
Work-Related Psychosocial Factors and Global Cognitive Function: Are Telomere Length and Low-Grade Inflammation Potential Mediators of This Association?

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
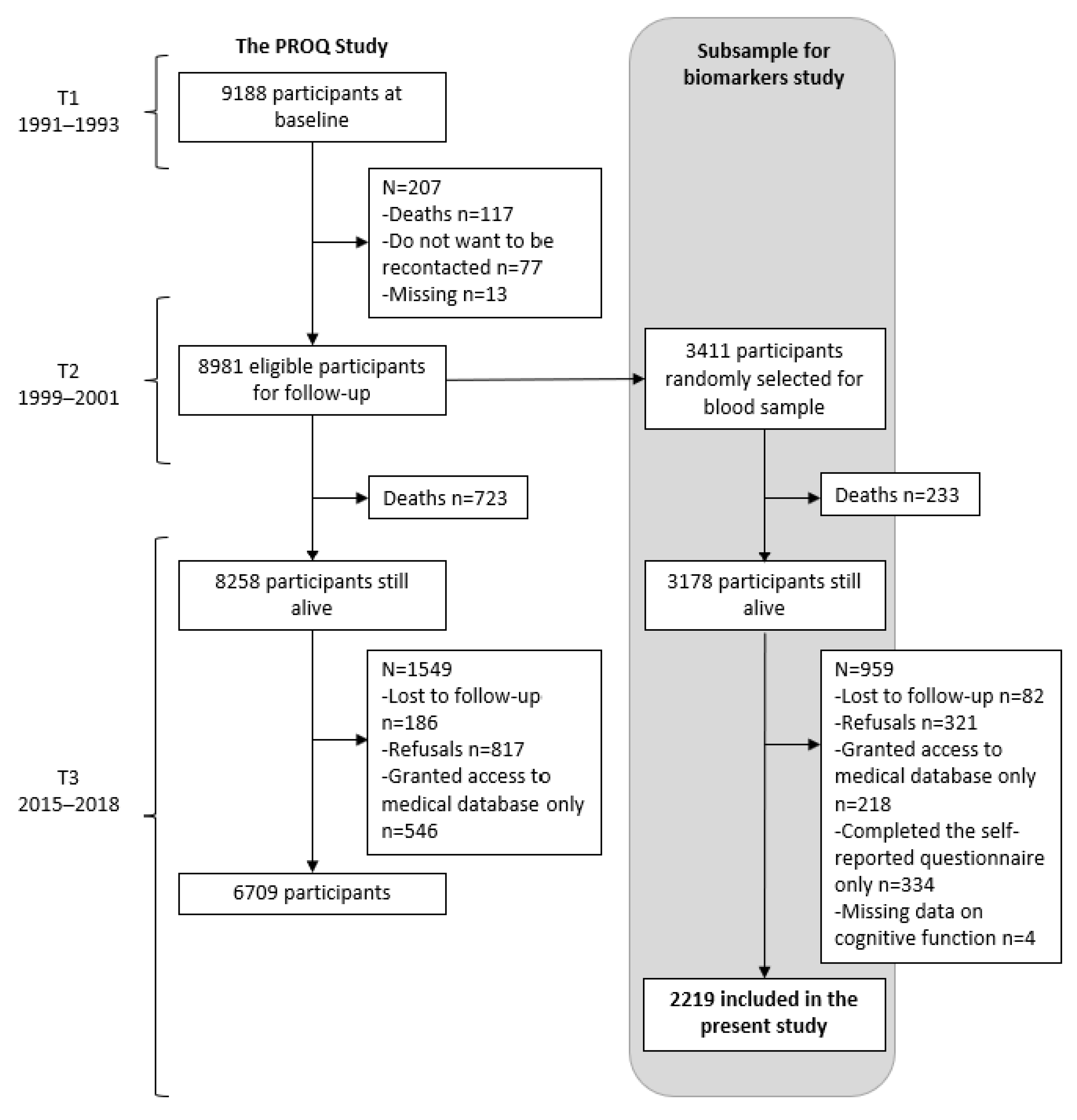
2.1. Study Design and Data Collection
2.2. Work-Related Psychosocial Factors
2.3. Cognitive Function
2.4. Blood Samples
2.5. Telomere Length
2.6. Inflammatory Biomarkers
2.7. Covariates
2.8. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Longitudinal Associations of Work-Related Psychosocial Factors with Telomere Length and Inflammatory Index
3.3. Cross-Sectional (T3) Associations of Telomere Length and Inflammatory Index with Cognitive Function
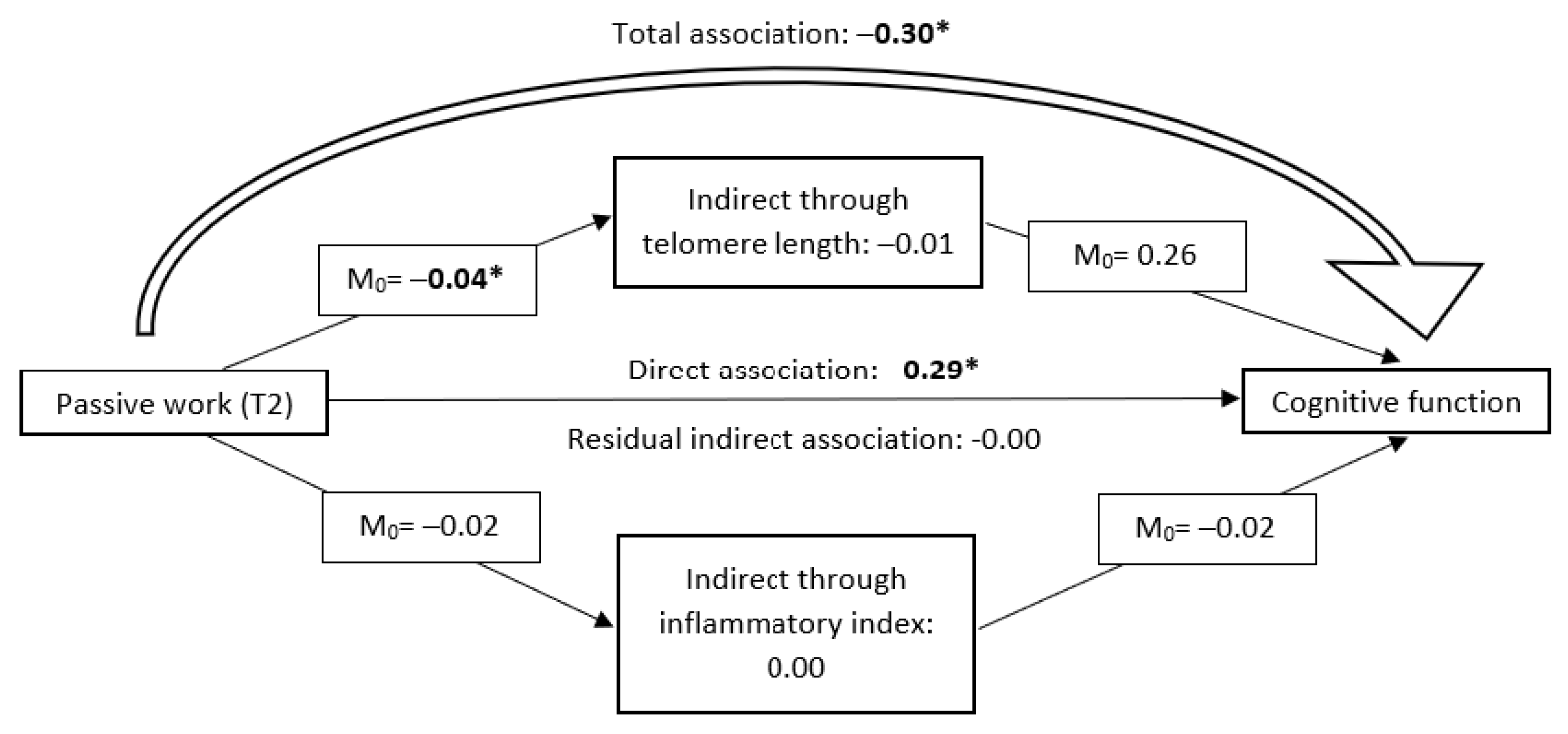
3.4. Mediating Effects of Telomere Length and Inflammatory Index
4. Discussion
4.1. Interpretation of Results
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Disease International. From Plan to Impact IV: Progress towards Targets of the WHO Global Action Plan on Dementia; Alzheimer’s Disease International: London, UK, 2021. [Google Scholar]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2020, 16, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Nexo, M.A.; Meng, A.; Borg, V. Can psychosocial work conditions protect against age-related cognitive decline? Results from a systematic review. Occup. Environ. Med. 2016, 73, 487–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Then, F.S.; Luck, T.; Luppa, M.; Thinschmidt, M.; Deckert, S.; Nieuwenhuijsen, K.; Seidler, A.; Riedel-Heller, S.G. Systematic review of the effect of the psychosocial working environment on cognition and dementia. Occup. Environ. Med. 2014, 71, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.Y.; Hu, H.Y.; Wang, Z.T.; Ma, Y.H.; Dong, Q.; Tan, L.; Yu, J.T. Association of Occupational Factors and Dementia or Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2020, 78, 217–227. [Google Scholar] [CrossRef]
