
Acute Effects of Static and Proprioceptive Neuromuscular Facilitation Stretching of the Plantar Flexors on Ankle Range of Motion and Muscle-Tendon Behavior in Children with Spastic Cerebral Palsy—A Randomized Clinical Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Randomization
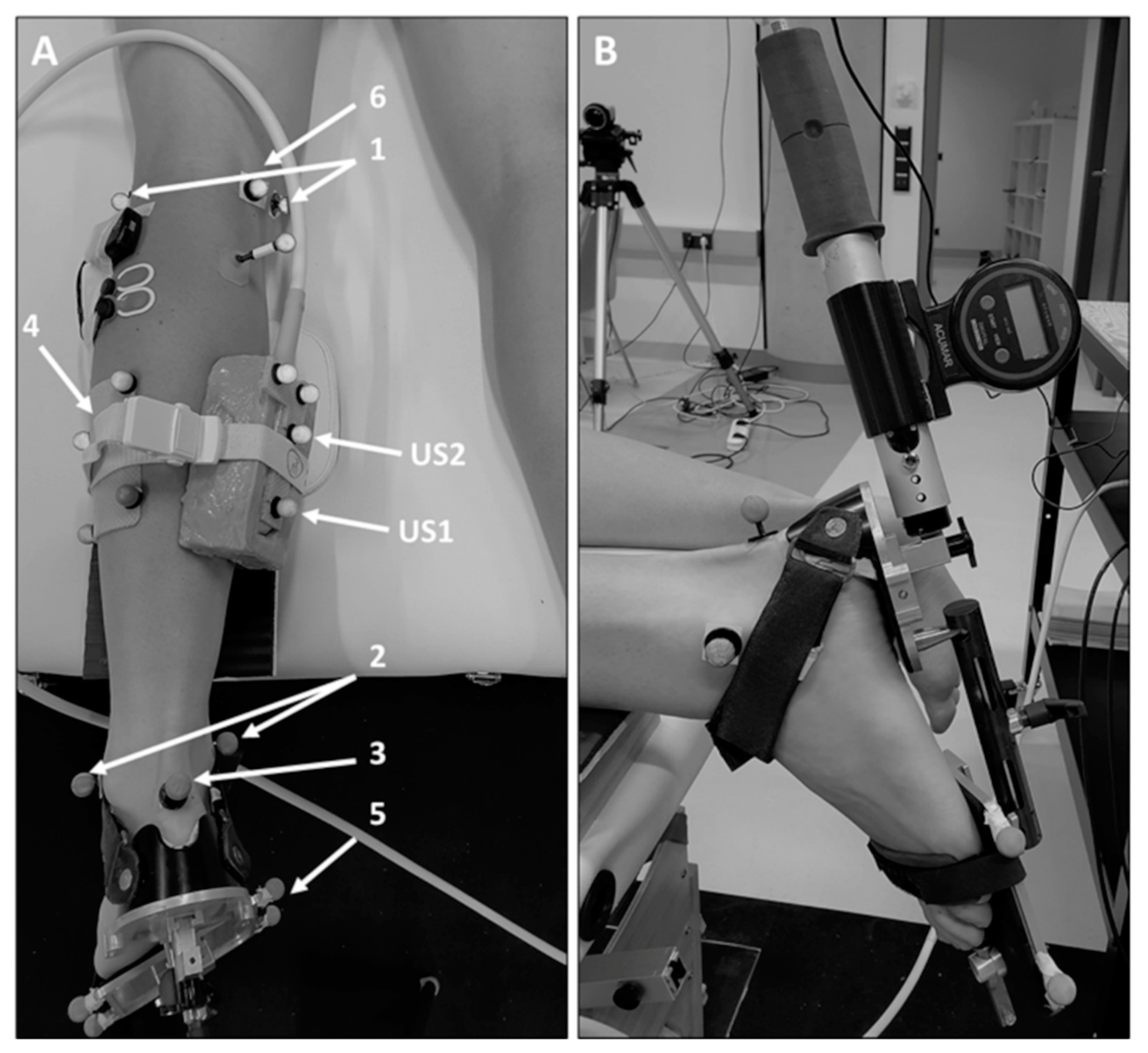
2.2. Data Collection
2.3. Stretching Procedures
2.4. Data Analysis
2.5. Statistics
3. Results
3.1. Participants
3.2. Joint Range of Motion and Muscle Activation
3.3. Muscle-Tendon Unit, Muscle Belly, and Tendon Length Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.-P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral palsy. Nat. Rev. Dis. Primers 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.J.; Herzog, W. Skeletal Muscle in Cerebral Palsy: From Belly to Myofibril. Front. Neurol. 2021, 12, 620852. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L.; Martellotta, T.L.; Sullivan, D.J.; Granata, K.P.; Abel, M.F. Muscle force production and functional performance in spastic cerebral palsy: Relationship of cocontraction. Arch. Phys. Med. Rehabil. 2000, 81, 895–900. [Google Scholar] [CrossRef]
- Lieber, R.L.; Friden, J. Muscle Contracture and Passive Mechanics in Cerebral Palsy. J. Appl. Physiol. 2019, 126, 1492–1501. [Google Scholar] [CrossRef]
- Pingel, J.; Bartels, E.M.; Nielsen, J.B. New perspectives on the development of muscle contractures following central motor lesions. J. Physiol 2017, 595, 1027–1038. [Google Scholar] [CrossRef]
- Barber, L.; Hastings-Ison, T.; Baker, R.; Barrett, R.; Lichtwark, G. Medial gastrocnemius muscle volume and fascicle length in children aged 2 to 5 years with cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 543–548. [Google Scholar] [CrossRef]
- Fry, N.R.; Gough, M.; McNee, A.E.; Shortland, A.P. Changes in the volume and length of the medial gastrocnemius after surgical recession in children with spastic diplegic cerebral palsy. J. Pediatr. Orthop. 2007, 27, 769–774. [Google Scholar] [CrossRef]
- Malaiya, R.; McNee, A.E.; Fry, N.R.; Eve, L.C.; Gough, M.; Shortland, A.P. The morphology of the medial gastrocnemius in typically developing children and children with spastic hemiplegic cerebral palsy. J. Electromyogr. Kinesiol. 2007, 17, 657–663. [Google Scholar] [CrossRef]
- Noble, J.J.; Fry, N.R.; Lewis, A.P.; Keevil, S.F.; Gough, M.; Shortland, A.P. Lower limb muscle volumes in bilateral spastic cerebral palsy. Brain Dev. 2014, 36, 294–300. [Google Scholar] [CrossRef]
- Willerslev-Olsen, M.; Lorentzen, J.; Sinkjaer, T.; Nielsen, J.B. Passive muscle properties are altered in children with cerebral palsy before the age of 3 years and are difficult to distinguish clinically from spasticity. Dev. Med. Child Neurol. 2013, 55, 617–623. [Google Scholar] [CrossRef]
