
Conceptual Framework of a Psychotherapeutic Consultation in the Workplace: A Qualitative Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Participants and Data Collection
2.2.1. Participants and Location of Study
2.2.2. Interviewers
2.2.3. Data Collection
2.2.4. Interview Guideline
2.3. Data Analysis
2.4. Researcher Reflexivity
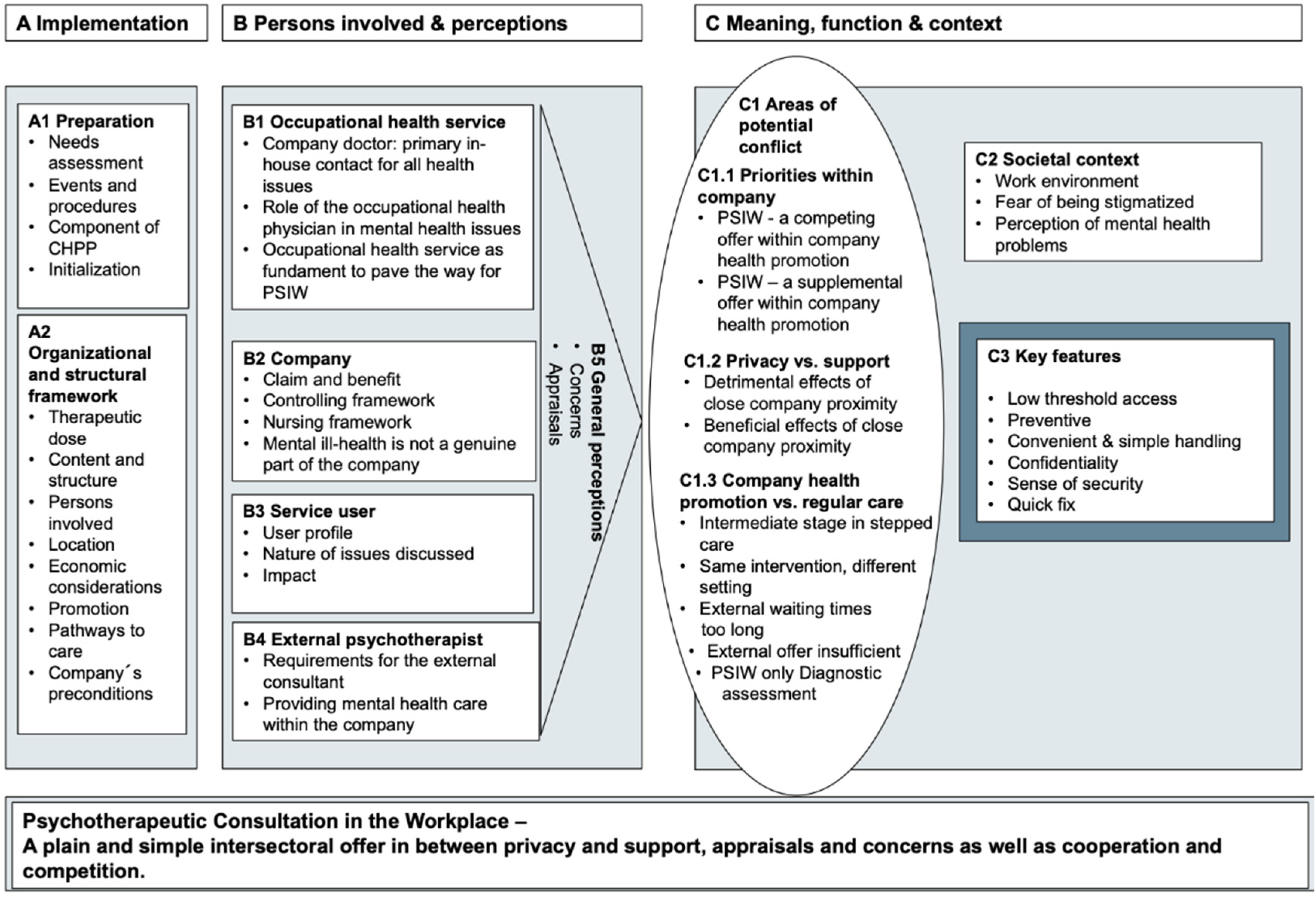
3. Results
3.1. Implementation (A1 and A2)
3.1.1. Preparation (A1)
3.1.2. Organizational and Structural Elements (A2)
3.2. Persons Involved and Perceptions (B)
3.2.1. Occupational Health Service (B1)
3.2.2. Company (B2)
3.2.3. Service Users (B3)
3.2.4. External Mental Health Specialist (B4)
3.2.5. General Perceptions of PSIW (B5)
3.3. Meaning, Function and Context (C)
3.3.1. Areas of Potential Conflict (C1)
C1.1 Priorities within the Company
C1.2 Privacy and Support
C1.3 Company Health Promotion and Regular Care
3.3.2. Societal Context (C2)
3.3.3. Key Features of PSIW (C3)
- A low threshold access: PSIW was stated to be easily accessible. Referrals were reported to be predominantly performed by the company doctor. Due to the missing sterile hospital atmosphere, service users can be more relaxed (Quote C3.1–3);
- Preventive character: The company health promotion team experienced PSIW as a tool to reach individuals early in the course of disease. External psychotherapists reported it as a means to prevent severe mental disorders and chronification (C3.4–5);
- Convenient and simple handling: local closeness of worksite, rapid appointment allocation, little expenditure of time, and easy integration into daily work routine were stated to contribute to convenient and simple handling of PSIW from all three perspectives (Quote C3.6–8);
- Confidentiality and sense of security: Users and staff alike described the offer as being confidential, which means that they users can have access to it, without being recognized by colleagues. Having the possibility to go there unseen was named an important feature of the service (Table A3, Quote C3.9–11). Additionally, the participants reported that a feeling of mutual trust is necessary for the functioning of the PSIW. Security and trust (of users) are established by clarifying roles and tasks and offering a reliable and punctual service. (Table A3, Quote C3.12–14);
- Quick fix: PSIW was considered as a quick and prompt answer to acute mental health problems without getting through a lot of bureaucracy for a first appointment (Quote C3.15, -16, -17). For an overview of quotations on the above-mentioned points, see Appendix A, Table A3.
