
Competence Development and Collaborative Climate as Antecedents of Job Performance, Job Commitment and Uncertainty: Validation of a Theoretical Model across Four Hospitals

Abstract
:1. Introduction
2. Theoretical Background and Hypothesis Development
2.1. Uncertainty in Patient Treatment and Its Determinants
2.2. Collaborative Climate as an Aspect of Organizational Climate
2.3. The Importance of Competence Development and Its Relation to Collaborative Climate
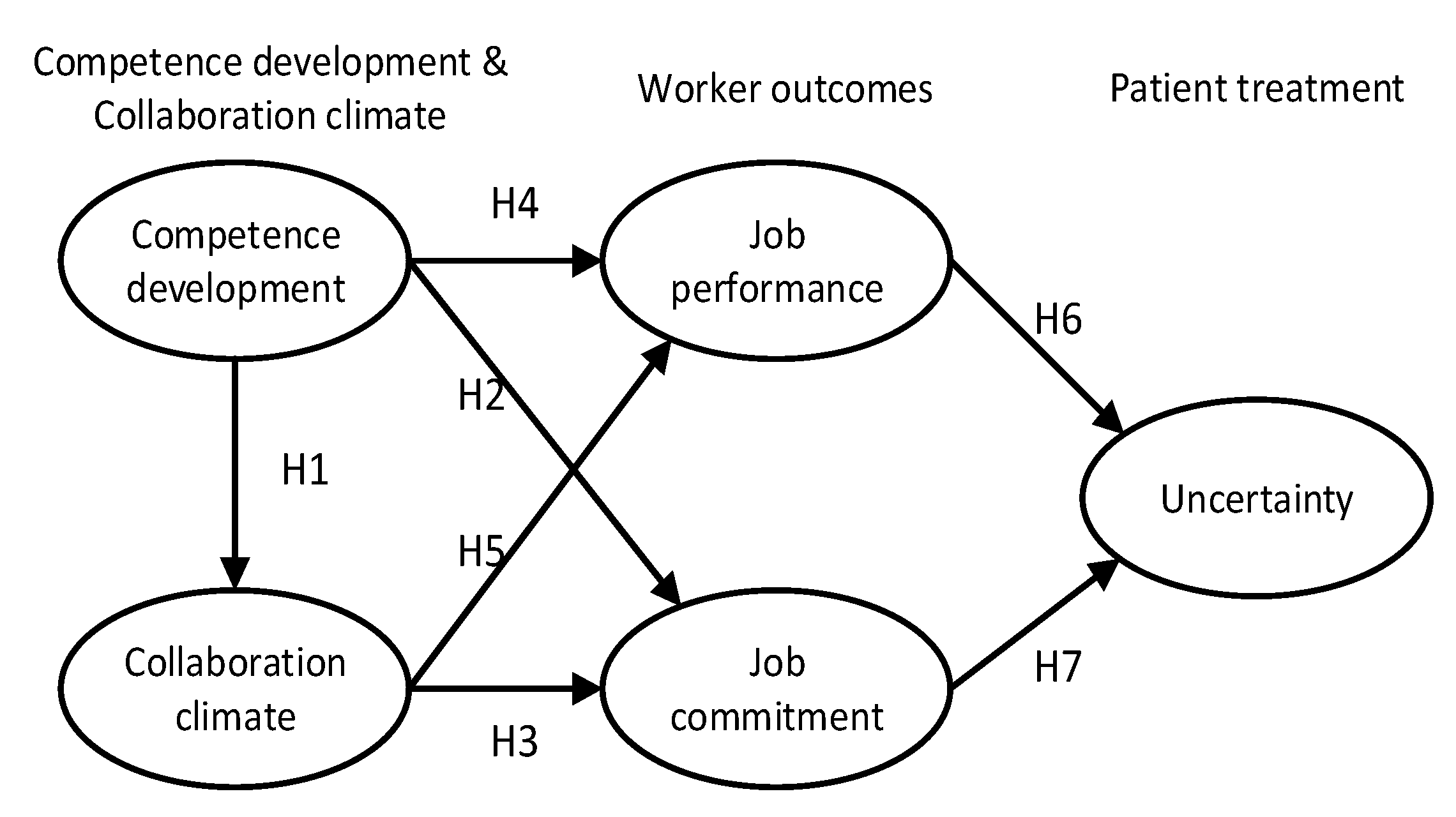
2.4. Competence Development and Collaboration Climate as Antecedents of Job Performance and Job Commitment and the Implications for Uncertainty
3. Materials and Methods
3.1. Sample and data Collection
3.2. Measures
3.3. Data Analysis
4. Results
4.1. Descriptive Statistics, Correlations and Internal Consistency
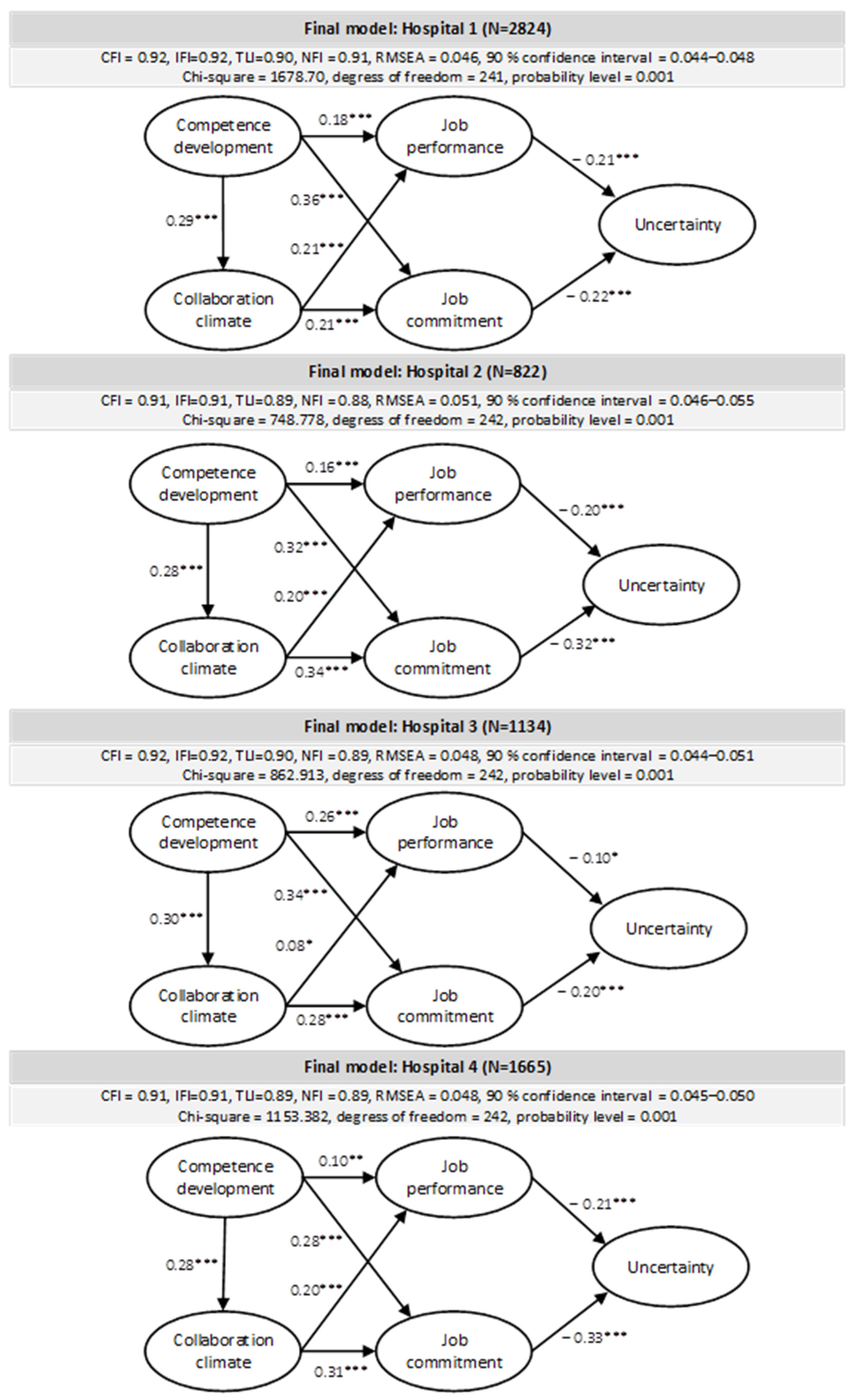
4.2. Confirmatory Factor Analysis and Structural Relationships
5. Discussion
Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fox, R.C. The evolution of medical uncertainty. Milbank Meml. Fund Q. Health Soc. 1980, 58, 1–49. [Google Scholar] [CrossRef]
- Han, P.K.; Klein, W.M.; Arora, N.K. Varieties of uncertainty in health care: A conceptual taxonomy. Med. Decis. Mak. 2011, 31, 828–838. [Google Scholar] [CrossRef]
- Han, P.K.; Babrow, A.; Hillen, M.A.; Gulbrandsen, P.; Smets, E.M.; Ofstad, E.H. Uncertainty in health care: Towards a more systematic program of research. Patient Educ. Couns. 2019, 102, 1756–1766. [Google Scholar] [CrossRef] [PubMed]
- Galbraith, J. Designing complex organizations. In Reading Mass; Addisson-Weslay: Boston, MA, USA, 1973. [Google Scholar]
- Olsen, E.; Mikkelsen, A. Development and Investigation of a New Model Explaining Job Performance and Uncertainty among Nurses and Physicians. Int. J. Environ. Res. Public Health 2021, 18, 164. [Google Scholar] [CrossRef] [PubMed]
- Boxall, P.; Purcell, J. Strategy and Human Resource Management; Bloomsbury Publishing: New York, NY, USA, 2022. [Google Scholar]
- Huselid, M.A.; Becker, B.E. Bridging Micro and Macro Domains: Workforce Differentiation and Strategic Human Resource Management; Sage Publications Sage CA: Los Angeles, CA, USA, 2011; Volume 37, pp. 421–428. [Google Scholar]
- Boon, C.; Kalshoven, K. How high-commitment HRM relates to engagement and commitment: The moderating role of task proficiency. Hum. Resour. Manag. 2014, 53, 403–420. [Google Scholar] [CrossRef]
- Raineri, A. Linking human resources practices with performance: The simultaneous mediation of collective affective commitment and human capital. Int. J. Hum. Resour. Manag. 2017, 28, 3149–3178. [Google Scholar] [CrossRef]
- Blau, P. Exchange and Power in Social Life; John Wiley: New York, NY, USA, 1964. [Google Scholar]
