
Assessment of Exercise Intensity for Uphill Walking in Healthy Adults Performed Indoors and Outdoors
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Walking Test Settings
- (1)
- Maximal Borg value of at least 18 (Borgmax ≥ 18);
- (2)
- Respiratory exchange ratio of at least 1.1 (RER ≥ 1.1);
- (3)
- Maximal heart rate of at least 85% of the age-predicted HRmax using the equation: 220–age (HRmax ≥ 85%);
- (4)
- Leveling-off oxygen consumption despite an increasing workload, increase in O2 ≤ 150 mL·min−1.
2.3. Exercise Intensity Measurements
2.4. Statistical Analysis
3. Results
3.1. HR, V̇O2, and BRPE Measurements during the Walking Tests
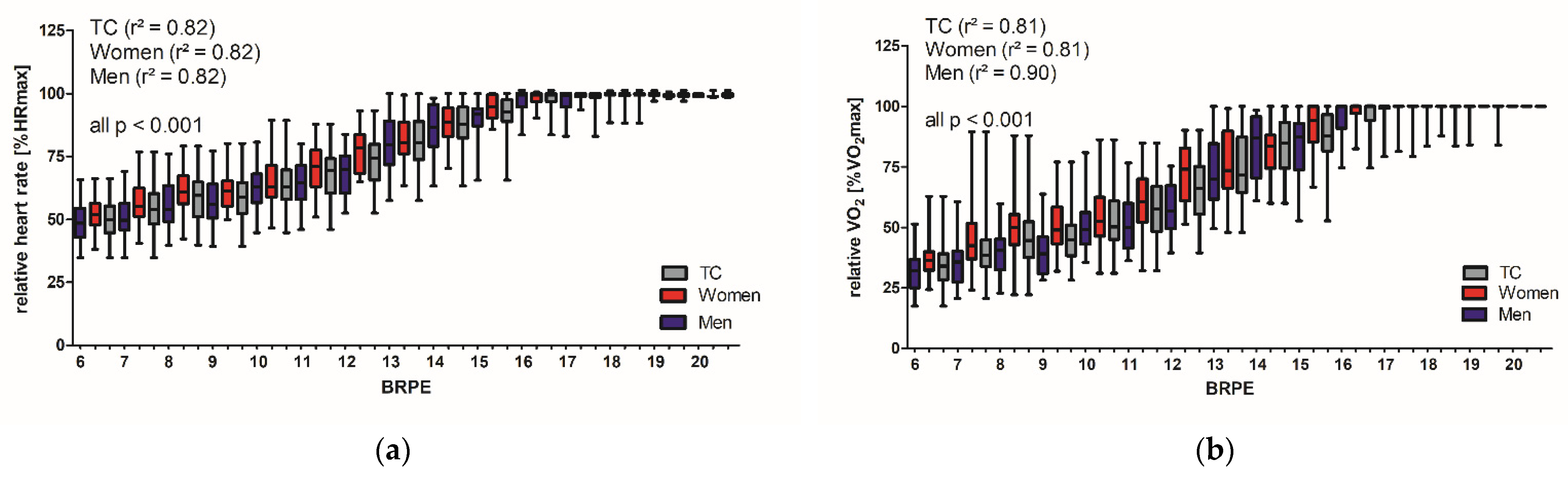
3.2. BRPE in Relation to HR and V̇O2 during the Treadmill Walking Test
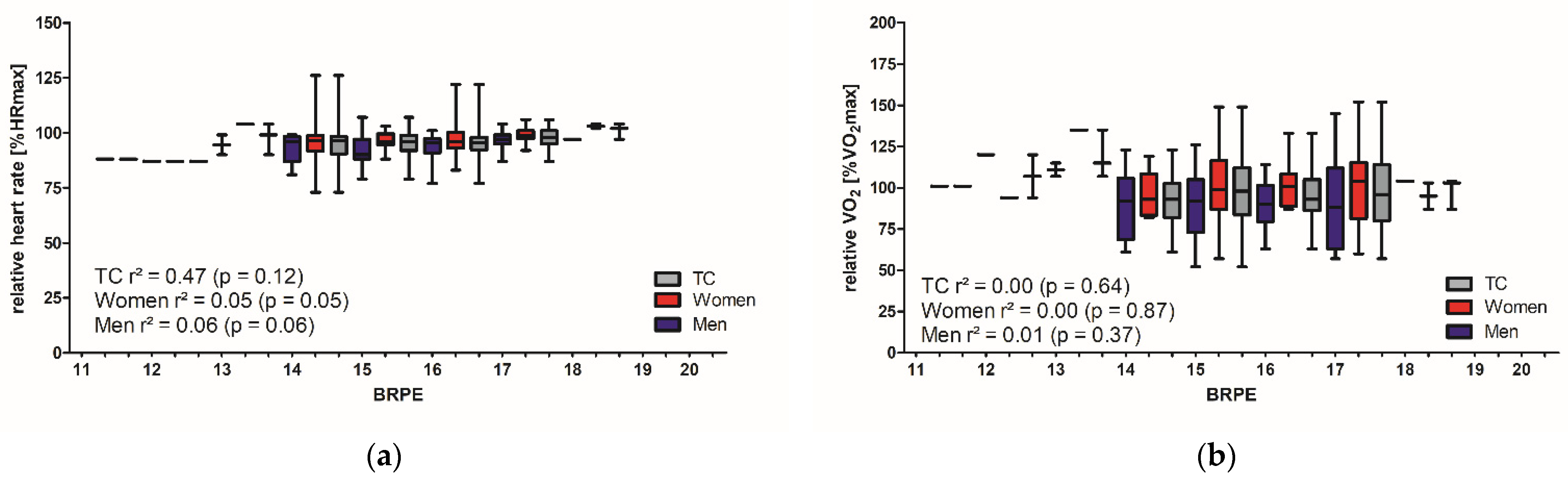
3.3. BRPE in Relation to HR and V̇O2 during the 1 km CTT
4. Discussion
4.1. Study Limitations
4.2. Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| %HRmax | Relative maximal heart rate |
| %V̇O2max | Relative maximal oxygen consumption |
| CPET | Cardiopulmonary exercise testing |
| CRF | Cardiorespiratory fitness |
| CTT | Cardio-trekking test |
| CVD | Cardiovascular disease |
| HR | Heart rate |
| HRmax | Maximal heart rate |
| PA | Physical activity |
| RER | Respiratory exchange ratio |
| RERmax | Maximal respiratory exchange ratio |
| BRPE | Borg’s rating of perceived exertion |
| BRPEmax | Maximal value of Borg’s rating of perceived exertion |
| TC | Total cohort |
| V̇O2 | Oxygen consumption |
| V̇O2max | Maximal oxygen consumption (treadmill) |
| V̇O2peak | Peak oxygen consumption (1 km CTT) |
References
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise Standards for Testing and Training. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting Physical Activity and Exercise. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for Healthier World; World Health Organization Stylus Publishing: Geneva, Switzerland; LLC [Distributor]: Herndon, VA, USA, 2019; p. 101. [Google Scholar]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex: Evidence Profiles; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Harber, M.P.; Kaminsky, L.A.; Arena, R.; Blair, S.N.; Franklin, B.A.; Myers, J.; Ross, R. Impact of Cardiorespiratory Fitness on All-Cause and Disease-Specific Mortality: Advances Since 2009. Prog. Cardiovasc. Dis. 2017, 60, 11–20. [Google Scholar] [CrossRef]
- Vuori, I.M.; Lavie, C.J.; Blair, S.N. Physical Activity Promotion in the Health Care System. Mayo Clin. Proc. 2013, 88, 1446–1461. [Google Scholar] [CrossRef] [Green Version]
- Wisloff, U.; Lavie, C.J. Taking Physical Activity, Exercise, and Fitness to a Higher Level. Prog. Cardiovasc. Dis. 2017, 60, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Albouaini, K.; Egred, M.; Alahmar, A.; Wright, D.J. Cardiopulmonary exercise testing and its application. Postgrad. Med. J. 2007, 83, 675–682. [Google Scholar] [CrossRef] [Green Version]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to Cardiopulmonary Exercise Testing in Adults. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Myers, J.; Williams, M.A.; Gulati, M.; Kligfield, P.; Balady, G.J.; Collins, E.; Fletcher, G. Assessment of Functional Capacity in Clinical and Research Settings. Circulation 2007, 116, 329–343. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.; Dahlstrom, H. A pilot study of perceived exertion and physical working capacity. Acta Soc. Med. Ups. 1962, 67, 21–27. [Google Scholar] [PubMed]
- Borg, G.; Linderholm, H. Perceived Exertion and Pulse Rate during Graded Exercise in Various Age Groups. Acta Med. Scand. 1967, 181, 194–206. [Google Scholar] [CrossRef]
- Borg, G.A. Perceived exertion: A note on “history” and methods. Med. Sci. Sports Exerc. 1973, 5, 90–93. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Hulteen, R.M.; Smith, J.J.; Morgan, P.J.; Barnett, L.M.; Hallal, P.C.; Colyvas, K.; Lubans, D.R. Global participation in sport and leisure-time physical activities: A systematic review and meta-analysis. Prev. Med. 2017, 95, 14–25. [Google Scholar] [CrossRef]
- Ciolac, E.G.; Mantuani, S.S.; Neiva, C.M.; Verardi, C.; Pessôa-Filho, D.M.; Pimenta, L. Rating of perceived exertion as a tool for prescribing and self regulating interval training: A pilot study. Biol. Sport 2015, 32, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Dunbar, C.C.; Robertson, R.J.; Baun, R.; Blandin, M.F.; Metz, K.; Burdett, R.; Goss, F.L. The validity of regulating exercise intensity by ratings of perceived exertion. Med. Sci. Sports Exerc. 1992, 24, 94–99. [Google Scholar] [CrossRef]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur. J. Appl. Physiol. 2013, 113, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Bar-or, O.; Skinner, J.S.; Buskirk, E.R.; Borg, G.A.V. Physiological and perceptual indicators of physical stress in 41-to 60-year-old men who vary in conditioning level and in body fatness. Med. Sci. Sports Exerc. 1972, 4, 96–100. [Google Scholar] [CrossRef]
- Chen, M.J.; Fan, X.; Moe, S.T. Criterion-related validity of the Borg ratings of perceived exertion scale in healthy individuals: A meta-analysis. J. Sports Sci. 2002, 20, 873–899. [Google Scholar] [CrossRef] [PubMed]
- Eston, R.; Davies, B.; Williams, J. Use of perceived effort ratings to control exercise intensity in young healthy adults. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, R.; Ueno, L.M.; Nakagaichi, M.; Nho, H.; Tanaka, K. Rate of Perceived Exertion as a Tool to Monitor Cycling Exercise Intensity in Older Adults. J. Aging Phys. Act. 2004, 12, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi Uk, L.; Tai Ryoon, H. Study on Usefulness of RPE Scale for the Prescription of Exercise Intensity. J. Korean Acad. Rehabil. Med. 1997, 21, 1167–1174. [Google Scholar]
- Physical activity and cardiovascular health. NIH Consensus Development Panel on Physical Activity and Cardiovascular Health. JAMA 1996, 276, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Wannamethee, S.G.; Shaper, A.G. Physical Activity in the Prevention of Cardiovascular Disease. Sports Med. 2001, 31, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, E.M.; Murphy, M.H.; Boone-Heinonen, J. Walking: The first steps in cardiovascular disease prevention. Curr. Opin. Cardiol. 2010, 25, 490–496. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Kelly, P.; Strain, T.; Murtagh, E.M.; Ding, D.; Murphy, M.H. Self-rated walking pace and all-cause, cardiovascular disease and cancer mortality: Individual participant pooled analysis of 50,225 walkers from 11 population British cohorts. Br. J. Sports Med. 2018, 52, 761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, M.S.; Søgaard, K.; Prescott, E.; Marott, J.L.; Schnohr, P.; Holtermann, A.; Korshøj, M. Can we walk away from cardiovascular disease risk or do we have to ‘huff and puff’? A cross-sectional compositional accelerometer data analysis among adults and older adults in the Copenhagen City Heart Study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 84. [Google Scholar] [CrossRef]
- Fredman, P.; Tyrväinen, L. Frontiers in nature-based tourism. Scand. J. Hosp. Tour. 2010, 10, 177–189. [Google Scholar] [CrossRef]
- Burtscher, M. Endurance performance of the elderly mountaineer: Requirements, limitations, testing, and training. Wien. Klin. Wochenschr. 2004, 116, 703–714. [Google Scholar] [CrossRef]
- Mitten, D.; Overholt, J.R.; Haynes, F.I.; D’Amore, C.C.; Ady, J.C. Hiking: A Low-Cost, Accessible Intervention to Promote Health Benefits. Am. J. Lifestyle Med. 2018, 12, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.; Adams, R.; Brown, T. Health benefits of hiking. Circulation 2010, 121, e1–e170. [Google Scholar]
- Noble, B.J. Clinical applications of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Eston, R.; Lambrick, D.; Sheppard, K.; Parfitt, G. Prediction of maximal oxygen uptake in sedentary males from a perceptually regulated, sub-maximal graded exercise test. J. Sports Sci. 2008, 26, 131–139. [Google Scholar] [CrossRef]
- Whaley, M.H.; Woodall, T.; Kaminsky, L.A.; Emmett, J.D. Reliability of perceived exertion during graded exercise testing in apparently healthy adults. J. Cardiopulm. Rehabil. Prev. 1997, 17, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Groslambert, A.; Mahon, A.D. Perceived exertion: Influence of age and cognitive development. Sports Med. 2006, 36, 911–928. [Google Scholar] [CrossRef]
- Garnacho-Castaño, M.V.; Domínguez, R.; Muñoz González, A.; Feliu-Ruano, R.; Serra-Payá, N.; Maté-Muñoz, J.L. Exercise Prescription Using the Borg Rating of Perceived Exertion to Improve Fitness. Int. J. Sports Med. 2018, 39, 115–123. [Google Scholar] [CrossRef]
- Whaley, M.H.; Brubaker, P.H.; Kaminsky, L.A.; Miller, C.R. Validity of Rating of Perceived Exertion During Graded Exercise Testing in Apparently Healthy Adults and Cardiac Patients. J. Cardiopulm. Rehabil. Prev. 1997, 17, 261–267. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.-P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: The Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 42, 17–96. [Google Scholar] [CrossRef]
- Mayr, B.; Beck, M.; Eisenberger, L.; Venek, V.; Kranzinger, C.; Menzl, A.; Reich, B.; Hornung-Prähauser, V.; Oberhoffer-Fritz, R.; Böhm, B.; et al. Valorization of Natural Cardio Trekking Trails Through Open Innovation for the Promotion of Sustainable Cross-generational Health-Oriented Tourism in the Connect2Move Project: Protocol for a Cross-sectional Study. JMIR Res. Protoc. 2022, 11, e39038. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, L.; Mayr, B.; Beck, M.; Venek, V.; Kranzinger, C.; Menzl, A.; Jahn, I.; Sareban, M.; Oberhoffer-Fritz, R.; Niebauer, J.; et al. Development and validation of a 1-km cardio-trekking test to estimate cardiorespiratory fitness in healthy adults. Prev. Med. Rep. 2022, 30, 102039. [Google Scholar] [CrossRef]
- Bruce, R.A.; Kusumi, F.; Hosmer, D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. Am. Heart J. 1973, 85, 546–562. [Google Scholar] [CrossRef]
- Yang, H.i.; Cho, W.; Lee, D.H.; Suh, S.-H.; Jeon, J.Y. Development of a New Submaximal Walk Test to Predict Maximal Oxygen Consumption in Healthy Adults. Sensors 2021, 21, 5726. [Google Scholar] [CrossRef] [PubMed]
- Kline, G.M.; Porcari, J.P.; Hintermeister, R.; Freedson, P.S.; Ward, A.; McCarron, R.F.; Ross, J.; Rippe, J.M. Estimation of VO2max from a one-mile track walk, gender, age, and body weight. Med. Sci. Sports Exerc. 1987, 19, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Bärtsch, P.; Saltin, B. General introduction to altitude adaptation and mountain sickness. Scand. J. Med. Sci. Sports 2008, 18 (Suppl. 1), 1–10. [Google Scholar] [CrossRef] [PubMed]
- Brocherie, F.; Girard, O.; Millet, G.P. Emerging Environmental and Weather Challenges in Outdoor Sports. Climate 2015, 3, 492–521. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Casa, D.J.; Millard-Stafford, M.; Moran, D.S.; Pyne, S.W.; Roberts, W.O. American College of Sports Medicine position stand. Exertional heat illness during training and competition. Med. Sci. Sports Exerc. 2007, 39, 556–572. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [PubMed]
- Winkert, K.; Kirsten, J.; Kamnig, R.; Steinacker, J.M.; Treff, G. Differences in VO2max Measurements Between Breath-by-Breath and Mixing-Chamber Mode in the COSMED K5. Int. J. Sports Physiol. Perform. 2021, 16, 1335–1340. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Hopkins, W.G. A New View of Statistics. Available online: https://sportsci.org/resource/stats/ (accessed on 4 November 2022).
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. (Eds.) ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA; Baltimore, MD, USA; New York, NY, USA, 2018; p. 472. [Google Scholar]
- Gondoni, L.A.; Nibbio, F.; Caetani, G.; Augello, G.; Titon, A.M. What are we measuring? Considerations on subjective ratings of perceived exertion in obese patients for exercise prescription in cardiac rehabilitation programs. Int. J. Cardiol. 2010, 140, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Travlos, A.K.; Marisi, D.Q. Perceived Exertion during Physical Exercise among Individuals High and Low in Fitness. Percept. Mot. Ski. 1996, 82, 419–424. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, M. Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 968. [Google Scholar] [CrossRef] [PubMed]
- Winborn, M.D.; Meyers, A.W.; Mulling, C. The Effects of Gender and Experience on Perceived Exertion. J. Sport Exerc. Psychol. 1988, 10, 22–31. [Google Scholar] [CrossRef]
- Eston, R.; Evans, H.; Faulkner, J.; Lambrick, D.; Al-Rahamneh, H.; Parfitt, G. A perceptually regulated, graded exercise test predicts peak oxygen uptake during treadmill exercise in active and sedentary participants. Eur. J. Appl. Physiol. 2012, 112, 3459–3468. [Google Scholar] [CrossRef] [PubMed]
- Demello, J.J.; Cureton, K.J.; Boineau, R.E.; Singh, M.M. Ratings of perceived exertion at the lactate threshold in trained and untrained men and women. Med. Sci. Sports Exerc. 1987, 19, 354–362. [Google Scholar] [CrossRef]
- Miller, G.D.; Bell, R.D.; Collis, M.L.; Hoshizaki, T.B. The relationship between perceived exertion and heart rate of post 50 year-old volunteers in two different walking activites. J. Hum. Mov. Stud. 1985, 11, 187–195. [Google Scholar]
- Grant, S. A comparison of physiological responses and rating of perceived exertion in two modes of aerobic exercise in men and women over 50 years of age. Br. J. Sports Med. 2002, 36, 276–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flairty, J.E.; Scheadler, C.M. Perceived and Heart Rate-based Intensities during Self-paced Walking: Magnitudes and Comparison. Int. J. Exerc. Sci. 2020, 13, 677–688. [Google Scholar] [PubMed]
- Hassmén, P. Environmental effects on the ratings of perceived exertion in males and females. J. Sport Behav. 1996, 19, 235. [Google Scholar]
- Ceci, R.; Hassmén, P. Self-monitored exercise at three different RPE intensities in treadmill vs field running. Med. Sci. Sports Exerc. 1991, 23, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Krinski, K.; Machado, D.G.S.; Lirani, L.S.; DaSilva, S.G.; Costa, E.C.; Hardcastle, S.J.; Elsangedy, H.M. Let’s Walk Outdoors! Self-Paced Walking Outdoors Improves Future Intention to Exercise in Women With Obesity. J. Sport Exerc. Psychol. 2017, 39, 145–157. [Google Scholar] [CrossRef]
- Faulkner, J.; Parfitt, G.; Eston, R. Prediction of maximal oxygen uptake from the ratings of perceived exertion and heart rate during a perceptually-regulated sub-maximal exercise test in active and sedentary participants. Eur. J. Appl. Physiol. 2007, 101, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Pincivero, D.M.; Polen, R.R.; Byrd, B.N. Gender and contraction mode on perceived exertion. Int. J. Sports Med. 2010, 31, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Ekkekakis, P. Let them roam free? Physiological and psychological evidence for the potential of self-selected exercise intensity in public health. Sports Med. (Auckland, N.Z.) 2009, 39, 857–888. [Google Scholar] [CrossRef] [PubMed]
- Rose, E.A.; Parfitt, G. Can the feeling scale be used to regulate exercise intensity? Med. Sci. Sports Exerc. 2008, 40, 1852–1860. [Google Scholar] [CrossRef]
- Rose, E.A.; Parfitt, G. Exercise experience influences affective and motivational outcomes of prescribed and self-selected intensity exercise. Scand. J. Med. Sci. Sports 2012, 22, 265–277. [Google Scholar] [CrossRef]
- Marsh, A.P.; Katula, J.A.; Pacchia, C.F.; Johnson, L.C.; Koury, K.L.; Rejeski, W.J. Effect of treadmill and overground walking on function and attitudes in older adults. Med. Sci. Sports Exerc. 2006, 38, 1157–1164. [Google Scholar] [CrossRef]
- Parvataneni, K.; Ploeg, L.; Olney, S.J.; Brouwer, B. Kinematic, kinetic and metabolic parameters of treadmill versus overground walking in healthy older adults. Clin. Biomech. (Bristol, Avon) 2009, 24, 95–100. [Google Scholar] [CrossRef]
- Pearce, M.E.; Cunningham, D.A.; Donner, A.P.; Rechnitzer, P.A.; Fullerton, G.M.; Howard, J.H. Energy cost of treadmill and floor walking at self-selected paces. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 52, 115–119. [Google Scholar] [CrossRef]
- Dasilva, S.G.; Guidetti, L.; Buzzachera, C.F.; Elsangedy, H.M.; Krinski, K.; De Campos, W.; Goss, F.L.; Baldari, C. Psychophysiological responses to self-paced treadmill and overground exercise. Med. Sci. Sports Exerc. 2011, 43, 1114–1124. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Percent Grad (%) | Speed (km·h−1) | |
|---|---|---|
| Stage 1 | 0 | 2.7 |