4. Discussion
4.1. Specific Problems of the PSIW and Possible Solutions
4.1.1. Problems in the Field of Implementation (A)
4.1.2. Problems in the Field of Persons Involved and Perceptions (B)
4.1.3. Problems Concerning Meaning, Function, and Context (C)
4.2. Synthesis
4.3. Strengths and Limitations
4.4. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
Appendix A. Result Tables

{kind=link}
| A Implementation | |||
|---|---|---|---|
| A 1 Preparation | |||
| Number of Codes by Expert Group | |||
| Company Health Promotion Team (n = 9) | Service User (n = 5) | External Psycho-Therapists (n = 6) | |
| Needs assessment (16 codes) A1.1 If something is offered, there is always a need. “[…], in this case there is less need, but demand will increase because if something is offered, there is always a need. This holds true for any place in the world. If McDonald’s wouldn’t exist at all, nobody would need chicken wings. That’s the way it is. There is always some need if something is offered on the market and after a while, the demand is slowly increasing and then remains on a certain level. At least as far as our experiences with offered services are concerned.” (Quote 16:42, Company mental health promotion team) | 15 | 0 | 1 |
| Events and procedures to be taken in advance of the implementation (20 codes) A1.2 Sensitizing incident: conversation with a colleague who suffered from burnout and received medical treatment. “There is a large number of burnout sufferers right now... Last Saturday, I just talked to one of my colleagues who are meanwhile in medical treatment due to burnout and I believe that this should really give food for thought to a company.” (Quote 8:14, Service user) | 16 | 3 | 1 |
| PSIW as an integral component of the company health promotion program (17 codes) A1.3 PSIW is one outcome of the work undertaken by a project group in the company. “This holds true for the first year and then I launched and managed a project group which worked on concrete measures and one... one very important measure resulting from this overall project, which deals with a number of further aspects, was psychotherapeutic consultation in the workplace.” (Quote 19:8, Company mental health promotion team) | 15 | 6 | 2 |
| Initialization (12 codes) A1.4 Describing the initialization of the consultation/getting in contact with an external organization. “The first contact … well, someone then came up with the idea to get in touch with them. This happened in a straightforward way, because they had expressed their interest and some projects were already running in cooperation with other companies in [city name]. Hence, we could say the door was open.” (Quote 9:15, Company mental health promotion team) | 8 | 0 | 4 |
| A2 Organizational and structural needs | |||
| Therapeutic dose (14 codes) A2.1 The amount of sessions is sufficient/could possibly be a little bit more. “The sessions only took one hour, that’s to say 50 min plus a 10-min cool-down phase. All in all, that’s sufficient. At first, you are, of course, hoping for a 5-h talk which clears up your mountain of problems right away and then everything is fine. This is how you’ve always imagined it but, of course, your head tells you that this won’t work. Somehow you still hope for it to be so. Hence, you might possibly like to have some more appointments.” (Quote 14:18, Service user) | 5 | 4 | 5 |
| Content and administrative form (35 codes) A2.2 PSIW is focusing on communication and attitude. “The thing is, that it’s not so much about constructive solutions or the actual situation but it’s all about communication with one another within the company or the way how people tackle their work, e.g., with great accuracy or in a very structured manner.” (Quote 2:35, External consultant) | 9 | 10 | 17 |
| Persons involved (10 codes) A2.3 Personnel and management play a major role and must be well-disposed towards the project. “Well, honestly speaking, it certainly wouldn’t have been possible without having the right site management. In our case, the management has done excellent work. At that time, we had a personnel manager who took care of the matter.” (Quote 9:67, Company mental health promotion team) | 7 | 0 | 3 |
| Location (24 codes) A2.4 It is difficult to maintain anonymity within the company. “Yes. The problem is that a company is like a big village. People in the company are closely watching each other. We’ve got an in-company social advisory service. And of course, people have an eye on who is going there. For some people the mere fact that someone is going there is sufficient to tell that they are nuts.” (Quote 17:12, Company mental health promotion team) | 10 | 9 | 5 |
| Economic considerations (21 codes) A2.5 PSIW really pays since, in the long term, incapacity for work generates large costs. “We didn’t discuss costs in the first place. For such cases, we’ve got an expert adviser who makes sure that the cost-to-benefit ratio is positive. That’s why I am willing to pay for this.” (Quote 15:36, Company mental health promotion team) | 16 | 1 | 4 |
| Promotion (19) A2.6 Positive feedback of other users of PSIW provides inspiration to participate as well. “When my colleagues told me that they have been there too I decided to go there as well. And I found it a very good thing to do.” (Quote 8:43, Service user) | 10 | 5 | 4 |
| Pathways to care (18) A2.7 In order to find an indication for PSIW it can be helpful to keep asking questions about ordinary diseases. “Let’s say someone has an appointment for a hearing test and talks about one or another phenomenon and when you keep asking questions suddenly psychological stress is the answer. Thus, it can happen that someone who came for a hearing test ends up with going to the psychosomatic consultation service and this is precisely a good thing if it is indicated.” (Quote 19:18, Company mental health promotion team) | 14 | 2 | 2 |
| Company’s preconditions (12) A2.8 Taking part in a factory tour is particularly useful in order to better understand the actual workflows. “That’s true. That’s really true. In my opinion, this was very useful. I once took part in a factory tour for one hour or so. Somehow it made very much sense, having seen the working environment of some people working at that time, to walk through the production halls and to see the single workplaces. Yes, I believe that this was very important and made sense.” (Quote 02:36, External consultant) | 3 | 3 | 6 |
| B Persons Involved and Perceptions | |||
|---|---|---|---|
| B1 Occupational Health Service | |||
| Number of Codes by Expert Group Absolute Number of Codes (Codes per Participants of Respective Treatment Group) | |||
| Company Health Promotion Team (n = 9) | Service User (n = 5) | External Psycho-Therapists (n = 6) | |
| Company doctor: primary in-house contact for all health issues (21) B1.1 Everyone can consult the company doctor even though there is no work-related cause. “During my work as a company doctor here, where every employee can liberally consult me even without having any work-related problem … I noted that mental problems have obviously increased significantly.” (Quote 19:2, Company mental health promotion team) | 13 | 0 | 8 |
| Company doctor’s role in mental health issues (10) B1.2 The company doctor is insufficiently qualified for psychosomatic treatment. “We’ve also talked about it. But Only in his capacity as physician for general medicine … Mr [the person interviewed] is under enormous pressure because everything is simply too much and then he starts reporting all his problems and that’s it. The doctor listens to the patient, tells him that this situation cannot continue and that something must be changed.” (Quote 14:14, Service user) | 3 | 2 | 5 |
| Occupational health service as fundament on the way to PSIW (17) B1.3 The company doctor enjoys great trust among the employees. “Well, furthermore, I believe we enjoy great trust among the employees and partially we know the workers much better than the general practitioner. Thus, the employees seem to feel in good hands even in this field.” (Quote 18:24, Company mental health promotion team) | 9 | 1 | 7 |
| B2 Company | |||