- Gouldner, A.W. The norm of reciprocity: A preliminary statement. Am. Sociol. Rev. 1960, 25, 161–178. [Google Scholar] [CrossRef]
- Appelbaum, E.; Bailey, T.; Berg, P.; Kalleberg, A.L. Manufacturing Advantage: Why High-Performance Work Systems Pay off; Cornell University Press: Ithaca, NY, USA, 2000. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68. [Google Scholar] [CrossRef]
- Mostafa, A.M.S. High-performance HR practices, positive affect and employee outcomes. J. Manag. Psychol. 2017, 32, 163–176. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, R.D.; Karasick, B.W. The effects of organizational climate on managerial job performance and job satisfaction. Organ. Behav. Hum. Perform. 1973, 9, 126–146. [Google Scholar] [CrossRef]
- Bowen, D.E.; Ostroff, C. Understanding HRM–firm performance linkages: The role of the “strength” of the HRM system. Acad. Manag. Rev. 2004, 29, 203–221. [Google Scholar]
- Dastmalchian, A. Environmental characteristics and organizational climate: An exploratory study. J. Manag. Stud. 1986, 23, 609–633. [Google Scholar] [CrossRef]
- Schneider, B.; Ehrhart, M.G.; Macey, W.H. Organizational climate and culture. Annu. Rev. Psychol. 2013, 64, 361–388. [Google Scholar] [CrossRef] [Green Version]
- Olsen, E.; Bjaalid, G.; Mikkelsen, A. Work climate and the mediating role of workplace bullying related to job performance, job satisfaction, and work ability: A study among hospital nurses. J. Adv. Nurs. 2017, 73, 2709–2719. [Google Scholar] [CrossRef]
- Hong, Y.; Liao, H.; Hu, J.; Jiang, K. Missing link in the service profit chain: A meta-analytic review of the antecedents, consequences, and moderators of service climate. J. Appl. Psychol. 2013, 98, 237. [Google Scholar] [CrossRef]
- Addo, S.A.; Mykletun, R.J.; Olsen, E. Validation and Adjustment of the Patient Experience Questionnaire (PEQ): A Regional Hospital Study in Norway. Int. J. Environ. Res. Public Health 2021, 18, 7141. [Google Scholar] [CrossRef]
- Zohar, D.; Polachek, T. Discourse-based intervention for modifying supervisory communication as leverage for safety climate and performance improvement: A randomized field study. J. Appl. Psychol. 2014, 99, 113. [Google Scholar] [CrossRef]
- Olsen, E.; Leonardsen, A.-C.L. Use of the Hospital Survey of Patient Safety Culture in Norwegian Hospitals: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6518. [Google Scholar] [CrossRef]
- Olsen, E. Exploring the possibility of a common structural model measuring associations between safety climate factors and safety behaviour in health care and the petroleum sectors. Accid. Anal. Prev. 2010, 42, 1507–1516. [Google Scholar] [CrossRef]
- Olsen, E.; Aase, K. A comparative study of safety climate differences in healthcare and the petroleum industry. Qual. Saf. Health Care 2010, 19, i75–i79. [Google Scholar] [CrossRef]
- Olsen, E. Safety Climate and Safety Culture in Health Care and the Petroleum Industry: Psychometric Quality, Longitudinal Change, and Structural Models. Ph.D. Thesis, University of Stavanger, Stavanger, Norway, 2009. [Google Scholar]
- Tharaldsen, J.E.; Olsen, E.; Rundmo, T. A longitudinal study of safety climate on the Norwegian Sontinental Shelf. Saf. Sci. 2007, 46, 427–439. [Google Scholar] [CrossRef]
- Sveiby, K.E.; Simons, R. Collaborative climate and effectiveness of knowledge work—An empirical study. J. Knowl. Manag. 2002, 6, 420–433. [Google Scholar] [CrossRef] [Green Version]
- House, R.J. Path-goal theory of leadership: Lessons, legacy, and a reformulated theory. Leadersh. Q. 1996, 7, 323–352. [Google Scholar] [CrossRef]
- Huxham, C.; Vangen, S. Leadership in the shaping and implementation of collaboration agendas: How things happen in a (not quite) joined-up world. Acad. Manag. J. 2000, 43, 1159–1175. [Google Scholar] [CrossRef]
- Tsasis, P.; Evans, J.M.; Rush, L.; Diamond, J. Learning to learn: Towards a relational and transformational model of learning for improved integrated care delivery. Adm. Sci. 2013, 3, 9–31. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The” what” and” why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Baard, P.P.; Deci, E.L.; Ryan, R.M. Intrinsic need satisfaction: A motivational basis of performance and weil-being in two work settings. J. Appl. Soc. Psychol. 2004, 34, 2045–2068. [Google Scholar] [CrossRef]
- Sisson, K.; Storey, J. Realities of Human Resource Management: Managing the Employment Relationship; Open University Press: Birmingham, UK, 2000. [Google Scholar]
- Fredrickson, B.L.; Losada, M.F. Positive affect and the complex dynamics of human flourishing. Am. Psychol. 2005, 60, 678. [Google Scholar] [CrossRef] [Green Version]
- Mowday, R.T.; Porter, L.W.; Steers, R.M. Employee—Organization Linkages: The psychology of Commitment, Absenteeism, and Turnover; Academic Press: New York, NY, USA, 2013. [Google Scholar]
- Wright, T.A.; Hobfoll, S.E. Commitment, psychological well-being and job performance: An examination of conservation of resources (COR) theory and job burnout. J. Bus. Manag. 2004, 9, 389–406. [Google Scholar]
- Meyer, J.P. Employee commitment, motivation, and engagement: Exploring the links. The Oxford Handbook of Work Engagement, Motivation, and Self-Determination Theory; Oxford University Press: Oxford, UK, 2014; pp. 33–49. [Google Scholar]
- Barsade, S.G.; Gibson, D.E. Why does affect matter in organizations? Acad. Manag. Perspect. 2007, 21, 36–59. [Google Scholar] [CrossRef]
- Chen, C.-J.; Huang, J.-W. How organizational climate and structure affect knowledge management—The social interaction perspective. Int. J. Inf. Manag. 2007, 27, 104–118. [Google Scholar] [CrossRef]
- Bock, G.-W.; Zmud, R.W.; Kim, Y.-G.; Lee, J.-N. Behavioral intention formation in knowledge sharing: Examining the roles of extrinsic motivators, social-psychological forces, and organizational climate. MIS Q. 2005, 29, 87–111. [Google Scholar] [CrossRef]
- Luthans, F.; Norman, S.M.; Avolio, B.J.; Avey, J.B. The mediating role of psychological capital in the supportive organizational climate—Employee performance relationship. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2008, 29, 219–238. [Google Scholar] [CrossRef] [Green Version]
- Grant, A.M.; Berry, J.W. The necessity of others is the mother of invention: Intrinsic and prosocial motivations, perspective taking, and creativity. Acad. Manag. J. 2011, 54, 73–96. [Google Scholar] [CrossRef] [Green Version]
- Grant, A.M. Giving time, time after time: Work design and sustained employee participation in corporate volunteering. Acad. Manag. Rev. 2012, 37, 589–615. [Google Scholar] [CrossRef] [Green Version]
- Janz, B.D.; Prasarnphanich, P. Understanding the antecedents of effective knowledge management: The importance of a knowledge-centered culture. Decis. Sci. 2003, 34, 351–384. [Google Scholar] [CrossRef]
- Slåtten, T.; Lien, G. Frontline nurses’ appraisal of organizational attractiveness and the role of management support, interdepartmental collaboration climate and service quality of care. Int. J. Qual. Serv. Sci. 2021, 1–20. [Google Scholar] [CrossRef]
- Cummings, G.G.; MacGregor, T.; Davey, M.; Lee, H.; Wong, C.A.; Lo, E.; Muise, M.; Stafford, E. Leadership styles and outcome patterns for the nursing workforce and work environment: A systematic review. Int. J. Nurs. Stud. 2010, 47, 363–385. [Google Scholar] [CrossRef]
- Millward, L.J.; Hopkins, L.J. Psychological contracts, organizational and job commitment. J. Appl. Soc. Psychol. 1998, 28, 1530–1556. [Google Scholar] [CrossRef]
- Motowidlo, S.J. Job performance. Handb. Psychol. Ind. Organ. Psychol. 2003, 12, 39–53. [Google Scholar]
- Kristensen, T. A new tool for assessing psychosocial work environment factors: The Copenhagen Psychosocial Questionnaire. Arb. Och Hälsa 2001, 10, 210–213. [Google Scholar]
- Rugulies, R.; Aust, B.; Pejtersen, J.H. Do psychosocial work environment factors measured with scales from the Copenhagen Psychosocial Questionnaire predict register-based sickness absence of 3 weeks or more in Denmark? Scand. J. Public Health 2010, 38, 42–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michela, J.L.; Lukaszewski, M.P.; Allegrante, J.P. Organizational climate and work stress: A general framework applied to inner-city schoolteachers. In Organizational Risk Factors for Job Stress; American Psychological Association: Washington, DC, USA, 1995. [Google Scholar]
- Allen, N.J.; Meyer, J.P. The measurement and antecedents of affective, continuance and normative commitment to the organization. J. Occup. Psychol. 1990, 63, 1–18. [Google Scholar] [CrossRef]
- Ørhede, E.; Hottinen, V.; Skogstad, A.; Knardahl, S.; Elo, A.-L.; Dallner, M.; Gamberale, F. User’s Guide for the QPSNordic: General Nordic Questionnaire for Psychological and Social Factors at Work; Nordic Council of Ministers: Copenhagen, Denmark, 2000; ISBN 9289305355. [Google Scholar]
- Sorra, J.; Gray, L.; Streagle, S.; Famolaro, T.; Yount, N.; Behm, J. AHRQ Hospital Survey on Patient Safety Culture: User’s Guide; Prepared by Westat, under contract no. HHSA290201300003C. AHRQ publication no. 15–0049-EF (Replaces 04–0041) (Vol. AHRQ Publication. No. 15 (16)-0049-EF. Replaces 04–0041); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2016. [Google Scholar]
- Arbuckle, J. Amos 21 User’s Guide; International Business Machines Corp: Boston, MA, USA, 2012. [Google Scholar]
- Jyoti, J. Impact of organizational climate on job satisfaction, job commitment and intention to leave: An empirical model. J. Bus. Theory Pract. 2013, 1, 66–82. [Google Scholar] [CrossRef]
- Lee, C.H.; Bruvold, N.T. Creating value for employees: Investment in employee development. Int. J. Hum. Resour. Manag. 2003, 14, 981–1000. [Google Scholar] [CrossRef]
- Drejer, A. Organisational learning and competence development. Learn. Organ. 2000, 7, 206–220. [Google Scholar] [CrossRef] [Green Version]
- Leonard, D. Wellsprings of Knowledge; Harvard Business School Press: Boston, MA, USA, 1995. [Google Scholar]
- Drejer, A.; Riis, J.O. Competence development and technology: How learning and technology can be meaningfully integrated. Technovation 1999, 19, 631–644. [Google Scholar] [CrossRef]
- Podsakoff, P.; MacKenzie, S.; Lee, K.e.a. Commom method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Pasban, M.; Nojedeh, S.H. A Review of the Role of Human Capital in the Organization. Procedia-Soc. Behav. Sci. 2016, 230, 249–253. [Google Scholar] [CrossRef] [Green Version]
- Hognestad Haaland, G.; Olsen, E.; Mikkelsen, A. The association between supervisor support and ethical dilemmas on Nurses’ intention to leave: The mediating role of the meaning of work. J. Nurs. Manag. 2021, 29, 286–293. [Google Scholar] [CrossRef]
- Bjaalid, G.; Olsen, E.; Melberg, K.; Mikkelsen, A. Institutional stress and job performance among hospital employees. Int. J. Organ. Anal. 2019, 28, 365–382. [Google Scholar] [CrossRef]
- Haver, A.; Olsen, E.; Akerjordet, K. Well-being among hotel managers: A study on the influence of job stressors and cognitive reappraisal. Int. J. Contemp. Hosp. Manag. 2019, 31, 1819–1835. [Google Scholar] [CrossRef]
- Olsen, E. Reliability and validity of the Hospital Survey on Patient Safety Culture at a Norwegian hospital. In Quality and Safety Improvement Research: Methods and Research Practice from the International Quality Improvement Research Network (QIRN); National School of Public Health: Lisboa, Portugal, 2008; pp. 173–186. [Google Scholar]
- Dahl, Ø.; Olsen, E. Safety compliance on offshore platforms: A multi-sample survey on the role of perceived leadership involvement and work climate. Saf. Sci. 2013, 54, 17–26. [Google Scholar] [CrossRef]
- Dahl, Ø.; Rundmo, T.; Olsen, E. The Impact of Business Leaders’ Formal Health and Safety Training on the Establishment of Robust Occupational Safety and Health Management Systems: Three Studies Based on Data from Labour Inspections. Int. J. Environ. Res. Public Health 2022, 19, 1269. [Google Scholar] [CrossRef]
- Bollestad, V.; Amland, J.-S.; Olsen, E. The pros and cons of remote work in relation to bullying, loneliness and work engagement: A representative study among Norwegian workers during COVID-19. Front. Psychol. 2022, 13, 6717. [Google Scholar] [CrossRef]
- Olsen, E.; Jensen, M.T.; Bjaalid, G.; Mikkelsen, A. Job resources and outcomes in the process of bullying: A study in a Norwegian healthcare setting. In Increasing Occupational Health and Safety in Workplaces; Edward Elgar Publishing: Northampton, MA, USA, 2019. [Google Scholar]
- Shamsi, M.; Iakovleva, T.; Olsen, E.; Bagozzi, R.P. Employees’ Work-Related Well-Being during COVID-19 Pandemic: An Integrated Perspective of Technology Acceptance Model and JD-R Theory. Int. J. Environ. Res. Public Health 2021, 18, 11888. [Google Scholar] [CrossRef]
- Øygarden, O.; Olsen, E.; Mikkelsen, A. Changing to improve? Organizational change and change-oriented leadership in hospitals. J. Health Organ. Manag. 2020, 34, 687–706. [Google Scholar] [CrossRef]
- Mikkelsen, A.; Olsen, E. The influence of change-oriented leadership on work performance and job satisfaction in hospitals–the mediating roles of learning demands and job involvement. Leadersh. Health Serv. 2019, 32, 37–53. [Google Scholar] [CrossRef]
- Olsen, E.; Aase, K. The challenge of improving safety culture in hospitals: A longitudinal study using hospital survey on patient safety culture. In Proceedings of the 11th International Probabilistic Safety Assessment and Management Conference and the Annual European Safety and Reliability Conference 2012, Helsinki, Finland, 25–29 June 2012; Curran Associates, Inc: New York, NY, USA, 2012; pp. 5929–5936. [Google Scholar]
- Olsen, E.; Bjerkan, A.M.; Nævestad, T.O. Modelling the effects of a large-scale safety culture programme: A combined qualitative and quantitative approach. J. Risk Res. 2010, 12, 389–409. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Hospital 1 | Hospital 2 | Hospital 3 | Hospital 4 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Gender | 1.18 | 0.39 | 1.19 | 0.4 | 1.15 | 0.36 | 1.14 | 0.35 | 1.17 | 0.38 |
| Number of working hours | 33.95 | 9.09 | 33.79 | 10.70 | 32.45 | 8.93 | 33.11 | 9.74 | 33.47 | 9.45 |
| Competence development | 4.37 | 0.58 | 4.36 | 0.60 | 4.35 | 0.59 | 4.37 | 0.60 | 4.36 | 0.59 |
| Collaborative climate | 3.47 | 0.70 | 3.35 | 0.73 | 3.42 | 0.70 | 3.45 | 0.70 | 3.44 | 0.71 |
| Job performance | 4.11 | 0.48 | 4.07 | 0.50 | 4.05 | 0.48 | 4.10 | 0.46 | 4.09 | 0.48 |
| Job commitment | 3.89 | 0.91 | 3.84 | 0.95 | 3.78 | 0.97 | 3.83 | 0.92 | 3.85 | 0.93 |
| Uncertainty | 1.79 | 0.43 | 1.81 | 0.43 | 1.84 | 0.42 | 1.87 | 0.44 | 1.82 | 0.43 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. Gender | - | ||||||
| 2. Number of working hours | 0.05 ** | - | |||||
| 3. Competence development | –0.06 ** | –0.02 | (0.77) | ||||
| 4. Collaborative climate | 0.05 ** | 0.01 | 0.30 ** | (0.74) | |||
| 5. Job performance | 0.00 | –0.01 | 0.17 ** | 0.26 ** | (0.78) | ||
| 6. Job commitment | –0.03 * | 0.00 | 0.33 ** | 0.24 ** | 0.27 ** | (0.89) | |
| 7. Uncertainty | 0.03 * | 0.06 ** | –0.09 ** | –0.08 ** | –0.15 ** | –0.20 ** | (0.89) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jensen, M.T.; Øygarden, O.; Mikkelsen, A.; Olsen, E. Competence Development and Collaborative Climate as Antecedents of Job Performance, Job Commitment and Uncertainty: Validation of a Theoretical Model across Four Hospitals. Int. J. Environ. Res. Public Health 2023, 20, 425. https://doi.org/10.3390/ijerph20010425
Jensen MT, Øygarden O, Mikkelsen A, Olsen E. Competence Development and Collaborative Climate as Antecedents of Job Performance, Job Commitment and Uncertainty: Validation of a Theoretical Model across Four Hospitals. International Journal of Environmental Research and Public Health. 2023; 20(1):425. https://doi.org/10.3390/ijerph20010425
Chicago/Turabian StyleJensen, Maria Therese, Olaug Øygarden, Aslaug Mikkelsen, and Espen Olsen. 2023. "Competence Development and Collaborative Climate as Antecedents of Job Performance, Job Commitment and Uncertainty: Validation of a Theoretical Model across Four Hospitals" International Journal of Environmental Research and Public Health 20, no. 1: 425. https://doi.org/10.3390/ijerph20010425