- Rugulies, R.; Aust, B.; Madsen, I.E. Effort-reward imbalance at work and risk of depressive disorders. A systematic review and meta-analysis of prospective cohort studies. Scand. J. Work Environ. Health 2017, 43, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Duchaine, C.S.; Aubé, K.; Gilbert-Ouimet, M.; Vézina, M.; Ndjaboué, R.; Massamba, V.; Talbot, D.; Lavigne-Robichaud, M.; Trudel, X.; Pena-Gralle, A.B.; et al. Psychosocial Stressors at Work and the Risk of Sickness Absence Due to a Diagnosed Mental Disorder: A Systematic Review and Meta-analysis. JAMA Psychiatry 2020, 77, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Madsen, I.E.H.; Nyberg, S.T.; Magnusson Hanson, L.L.; Ferrie, J.E.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Job strain as a risk factor for clinical depression: Systematic review and meta-analysis with additional individual participant data. Psychol. Med. 2017, 47, 1342–1356. [Google Scholar] [CrossRef] [Green Version]
- Straub, R.H.; Cutolo, M. Psychoneuroimmunology-developments in stress research. Wien. Med. Wochenschr. 2018, 168, 76–84. [Google Scholar] [CrossRef]
- Zhang, J.; Rane, G.; Dai, X.; Shanmugam, M.K.; Arfuso, F.; Samy, R.P.; Lai, M.K.; Kappei, D.; Kumar, A.P.; Sethi, G. Ageing and the telomere connection: An intimate relationship with inflammation. Ageing Res. Rev. 2016, 25, 55–69. [Google Scholar] [CrossRef]