| Claim and benefit (14) B2.1 PSIW really pays since incapacity for work generates large costs in the long term. “We didn’t discuss costs in the first place. For such cases, we’ve got an expert adviser who makes sure that the cost-to-benefit ratio is positive. That’s why I am willing to pay for this.” (Quote 15:36, Company mental health promotion team) | 9 | 3 | 2 |
| Controlling framework (10) B2.2 Company doctors wants to be involved. “[…] I believe, that this would inspire more patients to look for direct contact with us, instead of first consulting the company doctor. However, company doctors obviously still want to be involved and don’t want the patients to contact us directly.” (Quote 7:55, External psychotherapist) | 7 | 1 | 2 |
| Nursing framework (10) B2.3 PSIW sets a clear signal that they [the company] care for employees. “Yes, I believe so, because many topics are mostly work-related. That’s to say, a lot of frustration, overburdening, expressions like ‘I cannot take it any longer’/‘I don’t want anymore’, even though there are no problems in private and family life and in those cases, I believe, it is at least a sign for responsibility towards the employee. Saying “Listen! We care for you!” Hence, I believe, something is happening.” (Quote 14:21, Service user) | 5 | 1 | 4 |
| Mental ill-health is not considered to be a relevant issue for a company (7) B2.4 Psychosomatic complaints render corporate actors helpless and are perceived as hopeless and diffuse. “Not exactly, but it has always been a big issue in meetings of the works council. Because those cases were perceived as absolutely hopeless and difficult to deal with. Hence, it is much easier to prescribe medical rehabilitation for someone who suffers from an organic disease and foster reintegration following illness and things like that than to deal with someone who suffers from mental health problems and where the clinical picture is not even clear.” (Quote 17:30, Company mental health promotion team) | 5 | 0 | 2 |
| B3 Service user | |||
| User profile (30 codes) B3.1 Men in technical professions have problems to open up. “[…] I think […] many still have a technical or primarily technical view of the world and instead of taking care of themselves and acknowledging their own fragility or becoming more open minded towards such things [mental health issues] they rather try to pull themselves together and deal with the problem by themselves because this is much easier for men, especially for men working in technical professions.” (Quote 2:6, External psychotherapist) | 8 | 0 | 22 |
| Nature of problems (38) B3.2 PSIW strengthens self-confidence. “I’ve talked to my boss about it in advance, however, talking to an external psychotherapist has helped me to figure out that I wasn’t wrong and this helped me to be more confident about going to my boss again and instead of only asking if we could change something I confidently said: we need to change something. Hence, it definitely does have a strong influence.” (Quote 13:39, Service user) | 11 | 2 | 25 |
| Impact (14) B3.3 The consultation service helped to regain strength. “Yes, I believe it makes sense and helps to get back on your feet.” (Quote 11:28, Service user) B3.4 The advantages for the employees are a low rate of absence due to illness and thus less workload and pressure for each single employee. “I believe it is advantageous for the colleagues as well because it creates a nicer atmosphere in the department if the team is complete especially in the context of long-term incapacity to work or working shifts. Taking up work for someone who is incapable to work for a long time or for someone working shifts creates dissatisfaction, additional work and stress. Thus, if more people are able to work due to this service the happier they are and the total number of absences due to illness drops because the work load is no longer exceedingly high.” (Quote 7:47, External Consultant) B3.5 PSIW can place the company under pressure to take actions or make changes. “It makes a difference, if this service advises to take appropriate actions or changes. It might become difficult for a company especially if it is recommended not to put back the employee in their former workplace or to stop working shifts. In this case, the company is put under pressure to act. Are there ways of assigning the employee a light duty work or digs the company its heels in and everything remains as it is?” (Quote 7:21, External consultant) | 5 | 3 | 6 |
| B4 External mental health specialist | |||
| Requirements for the external consultant (28) B4.1 An external psychotherapist guarantees complete discretion and confidentiality. “I think it’s good that someone from outside the company takes care for it. The thing is that you never know if the HR department, at the end, still gets wind of some of the information’s or […]” (Quote 8:17, Service user) | 14 | 5 | 9 |
| Providing mental health care within the company (18) B4.2 In your function as psychotherapist you can learn a lot about working conditions—further training for psychotherapists. “In your function as psychotherapist you learn a lot about working life. That’s for sure. Not only because you work on it down to the last detail with your patients but also because you start reading about it in theory. I think you learn a lot about working conditions and, yes, indeed, about what makes you ill and what keeps you healthy, etc. All in all, it’s a great training program for psychotherapists who are suddenly confronted with real life.” (Quote 4:61, External psychotherapist) | 5 | 2 | 11 |
| B5 Overall judging | |||
| Concerns (21) B5.1 Uncertainty: Do people make use of PSIW not knowing exactly in which way it would help? “Well, yes, I was very uncertain as to which way it would be accepted, in addition, I wasn’t sure whether it’s more of medical or psychological nature. At first, it seemed ambiguous, because it is somehow situated in between the company doctor and me. That’s why I was very uncertain if people would go there at all and who would advise them to go there.” (Quote 16:1, Company mental health promotion team) B5.2 In fact, some of the employees were also disappointed by PSIW. “Now that the service has started, I realized that, of course, for some people it’s a big help, for others, on the contrary, it isn’t. It all depends on how somebody opens up and how urgent the problems are. Well, of course, there are people who don’t care about things like that and there are those who, indeed, expect more from what is finally offered.” (Quote 21:17, Company mental health promotion team) | 8 | 5 | 8 |
| Appraisals (43) B5.3 Establishing PSIW is ‘a great thing’. “Viewed realistically, it couldn’t have done better. It was really well-done. We can be proud on what we have. It’s actually an excellent thing. Personally, I would have preferred it to go faster. Retrospectively, considering the very complex company structures, I have to say that it couldn’t have gone differently. Otherwise, if we hadn’t done it this way, it wouldn’t have been so successful […]” (Quote 9:76, Company mental health promotion team) | 24 | 5 | 15 |
| C Meaning, Function and Context | |||
|---|---|---|---|
| C1 Areas of Potential Conflict | |||
| C1.1 Priorities within the Company | |||
| Number of Codes by Expert Group | |||
| Company Health Promotion Team (n = 9) | Service User (n = 5) | External Psycho-Therapists (n = 6) | |
| PSIW—a competing offer within company health promotion (14) Quote C1.1_1 This service may not render existing institutions within the company unnecessary. “In fact, you need to be particularly careful not to offer any service that makes the tasks of people already working within the factory, such as psychological and social consultants, superfluous. Considering the fact that nowadays everything that isn’t nailed down is being outsourced in bigger companies, it must be a differentiated offer.” (External consultant 4:22) Quote C1.1_2 Fear: PSIW might be a too strong competitor and far to prevalent. “This is what the people here in the company were afraid of. This equally applies to us since the works council and the internal social counselling service were initially reluctant to the new service due to fear of competition. At the beginning our own position seemed to be challenged. We were a bit afraid that this service would intervene too much and would lose sight of being a detached consultancy service.” (Company mental health promotion team 17:15) | 11 | 1 | 3 |
| PSIW—an enrichment in the field of company health promotion (28) Quote C1.1_3 Release from the duty to preserve secrecy enables the adviser in the company to give advance information to the therapist. “Being released from the confidentiality obligation shows that people are open for treatment and as soon as an underlying cause is suspected I could give the therapist a useful advice at what should be looked first.” (Company mental health promotion team 20:29) Quote C1.1_4 PSIW improves the psychosocial structure within a company. “Furthermore, I simply believe that it is advantageous because it improves or rather enriches the psychosocial structure within a company. Let’s put it this way: it’s simply an additional offer such as offering workplace sports groups. That’s quite an advantage.” (Company mental health promotion team 16:14) | 21 | 3 | 4 |
| C1.2 Conflicting interests of privacy and support | |||
| Detrimental effects of close company proximity (21) Quote C1.2_1 In case of problems with my supervisor I would not have consulted PSIW. “However, if I had difficulty working with my supervisor, I would not have used this service in this way.” (Service user 10:9) Quote C1.2_2 Fear: informal sounding out of employees’ opinions. “Yes. I believe that there are some concerns. Especially at times when you read about the Deutsche Bahn scandal concerning their sounding out of employees. That’s, let’s say, a big company where it’s always possible that someone wants to do things like that. But basically, the same may hold true for the in-house medical service at all. There are also concerns about having to undergo health checks, etc. In theory, there could also be someone who passes on the data and this, in turn, might have negative impact on your career.” (Service User 13:16) | 5 | 8 | 7 |
| Benefits of company-internal work (19) Quote C1.2_3 Company-internal work promotes the willingness to talk about work-related problems. “Simply talking about things that pose problems at work in a frank and open way. And Because it seems so natural that this is offered in the framework of occupational health management.” (External consultant 7:15) Quote C1.2_4 PSIW enables the therapist to get a detailed impression of the workplace. “Indeed, in this way, you get to know the employees’ workplace and the corresponding relations and conflicts much better. In the meantime, we have, of course, learned quite a number of stress models. We know what gratification crises are and so on. In this way you get to know a lot about a specific workplace.” (External consultant 4:56) | 7 | 2 | 10 |
| C1.3 Company health promotion vs. regular care | |||
| PSIW—an intermediate step in a multi-stage care approach (29) Quote C1.3_1 People working in the framework of PSIW help the patient to get a secondary treatment. “And we are helping the patients, speaking for myself, to get a secondary treatment following the short-term therapy that has taken place within this framework. This is what I would do … am trying to do, somehow …” (External consultant 3:43) Quote C1.3_2 Being in contact with PSIW helps to get a secondary treatment much earlier. “Well, of course most of the patients expected this since we promoted it this way. It was and still is expected that, in particular, direct referrals to a clinic, a medical specialist, a psychiatrist, a psychologist or for a therapy go much quicker.” (External consultant 16:16) | 9 | 11 | 13 |
| PSIW vs. PSOC: same intervention, different setting (9) Quote C1.3_3 Treatment at the clinic offers more time for treatment and a higher treatment frequency. “This way [ i.e., if a patient comes to the clinic], I know, the patient has already decided to make a therapy, we have more time and we meet more often in order to work on changes. After an appointment with someone from the company we meet again after three, four or five weeks at the earliest in order to work on changes.” (External consultant 2:27) Quote C1.3_4 PSIW basically concentrates on the same problems as the clinic. “Well… yes, I actually expected it to be like this—a high degree on affective disorders. I believe that’s more or less true. That’s similar to everyday business. I’ve got less anxiety disorders than in everyday business or in my medical office. I believe, there is a quite realistic explanation for it. Yes. I didn’t have any.” (External consultant 5:10) | 0 | 1 | 8 |
| PSIW—a diagnostic assessment (20) Quote C1.3_5 PSIW is supposed to make a diagnosis and to decide how to proceed. “Whether the patient needs an inpatient treatment, so that, in any case, the further proceeding is clear...that someone decides, based on the diagnosis, whether a hospital stay is urgently needed, that is, inpatient treatment, day-care treatment or outpatient treatment.” (Company mental health promotion team 21:15) Quote C1.3_6 Basic concept: the main task of the PSIW is to determine whether further treatment is necessary. “And then they asked how this could look like. As an example, I mentioned talks which we conduct in our outpatient psychotherapeutic clinic. That it’s all about diagnosis and that at the end of a session you can say, yes, you need an outpatient psychotherapy, a day-care therapy or rather an inpatient therapy […].” (External consultant 6:8) | 12 | 2 | 6 |
| External offers are perceived as insufficient (20) Quote C1.3_7 External offers are perceived as too complicated, unsympathetic and less understanding. “In case of seeking an external consultant you first need to go to the general practitioner in order to get started. That doesn’t make it easy at all. Then you need to decide where to make an appointment? Who seems to be trustworthy? Since there are topics with higher needs for intimacy. Then there is a waiting time. If you are very lucky you get an appointment within one month. Usually within two, three or four months. Some even might not offer any appointment at all. Above all, the question arises whether to see a second or third therapist before starting the therapy in order to know who fits best. At the end, that’s all quite complicated.” (Company mental health promotion team 9:26) Quote C1.3_8 External offers don’t leave much room for selection criteria. “Though there are quite a number of criteria and selection mechanisms, there are much more healthy than sick persons who get psychotherapy. In Germany, there are groups of people who indeed have trouble gaining access, such as migrants not speaking High German, etc. […]” (External consultant 4:6) Quote C1.3_9 “No. A few years ago I went to an external consultant. It was very disappointing. I stopped therapy. Two years ago, I tried it again during my rehabilitation care. They gave me the advice to look for somebody here. After having searched for a place for therapy for around half a year I gave up.” (Service user 11:5) | 10 | 6 | 4 |
| External offers have too long waiting times (16) Quote C1.3_10 Employees don’t ask for secondary treatment since it is too complicated to get an appointment. “The thing that doesn’t work is to get people in further therapy. This is rejected by our employees as well. They say, therapy—no, thanks. This seems to be a critical point. It may be due to the great difficulty getting a place for therapy.” (Company mental health promotion team 12:31) Quote C1.3_11 External offers have too long waiting periods during which patient’s life changes too much. “That it goes quicker and thus the employee doesn’t lose track. In most cases, patients who are looking for an external consultant for therapy and only get an appointment within five months no longer need the place since their entire life has meanwhile changed.” (Company mental health promotion team 16:17) | 8 | 3 | 5 |
| C2 Societal context | |||
| Challenging work environment (24) Quote C2.1 Employees in sandwich positions are put under enormous pressure in their daily working life. “I believe that employees in middle management positions are mostly affected. They find themselves in sandwich positions, having departments with 20, 50, 80 employees on the one hand and a management on the other hand that stipulates tasks which have been decided in the headquarters of the company or a big division somewhere in city X or city Y, only thinking about their own career without questioning things whether they could apply or not. That means that tasks are transferred to the middle management without any change or even with an additional task.” (Service user 14:36) Quote C2.2 Excessive working time is one of the reasons why external help is not accepted. “Right now, it’s due to my workload. Two colleagues of my department have quit their jobs. And I had to fully take on their work. In addition to my work. Thus, my health and preventive health care were neglected during the last months.” (Service user 8:6) | 8 | 14 | 4 |
