (0.10) | 1.38 (1.14–1.68) | 10.79 (1) | 0.001 | 0.14 (0.09) | 1.15 (0.97–1.36) | 2.42 | 0.12 |
| Co-morbid Medical Condition | 0.57 (0.32) | 1.77 (0.94–3.32) | 3.17 (1) | 0.08 | 0.78 (0.32) | 2.19 (1.18–4.05) | 6.15 | 0.01 |
| Race | ||||||||
| Black | 1.00 (0.45) | 2.72 (1.12–6.61) | 4.86 (1) | 0.03 | −0.12 (0.55) | 0.89 (0.30–2.59) | 0.05 (1) | 0.83 |
| Other | 0.63 (0.53) | 1.88 (0.67–5.30) | 1.42 (1) | 0.23 | −0.81 (0.72) | 0.45 (0.11–1.81) | 1.28 (1) | 0.26 |
| White | Reference | --- | --- | --- | Reference | --- | --- | --- |
| Ethnicity | 0.48 (0.48) | 1.62 (0.63–4.14) | 1.01 (1) | 0.32 | 0.73 (0.48) | 2.07 (0.81–5.32) | 2.28 (1) | 0.13 |
| Gender | 0.17 (0.34) | 1.19 (0.61–2.32) | 0.26 (1) | 0.61 | −0.47 (0.34) | 0.62 (0.32–1.22) | 1.89 (1) | 0.17 |
| Age | −0.03 (0.13) | 0.98 (0.95–1.00) | 4.75 (1) | 0.03 | −0.02 (0.01) | 0.98 (0.96–1.01) | 1.84 (1) | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fucito, L.M.; Bold, K.W.; Cannon, S.; Serrantino, A.; Marrero, R.; O’Malley, S.S. Cigarette Smoking in Response to COVID-19: Examining Co-Morbid Medical Conditions and Risk Perceptions. Int. J. Environ. Res. Public Health 2022, 19, 8239. https://doi.org/10.3390/ijerph19148239
Fucito LM, Bold KW, Cannon S, Serrantino A, Marrero R, O’Malley SS. Cigarette Smoking in Response to COVID-19: Examining Co-Morbid Medical Conditions and Risk Perceptions. International Journal of Environmental Research and Public Health. 2022; 19(14):8239. https://doi.org/10.3390/ijerph19148239
Chicago/Turabian StyleFucito, Lisa M., Krysten W. Bold, Sydney Cannon, Alison Serrantino, Rebecca Marrero, and Stephanie S. O’Malley. 2022. "Cigarette Smoking in Response to COVID-19: Examining Co-Morbid Medical Conditions and Risk Perceptions" International Journal of Environmental Research and Public Health 19, no. 14: 8239. https://doi.org/10.3390/ijerph19148239