- Blackburn, E.H. Telomere states and cell fates. Nature 2000, 408, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Devore, E.E.; Prescott, J.; De Vivo, I.; Grodstein, F. Relative telomere length and cognitive decline in the Nurses’ Health Study. Neurosci. Lett. 2011, 492, 15–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaffe, K.; Lindquist, K.; Kluse, M.; Cawthon, R.; Harris, T.; Hsueh, W.C.; Simonsick, E.M.; Kuller, L.; Li, R.; Ayonayon, H.N.; et al. Telomere length and cognitive function in community-dwelling elders: Findings from the Health ABC Study. Neurobiol. Aging 2011, 32, 2055–2060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pudas, S.; Josefsson, M.; Nordin Adolfsson, A.; Landfors, M.; Kauppi, K.; Veng-Taasti, L.M.; Hultdin, M.; Adolfsson, R.; Degerman, S. Short leukocyte telomeres, but not telomere attrition rates, predict memory decline in the 20-year longitudinal Betula study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 76, 955–963. [Google Scholar] [CrossRef] [PubMed]
- West, N.A.; Kullo, I.J.; Morris, M.C.; Mosley, T.H. Sex-specific associations of inflammation markers with cognitive decline. Exp. Gerontol. 2020, 138, 110986. [Google Scholar] [CrossRef] [PubMed]
- Lindbergh, C.A.; Casaletto, K.B.; Staffaroni, A.M.; Elahi, F.; Walters, S.M.; You, M.; Neuhaus, J.; Rivera Contreras, W.; Wang, P.; Karydas, A.; et al. Systemic Tumor Necrosis Factor-Alpha Trajectories Relate to Brain Health in Typically Aging Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1558–1565. [Google Scholar] [CrossRef]
- Walker, K.A.; Gottesman, R.F.; Wu, A.; Knopman, D.S.; Gross, A.L.; Mosley, T.H., Jr.; Selvin, E.; Windham, B.G. Systemic inflammation during midlife and cognitive change over 20 years: The ARIC Study. Neurology 2019, 92, e1256–e1267. [Google Scholar] [PubMed]
- