

Acoustic Biotopes, Listeners and Sound-Induced Action: A Case Study of Operating Rooms

 ,
,
Abstract
:1. Introduction
This Paper and the Use Case
2. Background into Listening in Complex Sound Environments
2.1. OR as a Rich Sound Environment
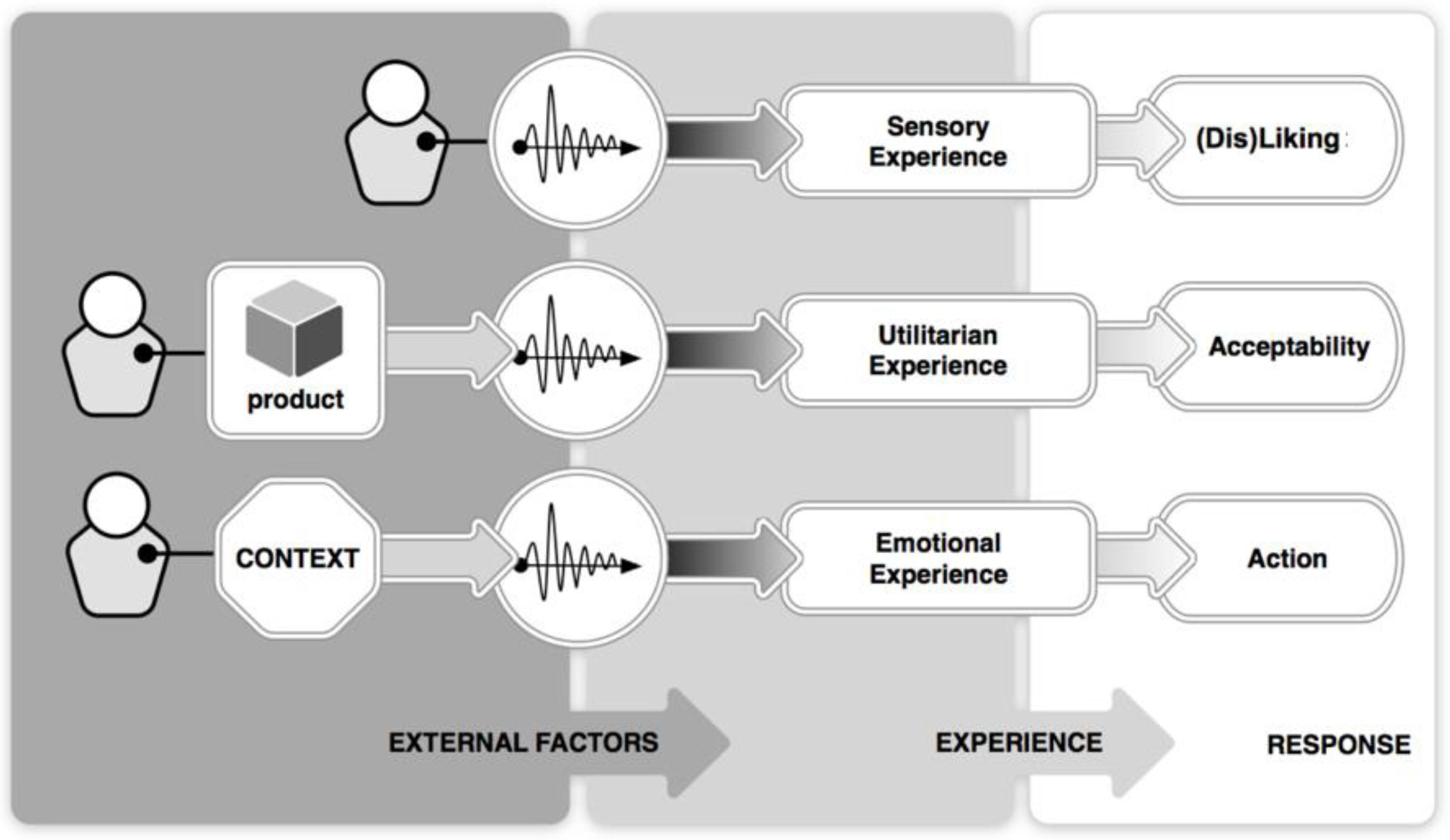
2.2. Listeners and Sound Environments
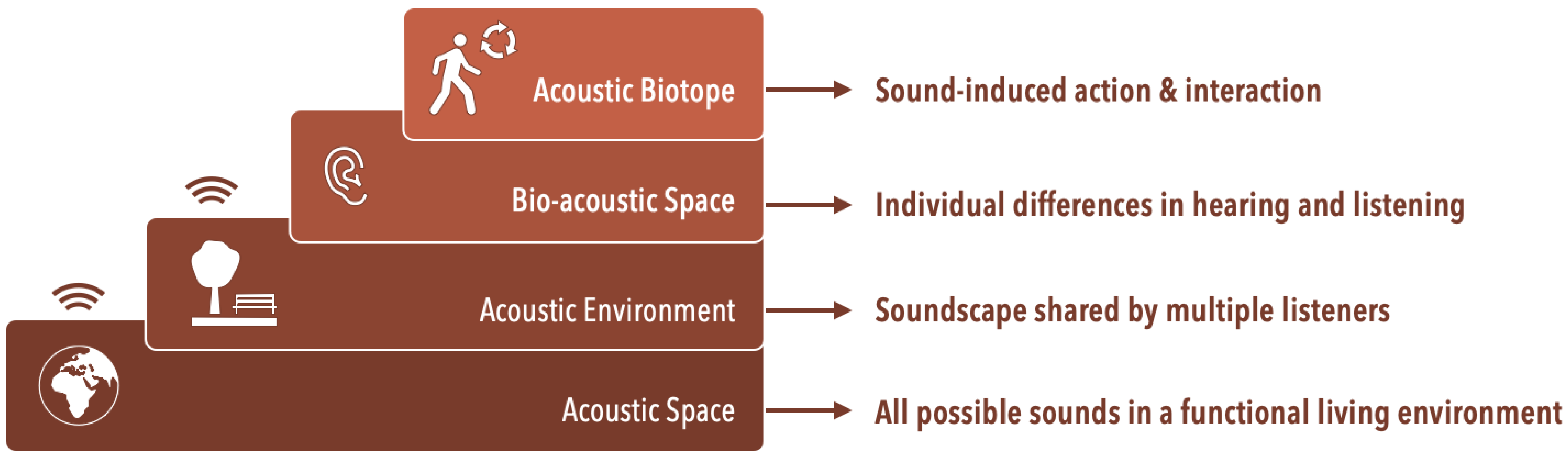
2.3. From Acoustic Space to Bio Acoustic Space and Acoustic Biotopes
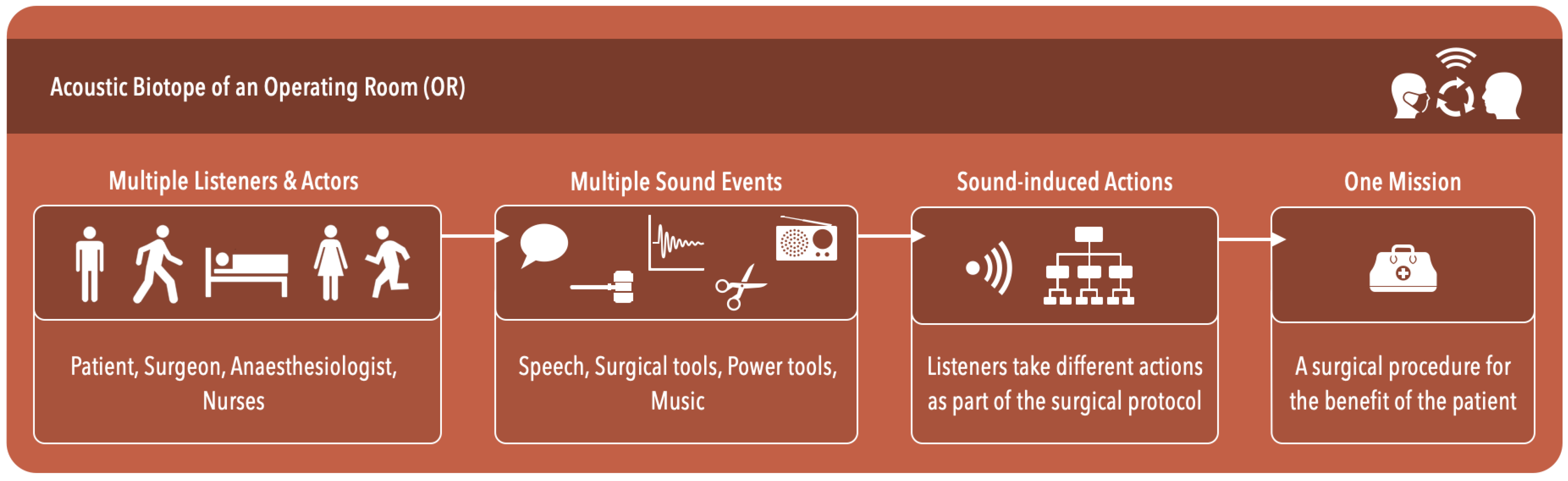
2.4. Acoustic Biotopes of Operating Rooms
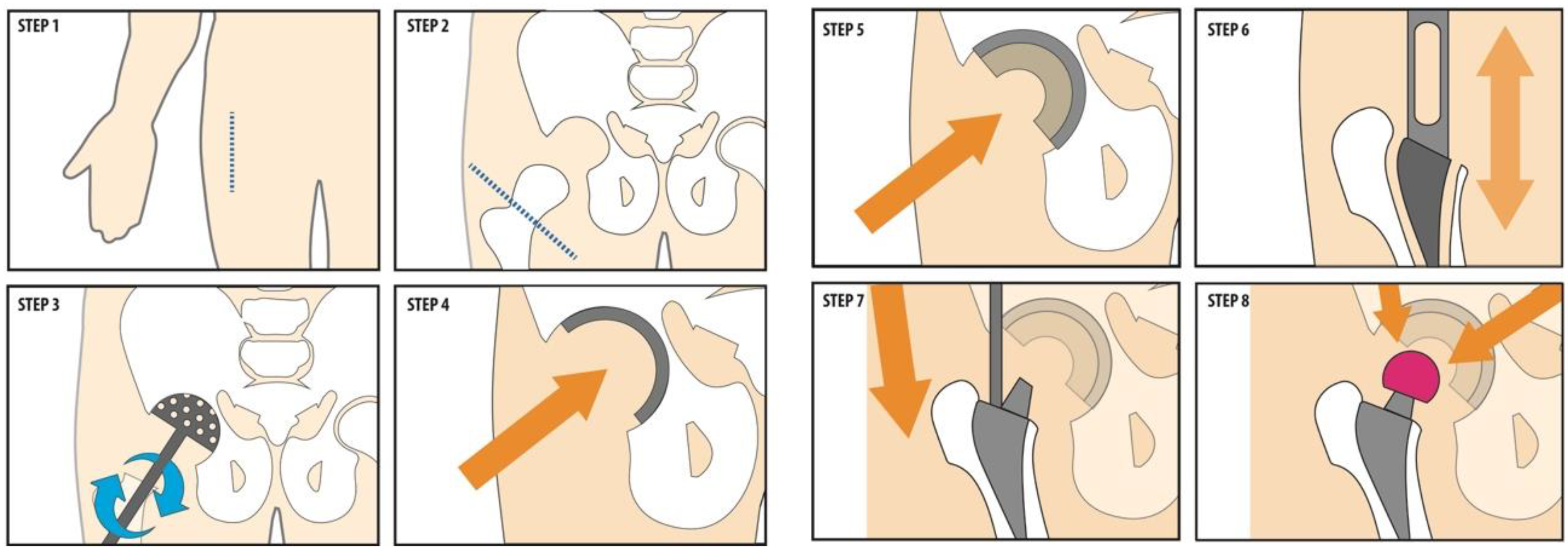
3. Observational Study in an Orthopaedic OR
3.1. Method
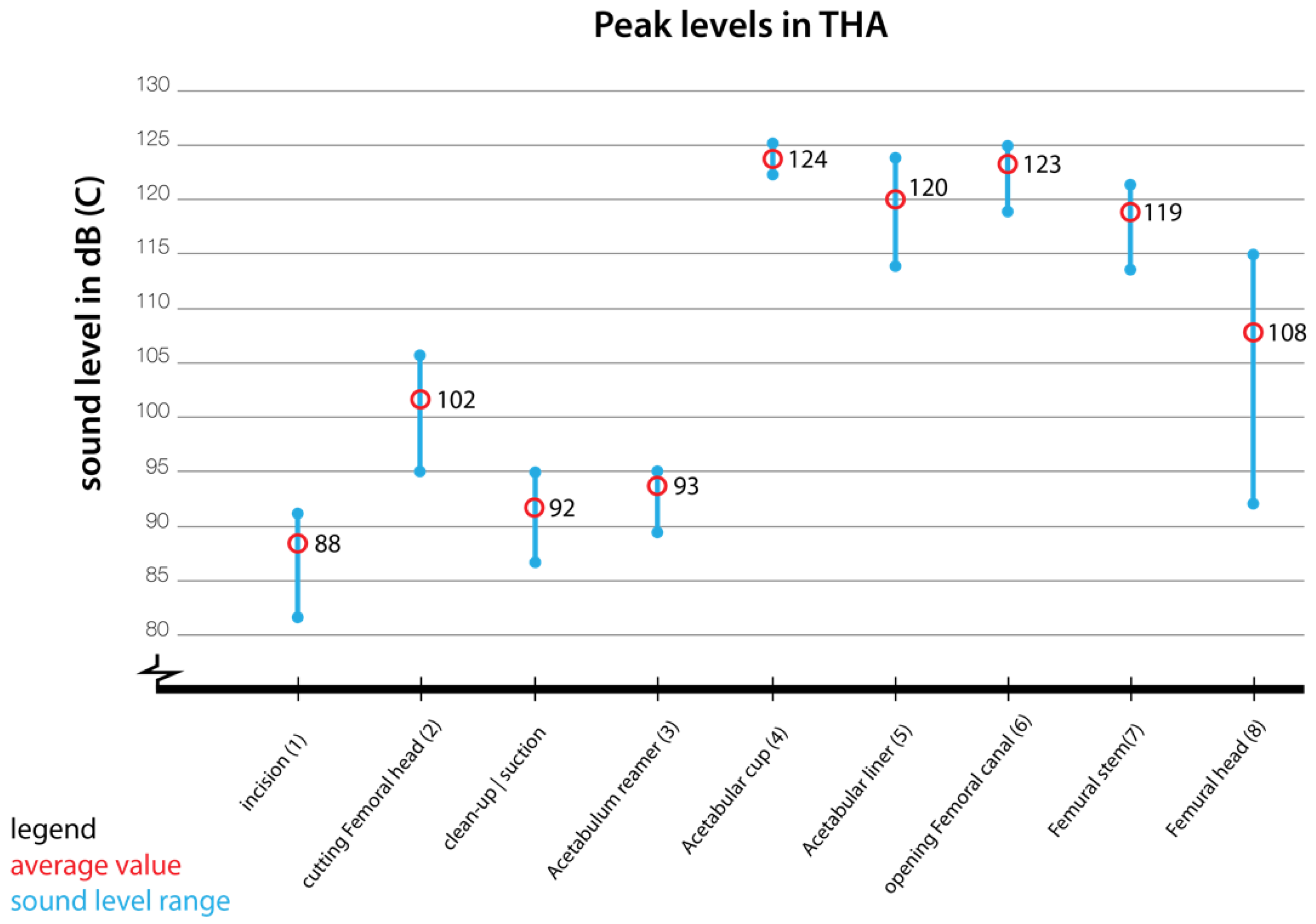
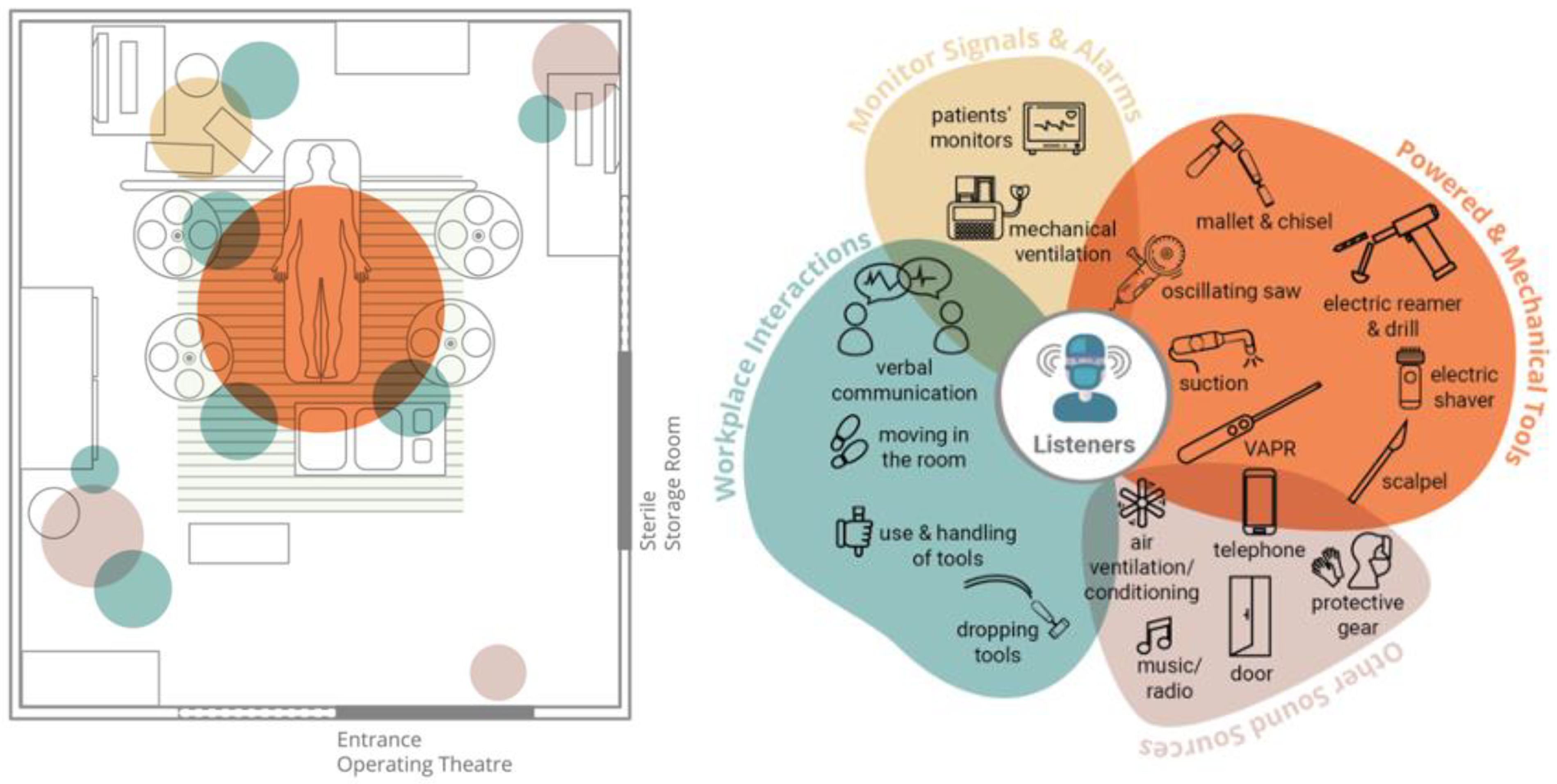