| Fear of being stigmatized (36) Quote C2.3 Fear: psychosomatic treatment can have negative effects on the career. “He took it quite easy. Nevertheless, I believe that it is not that easy if the HR department gets wind of it, especially in the case of an employee who wants to pursue a successful career. In most cases people think you’ve got problems. In this respect, you need to be careful.” (Service user 8:18) Quote C2.4 Many people only read about psychological disorders in newspapers and don’t want to be part of it. “Similar to a patient visiting the medical office of a general practitioner who has a bit of an idea about mental diseases due to their reading of magazines and who is convinced not to be like the person described in the article and who definitely doesn’t want to be like that person. Thus, the inhibitions to talk are too big.” (External consultant 3:66) | 13 | 11 | 12 |
| Perception of mental health problems from three perspectives | |||
| Perception of psychosomatic problems (68) Quote C2.5 Indices of need for PSIW Increasing number of burnouts or breakdowns. “There is an increasing demand. I noticed it since I am acting in an operative capacity. In more concrete terms, I take care of people working in a particular field. There is an increasing demand as well. They of course only come to me after having suffered a burnout or breakdown. Lately, this has increased.” (Company mental health promotion team 12:1) Quote C2.6 Perception of psychosomatic problems in the form of aggressiveness, sleep disorders and depression. “Employees showing workplace aggressions. In this case, they come to us after having realized by themselves that something is wrong. As soon as you suffer from sleep disorders or depression you start looking for help.” (Company mental health promotion team 12:8) Quote C2.7 Perception of psychosomatic problems in the form of loss of physical or mental fitness. “Caused by the increasing need for help, support or time to recover since you could no longer bear it due to the increasing loss of physical and mental fitness.” (Service user 14:1) Quote C2.8 Perception of psychosomatic problems in the form of irritability, stress or inability to relax. “I realized that certain stressful situations caused me to be partially short-tempered. If something went wrong at work and upset me I couldn’t stop stressing about work in my spare time or at night. I noticed that this wasn’t good for me.” (Service user 8:1) Quote C2.9 Most patients suffer from increasing strain, mood swings and exhaustion. “Although there is no clearly defined term for it… there is a trend towards increasing strain, mood swings and exhaustion—a feeling of having reached or even exceeded a limit. This is what I expected in advance and I believe that this holds true for the majority of patients.” (External consultant 3:19) Quote C2.10 Patient with personality disorder visiting PSIW. “Yes. It’s a matter of principle. I’ve got a patient who wouldn’t go anywhere else at the moment. That’s for sure. A person with a serious personality disorder. Someone who is very anxious, difficult or evasive when it comes to social contacts and does not even have any social contacts at all.” (External consultant 5:24) | 38 | 15 | 15 |
| C3 Key features of PSIW | |||
| Low threshold access (15) Quote C3.1 ‘Non-hospital atmosphere’ reduces inhibitions. “I believe that patients feel much more at ease going to PSIW than to a hospital where their first contact would be the hospital reception. I guess this would pose difficulties for the patients.” (External consultant 7:27) Quote C3.2 PSIW taking place in the company doctor’s premises makes access easy. “Insofar, for a big company it seemed to be interesting and encouraging to offer such a service at the company doctor’s premises since you can simply make an appointment with the doctor or the doctor’s receptionist.” (External consultant 3:11) Quote C3.3 Aim of PSIW in company [name of the company] was to create a low threshold offer. “This means that our concept primarily aimed at reducing this threshold.” (Company mental health promotion team 18:12) | 7 | 2 | 6 |
| Preventive (25) Quote C3.4 PSIW deals with patients who are not yet seriously ill. “Honestly speaking, I didn’t expect that patients being transferred to our office by their general practitioner have already endured such extensive periods of serious suffering. Based on my personal experience, I honestly believe that some of the cases could be, in inverted commas, declared as burnout syndrome.” (External consultant 3:18) Quote C3.5 For quite some time now, the works council is trying to find a way to get in contact with those people at an early stage. “Let’s say—at a time when the disease has not yet caused permanent damage. This is where psychosomatics comes in—psychosomatic consultation. Simply, recognizing the disease at an early stage in order to counter steer immediately instead of waiting until someone breaks down and then to say: ‘Everything is ruined. What are we doing now?” (Company mental health promotion team 17:38) | 10 | 1 | 15 |
| Convenient and simple handling (28) Quote C3.6 It is very convenient to find PSIW directly ‘across the courtyard’. “I simply made use of this offer because it was so easy. You just need to walk across the courtyard and say ‘yes’.” (Service user 8:5) Quote C3.7 The fact that the employee doesn’t have to take a day off makes it much easier to use the offer. “Yes, that’s quite an advantage. Pragmatically speaking, one big advantage is that it is offered close by. That means, people don’t need to invest much effort since they don’t need to go anywhere else, don’t have to take one or half a day off or apply for leave of absence. Of course, this is a big advantage. If something is close by, it is used more frequently. This is an old rule in the services business and holds true for every service and this is what it is.” (Company mental health promotion team 16:13) Quote C3.8 The employees are reluctant to visit a psychosomatic clinic, visiting PSIW is easier “Another plus: it is very helpful since it’s easy to explain where to go to and there are no things that need to be arranged in advance, so it’s much easier than to say ‘You need to go to the psychosomatic hospital in order to make an appointment’. No. That would be too complicated. And People rather refrain from doing so.” (Company mental health promotion team 20:15) | 7 | 14 | 8 |
| Confidentiality (15) Quote C3.9 The company medical center guarantees a sufficiently high level of anonymity. “Due to the number of people going in and out, it won’t be noticed at all in case you would like to use the service in the building. We didn’t have any concerns at all. We were convinced that no one would even notice you going there since it is located at the company doctor’s premises and basically you could also just have a doctor’s appointment there and no one considers it to be a problem neither.” (Company mental health promotion team 12:15) Quote C3.10 The in-house medical service should not be located to closely to the company management. “If this isn’t the case, if it is located close to the management and HR department, it would be the wrong place. However, I believe that this cannot be one-to-one translated to each company. Similar to the works council. There are companies that have an independent works council. In this case you can go there and talk openly about your worries. However, there are companies where I would never go to the works council because they are favorably disposed towards the management.” (Service user 13:43) Quote C3.11 “Well, there are employees who tell me that they don’t like the service to be installed here… they don’t want to be seen here for an hour or so because someone could conclude that they are using the psychosomatic consultation service. Simply because having a vaccination wouldn’t take so long. Some of the employees do in fact think so.” (Company mental health promotion team 19:27) | 9 | 4 | 2 |
| Sense of security (8) Quote C3.12 There must be a clear definition of the functions of an external consultant in order to prevent mistrust. “Defining my function in much more detail makes the main difference. If a patient visits me at the hospital I assume [they know my function], (…) [deleted in order to ensure anonymity]. However, the function of an external psychotherapist provided by [name of company] needs to be explained. That’s the clear difference. I need to define my function and tasks very clearly in respect to my patient. What does the company expect from me? Otherwise, there is mistrust and confusion among the patients or rather employees.” (External consultant 4:31) Quote C3.13 Reliable appointments scheduling is very important and makes psychotherapeutic sessions more convenient. “Especially in the case of a company called [name of the company] and considering the fact that it is essential in everyday life, I believe, it’s quite counterproductive if appointments are not met and the logistics are not right. I think some people will lose trust if making an appointment turns out to be complicated for whatever reason.” (External consultant 10:40) Quote C3.14 PSIW is a matter of trust. “We want to address security needs and show corporate responsibility. I can confidently place myself in their hands. I can try things which are offered here. Offering this consultation service is, again, such a matter of trust.” (Company mental health promotion team 9:19) | 2 | 3 | 3 |
| Quick fix (22) Quote C3.15 PSIW may also provide a quick fix for “smaller” problems in everyday work. “Well, of course. There are some cases with not clearly identified problems for example. In this case, I explain, for example, two or three cognitive ways of dealing with it. With those problems. Sometimes I suggest one or the other role play. In order to find out whether it would be useful right now to actively approach the matter with the boss. Such things, I would say. And Then this is done and everything is fine. This is sometimes also the case. But I personally think this is rarely the case.” (External consultant 5:31) Quote C3.16 Patients shall get their problems solved quickly. “As far as the patients are concerned, I didn’t meet all their needs at the beginning. What they needed was a faster solution and me too, I was hoping to be able to give them something to work on their way out.” (External consultant 6:62) Quote C3.17 PSIW has helped me to solve the problem so far. “I have thought about my situation and I believe that there is no need to talk about it any longer. I will take care of it by myself and if the situation with my boss doesn’t get worse I am fine.” (Service user 13:35) | 8 | 5 | 11 |
References
- OECD. Fit Mind, Fit Job: From Evidence to Practice in Mental Health and Work, Mental Health and Work; OECD Publishing: Paris, France, 2015. [Google Scholar] [CrossRef]
- Thornicroft, G.; Chatterji, S.; Evans-Lacko, S.; Gruber, M.; Sampson, N.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Andrade, L.; Borges, G.; et al. Undertreatment of people with major depressive disorder in 21 countries. Br. J. Psychiatry 2017, 210, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Clement, S.; Schauman, O.; Graham, T.; Maggioni, F.; Evans-Lacko, S.; Bezborodovs, N.; Morgan, C.; Rüsch, N.; Brown, J.S.L.; Thornicroft, G. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 2015, 45, 11–27. [Google Scholar] [CrossRef]
- Rüsch, N.; Müller, M.; Ajdacic-Gross, V.; Rodgers, S.; Corrigan, P.W.; Rössler, W. Shame, perceived knowledge and satisfaction associated with mental health as predictors of attitude patterns towards help-seeking. Epidemiol. Psychiatr. Sci. 2014, 23, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Evans-Lacko, S.; Knapp, M. Importance of Social and Cultural Factors for Attitudes, Disclosure and Time off Work for Depression: Findings from a Seven Country European Study on Depression in the Workplace. PLoS ONE 2014, 9, e91053. [Google Scholar] [CrossRef] [Green Version]
- Harris, M.G.; Baxter, A.J.; Reavley, N.; Diminic, S.; Pirkis, J.; Whiteford, H.A. Gender-related patterns and determinants of recent help-seeking for past-year affective, anxiety and substance use disorders: Findings from a national epidemiological survey. Epidemiol. Psychiatr. Sci. 2016, 25, 548–561. [Google Scholar] [CrossRef] [Green Version]
- Azagba, S.; Sharaf, M.F. Psychosocial working conditions and the utilization of health care services. BMC Public Health 2011, 11, 642–649. [Google Scholar] [CrossRef] [Green Version]
- Mack, S.; Jacobi, F.; Gerschler, A.; Strehle, J.; Höfler, M.; Busch, M.A.; Maske, U.E.; Hapke, U.; Seiffert, I.; Gäbel, W.; et al. Self-reported utilization of mental health services in the adult German population–evidence for unmet needs? Results of the DEGS1-Mental Health Module (DEGS1-MH). Int. J. Methods Psychiatr. Res. 2014, 23, 289–303. [Google Scholar] [CrossRef]
- Kroll, L.E.; Müters, S.; Lampert, T. Arbeitslosigkeit und ihre Auswirkungen auf die Gesundheit. Bundesgesundheitsblatt-Gesundheitsforsch-Gesundheitsschutz 2016, 59, 228–237. [Google Scholar] [CrossRef] [Green Version]
- Rossom, R.C.; Solberg, L.I.; Vazquez-Benitez, G.; Whitebird, R.R.; Crain, A.L.; Beck, A.; Unützer, J. Predictors of Poor Response to Depression Treatment in Primary Care. Psychiatr. Serv. 2016, 67, 1362–1367. [Google Scholar] [CrossRef]
- Fava, G.A.; Belaise, C.; Sonino, N. Psychosomatic medicine is a comprehensive field, not a synonym for consultation liaison psychiatry. Curr. Psychiatry Rep. 2010, 12, 215–221. [Google Scholar] [CrossRef]
- Andersson, B. Finding ways to the hard to reach-considerations on the content and concept of outreach work. Eur. J. Soc. Work 2013, 16, 171–186. [Google Scholar] [CrossRef]
- Azaroff, L.S.; Champagne, N.J.; Nobrega, S.; Shetty, K.; Punnett, L. Getting to know you: Occupational health researchers investigate employee assistance professionals’ approaches to workplace stress. J. Workplace Behav. Health 2010, 25, 296–319. [Google Scholar] [CrossRef]
- McLeod, J. The effectiveness of workplace counselling: A systematic review. Couns. Psychother. Res. 2010, 10, 238–248. [Google Scholar] [CrossRef]
- Joseph, B.; Walker, A.; Fuller-Tyszkiewicz, M. Evaluating the effectiveness of employee assistance programmes: A systematic review review. Eur. J. Work Organ. Psychol. 2018, 27, 1–15. [Google Scholar] [CrossRef]
- Gill, M.; Newman, R.; Redlich, F.; Sommers, M. The Initial Interview in Psychiatric Practice, with Phonograph Records Available to Professional Persons and Institutions; International University Press, Inc.: Madison, CT, USA, 1954. [Google Scholar]
- Rothermund, E.; Hölzer, M.; Wegewitz, U. Die psychosomatische Sprechstunde im Betrieb–Angebot mit Konsiliarcharakter. [The psychotherapeutic consultation in the workplace—An offer with the character of a council]. PiD-Psychother. Dialog 2018, 19, 50–54. [Google Scholar]
- Nieuwenhuijsen, K.; Faber, B.; Verbeek, J.H.; Neumeyer-Gromen, A.; Hees, H.L.; Verhoeven, A.C.; van der Feltz-Cornelis, C.M.; Bültmann, U. Interventions to improve return to work in depressed people. Cochrane Database Syst. Rev. 2014, 12, 006237. [Google Scholar] [CrossRef]
- Martin, A.; Sanderson, K.; Cocker, F. Meta-analysis of the effects of health promotion intervention in the workplace on depression and anxiety symptoms. Scand. J. Work Environ. Health 2009, 35, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Vlasveld, M.C.; van der Feltz-Cornelis, C.M.; Adèr, H.J.; Anema, J.R.; Hoedeman, R.; van Mechelen, W.; Beekman, A.T.F. Collaborative care for major depressive disorder in an occupational healthcare setting. Br. J. Psychiatry 2012, 200, 510–511. [Google Scholar] [CrossRef] [Green Version]
- Van der Feltz-Cornelis, C.M.; Hoedeman, R.; de Jong, F.J.; Meeuwissen, J.A.; Drewes, H.W.; van der Laan, N.C.; Adèr, H.J. Faster return to work after psychiatric consultation for sicklisted employees with common mental disorders compared to care as usual. A randomized clinical trial. In Neuropsychiatr. Dis. Treat; 2010; 6, pp. 375–385. Available online: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2938286&tool=pmcentrez&rendertype=abstract (accessed on 1 November 2022).
- Arends, I.; van der Klink, J.J.L.; van Rhenen, W.; de Boer, M.R.; Bültmann, U. Prevention of recurrent sickness absence in workers with common mental disorders: Results of a cluster-randomised controlled trial. Occup. Environ. Med. 2013, 71, 21–29. [Google Scholar] [CrossRef]
- Rothermund, E.; Gündel, H.; Kilian, R.; Hölzer, M.; Reiter, B.; Mauss, D.; Rieger, M.A.; Müller-Nübling, J.; Wörner, A.; von Wietersheim, J.; et al. Behandlung psychosomatischer Beschwerden im Arbeitskontext-Konzept und erste Daten. [Treatment of psychosomatic disorders occurring in the vocational context–concept and first findings]. Z. Psychosom. Med. Psychother. 2014, 60, 177–189. [Google Scholar]
- Rothermund, E.; Kilian, R.; Rottler, E.; Hölzer, M.; Mayer, D.; Rieger, M.A.; Gündel, H. Improving access to mental health care by delivering psychotherapeutic care in the workplace: A cross-sectional exploratory trial. PLoS ONE 2017, 12, e0169559. [Google Scholar] [CrossRef]
- Barrech, A.; Kilian, R.; Rottler, E.; Jerg-Bretzke, L.; Hölzer, M.; Rieger, M.; Jarczok, M.; Gündel, H.; Rothermund, E. Do working conditions of patients in psychotherapeutic consultation in the workplace differ from those in outpatient care? Results from an observational study. Int. J. Environ. Res. Public Health 2018, 15, 227. [Google Scholar] [CrossRef] [Green Version]
- Rothermund, E.; Gündel, H.; Rottler, E.; Hölzer, M.; Mayer, D.; Rieger, M.; Kilian, R. Effectiveness of psychotherapeutic consultation in the workplace: A controlled observational trial. BMC Public Health 2016, 16, 891. [Google Scholar] [CrossRef] [Green Version]
- Evans-Lacko, S.; Koeser, L.; Knapp, M.; Longhitano, C.; Zohar, J.; Kuhn, K. Evaluating the economic impact of screening and treatment for depression in the workplace. Eur. Neuropsychopharmacol. 2016, 26, 1004–1013. [Google Scholar] [CrossRef] [Green Version]
- Henderson, M.; Harvey, S.B.; Overland, S.; Mykletun, A.; Hotopf, M. Work and common psychiatric disorders. J. R. Soc. Med. 2011, 104, 198–207. [Google Scholar] [CrossRef] [Green Version]
- EU-OSHA. Second European Survey of Enterprises on New and Emerging Risks (ESENER-2) Main Findings; EU-OSHA: Bilbao, Spain, 2015; Available online: http://osha.europa.eu (accessed on 1 November 2022).
- Pomaki, G.; Franche, R.-L.; Murray, E.; Khushrushahi, N.; Lampinen, T.M. Workplace-based work disability prevention interventions for workers with common mental health conditions: A review of the literature. J. Occup. Rehabil. 2012, 22, 182–195. [Google Scholar] [CrossRef]
- Gensby, U.; Labriola, M.; Irvin, E.; Amick, B.C.; Lund, T. A classification of components of workplace disability management programs: Results from a systematic review. J. Occup. Rehabil. 2014, 24, 220–241. [Google Scholar] [CrossRef]
- Burman-Roy, S.; Butterworth, M.; Madan, I.; Henderson, M.; Harvey, S.B. Which patients are seen by an occupational psychiatry service? Occup. Med. 2013, 63, 507–509. [Google Scholar] [CrossRef] [Green Version]
- Preiser, C.; Rothermund, E.; Wittich, A.; Gündel, H.; Rieger, M.A. Psychosomatic consultation in the workplace-opportunities and limitations of the services offered. Results of a qualitative study. Int. Arch. Occup. Environ. Health 2016, 89, 599–608. [Google Scholar] [CrossRef] [Green Version]
- Bode, K.; Wunsch, E.-M.; Finger, F.; Kröger, C. Interdisciplinary care of employees with mental disorders: A fact check using the Salzgitter-Model as an example. [Interdisziplinäre Versorgung von Arbeitnehmern mit psychischen Störungen: Ein Faktencheck am Beispiel des Salzgitter-Modells]. Psychother. Psychosom. Medizinische Psychol. 2016, 66, 235–241. [Google Scholar]
- Kröger, C.; Bode, K.; Wunsch, E.; Kliem, S.; Grocholewski, A.; Finger, F. Work-related treatment for major depressive disorder and incapacity to work: Preliminary findings of a controlled, matched study. J. Occup. Health Psychol. 2015, 20, 248. [Google Scholar] [CrossRef]
- Diefenbacher, A. Psychiatry, psychosomatic medicine and the general hospital in Germany. In World Psychiatr.; 2003; 2, pp. 95–97. Available online: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1525090&tool=pmcentrez&rendertype=abstract (accessed on 1 November 2022).
- Mayer, D.; Schmidt, H.; Hölzer, M. “Psychosomatische Sprechstunde” und “Psychosomatische Grundversorgung in der Arbeitsmedizin” [„Psychotherapeutic consulation“ and „Psychotherapeutic basic care“ in occupational medicine]. Arb. Soz. Umw. 2010, 45, 593–597. [Google Scholar]
- Wege, N.; Angerer, P. Psychische Erkrankungen-Auswirkungen auf die Arbeitsfähigkeit und Versorgung psychisch erkrankter Erwerbstätiger [Mental illness - Implications for the ability to work and the care of workers with mental illnesses]. Die Psychiatr. 2013, 10, 71–81. [Google Scholar] [CrossRef]
- Preiser, C.; Wittich, A.; Rieger, M.A. Psychosomatische Sprechstunde im Betrieb--Gestaltungsformen des Angebots [Psychosomatic Consultation in the Workplace—Description and Modelling of a New Health-Related Service]. Gesundheitswesen 2015, 77, e166-71. [Google Scholar] [CrossRef] [Green Version]
- Lerner, D.; Adler, D.; Hermann, R.C.; Chang, H.; Ludman, E.J.; Greenhill, A.; Perch, K.; McPeck, W.C.; Rogers, W.H. Impact of a work-focused intervention on the productivity and symptoms of employees with depression. J. Occup. Environ. Med. 2012, 54, 128–135. [Google Scholar] [CrossRef] [Green Version]
- Martin, M.H.T.; Nielsen, M.B.D.; Petersen, S.M.; Jakobsen, L.M.; Rugulies, R. Implementation of a coordinated and tailored return-to-work intervention for employees with mental health problems. J. Occup. Rehabil. 2012, 22, 427–436. [Google Scholar] [CrossRef]
- Reme, S.E.; Grasdal, A.L.; Løvvik, C.; Lie, S.A.; Øverland, S. Work-focused cognitive–behavioural therapy and individual job support to increase work participation in common mental disorders: A randomised controlled multicentre trial. Occup. Environ. Med. 2015, 72, 745–752. [Google Scholar] [CrossRef] [Green Version]
- Balint, E.M.; Gantner, M.; Gündel, H.; Hermann, K.; Pößnecker, T.; Rothermund, E.; von Wietersheim, J. Rasche Hilfe bei psychischen Belastungen am Arbeitsplatz: Die Psychosomatische Sprechstunde im Betrieb. [Providing Rapid Help for Mental Strain at the Workplace: Psychosomatic Consultation in the Workplace]. Psychother. Psychosom. Med. Psychol. 2021, 71, 437–445. [Google Scholar] [CrossRef]
- Weber, J.; Angerer, P.; Brenner, L.; Brezinski, J.; Chysanthou, S.; Erim, Y.; Feißt, M.; Hamsmann, M.; Hondong, S.; Kessemeier, F.; et al. Early intervention, treatment and rehabilitation of employees with common mental disorders by using psychotherapeutic consultation at work: Study protocol of a randomised controlled multicentre trial (friaa project). BMC Public Health 2021, 21, 1187. [Google Scholar] [CrossRef]
- Mellor, N.; Mackay, C.; Packham, C.; Jones, R.; Palferman, D.; Webster, S.; Kelly, P. “Management Standards” and work-related stress in Great Britain: Progress on their implementation. Saf. Sci. 2011, 49, 1040–1046. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Rothermund, E.; Kilian, R.; Hölzer, M.; Mayer, D.; Mauss, D.; Krüger, M.; Rieger, M.A.; Gündel, H. “Psychosomatic consultation in the workplace”—A new model of care at the interface of company-supported mental health care and consultation-liaison psychosomatics: Design of a mixed methods implementation study. BMC Public Health 2012, 12, 780. [Google Scholar] [CrossRef]
- Strauss, A.L.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 3rd ed; CA-Sage: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Dourdouma, A.; Mörtl, K. The Creative Journey of Grounded Theory Analysis: A Guide to its Principles and Applications. Res. Psychother. Psychopathol. Process Outcome 2012, 15, 96–106. [Google Scholar] [CrossRef]
- Nielsen, K.; Miraglia, M. What works for whom in which circumstances? On the need to move beyond the ‘what works?’ question in organizational intervention research. Hum. Relat. 2017, 70, 40–62. [Google Scholar] [CrossRef] [Green Version]
- Moll, S.E. The web of silence: A qualitative case study of early intervention and support for healthcare workers with mental ill-health. BMC Public Health 2014, 14, 138. [Google Scholar] [CrossRef] [Green Version]
- Rothe, I.; Adolph, L.; Beermann, B.; Schütte, M.; Windel, A.; Grewer, A.; Lenhardt, U.; Michel, J.; Thomson, B.; Formazin, M. Psychische Gesundheit in der Arbeitswelt–Wissenschaftliche Standortbestimmung [Mental Health at the Workplace—Scientific determination of standpoint], 1st ed.; BauA: Dortmund, Germany, 2017. [Google Scholar] [CrossRef] [Green Version]
- Gulliver, A.; Griffiths, K.M.; Christensen, H.; Brewer, J.L. A systematic review of help-seeking interventions for depression, anxiety and general psychological distress (Structured abstract). BMC Psychiatr. 2012, 12, 81. Available online: http://onlinelibrary.wiley.com/o/cochrane/cldare/articles/DARE-12012044570/frame.html (accessed on 1 November 2022).
- Rothermund, E.; Michaelis, M.; Jarczok, M.N.; Balint, E.M.; Lange, R.; Zipfel, S.; Gündel, H.; Id, M.A.R.; Junne, F. Prevention of Common Mental Disorders in Employees. Perspectives on Collaboration from Three Health Care Professions. Int. J. Environ. Res. Public Health 2018, 15, 278. [Google Scholar] [CrossRef] [Green Version]
- Junne, F.; Michaelis, M.; Rothermund, E.; Stuber, F.; Gündel, H.; Zipfel, S.; Rieger, M.A. The Role of Work-Related Factors in the Development of Psychological Distress and Associated Mental Disorders: Differential Views of Human Resource Managers, Occupational Physicians, Primary Care Physicians and Psychotherapists in Germany. Int. J. Environ. Res. Public Health 2018, 15, 559. [Google Scholar] [CrossRef] [Green Version]
- Dewa, C.S.; Hoch, J.S. Barriers to Mental Health Service Use Among Workers With Depression and Work Productivity. J. Occup. Environ. Med. 2015, 57, 726–731. [Google Scholar] [CrossRef] [Green Version]
- Dalgaard, V.L.; Andersen, L.P.S.; Andersen, J.H.; Willert, M.V.; Carstensen, O.; Glasscock, D.J. Work-focused cognitive behavioral intervention for psychological complaints in patients on sick leave due to work-related stress: Results from a randomized controlled trial. J. Negat. Results Biomed. 2017, 16, 13. [Google Scholar] [CrossRef]

| Number of Participants: Total Sample N = 20 | ||
|---|---|---|
| Age | 19–30 years | 0 |
| 31–45 years | 6 | |
| 46–67 years | 14 | |
| Sex | Female | 10 |
| Male | 10 | |
| Perspective | Company health promotion team - Company doctors - Human resource staff - Members of the work council - Other (social service, case management) | 3 1 4 1 |
| Service users: Employees who experienced the offer | 5 | |
| External psychotherapist: Medical or psychological psychotherapists | 6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rothermund, E.; Pößnecker, T.; Antes, A.; Kilian, R.; Kessemeier, F.; von Wietersheim, J.; Mayer, D.; Rieger, M.A.; Gündel, H.; Hölzer, M.; et al. Conceptual Framework of a Psychotherapeutic Consultation in the Workplace: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 14894. https://doi.org/10.3390/ijerph192214894
Rothermund E, Pößnecker T, Antes A, Kilian R, Kessemeier F, von Wietersheim J, Mayer D, Rieger MA, Gündel H, Hölzer M, et al. Conceptual Framework of a Psychotherapeutic Consultation in the Workplace: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(22):14894. https://doi.org/10.3390/ijerph192214894
Chicago/Turabian StyleRothermund, Eva, Tim Pößnecker, Andreas Antes, Reinhold Kilian, Franziska Kessemeier, Jörn von Wietersheim, Dorothea Mayer, Monika A. Rieger, Harald Gündel, Michael Hölzer, and et al. 2022. "Conceptual Framework of a Psychotherapeutic Consultation in the Workplace: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 22: 14894. https://doi.org/10.3390/ijerph192214894