- Herskind, A.; Ritterband-Rosenbaum, A.; Willerslev-Olsen, M.; Lorentzen, J.; Hanson, L.; Lichtwark, G.; Nielsen, J.B. Muscle growth is reduced in 15-month-old children with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Zhao, H.; Gaebler-Spira, D.; Zhang, L.Q. In vivo evaluations of morphologic changes of gastrocnemius muscle fascicles and achilles tendon in children with cerebral palsy. Am. J. Phys. Med. Rehabil. 2011, 90, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Mohagheghi, A.A.; Khan, T.; Meadows, T.H.; Giannikas, K.; Baltzopoulos, V.; Maganaris, C.N. In vivo gastrocnemius muscle fascicle length in children with and without diplegic cerebral palsy. Dev. Med. Child Neurol. 2008, 50, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Kruse, A.; Schranz, C.; Tilp, M.; Svehlik, M. Muscle and tendon morphology alterations in children and adolescents with mild forms of spastic cerebral palsy. BMC Pediatr. 2018, 18, 156. [Google Scholar] [CrossRef]
- Booth, C.M.; Cortina-Borja, M.J.; Theologis, T.N. Collagen accumulation in muscles of children with cerebral palsy and correlation with severity of spasticity. Dev. Med. Child Neurol. 2001, 43, 314–320. [Google Scholar] [CrossRef]
- Gordon, A.M.; Huxley, A.F.; Julian, F.J. The variation in isometric tension with sarcomere length in vertebrate muscle fibres. J. Physiol. 1966, 184, 170–192. [Google Scholar] [CrossRef]
- Matthiasdottir, S.; Hahn, M.; Yaraskavitch, M.; Herzog, W. Muscle and fascicle excursion in children with cerebral palsy. Clin. Biomech. 2014, 29, 458–462. [Google Scholar] [CrossRef]
- Wiart, L.; Darrah, J.; Kembhavi, G. Stretching with children with cerebral palsy: What do we know and where are we going? Pediatr. Phys. Ther. 2008, 20, 173–178. [Google Scholar] [CrossRef]
- Williams, P.E. Use of intermittent stretch in the prevention of serial sarcomere loss in immobilised muscle. Ann. Rheum. Dis. 1990, 49, 316–317. [Google Scholar] [CrossRef]
- Kay, A.D.; Husbands-Beasley, J.; Blazevich, A.J. Effects of Contract-Relax, Static Stretching, and Isometric Contractions on Muscle-Tendon Mechanics. Med. Sci. Sports Exerc. 2015, 47, 2181–2190. [Google Scholar] [CrossRef] [Green Version]
- Kay, A.D.; Dods, S.; Blazevich, A.J. Acute effects of contract-relax (CR) stretch versus a modified CR technique. Europ. J. Appl. Physiol. 2016, 116, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ikezoe, T.; Tokugawa, T.; Ichihashi, N. Acute Effects of Stretching on Passive Properties of Human Gastrocnemius Muscle-Tendon Unit: Analysis of Differences Between Hold-Relax and Static Stretching. J. Sport Rehabil. 2015, 24, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Harvey, L.A.; Katalinic, O.M.; Herbert, R.D.; Moseley, A.M.; Lannin, N.A.; Schurr, K. Stretch for the treatment and prevention of contractures. Cochrane Database Syst. Rev. 2017, 1, CD007455. [Google Scholar] [CrossRef] [PubMed]
- Kalkman, B.M.; Bar-On, L.; Cenni, F.; Maganaris, C.N.; Bass, A.; Holmes, G.; Desloovere, K.; Barton, G.J.; O’Brien, T.D. Medial gastrocnemius muscle stiffness cannot explain the increased ankle joint range of motion following passive stretching in children with cerebral palsy. Exp. Physiol. 2018, 103, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Theis, N.; Korff, T.; Kairon, H.; Mohagheghi, A.A. Does acute passive stretching increase muscle length in children with cerebral palsy? Clin. Biomech. 2013, 28, 1061–1067. [Google Scholar] [CrossRef]
- Kruse, A.; Rivares, C.; Weide, G.; Tilp, M.; Jaspers, R.T. Stimuli for Adaptations in Muscle Length and the Length Range of Active Force Exertion—A Narrative Review. Front. Physiol. 2021, 12, 742034. [Google Scholar] [CrossRef]
- Kalkman, B.M.; Holmes, G.; Bar-On, L.; Barton, G.J.; Maganaris, C.N.; Bass, A.; Wright, D.M.; Walton, R.; O’Brien, T.D. Resistance training combined with stretching increases tendon stiffness and is more effective than stretching alone in children with cerebral palsy: A randomised controlled trial. Front. Pediatr. 2019, 7, 333. [Google Scholar] [CrossRef]
- Chen, K.; Wu, Y.-N.; Ren, Y.; Liu, L.; Gaebler-Spira, D.; Tankard, K.; Lee, J.; Song, W.; Wang, M.; Zhang, L.-Q. Home-Based Versus Laboratory-Based Robotic Ankle Training for Children With Cerebral Palsy: A Pilot Randomized Comparative Trial. Arch. Phys. Med. Rehabil. 2016, 97, 1237–1243. [Google Scholar] [CrossRef]
- Wu, Y.-N.; Hwang, M.; Ren, Y.; Gaebler-Spira, D.; Zhang, L.-Q. Combined passive stretching and active movement rehabilitation of lower-limb impairments in children with cerebral palsy using a portable robot. Neurorehabilit. Neural Repair 2011, 25, 378–385. [Google Scholar] [CrossRef]
- Zhao, H.; Wu, Y.-N.; Hwang, M.; Ren, Y.; Gao, F.; Gaebler-Spira, D.; Zhang, L.-Q. Changes of calf muscle-tendon biomechanical properties induced by passive-stretching and active-movement training in children with cerebral palsy. J. Appl. Physiol. 2011, 111, 435–442. [Google Scholar] [CrossRef] [Green Version]
- Sharman, M.J.; Cresswell, A.G.; Riek, S. Proprioceptive neuromuscular facilitation stretching: Mechanisms and clinical implications. Sports Med. 2006, 36, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Etnyre, B.R.; Abraham, L.D. Gains in range of ankle dorsiflexion using three popular stretching techniques. Am. J. Phys. Med. 1986, 65, 189–196. [Google Scholar]
- Tanigawa, M.C. Comparison of the hold-relax procedure and passive mobilization on increasing muscle length. Phys. Ther. 1972, 52, 725–735. [Google Scholar] [CrossRef]
- Miyahara, Y.; Naito, H.; Ogura, Y.; Katamoto, S.; Aoki, J. Effects of proprioceptive neuromuscular facilitation stretching and static stretching on maximal voluntary contraction. J. Strength Cond. Res. 2013, 27, 195–201. [Google Scholar] [CrossRef]
- Fowler, E.G.; Staudt, L.A.; Greenberg, M.B.; Oppenheim, W.L. Selective Control Assessment of the Lower Extremity (SCALE): Development, validation, and interrater reliability of a clinical tool for patients with cerebral palsy. Dev. Med. Child Neurol. 2009, 51, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, L.; Kalkman, B.M.; Cenni, F.; Schless, S.-H.; Molenaers, G.; Maganaris, C.N.; Bass, A.; Holmes, G.; Barton, G.J.; O’Brien, T.D.; et al. The Relationship Between Medial Gastrocnemius Lengthening Properties and Stretch Reflexes in Cerebral Palsy. Front. Pediatr. 2018, 6, 259. [Google Scholar] [CrossRef] [PubMed]
- Habersack, A.; Zussner, T.; Thaller, S.; Tilp, M.; Svehlik, M.; Kruse, A. Validity and reliability of a novel 3D ultrasound approach to assess static lengths and the lengthening behavior of the gastrocnemius medialis muscle and the Achilles tendon in vivo. Knee Surg. Sports Traumatol. Arthrosc. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Huijing, P.A.; Benard, M.R.; Harlaar, J.; Jaspers, R.T.; Becher, J.G. Movement within foot and ankle joint in children with spastic cerebral palsy: A 3-dimensional ultrasound analysis of medial gastrocnemius length with correction for effects of foot deformation. BMC Musculoskelet. Disord. 2013, 14, 365. [Google Scholar] [CrossRef]
- Weide, G.; Huijing, P.A.; Becher, J.G.; Jaspers, R.T.; Harlaar, J. Foot flexibility confounds the assessment of triceps surae extensibility in children with spastic paresis during typical physical examinations. J. Biomech. 2020, 99, 109532. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Zhou, Z.; Sun, Y.; Wang, N.; Gao, F.; Wei, K.; Wang, Q. Robot-Assisted Rehabilitation of Ankle Plantar Flexors Spasticity: A 3-Month Study with Proprioceptive Neuromuscular Facilitation. Front. Neurorobotics 2016, 10, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feland, J.B.; Marin, H.N. Effect of submaximal contraction intensity in contract-relax proprioceptive neuromuscular facilitation stretching. Br. J. Sports Med. 2004, 38, E18. [Google Scholar] [CrossRef]
- Kruse, A.; Schranz, C.; Svehlik, M.; Tilp, M. Mechanical muscle and tendon properties of the plantar flexors are altered even in highly functional children with spastic cerebral palsy. Clin. Biomech. 2017, 50, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Schless, S.-H.; Desloovere, K.; Aertbelien, E.; Molenaers, G.; Huenaerts, C.; Bar-On, L. The Intra- and Inter-Rater Reliability of an Instrumented Spasticity Assessment in Children with Cerebral Palsy. PLoS ONE 2015, 10, e0131011. [Google Scholar] [CrossRef]
- Johnson, N.L. Systems of frequency curves generated by methods of translation. Biometrika 1949, 36, 149–176. [Google Scholar] [CrossRef] [PubMed]
- Hösl, M.; Bohm, H.; Eck, J.; Doderlein, L.; Arampatzis, A. Effects of backward-downhill treadmill training versus manual static plantarflexor stretching on muscle-joint pathology and function in children with spastic Cerebral Palsy. Gait Posture 2018, 65, 121–128. [Google Scholar] [CrossRef]
- Hösl, M.; Bohm, H.; Arampatzis, A.; Doderlein, L. Effects of ankle-foot braces on medial gastrocnemius morphometrics and gait in children with cerebral palsy. J. Child Orthop. 2015, 9, 209–219. [Google Scholar] [CrossRef]
- Kalkman, B.M.; Bar-On, L.; O’Brien, T.D.; Maganaris, C.N. Stretching Interventions in Children With Cerebral Palsy: Why Are They Ineffective in Improving Muscle Function and How Can We Better Their Outcome? Front. Physiol. 2020, 11, 131. [Google Scholar] [CrossRef]
- Konrad, A.; Stafilidis, S.; Tilp, M. Effects of acute static, ballistic, and PNF stretching exercise on the muscle and tendon tissue properties. Scand. Med. Sci. Sports 2017, 27, 1070–1080. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anthropometrics | SS | PNF |
|---|---|---|
| Number | 8 | 10 |
| Gender (female/male) | 5/3 | 3/7 |
| Age (years) | 10.8 (2.1) | 11.3 (2.3) |
| Body mass (kg) | 44.9 (13.2) | 47.8 (16.5) |
| Body height (cm) | 148.3 (9.5) | 149.1 (16.8) |
| Lower leg length (cm) | 36.1 (3.0) | 35.4 (4.2) |
| Patient characteristics | ||
| GMFCS level I/II/III | 7/1/0 | 7/1/2 |
| Affected (unilateral/bilateral) | 3/5 | 4/6 |
| SCALE (points: 2/1/0) | 1/5/2 | 2/8/0 |
| Parameter | Group | n | Pre | Post | %ΔPre-Post | Effect | F | p | Partial η² |
|---|---|---|---|---|---|---|---|---|---|
| Range of motion (deg) | PNF | 10 | 51.1 (8.2) | 52.2 (9.0) | 2.2 | Time | 7.261 | 0.016 * | 0.312 |
| SS | 8 | 48.3 (3.0) | 51.9 (2.9) | 7.4 | Time × group | 1.980 | 0.179 | 0.110 | |
| Maximum dorsiflexion (deg) | PNF | 10 | −7.3 (10.3) | −4.0 (9.0) | n.a. | Time | 4.900 | 0.042 * | 0.234 |
| SS | 8 | −14.5 (8.0) | −10.4 (4.3) | n.a. | Time × group | 0.051 | 0.824 | 0.003 | |
| Foot sole angle changecommonT (deg) | PNF | 8 | 28.9 (6.7) | 28.9 (5.5) | −0.3 | Time | 3.459 | 0.088 | 0.224 |
| SS | 6 | 26.9 (1.8) | 30.4 (3.3) | 13.1 | Time × group | 3.798 | 0.075 | 0.240 | |
| Resting angle (deg) | PNF | 10 | −47.5 (9.4) | −45.5 (9.4) | 4.2 | Time | 0.530 | 0.477 | 0.032 |
| SS | 8 | −52.2 (7.0) | −51.9 (5.4) | 0.6 | Time × group | 0.276 | 0.606 | 0.171 | |
| Peak externally applied torque (Nm) | PNF | 10 | 8.2 (0.9) | 8.5 (0.8) | 2.9 | Time | 1.517 | 0.236 | 0.087 |
| SS | 8 | 8.8 (1.1) | 9.2 (1.0) | 4.0 | Time × group | 0.060 | 0.809 | 0.004 | |
| Muscle activation (% of MVC) § | PNF | 8 | 2.3 (3.0) | 2.0 (2.3) | −10.8 | Time | 0.968 | 0.342 | 0.065 |