| Stage 2 | 5 | 2.7 |
| Stage 3 | 10 | 2.7 |
| Stage 4 | 12 | 4.0 |
| Stage 5 | 14 | 5.4 |
| Stage 6 | 16 | 6.7 |
| Stage 7 | 18 | 8.0 |
| Stage 8 | 20 | 8.8 |
| 6 | |
| 7 | Very, very light |
| 8 | |
| 9 | Very light |
| 10 | |
| 11 | Fairly light |
| 12 | |
| 13 | Somewhat hard |
| 14 | |
| 15 | Hard |
| 16 | |
| 17 | Very hard |
| 18 | |
| 19 | Very, very hard |
| 20 |
| Total Cohort (n = 134) | Men (n = 58) | Women (n = 76) | p | |
|---|---|---|---|---|
| Anthropometrics Age (years) | 56 [52–63] | 56 [52–62] | 57 [51–63] | <0.731 1 |
| Height (cm) | 171.6 [8.4] | 178.4 [6.9] | 166.5 [5.2] | |
| Weight (kg) | 71.1 [13.3] | 80.6 [11.2] | 63.8 [9.8] | |
| BMI (kg/m2) | 24.0 [3.4] | 25.3 [2.8] | 23.0 [3.5] | <0.001 *,1 |
| Total Cohort (n = 134) | Men (n = 58) | Women (n = 76) | p | |
|---|---|---|---|---|
| Exercise capacity on the treadmill | ||||
| V̇O2max (mL·min−1·kg−1) | 39.3 [7.7] | 42.8 [8.6] | 36.6 [5.8] | <0.001 *,1 |
| HRmax (bpm) | 165 [14] | 165 [16] | 165 [12] | 0.834 1 |
| RERmax | 1.1 [0.1] | 1.1 [0.1] | 1.1 [0.1] | 0.907 1 |
| Borgmax | 18 [17–19] | 18 [17–19] | 17 [17,18] | 0.180 2 |
| vmax (km·h−1) | 5.6 [5.0–5.9] | 5.8 [5.6–6.3] | 5.4 [4.9–5.8] | <0.001 *,2 |
| Exercise capacity in the 1 km CTT | ||||
| V̇O2peak (mL·min−1·kg−1) | 37.3 [6.3] | 40.2 [6.1] | 35.1 [5.6] | <0.001 *,1 |
| HRpeak (bpm) | 157 [15] | 154 [15] | 160 [14] | <0.01 *,1 |
| RERpeak | 1.1 [1.0–1.2] | 1.1 [1.0–1.2] | 1.1 [1.0–1.1] | 0.724 2 |
| Borgpeak | 15 [15,16] | 16 [15,16] | 15 [15,16] | 0.687 2 |
| vpeak (km·h−1) | 6.4 [5.7–7.2] | 6.8 [5.9–7.3] | 6.3 [5.4–7.0] | <0.05 *,2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eisenberger, L.; Mayr, B.; Beck, M.; Venek, V.; Kranzinger, C.; Menzl, A.; Jahn, I.; Sareban, M.; Oberhoffer-Fritz, R.; Niebauer, J.; et al. Assessment of Exercise Intensity for Uphill Walking in Healthy Adults Performed Indoors and Outdoors. Int. J. Environ. Res. Public Health 2022, 19, 16662. https://doi.org/10.3390/ijerph192416662
Eisenberger L, Mayr B, Beck M, Venek V, Kranzinger C, Menzl A, Jahn I, Sareban M, Oberhoffer-Fritz R, Niebauer J, et al. Assessment of Exercise Intensity for Uphill Walking in Healthy Adults Performed Indoors and Outdoors. International Journal of Environmental Research and Public Health. 2022; 19(24):16662. https://doi.org/10.3390/ijerph192416662
Chicago/Turabian StyleEisenberger, Laura, Barbara Mayr, Maximilian Beck, Verena Venek, Christina Kranzinger, Andrea Menzl, Inga Jahn, Mahdi Sareban, Renate Oberhoffer-Fritz, Josef Niebauer, and et al. 2022. "Assessment of Exercise Intensity for Uphill Walking in Healthy Adults Performed Indoors and Outdoors" International Journal of Environmental Research and Public Health 19, no. 24: 16662. https://doi.org/10.3390/ijerph192416662