1. Introduction
Caries in primary teeth are one of the most common health conditions among children globally and locally across a majority of world regions [
1]. Among the different types of caries in primary teeth, early childhood caries (ECC) and severe early childhood caries (S-ECC) have more profound societal impacts and pose a substantial public health concern [
2]. The global prevalence of ECC ranges from 16% to 89% [
3], in which S-ECC accounts for a large proportion [
4,
5]. Moreover, a high portion of the primary tooth caries were untreated dental caries [
4,
5]. Primary dental caries develop rapidly but can be easily neglected by parents, resulting in delayed or missed treatment. In the long term, untreated tooth decay may impact children’s systemic health, leading to conditions such as development deficits and psychological problems [
6]. The local effect of the untreated carious lesions include pulpal involvement, periapical lesions, abscess, and sinus tract [
7]. These constitute substantial direct and indirect costs to children, families, and society, and significantly impacts children’s quality of life.
Regarding lesions involving the pulp, partial pulpotomy, pulpectomy, and tooth extraction are all available options. The American Academy of Pediatric Dentistry (AAPD) states that when there is enough evidence, children should be subjected to nonvital pulp treatment [
8]. It is the only treatment to retain the teeth with irreversible pulpitis and periapical periodontitis. With the widespread application and ongoing research on primary tooth pulpectomy, some studies have shown that the treatment has a better prognosis, but definitive conclusions remain elusive. A negative attitude toward pulpectomy in primary teeth is mostly due to the potential risk of damage to the successor permanent tooth buds and difficulty in cleaning and shaping root canals [
9].
Meanwhile, there are various potential factors associated with the failure that cannot come into consistency [
8,
10,
11]. The success rate may vary depending on the etiology of lesions, preoperative pulp status, follow-up duration, filling materials, restorations, and clinicians. However, there is currently a lack of comprehensive and longitudinal evaluations of factors influencing the treatment outcome of pulpectomy in primary teeth.
Compared with other endodontic treatments in pediatric dentistry, pulpectomy is more complicated and requires a higher degree of cooperation. When performed under dental general anesthesia (DGA), pulpectomy of the primary tooth is a safe and effective procedure that avoids the interference of children’s uncooperative behaviors [
12]. Many studies have shown significant satisfaction and high acceptance of the treatment outcome of DGA [
13,
14].
Therefore, this study aims to retrospectively evaluate the survival rate of pulpectomy performed under DGA through long-term follow-up and to explore the risk factors associated with treatment failure while controlling for potential confounders such as children’s level of cooperation and contamination during the follow-up visit.
2. Materials and Methods
This study was approved by the Medical Ethics Committee of Xi’an Jiaotong University (xjkqll (2021) NO. 10).
2.1. Participants
The participants were children diagnosed with S-ECC without systemic illness who underwent DGA in the Department of Pediatric Dentistry, Stomatology Hospital of Xi’an Jiaotong University from 1 August 2014 to 31 December 2019. The participants’ medical records should be complete, and their follow-up period should last at least six months. Radiographs of the tooth under treatment before the operation or within two weeks after the treatment, together with at least one radiograph in the follow-up period, were needed.
The inclusion and exclusion criteria of the tooth are as follows.
Inclusion criteria:
- (1)
Diagnosed with irreversible pulpitis, pulp necrosis, or periapical periodontitis but reserved;
- (2)
Without internal resorption or radiolucency surrounding the tooth apex. For teeth with physiological or pathological root resorption, resorption should be limited to less than 1/3 of the root length.
Exclusion criteria:
- (1)
The crown is seriously damaged and cannot be restored;
- (2)
Root resorption involving more than 1/3 of the root length;
- (3)
Inflammation has affected the permanent teeth;
- (4)
Traumatic injury to the treated tooth during the observation period.
2.2. Pulpectomy Procedure
All operations were performed by dentists with at least an associate professorship and more than 15 years of experience and they were familiar with the practice process. All of the teeth were isolated by the rubber dam under the DGA. After removing all of the carious lesions, the pulp chamber was accessed by the high-speed handpiece. The pathological pulp was cleaned with barbed broaches. Root canal preparation was performed using manual (Mani #15 or #20 K files, MANI Inc. Tochigi, Japan) and a rotary (Protaper Universal, Dentsply Maillefer, Ballaigues, Switzerland) instrument. The canal enlargement was performed with ProTaper Universal instruments F1 and F2. The working length was determined by apex locators (ProPex Pixi, Dentsply Maillefer, Ballaigues, Switzerland) and practitioners’ experiences. The root canal was alternatively irrigated with 1.25% sodium hypochlorite and 2% chlorhexidine, and normal saline was used between the use of those two solutions. Sterilized paper point was used to dry the root canals, and the canals were obturated by the root canal filling paste. There are two kinds of filling pastes in clinical practice, zinc oxide eugenol paste (ZOE, Associated Dental Products Ltd., Purton, UK) and Vitapex (Neo Dental Chemical Products Co. Ltd., Tokyo, Japan). The decision on which type to use was made by the practitioners. The filling materials were sent into the root canal by lentuo spirals until there was obvious overflow at the root canal orifice. The choice of the restoration method depended on the size of the defective area and tooth position. The preformed metal crown (PMC, stainless steel crown, SSC) with GIC was routinely selected for molars. For anterior teeth, a strip crown with resin composite (Filtek Supreme Flowable Restorative, 3M ESPE, St. Paul, MN, USA) or direct resin composite (Filtek Z350 XT Universal Restorative, 3M ESPE, St. Paul, MN, USA) was used. The 2-step etch-and-rinse adhesive (Single bond, 3M ESPE) was adopted during the restoration.
2.3. DGA Treatment Requirement
All treatment procedures were followed and adjusted according to related guidelines and textbooks. All of the children who underwent DGA treatment were required to follow-up two weeks later the DGA treatment and subsequently every three to six months. No X-ray or clinical examination was conducted immediately after the operation. The patient was required to take a radiograph at the first follow-up visit. The other radiographs were taken every three to six months for teeth that underwent pulpectomy therapy. The radiographs were taken by the experienced technician and adopted by bisected angle technique.
Additionally, parents are advised to prepare non-prescription NSAIDS drugs. It can be taken for one to three days if fever occurs after DGA treatment. Oral health education was conducted for guardians and children at every follow-up visit, and fluoride application was carried out regularly every 3–6 months.
2.4. Criteria for the Outcome during the Follow-Up Examinations
The outcome was evaluated both clinically and radiographically.
Clinical criteria for success:
- (1)
No spontaneous pain or sensitivity to percussion;
- (2)
The surrounding soft tissues are healthy, or the sinus tract and abscess recovered;
- (3)
No abnormal mobility;
- (4)
Has physical function.
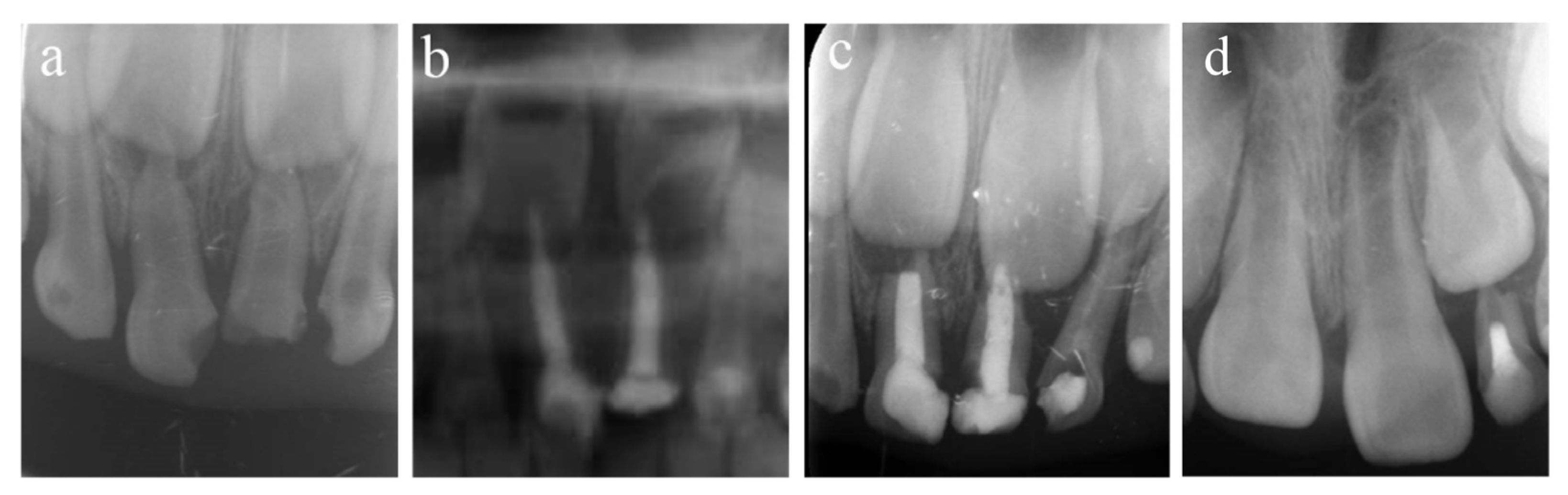
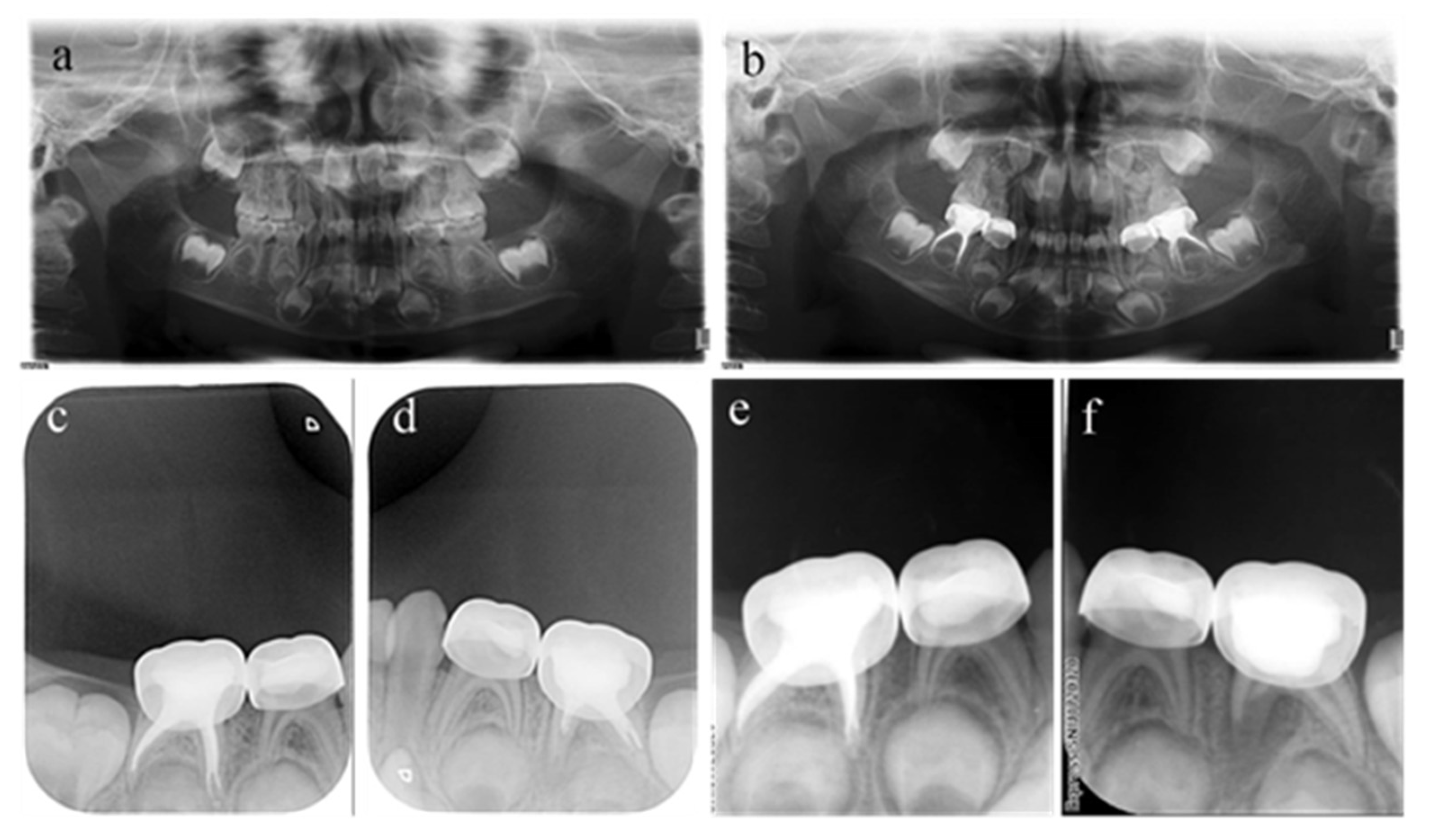
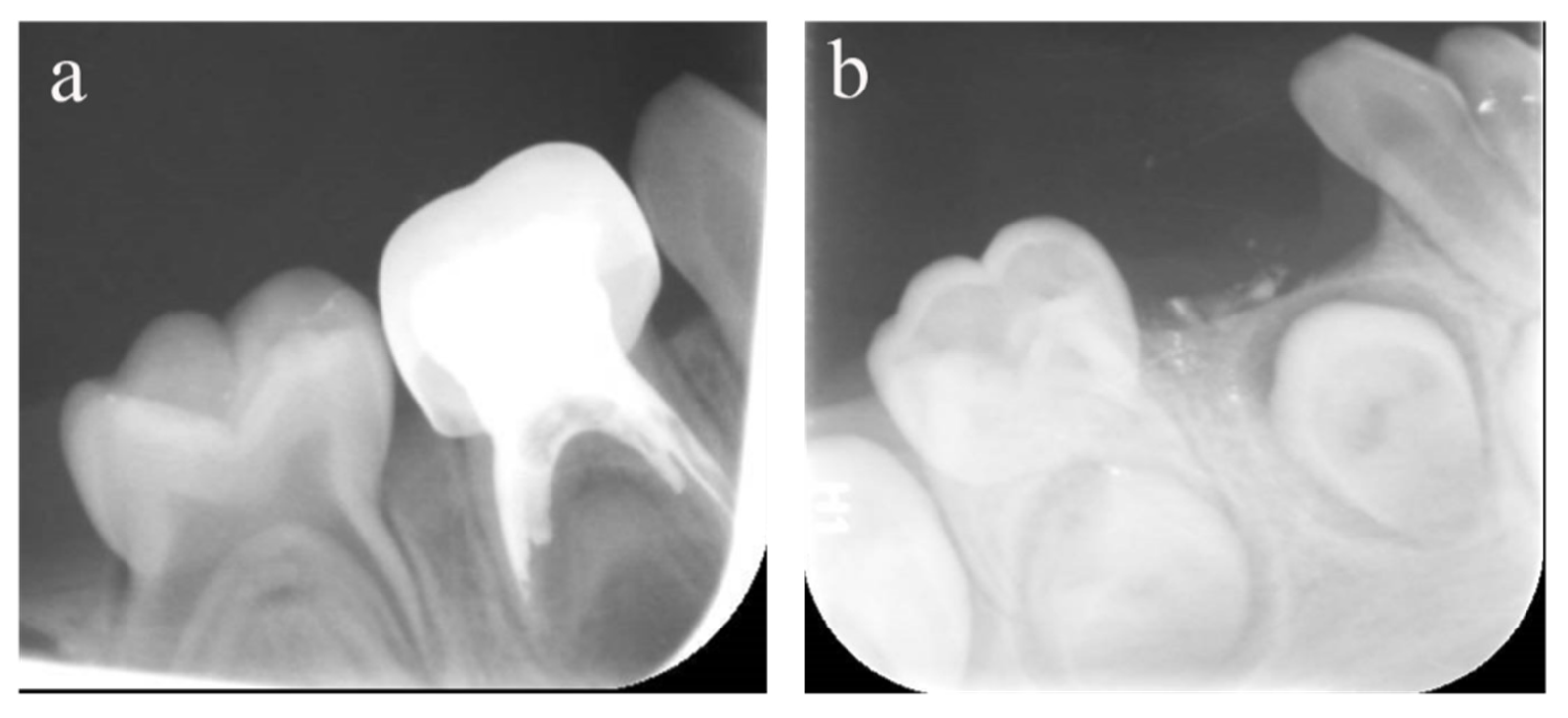
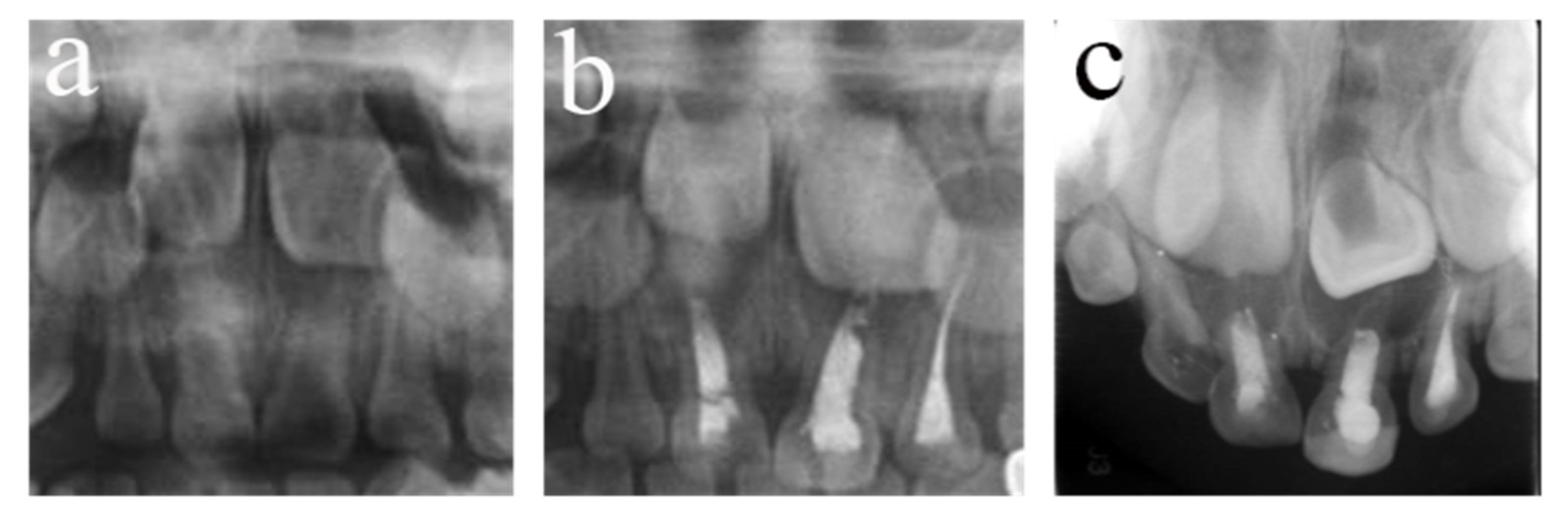
Radiographic criteria for success:
- (1)
The range of low-density shadows in the root area becomes small or disappears;
- (2)
The bone around the permanent tooth is intact;
- (3)
No pathological lesion presented in the successor permanent teeth;
- (4)
No pathological root resorption is observed.
The treatment is considered an overall failure if any one of the above items (regardless of clinical or radiological items) is not met or the primary teeth are lost prematurely.
2.5. Data Extraction
Data regarding (1) general information: case number, sex, and age of the patients; (2) preoperative information of teeth: tooth type, arch location, surfaces affected by caries, mobility, gingival condition, and radiological evaluation; (3) treatment information: root canal obturation materials, degree of root canal filling, and the restoration method; and (4) follow-up information: date, symptoms and signs, clinical examination, and radiographic evaluation were extracted independently by two paediatric dentistry postgraduates using a predesigned form in Microsoft Excel.
2.6. Consistency Test
Clinical evaluation is based on the medical record. The radiographic evaluation was independently evaluated by the two postgraduates. A professor resolved any disagreements between the two postgraduates. A pilot test was conducted on 30 images to estimate the consistency. The internal consistency (over two weeks) was 0.92 and 0.96, respectively, and the external consistency between them was 0.90.
2.7. Statistical Analysis
SPSS software (22.0 IBM SPSS statistics, Armonk, NY, USA) was used to calculate the mean and standard deviation (SD) and the frequency. R statistical computing software (version 4.04, Vienna, Austria) was used to estimate the survival rates at different times after treatment by the Kaplan-Meier method (K-M method). The annual mean failure rate was calculated according to the following formula [
15], where
y is the annual average failure rate and
x is the failure rate in the
zth year.
The shared frailty model is a proportional hazards model with random effects. The model was constructed for survival analysis and used to explore factors affecting the efficacy of pulpectomy in primary teeth. The significance level was taken as 0.05.
4. Discussion
Pulpectomy in the primary tooth is indicated for teeth with irreversible inflammation or necrosis. This treatment aims to remove debris and infection in the root canals, maintain the tooth’s physiological function, and extend its longevity [
16]. Extraction too early may not be a wise option for children. The premature loss of primary teeth may negatively impact masticatory performance and children phonation, which in turn affects the development of general and psychological health [
17,
18]. The early loss of primary teeth may also cause a space loss between the canines and molars and result in malocclusion and eruption abnormality [
17,
19,
20]. Pulpectomy in the primary tooth can maximize the retention of the nonvital primary tooth.
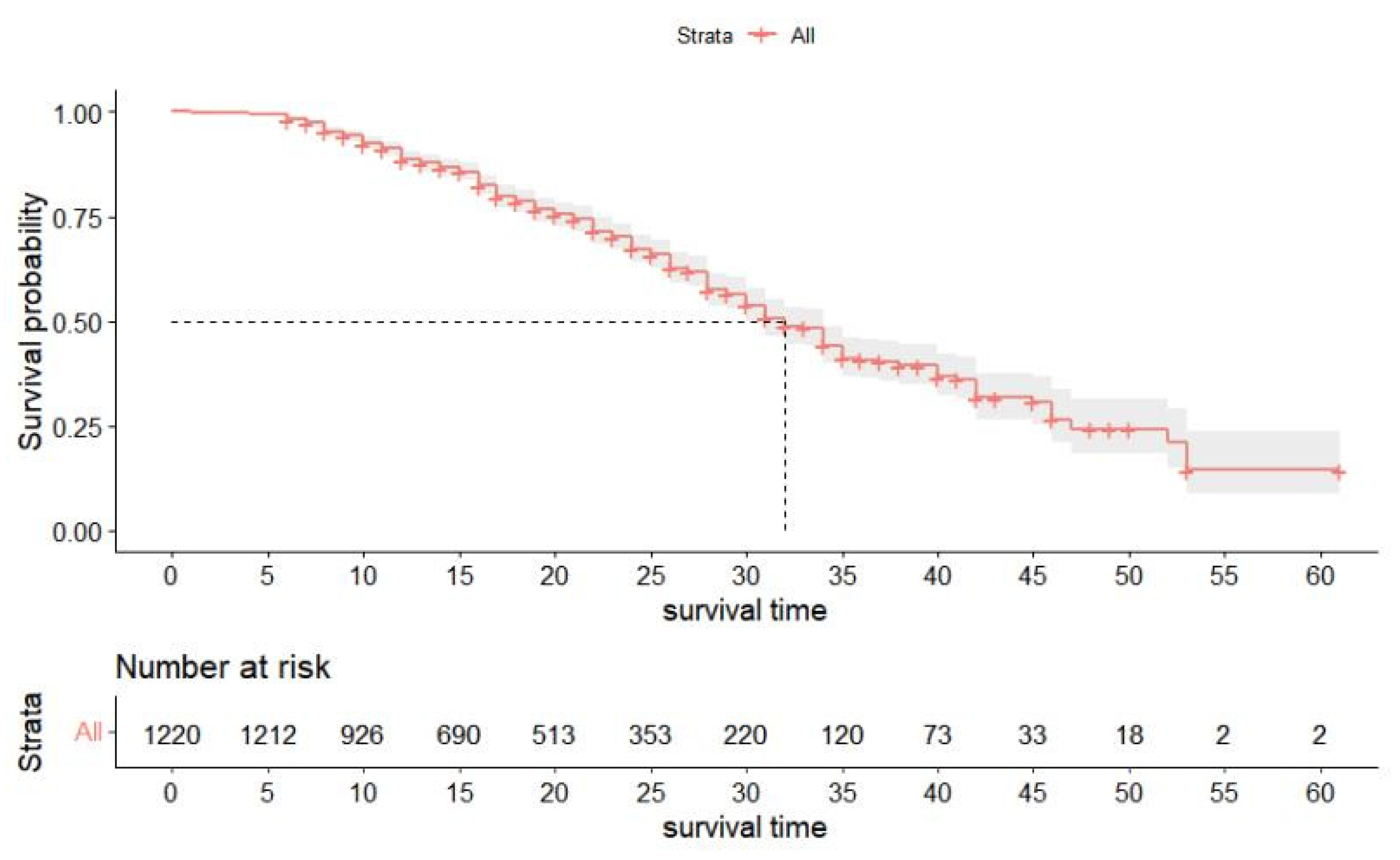
During the observation period of this study, 1671 children underwent pulpectomy, accounting for 86.54% of the total, and the average number of treated teeth per child was 3.70 ± 2.53. This indicates that pulpectomy in primary teeth accounted for a vast proportion of the pediatric dentist’s normal practice in China. This study showed a good prognosis in the short term, and the survival rate at 12 months reached above 85%, which can effectively control inflammation, relieve clinical symptoms, and restore mastication function. However, the long-term results are not satisfactory, especially in the posterior teeth, which may not survive until natural exfoliation. A recent systematic review of controlled studies found that the clinical and radiographic success rates of pulpectomy in the primary tooth ranged between 64% and 100% among the included studies with a 6–36 months observation period [
21]. However, only one study continued over 18 months (36 months) and studied the incisors only. Regarding the short-term prognosis, the result in the present study is consistent with and to some extent higher than other studies. However, for the long-term prognosis, the present study result is lower than the only study with 36 months (52.9% vs. 82%). However, the sample size in that study is much smaller than the present study. Additionally, the survival rate and change tendency is very similar with another study also conducted in China [
11].
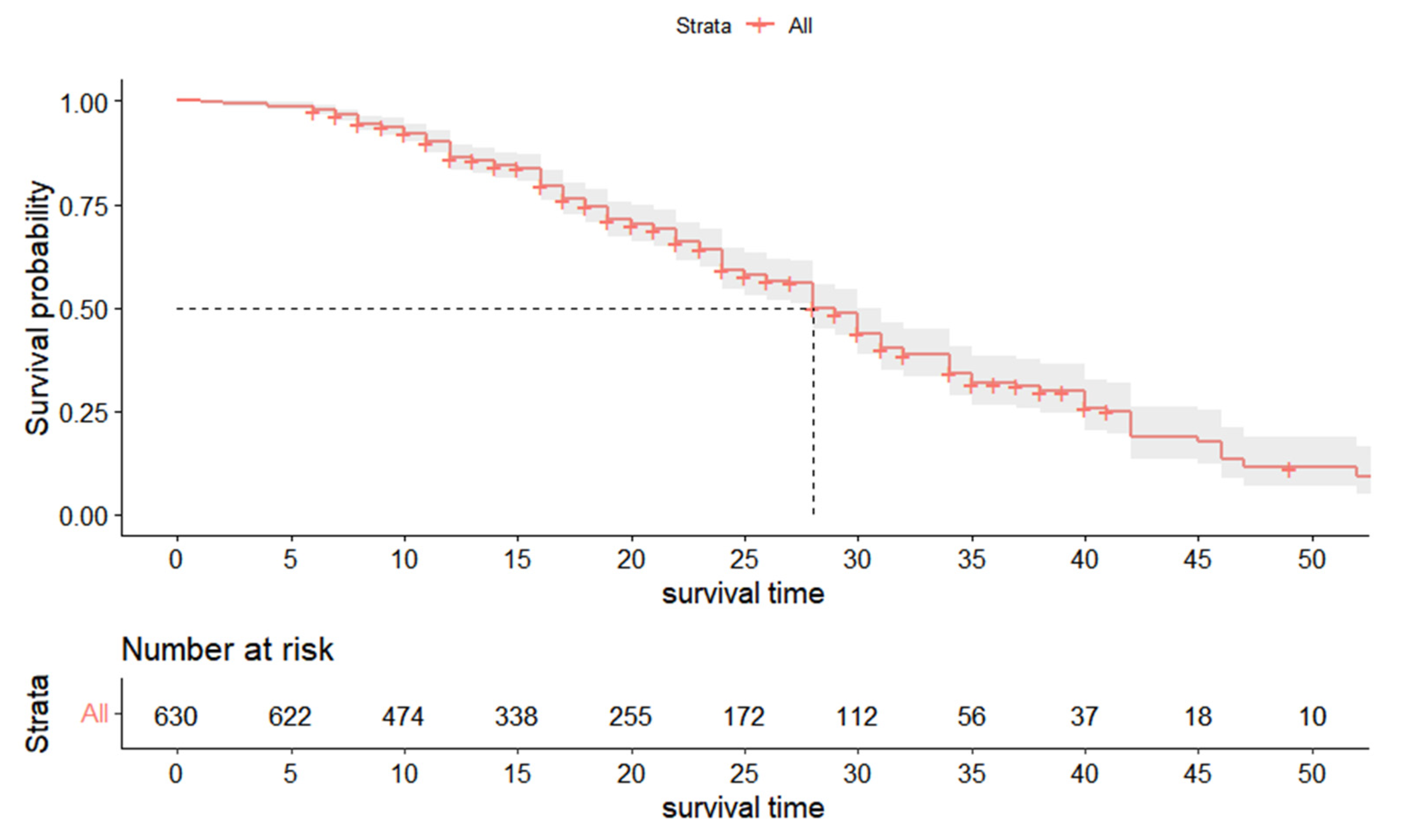
There are significant differences between the anterior and posterior teeth in root canal anatomy, bite force, and the time of eruption and exfoliation. Therefore, the survival curves of the anterior and posterior teeth were further analyzed separately, and there was a significant difference. Our findings resonate with a previous study suggesting that the median survival period of anterior teeth was significantly longer than that of posterior teeth [
11]. The difference is presumed to be induced by the anatomy of the root canal in the primary teeth. The root canal system in molars is much more complex than that in anterior teeth due to intricate microscopic structures such as accessory root canals and lateral root canals. Infection is more likely to reach the root apex and root bifurcation [
22], which makes adequate cleaning, shaping, and filling of root canals more difficult.
To explore the potential risk factors that may influence the survival of pulpectomy in primary teeth, this statistical analysis was based on the shared frailty model. The shared frailty model is a random-effects model where the frailties are common (or shared) among groups of individuals and are randomly distributed across groups [
23]. In the survival analysis, the Cox regression model is more common, but it assumes that the subjects in the model are independent. However, the survival time of different teeth in the same individual may be correlated. The shared frailty model can effectively reduce the random effects of such correlations [
24]. This study showed that the age of the children, tooth type, and radiographic evaluation are risk factors for pulpectomy survival. However, when separating the anterior and posterior teeth, it was found that survival in the anterior tooth was only associated with the tooth type and radiographic conditions. For the posterior tooth, the influencing factors were more complex, including age, tooth location, surfaces affected by caries, and radiological evaluation.
In line with a previous study, it was found that the tooth’s survival rate was significantly negatively correlated with age [
11]. The premature primary tooth has a prominent tooth pulp cavity, rich blood supply, and strong repair ability. As the age increases, the volume of the cavity and the repair capacity decrease [
25]. In addition, the complexity of the root canal system of primary teeth increases with the physiological or pathological resorption of the root [
22].
Regarding the tooth type and position, the prognosis of the primary canine and lateral incisor was significantly better than that of the central incisor. The possible reason is that the maxillary primary central incisor erupted early, and due to the existence of factors such as poor feeding habits, it is one of the predisposing sites of caries. The tooth condition may be relatively serious at the time of treatment. In addition, the eruption and exfoliation of the central incisor occurs much earlier than those of the lateral incisor and canine; thus, tooth resorption occurs earlier, which decreases the effect of treatment and lowers the survival time. The results of multivariate analysis in primary molars showed that the prognosis of maxillary primary molars was more favorable than that of mandibular primary molars, which may be related to the eruption time of the teeth and the anatomy of the root canal. Studies have confirmed that lateral and accessory canals are more prevalent in mandibular molars than in maxillary molars [
26]. In addition, there is some overlap between maxillary molars and successive permanent teeth on the radiological image, and small lesions may be relatively more difficult to identify. No statistically significant difference between the first and second primary molars was found in this study, which was consistent with the results of previous studies [
27,
28].
The number of surfaces affected by caries and the outcome of radiological evaluation are both related to the severity of the infections. After pulpectomy therapy, the resistance of dental hard tissue decreased. The larger the area affected by caries is, the higher the requirements for restoration after treatment and the more factors that need to be considered, such as the sealing ability of the materials, microleakage, and whether a good adjacency relationship can be established for the restoration. That is also why in our daily practice, it is routine to select PMC to restore the primary molars that underwent pulpectomy treatment. Therefore, the method of restoration was not analyzed as a covariate in the multivariate analysis. A previous study also confirmed that the use of PMC could improve the success rate [
29]. There was no significant difference in whether the anterior tooth used the strip resin crown. This may indicate that the survival rate does not depend on the restoration method but on the ability to retain the restorations and to avoid defects and microleakage. During the DGA, humidity and technique control could be carried well. In addition, due to the advantages of the strip resin crowns [
30], it became a preferred restoration method under DGA treatment when restoring the anterior tooth. Therefore, the number of teeth without strip resin crowns may not be sufficient to detect the difference. One study investigated differences in survival rates between irreversible pulpitis and periapical periodontitis [
31], and the findings were consistent with ours. This may be related to the fact that periapical periodontitis of the primary tooth is usually accompanied by root bifurcation lesions, which makes the inflammation more challenging to control [
31]. In addition, for teeth with periapical periodontitis, the short time of root canal disinfection under DGA and the lack of medicated disinfection during the interval between visits may be the other reasons for the lower survival rate.
There were also some variables, including mobility, gingival condition, root canal obturation materials, degree of root canal filling, and restoration methods, that did not show a significant correlation with the prognosis of pulpectomy in primary teeth. For the posterior molars, covariates including mobility, gingival condition, and the degree of root canal obturation showed statistical significance in the univariate analysis but not in the multivariate analysis. This indicates that these might have slight influences, but they do not contribute to the core outcome. It can be inferred from the result that radiographic evaluation is more important than clinical symptoms (abnormal ability, gingiva swelling, or fistula) in the primary molars when assessing the prognosis of pulpectomy. Taking radiographic images should be a regular method when necessary and call for the attention of practitioners. The degree of root canal obturation showed a significant difference in the univariate analysis but not in the multivariate analysis. However, in some other studies, the authors considered under- and overfilling to be the reasons for the failure of primary tooth pulpectomy [
32,
33]. This inconsistency may be due to the difficulty in measuring the primary tooth work length and the deviations of the root canal filling degree of classification.
There are many discussions on root canal obturation materials [
34,
35,
36]. Rabinowitch stated some requirements on the idea of filling materials [
37]. Currently, ZOE, calcium hydroxide, and iodoform are the commonly used materials for the filling paste. However, there is still no such primary root filling material that can fulfill all of these requirements, especially in terms of the requirement that the resorption rate should match the physiologic root resorption of the primary teeth [
38]. In our clinical, only ZOE paste and Vitapex paste are available. ZOE paste is a manual paste with Zinc oxide powder (0.36 g) and eugenol (0.28 g). ZOE paste had a better inhibitory activity compared with other fillings and a good work time, and it is also easy to mix, cost effective, and insoluble in tissue fluids [
39]. The disadvantages of ZOE paste is that the resorption rate of the ZOE particles extruded out of the apical foramen is slow and it alters the path of eruption of succedaneous teeth and causes soft tissue irritation and allergy to eugenol, and exhibits cytotoxicity and neurotoxicity [
39,
40]. Vitapex is a commercial product which contains 40.4% iodoform, 30.3% calcium hydroxide, and 22.4% silicone. The advantage of Vitapex is its absorbability. The extruded particle from the apex can be absorbed thoroughly and quickly. Meanwhile, the rate of resorption from within the canals is faster than physiological root resorption [
39]. A previous meta-analysis compared the success rate between the calcium hydroxide/iodoform paste and ZOE and found no statistically significant difference in the short term (6- and 12-month follow-up) [
41]. However, ZOE was shown to have significantly higher success rates at the ≥18-month follow-up [
41,
42]. In the present study, no significant difference was identified regarding the different filling materials, but a higher failure proportion can still be found in the Vitapex. This may be related to the fact that the absorption rate of Vitapex in the root canal is faster than that of the tooth root, and it is easy to form a cavity in the root canal, which can easily cause reinfection.
This study enriched the survival analysis of primary root canal therapy and the possible potential risk factors. Currently, the research in this field is insufficient, and this study is based on a relatively large sample size and an extended follow-up, so the results of this study are fairly reliable. However, this study still has some limitations that should be emphasized. First, this was a retrospective study. All of the data are extracted from the medical record, and there might be some mis-recording or inaccurate recordings that cannot be identified. Second, the recruited participants came from a convenience sampling and underwent DGA treatment with expert dentists. Thus, the participants and clinicians are not representative of the general population and are prone to selection bias. Third, snacking frequency, feeding and oral hygiene habits or conditions, parental education levels, and socioeconomic background are highly associated with ECC occurrence [
43], but in the present study, these factors cannot be controlled because in the previous medical record system, no related information was being recorded. These potential factors may confound the statistical results.
The two-year survival rate of primary tooth pulpectomy is relatively high and stable. The non-vital primary tooth can be maximally retained to rehabilitate the chewing function via pulpectomy. However, during the therapy, its indications should be strictly followed. Attention should be paid to risk factors such as age, tooth position, surfaces affected by caries, and preoperative tooth periapical condition. The AAPD recommends that primary teeth undergoing pulpectomy treatment should take radiographic evaluation biannually [
8]. For children with the above risk factors, compliance should be improved to achieve a customized frequency of dental visit, usually once every three to six months.
All of the treatments in the study are completed under DGA. Although it can eliminate the confounder of children’s cooperation, the time for root canal disinfection is shorter, which may be one of the reasons that affect its curative effect. Therefore, how to effectively control the infection of periapical teeth under DGA remains to be further studied. In addition, implementing more high-quality clinical randomized trials in the future can contribute to building a better evidence-based pulpectomy dentistry foundation.

 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}