3.2. Sound Measurements and Sound Sources

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| dB(A)-LAeq | 21.10/1 | 21.10/3 | 21.10/4 | 01.11/1 | 01.11/2 | 14.11/1 | 14.11/2 | Range | Average (log) | Set Average |
|---|---|---|---|---|---|---|---|---|---|---|
| Incision | 66.8 | 65.3 | 61.1 | 64.7 | 67.2 | 57.3 | 60.2 | 57–67 | 64.1 | 64 |
| Saw (osc) | 68.4 | 84.2 | 74.6 | 84.7 | 83.2 | 79.6 | 76.4 | 68-85 | 81.3 | 81 |
| Clean-up/suction | 72.2 | 65.8 | 64.6 | 66.6 | 63.2 | 62.6 | 69 | 63–73 | 67.7 | 68 |
| Reamer (elec) | 72.2 | 70.5 | 66.1 | 64.3 | 67.1 | 68.2 | 67.1 | 64–72 | 68.7 | 69 |
| Pelvis cup tit | 85.7 | 90.8 | 87.7 | 94.4 | 90.3 | 86.6 | 80.5 | 80–95 | 89.7 | 90 |
| Pelvis cup | 78.8 | 83.4 | 80.6 | 88.4 | 86 | 87 | 80.3 | 78–89 | 84.8 | 85 |
| Rasp. femur | 95.4 | 94 | 85.4 | 97.7 | 101.4 | 88.1 | 88.3 | 85–102 | 95.9 | 96 |
| Femur stem | 79.4 | 78.3 | 81.2 | 83.6 | 86 | 81.1 | 81.4 | 78–86 | 82.3 | 82 |
| Ball fix | 77 | 68.7 | 68.9 | 69.8 | 66.3 | 75.6 | 64 | 64–77 | 72.3 | 72 |
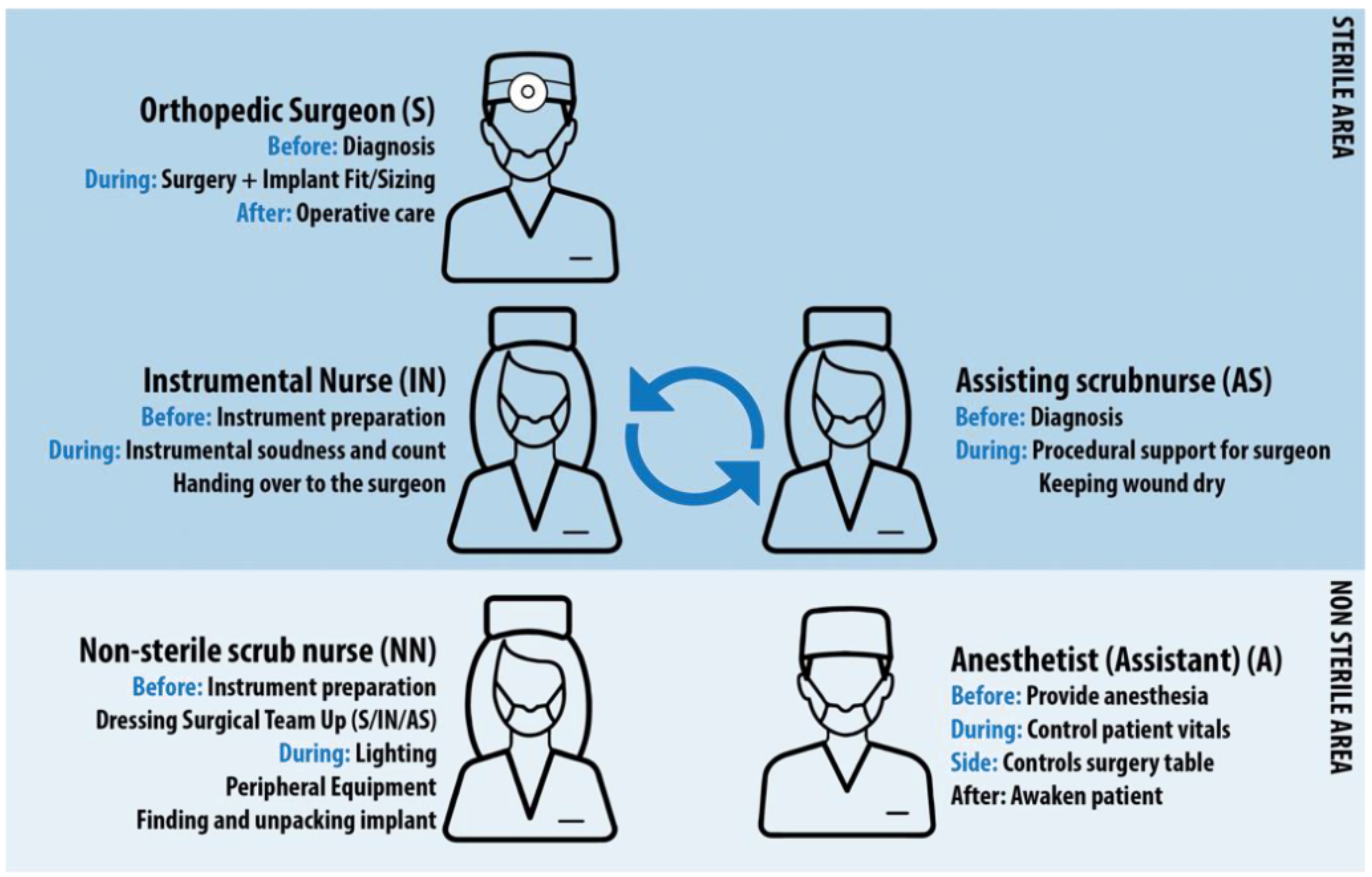
3.3. Task Analysis
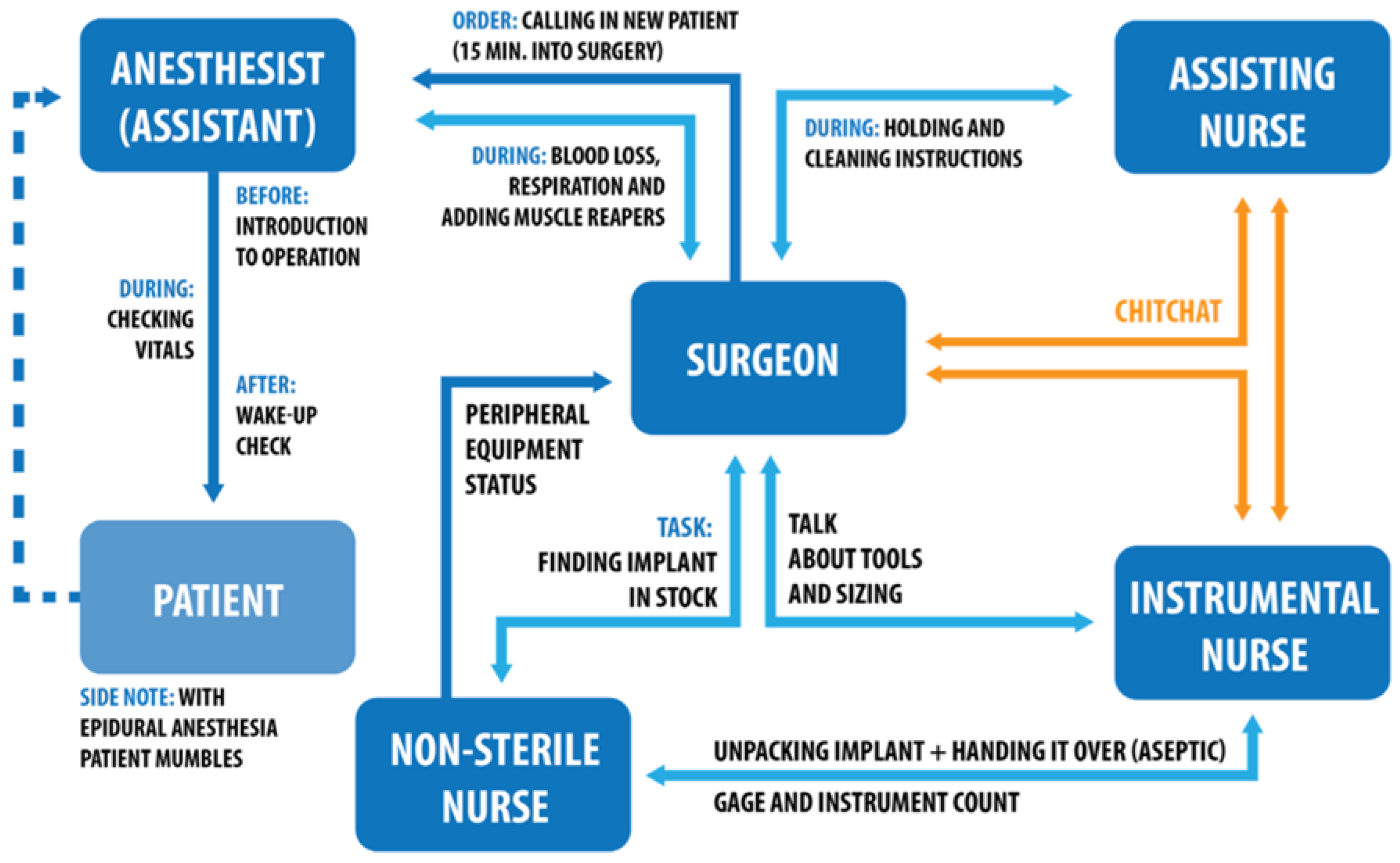
3.4. Information Flow
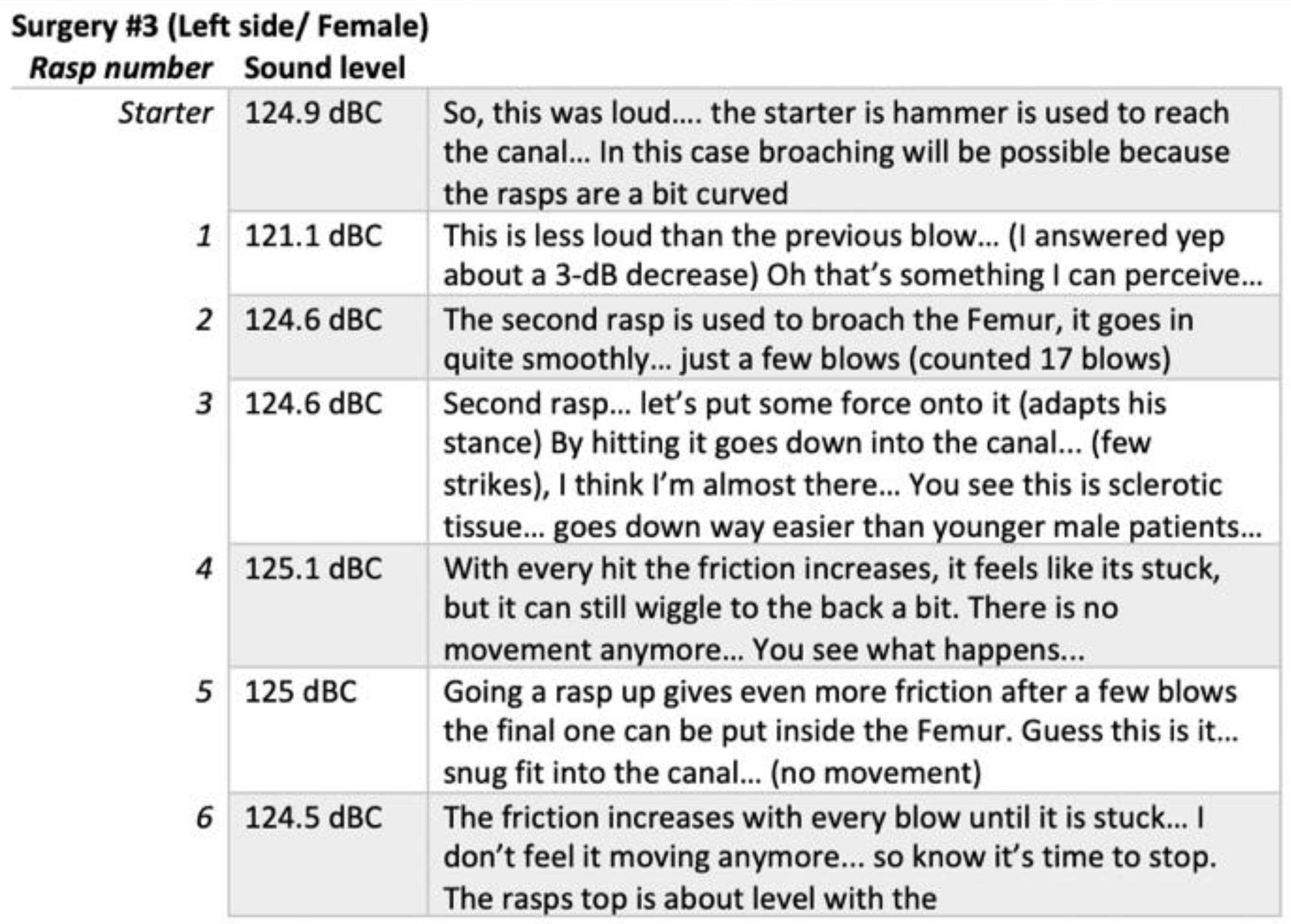
3.5. Auditory Cues and Instrument Feedback
3.6. Sound as a Tool for Surgeries
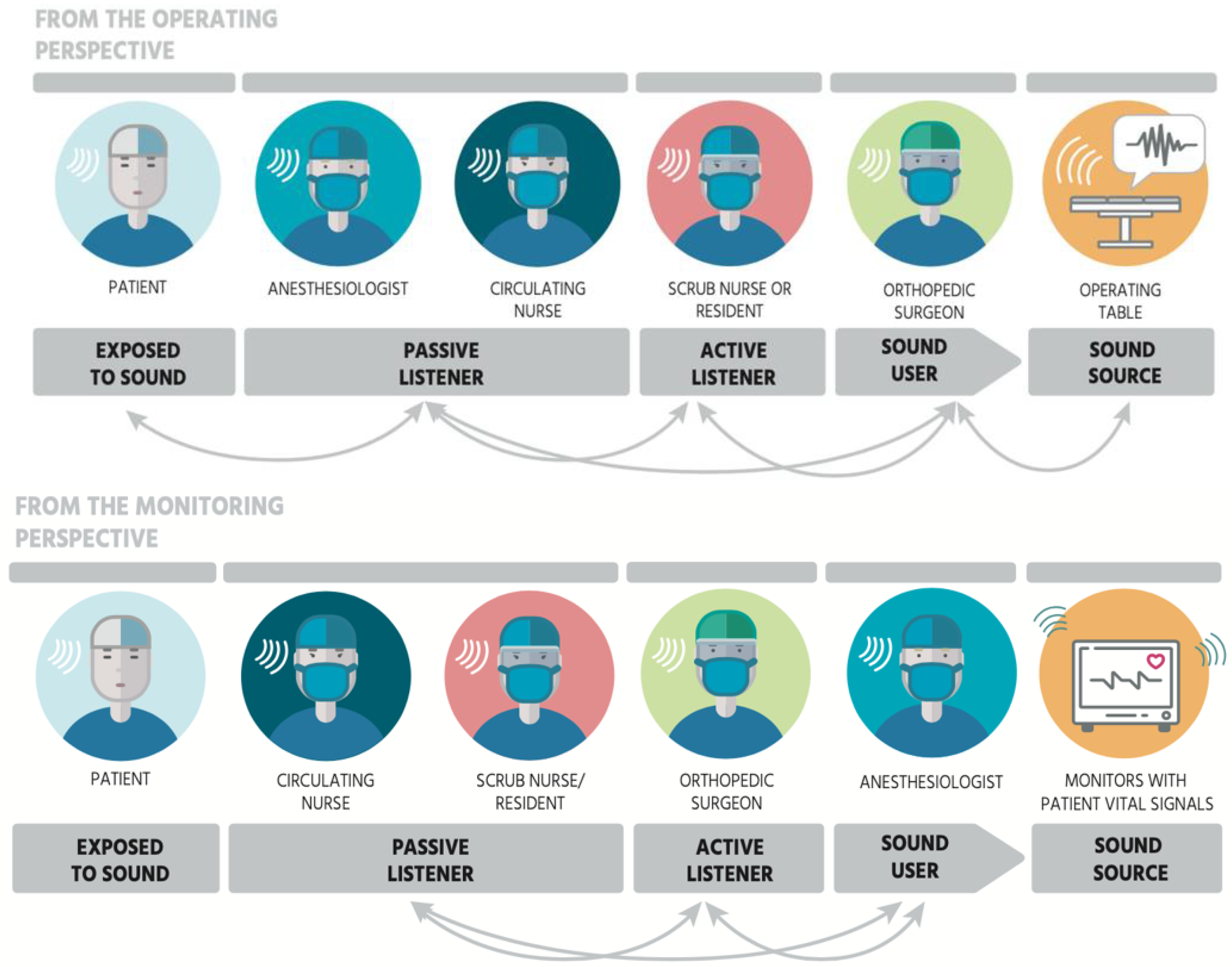
3.7. Types of Listeners within the OR
4. The Main Elements of Acoustic Biotopes of ORs
4.1. Listeners as Actors in an Acoustic Space
4.2. Sound Producing Events in the Acoustic Environment
4.3. Locals of Sound and Localizability in the Acoustic Environment
4.4. Listening Capacity within the Bio-Acoustic Space
4.5. Common Goal within the Acoustic Biotope
4.6. Interactions with and via Sounds in the Acoustic Biotope
5. Key Takeaways for Acoustic Biotopes
- Acoustic biotopes of socio-technological environments should be considered as functional professional settings in which teams collectively and individually strive for the success of the mission and the local tasks through sound-induced action.
- Listening in highly functional environments is an individual experience and is influenced by hearing function, physical position and role in an environment, and the task at hand. Other sound events in the environment and their spectro-temporal structure will influence hearing as well but would be considered as an external factor that could affect all listeners at a varying degree.
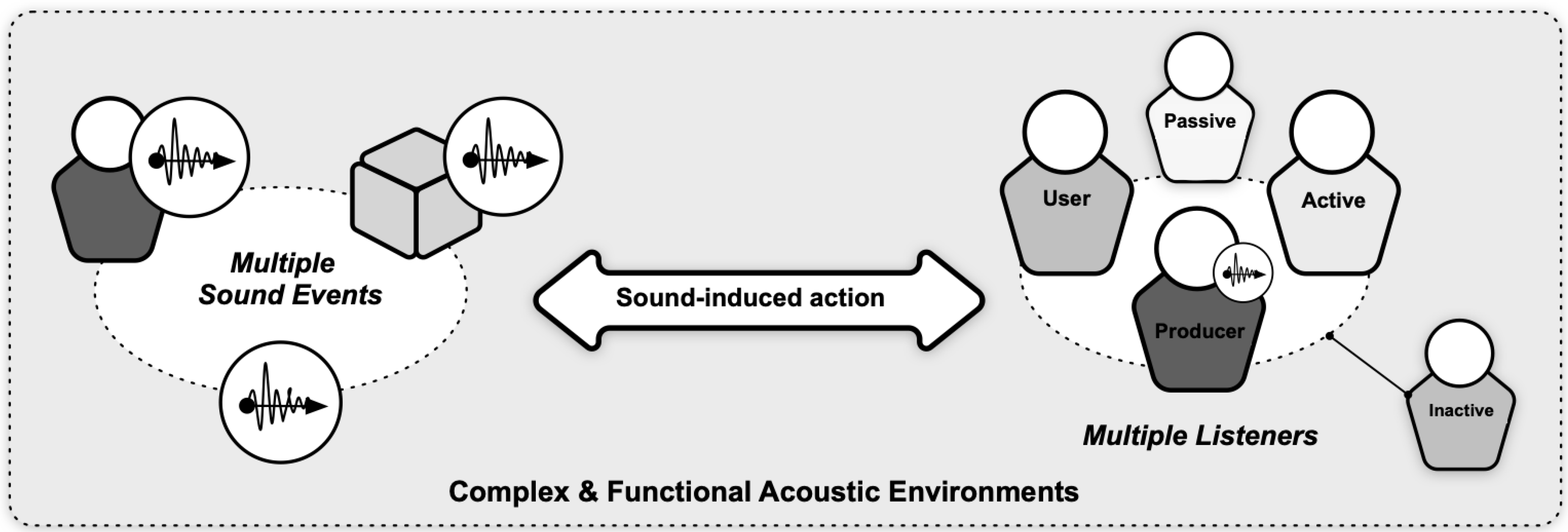
- Acoustic biotopes facilitate all kinds of interactions with sounds, system tools and team members via sound, and must offer opportunities for sound-induced action for all types of listeners.
- There are many different sound sources in the socio-technological environments and all of which can be used by different actors in different ways. Different uses of sound should be defined in relation to listener actions.
- In acoustic biotopes, there are different locals of sound events with different sound intensities and complexities as a result of the concentration of tasks. These sound zones are rich with sound-induced action and should be well organized.
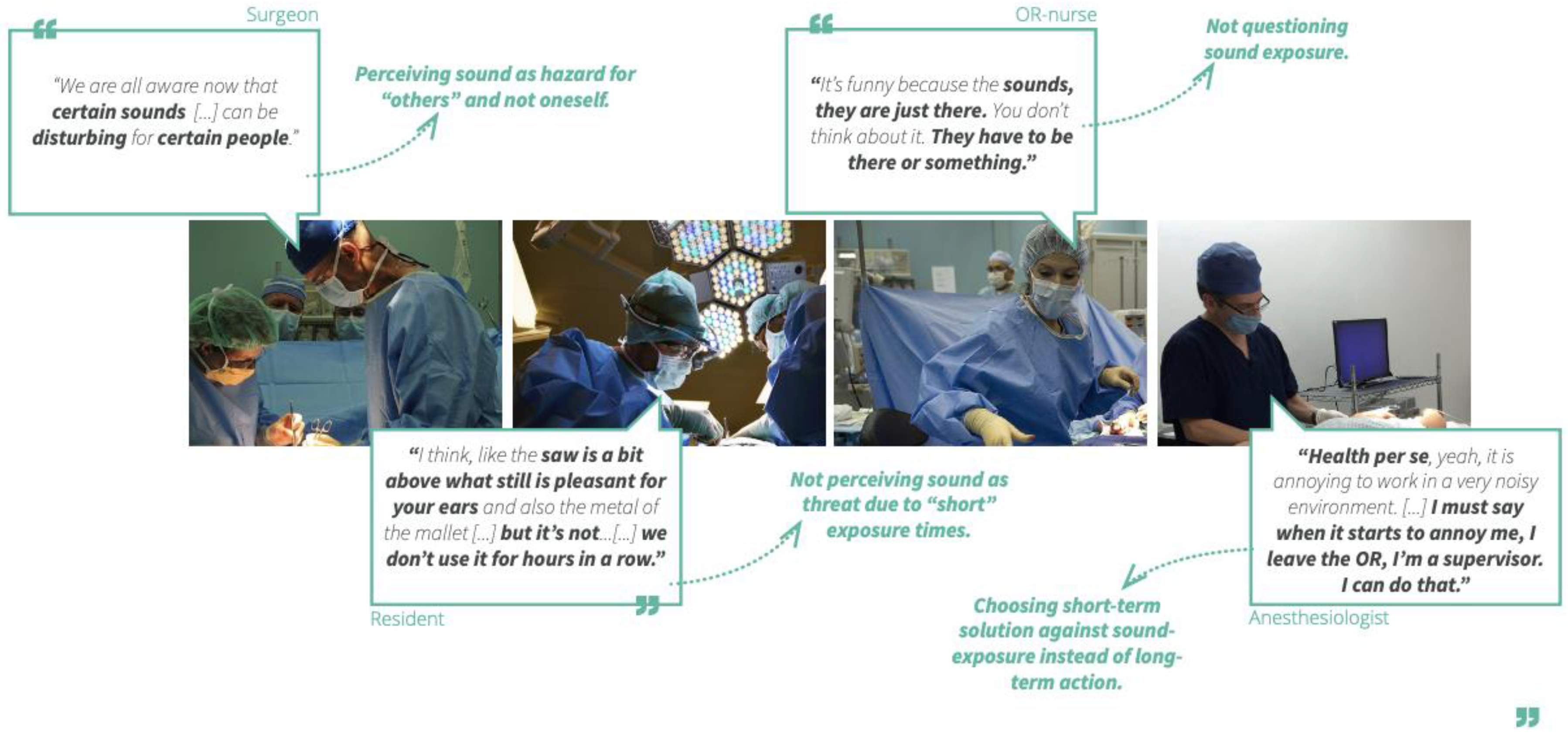
- Power tools, music, and verbal communication emit the loudest perceived sounds within the acoustic biotopes and some of these sound sources can be harmful for listeners.
- There is a range of active, passive and inactive sound listeners as a function of their attentive state and listeners as sound user as well as sound producers within the acoustic biotope. It is important to define these dynamics of how and when listeners switch attention and change the way they listen for assigning relevant tasks.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van den Bosch, K.A.-M.; Welch, D.; Andringa, T.C. The Evolution of Soundscape Appraisal Through Enactive Cognition. Front. Psychol. 2018, 9, 1129. [Google Scholar] [CrossRef] [Green Version]
- Tuuri, K.; Eerola, T. Formulating a Revised Taxonomy for Modes of Listening. J. New Music. Res. 2012, 41, 137–152. [Google Scholar] [CrossRef]
- Dubois, D. Categories as acts of meaning: The case of categories in olfaction and audition. Cogn. Sci. Q. 2000, 1, 35–68. [Google Scholar]
- Paine, G.; Bevilacqua, F.; Matuszewski, B. Editorial: Collective and networked sound practices. Organ. Sound 2021, 26, 303–304. [Google Scholar] [CrossRef]
- Langeveld, L.; van Egmond, R.; Jansen, R.; Özcan, E. Product sound design: Intentional and consequential sounds. In Advances in Industrial Design Engineering; Intech Open: London, UK, 2013; p. 47. [Google Scholar]
- Özcan, E. Product Sounds: Fundamentals & Application. Ph.D. Thesis, Delft University of Technology, Delft, The Netherlands, 2008. [Google Scholar]
- Jennings, P.; Cain, R. A framework for improving urban soundscapes. Appl. Acoust. 2013, 74, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Edworthy, J.R.; McNeer, R.R.; Bennett, C.L.; Dudaryk, R.; McDougall, S.J.P.; Schlesinger, J.J.; Bolton, M.L.; Edworthy, J.D.R.; Özcan, E.; Boyd, A.D.; et al. Getting Better Hospital Alarm Sounds into a Global Standard. Ergon. Des. Q. Hum. Factors Appl. 2018, 26, 4–13. [Google Scholar] [CrossRef]
- Monache, S.D.; Misdariis, N.; Ozcan, E. Conceptualising sound-driven design: An exploratory discourse analysis. Creat. Cogn. 2021, 1–8. [Google Scholar] [CrossRef]
- Monache, S.D.; Misdariis, N.; Özcan, E. Semantic models of sound-driven design: Designing with listening in mind. Des. Stud. 2022, 83, 101134. [Google Scholar] [CrossRef]
- Sleeswijk Visser, F.; Stappers, P.J.; Van Der Lugt, R.; Sanders, E.B.-N. Contextmapping: Experiences from practice. CoDesign 2005, 1, 119–149. [Google Scholar] [CrossRef]
- Johannesma, P.; Aertsen, A. Statistical and dimensional analysis of the neural representation of the acoustic biotope of the frog. J. Med. Syst. 1982, 6, 399–421. [Google Scholar] [CrossRef]
- Smolders, J.W.T.; Aertsen, A.M.H.J.; Johannesma, P.I.M. Neural representation of the acoustic biotope. Biol. Cybern. 1979, 35, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Schafer, R. The Tuning of the World; Knopf: New York, NY, USA, 1977. [Google Scholar]
- Grinfeder, E.; Lorenzi, C.; Haupert, S.; Sueur, J. What Do We Mean by “Soundscape”? A Functional Description. Front. Ecol. Evol. 2022, 10, 894232. [Google Scholar] [CrossRef]
- Farina, A.; Eldridge, A.; Li, P. Ecoacoustics and multispecies semiosis: Naming, semantics, semiotic characteristics, and competencies. Biosemiotics 2021, 14, 141–165. [Google Scholar] [CrossRef]
- Sueur, J.; Krause, B.; Farina, A. Acoustic biodiversity. Curr. Biol. 2021, 31, R1172–R1173. [Google Scholar] [CrossRef] [PubMed]
- Özcan, E.; Rietdijk, W.J.R.; Gommers, D. Shaping critical care through sound-driven innovation: Introduction, outline, and research agenda. Intensiv. Care Med. 2020, 46, 542–543. [Google Scholar] [CrossRef]
- Love, H. Noise exposure in the orthopaedic operating theatre: A significant health hazard. ANZ J. Surg. 2003, 73, 836–838. [Google Scholar] [CrossRef]
- Basner, M.; Dinges, D.F.; Mollicone, D.J.; Savelev, I.; Ecker, A.J.; Antonio, A.D.; Sutton, J.P. Psychological and Behavioral Changes during Confinement in a 520-Day Simulated Interplanetary Mission to Mars. PLoS ONE 2014, 9, e93298. [Google Scholar] [CrossRef] [Green Version]
- Rylander, R. Physiological aspects of noise-induced stress and annoyance. J. Sound Vib. 2004, 277, 471–478. [Google Scholar] [CrossRef]
- Wetzel, C.M.; Kneebone, R.L.; Woloshynowych, M.; Nestel, D.; Moorthy, K.; Kidd, J.; Darzi, A. The effects of stress on surgical performance. Am. J. Surg. 2006, 191, 5–10. [Google Scholar] [CrossRef]
- Szalma, J.L.; Hancock, P.A. Noise effects on human performance: A meta-analytic synthesis. Psychol. Bull. 2011, 137, 682–707. [Google Scholar] [CrossRef] [Green Version]
- Murthy, V.S.S.N.; Malhotra, S.K.; Bala, I.; Raghunathan, M. Detrimental effects of noise on anaesthetists. Can. J. Anaesth. 1995, 42, 608–611. [Google Scholar] [CrossRef]
- Zimmer, K.; Ghani, J.; Ellermeier, W. The role of task interference and exposure duration in judging noise annoyance. J. Sound Vib. 2008, 311, 1039–1051. [Google Scholar] [CrossRef] [Green Version]
- Kracht, J.M.; Busch-Vishniac, I.J.; West, J.E. Noise in the operating rooms of Johns Hopkins Hospital. J. Acoust. Soc. Am. 2007, 121, 2673–2680. [Google Scholar] [CrossRef]
- Hasfeldt, D.; Laerkner, E.; Birkelund, R. Noise in the Operating Room-What Do We Know? A Review of the Literature. J. PeriAnesthesia Nurs. 2010, 25, 380–386. [Google Scholar] [CrossRef]
- Bleakley, A.; Allard, J.; Hobbs, A. ‘Achieving ensemble’: Communication in orthopaedic surgical teams and the development of situation awareness-an observational study using live videotaped examples. Adv. Health Sci. Educ. 2013, 18, 33–56. [Google Scholar] [CrossRef]
- Heron, J.; Whitaker, D.; McGraw, P. Sensory uncertainty governs the extent of audio-visual interaction. Vis. Res. 2004, 44, 2875–2884. [Google Scholar] [CrossRef] [Green Version]
- Keller, S.; Tschan, F.; Beldi, G.; Kurmann, A.; Candinas, D.; Semmer, N.K. Noise peaks influence communication in the operating room. An observational study. Ergonomics 2016, 59, 1541–1552. [Google Scholar] [CrossRef]
- Darzi, A.; Munz, Y.; Dosis, A.; Bann, S.; Moorthy, K. The effect of stress-inducing conditions on the performance of a laparoscopic task. Surg. Endosc. 2003, 17, 1481–1484. [Google Scholar] [CrossRef]
- Hsu, K.E.; Man, F.-Y.; Gizicki, R.A.; Feldman, L.S.; Fried, G.M. Experienced surgeons can do more than one thing at a time: Effect of distraction on performance of a simple laparoscopic and cognitive task by experienced and novice surgeons. Surg. Endosc. 2008, 22, 196–201. [Google Scholar] [CrossRef]
- Suh, I.H.; Chien, J.-H.; Mukherjee, M.; Park, S.-H.; Oleynikov, D.; Siu, K.-C. The negative effect of distraction on performance of robot-assisted surgical skills in medical students and residents. Int. J. Med. Robot. Comput. Assist. Surg. 2010, 6, 377–381. [Google Scholar] [CrossRef]
- Katz, J.D. Noise in the Operating Room. Anesthesiology 2014, 121, 894–898. [Google Scholar] [CrossRef]
- Cvach, M. Monitor alarm fatigue: An integrative review. Biomed. Instrum. Technol. 2012, 46, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Özcan, E.; Gommers, D. Nine nurse-recommended design strategies to improve alarm management in the ICU: A qualitative study. ICU Manag. Pract. 2020, 2, 129–133. [Google Scholar]
- Drew, B.J.; Harris, P.; Zègre-Hemsey, J.K.; Mammone, T.; Schindler, D.; Salas-Boni, R.; Hu, X. Insights into the Problem of Alarm Fatigue with Physiologic Monitor Devices: A Comprehensive Observational Study of Consecutive Intensive Care Unit Patients. PLoS ONE 2014, 9, e110274. [Google Scholar] [CrossRef] [Green Version]
- Funk, M.; Clark, J.T.; Bauld, T.J.; Ott, J.C.; Coss, P. Attitudes and Practices Related to Clinical Alarms. Am. J. Crit. Care 2014, 23, e9–e18. [Google Scholar] [CrossRef]
- Imhoff, M.; Kuhls, S. Alarm Algorithms in Critical Care Monitoring. Anesth. Analg. 2006, 102, 1525–1537. [Google Scholar] [CrossRef]
- Edworthy, J. Medical audible alarms: A review. J. Am. Med. Inform. Assoc. 2013, 20, 584–589. [Google Scholar] [CrossRef] [Green Version]
- Borowski, M.; Görges, M.; Fried, R.; Such, O.; Wrede, C.; Imhoff, M. Medical device alarms. Biomed. Eng./Biomed. Tech. 2011, 56, 73–83. [Google Scholar] [CrossRef]
- McFarlane, D.C.; Doig, A.K.; Agutter, J.A.; Brewer, L.M.; Syroid, N.D.; Mittu, R. Faster clinical response to the onset of adverse events: A wearable metacognitive attention aid for nurse triage of clinical alarms. PLoS ONE 2018, 13, e0197157. [Google Scholar] [CrossRef] [Green Version]
- Pascale, M.T.; Sanderson, P.; Liu, D.; Mohamed, I.; Brecknell, B.; Loeb, R. The Impact of Head-Worn Displays on Strategic Alarm Management and Situation Awareness. Hum. Factors J. Hum. Factors Ergon. Soc. 2019, 61, 537–563. [Google Scholar] [CrossRef]
- Paterson, E.; Sanderson, P.; Paterson, N.; Loeb, R. Effectiveness of enhanced pulse oximetry sonifications for conveying oxygen saturation ranges: A laboratory comparison of five auditory displays. Br. J. Anaesth. 2017, 119, 1249. [Google Scholar] [CrossRef]
- Li, S.Y.; Tang, T.L.; Hickling, A.; Yau, S.; Brecknell, B.; Sanderson, P.M. Spearcons for patient monitoring: Laboratory investigation comparing earcons and spearcons. Hum. Factors 2017, 59, 765–781. [Google Scholar] [CrossRef]
- Edworthy, J.; Reid, S.; Peel, K.; Lock, S.; Williams, J.; Newbury, C.; Farrington, M. The impact of workload on the ability to localize audible alarms. Appl. Ergon. 2018, 72, 88–93. [Google Scholar] [CrossRef]
- Chion, M. Audio-Vision: Sound on Screen; Columbia University Press: New York, NY, USA, 1990. [Google Scholar]
- Gaver, W.W. The SonicFinder: An interface that uses auditory icons. Hum.–Comput. Interact. 1989, 4, 67–94. [Google Scholar] [CrossRef]
- Schaeffer, P. Traité Des Objets Musicaux; Éditions du Seuil: Paris, France, 1966. [Google Scholar]
- Truax, B. Handbook for Acoustic Ecology; Cambridge Street Publishing: Vancouver, BC, Canada, 1999. [Google Scholar]
- Hermes, D.J. Auditory Material Perception (Annual Progress Report No. 33); IPO: Eindhoven, The Netherlands, 1998. [Google Scholar]
- Klatzky, R.L.; Pai, D.K.; Krotkov, E.P. Perception of Material from Contact Sounds. Presence Teleoperators Virtual Environ. 2000, 9, 399–410. [Google Scholar] [CrossRef]
- Kunkler-Peck, A.J.; Turvey, M.T. Hearing shape. J. Exp. Psychol. Hum. Percept. Perform. 2000, 26, 279–294. [Google Scholar] [CrossRef]
- Lutfi, R.A. Auditory detection of hollowness. J. Acoust. Soc. Am. 2001, 10, 1010–1019. [Google Scholar] [CrossRef] [Green Version]
- Aljishi, S.T. Why does heating water in a kettle produce sound? Am. J. Phys. 1991, 59, 628–632. [Google Scholar] [CrossRef]
- Cabe, P.; Pittenger, J.B. Human sensitivity to acoustic information from vessel filling. J. Exp. Psychol. Hum. Percept. Perform. 2000, 26, 313–324. [Google Scholar] [CrossRef]
- Li, X.; Logan, R.J.; Pastore, R.E. Perception of acoustic source characteristics: Walking sounds. J. Acoust. Soc. Am. 1991, 90, 3036–3049. [Google Scholar] [CrossRef]
- Björk, E.A. The Perceived quality of natural sounds. Acustica 1985, 57, 185–188. [Google Scholar]
- Edworthy, J.; Hellier, E.; Hards, R. The semantic associations of acoustic parameters commonly used in the design of auditory information and warming signals. Ergonomics 1995, 38, 2341–2361. [Google Scholar] [CrossRef]
- Kendall, R.A.; Carterette, E.C. Verbal attributes of simultaneous wind instrument timbres: I. von Bismarck’s adjectives. Music Percept. 1993, 10, 445–468. [Google Scholar] [CrossRef]
- Solomon, L.N. Semantic approach to the perception of complex sounds. J. Acoust. Soc. Am. 1958, 30, 421–425. [Google Scholar] [CrossRef]
- Gygi, B.; Kidd, G.R.; Watson, C.S. Spectral-temporal factors in the identification of environmental sounds. J. Acoust. Soc. Am. 2004, 115, 1252–1265. [Google Scholar] [CrossRef]
- Coward, S.W.; Stevens, C.J. Extracting meaning from sound: Nomic mappings, everyday listening, and perceiving object size from frequency. Psychol. Rec. 2004, 54, 349–364. [Google Scholar] [CrossRef] [Green Version]
- Gaver, W.W. What in the world do we hear?: An ecological approach to auditory event perception. Ecol. Psychol. 1993, 5, 1–29. [Google Scholar] [CrossRef]
- Gaver, W.W. How do we hear in the world? Explorations in ecological acoustics. Ecol. Psychol. 1993, 5, 285–313. [Google Scholar] [CrossRef]
- Van Dyck, E.; Moens, B.; Buhmann, J.; Demey, M.; Coorevits, E.; Bella, S.D.; Leman, M. Spontaneous entrainment of running cadence to music tempo. Sports Med.-Open 2015, 1, 15. [Google Scholar] [CrossRef] [Green Version]
- Tajadura-Jiménez, A.; Basia, M.; Deroy, O.; Fairhurst, M.; Marquardt, N.; Bianchi-Berthouze, N. As light as your footsteps: Altering walking sounds to change perceived body weight, emotional state and gait. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Republic of Korea, 18–23 April 2015; pp. 2943–2952. [Google Scholar]
- Özcan, E.; Frankel, L.; Stewart, J. Uncommon music making: The functional roles of music in design for healthcare. Music Med. 2019, 11, 245–255. [Google Scholar] [CrossRef]
- Özcan, E. The Harley effect: Internal and external factors facilitating positive experiences with product sounds. J. Sonic Stud. 2014, 6, a07. [Google Scholar]
- Özcan, E.; Van Egmond, R. Memory for Product Sounds: The Effect of Sound and Label Type. Acta Psychol. 2007, 126, 196–215. [Google Scholar] [CrossRef] [PubMed]
- Özcan, E.; Van Egmond, R. The Effect of Visual Context on the Identification of Ambiguous Environmental Sounds. Acta Psychol. 2009, 131, 110–119. [Google Scholar] [CrossRef]
- Özcan, E.; Van Egmond, R. Basic Semantics of Product Sounds. Int. J. Des. 2012, 6, 41–54. [Google Scholar]
- Özcan, E.; Van Egmond, R.; Jacobs, J. Product Sounds: Basic Concepts and Categories. Int. J. Des. 2014, 8, 97–111. [Google Scholar]
- Dubois, D.; Guastavino, C.; Raimbault, M. A cognitive approach to soundscape: Using verbal data to access everyday life auditory categories. Acta Acust. United Acust. 2006, 92, 865–874. [Google Scholar]
- Fabiani, M.; Kazmerski, V.A.; Cycowicz, Y.M.; Friedman, D. Naming norms for brief environmental sounds: Effects of age and dementia. Psychophysiology 1996, 33, 462–475. [Google Scholar] [CrossRef]
- Marcell, M.E.; Borella, D.; Greene, M.; Kerr, E.; Rogers, S. Confrontation naming of environmental sounds. J. Clin. Exp. Neuropsychol. 2000, 22, 830–864. [Google Scholar] [CrossRef] [Green Version]
- Lageat, T.; Czellar, S.; Laurent, G. Engineering hedonic attributes to generate perceptions of luxury: Consumer perception of an everyday sound. Mark. Lett. 2003, 14, 97–109. [Google Scholar] [CrossRef]
- Spence, C.; Zampini, M. Auditory contributions to multisensory product perception. Acta Acust. 2006, 92, 1009–1025. [Google Scholar]
- Susini, P.; McAdams, S.; Winsberg, S.; Perry, I.; Viellard, S.; Rodet, X. Characterizing the sound quality of air-conditioning noise. Appl. Acoust. 2004, 65, 763–790. [Google Scholar] [CrossRef]
- Aletta, F.; Kang, J. Soundscape approach integrating noise mapping techniques: A case study in Brighton, UK. Noise Mapp. 2015, 2, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Brooks, B.M.; Schulte-Fortkamp, B.; Voigt, K.S.; Case, A.U. Exploring our sonic environment through soundscape research & theory. Acoust. Today 2014, 10, 30–40. [Google Scholar]
- Schulte-Fortkamp, B.; Dubois, D. “Recent advances Soundscape research, special issue”. Acta Acust. United Acust. 2016, 92, v–viii. [Google Scholar]
- Van Kamp, I.; Klaeboe, R.; Kruize, H.; Brown, A.L.; Lercher, P. August. Soundscapes, human restoration and quality of life. In INTER-NOISE and NOISE-CON Congress and Conference Proceedings; Institute of Noise Control Engineering: Reston, VA, USA, 2016; Volume 253, pp. 1205–1215. [Google Scholar]
- Schulte-Fortkamp, B.; Fiebig, A. Soundscape analysis in a residential area: An evaluation of noise and people’s mind. Acta Acust. United Acust. 2006, 92, 875–880. [Google Scholar]
- Schokkin, M.; Van Boeijen, A.; Özcan, E. Sound Cultures of Critical Care. How Design Could Tune Sound-Related Practices of Intensive Care Nurses. Master’s Thesis, Critical Alarms Lab, Delft University of Technology, Delft, The Netherlands, 2019. [Google Scholar]
- Kang, J.; Aletta, F. The impact and outreach of soundscape research. Environments 2018, 5, 58. [Google Scholar] [CrossRef] [Green Version]
- Axelsson, Ö.; Nilsson, M.E.; Berglund, B. A principal components model of soundscape perception. J. Acoust. Soc. Am. 2010, 128, 2836–2846. [Google Scholar] [CrossRef]
- Torresin, S.; Albatici, R.; Aletta, F.; Babich, F.; Oberman, T.; Siboni, S.; Kang, J. Indoor soundscape assessment: A principal components model of acoustic perception in residential buildings. Build. Environ. 2020, 182, 107152. [Google Scholar] [CrossRef]
- Aletta, F.; Kang, J.; Axelsson, Ö. Soundscape descriptors and a conceptual framework for developing predictive soundscape models. Landsc. Urban Plan. 2016, 149, 65–74. [Google Scholar] [CrossRef]
- ISO 12913-1:2014; Acoustics—Soundscape—Part 1: Definition and Conceptual Framework. ISO: Geneva, Switzerland, 2014.
- Deb, S.; Claudio, D. Alarm fatigue and its influence on staff performance. IIE Trans. Healthc. Syst. Eng. 2015, 5, 183–196. [Google Scholar] [CrossRef]
- Claudio, D.; Deb, S.; Diegel, E. A Framework to Assess Alarm Fatigue Indicators in Critical Care Staff. Crit. Care Explor. 2021, 3, e0464. [Google Scholar] [CrossRef] [PubMed]
- Giv, M.D.; Sani, K.G.; Alizadeh, M.; Valinejadi, A.; Majdabadi, H.A. Evaluation of noise pollution level in the operating rooms of hospitals: A study in Iran. Interv. Med. Appl. Sci. 2017, 9, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Le, T.N.; Straatman, L.V.; Lea, J.; Westerberg, B. Current insights in noise-induced hearing loss: A literature review of the underlying mechanism, pathop- hysiology, asymmetry, and management options. J. Otolaryngol.-Head Neck Surg. 2017, 46, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nave, R. Hyper Physics: Sound and Hearing; Georgia State University, Department of Physics and Astronomy: Atlanta, GA, USA, 2005; Available online: http://hyperphysics.phyastr.gsu.edu/hbase/Sound/soucon.html#soucon (accessed on 14 November 2019).
- Schlesinger, J.J.; Miller, S.H.B.; Nash, K.; Bruce, M.; Ashmead, D.; Shotwell, M.S.; Weinger, M.B. Acoustic features of auditory medical alarms—An experimental study of alarm volume. J. Acoust. Soc. Am. 2018, 143, 3688–3697. [Google Scholar] [CrossRef]
- Bolton, M.L.; Edworthy, J.; Boyd, A.D. A Formal Analysis of Masking Between Reserved Alarm Sounds of the IEC 60601-1-8 International Medical Alarm Standard. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2018, 62, 523–527. [Google Scholar] [CrossRef]
- Hasanain, B.; Boyd, A.D.; Edworthy, J.; Bolton, M.L. A formal approach to discovering simultaneous additive masking between auditory medical alarms. Appl. Ergon. 2017, 58, 500–514. [Google Scholar] [CrossRef] [Green Version]
- Fox, N.J. Space, sterility and surgery: Circuits of hygiene in the operating theatre. Soc. Sci. Med. 1997, 45, 649–657. [Google Scholar] [CrossRef]
- Bott, O.J.; Dresing, K.; Wagner, M.; Raab, B.-W.; Teistler, M. Informatics in radiology use of a C-arm fluoroscopy simulator to support training in intraoperative radiography. Radiographics 2011, 31, E65–E75. [Google Scholar] [CrossRef]
- Gloag, D. Noise and health: Public and private responsibility. BMJ 1980, 281, 1404–1406. [Google Scholar] [CrossRef] [Green Version]
- Miskovic, D.; Rosenthal, R.; Zingg, U.; Oertli, D.; Metzger, U.; Jancke, L. Randomized controlled trial investigating the effect of music on the virtual reality laparoscopic learning performance of novice surgeons. Surg. Endosc. 2008, 22, 2416–2420. [Google Scholar] [CrossRef]













| dB(C)-LCpk | 21.10/2 | 21.10/5 | 01.11/3 | 01.11/2 | 14.11/1 | 14.11/2 | Range | Average (log) | Set Average |
|---|---|---|---|---|---|---|---|---|---|
| Incision | 82.6 | 85.5 | 87.2 | 92.1 | 89 | 84 | 82–92 | 87.9 | 88 |
| Saw (osc) | 100.2 | 101.4 | 106.1 | 105.6 | 95.7 | 95 | 95–106 | 102.5 | 102.5 |
| Clean-up/suction | 93.4 | 88.2 | 90.6 | 86.8 | 94.9 | 95.1 | 86–95 | 92.6 | 92 |
| Reamer (elec) | 91.7 | 94.7 | 88.5 | 95.2 | 90.2 | 91.9 | 88–95 | 92.7 | 93 |
| Pelvis cup tit | 123.4 | 124 | 123.6 | 124.7 | 124.2 | 124 | 123–125 | 124 | 124 |
| Pelvis cup | 119.3 | 123.6 | 117.4 | 119 | 121.7 | 114.8 | 114–124 | 120.2 | 120 |
| Rasp. femur | 121.5 | 119 | 125.1 | 124.9 | 122.1 | 121.3 | 119–125 | 122.8 | 123 |
| Femur stem | 116.2 | 114 | 122.7 | 120.6 | 116.6 | 118.4 | 114–121 | 119.1 | 119 |
| Ball fix | 97.2 | 95.2 | 92.1 | 98.5 | 114.5 | 108.4 | 92–115 | 107.9 | 108 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Özcan, E.; Broekmeulen, C.L.H.; Luck, Z.A.; van Velzen, M.; Stappers, P.J.; Edworthy, J.R. Acoustic Biotopes, Listeners and Sound-Induced Action: A Case Study of Operating Rooms. Int. J. Environ. Res. Public Health 2022, 19, 16674. https://doi.org/10.3390/ijerph192416674
Özcan E, Broekmeulen CLH, Luck ZA, van Velzen M, Stappers PJ, Edworthy JR. Acoustic Biotopes, Listeners and Sound-Induced Action: A Case Study of Operating Rooms. International Journal of Environmental Research and Public Health. 2022; 19(24):16674. https://doi.org/10.3390/ijerph192416674
Chicago/Turabian StyleÖzcan, Elif, Cornelis L. H. Broekmeulen, Zoe Alexandra Luck, Monique van Velzen, Pieter Jan Stappers, and Judy Reed Edworthy. 2022. "Acoustic Biotopes, Listeners and Sound-Induced Action: A Case Study of Operating Rooms" International Journal of Environmental Research and Public Health 19, no. 24: 16674. https://doi.org/10.3390/ijerph192416674