| SS | 8 | 0.9 (0.6) | 0.7 (0.4) | −15.2 | Time × group | 0.058 | 0.813 | 0.004 | |
| Muscle activationcommonT (% of MVC) § | PNF | 8 | 2.2 (2.8) | 2.1 (2.3) | −4.4 | Time | 0.087 | 0.772 | 0.006 |
| SS | 8 | 0.8 (0.6) | 0.7 (0.4) | −16.5 | Time × group | 0.141 | 0.713 | 0.01 |
| Parameter | Group | n | Pre | Post | %ΔPre-Post | Effect | F | p | Partial η² |
|---|---|---|---|---|---|---|---|---|---|
| Muscle-tendon unit elongationcommonT (mm) | PNF | 8 | 20.3 (4.7) | 18.5 (3.1) | −8.8 | Time | 0.191 | 0.670 | 0.016 |
| SS | 6 | 18.3 (2.5) | 20.9 (4.6) | 14.6 | Time × group | 4.768 | 0.050 * | 0.284 | |
| Maximal muscle belly elongation (mm) | PNF | 9 | 17.7 (6.1) | 16.9 (6.5) | −4.1 | Time | 0.484 | 0.498 | 0.033 |
| SS | 7 | 17.6 (6.2) | 16.9 (9.3) | −3.5 | Time × group | 0.003 | 0.956 | 0.000 | |
| Muscle belly elongationcommonT (mm) | PNF | 8 | 13.6 (5.6) | 12.5 (5.7) | −7.5 | Time | 0.523 | 0.484 | 0.042 |
| SS | 6 | 12.9 (3.7) | 12.9 (6.0) | 0.2 | Time × group | 0.569 | 0.465 | 0.045 | |
| Muscle belly straincommonT (%) | PNF | 8 | 7.9 (3.9) | 7.2 (3.7) | −9.2 | Time | 0.606 | 0.451 | 0.048 |
| SS | 6 | 7.0 (1.3) | 7.0 (2.7) | 1.2 | Time × group | 0.968 | 0.345 | 0.075 | |
| Tendon elongationcommonT (mm) | PNF | 8 | 6.7 (3.7) | 6.0 (3.6) | −11.3 | Time | 1.326 | 0.272 | 0.099 |
| SS | 6 | 5.4 (2.5) | 8.0 (2.8) | 49.1 | Time × group | 4.308 | 0.060 | 0.264 | |
| Tendon straincommonT (%) | PNF | 8 | 3.9 (2.2) | 3.4 (2.1) | −12.4 | Time | 1.099 | 0.315 | 0.084 |
| SS | 6 | 3.4 (1.6) | 5.0 (1.4) | 45.9 | Time × group | 3.912 | 0.071 | 0.246 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kruse, A.; Habersack, A.; Jaspers, R.T.; Schrapf, N.; Weide, G.; Svehlik, M.; Tilp, M. Acute Effects of Static and Proprioceptive Neuromuscular Facilitation Stretching of the Plantar Flexors on Ankle Range of Motion and Muscle-Tendon Behavior in Children with Spastic Cerebral Palsy—A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 11599. https://doi.org/10.3390/ijerph191811599
Kruse A, Habersack A, Jaspers RT, Schrapf N, Weide G, Svehlik M, Tilp M. Acute Effects of Static and Proprioceptive Neuromuscular Facilitation Stretching of the Plantar Flexors on Ankle Range of Motion and Muscle-Tendon Behavior in Children with Spastic Cerebral Palsy—A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2022; 19(18):11599. https://doi.org/10.3390/ijerph191811599
Chicago/Turabian StyleKruse, Annika, Andreas Habersack, Richard T. Jaspers, Norbert Schrapf, Guido Weide, Martin Svehlik, and Markus Tilp. 2022. "Acute Effects of Static and Proprioceptive Neuromuscular Facilitation Stretching of the Plantar Flexors on Ankle Range of Motion and Muscle-Tendon Behavior in Children with Spastic Cerebral Palsy—A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 19, no. 18: 11599. https://doi.org/10.3390/ijerph191811599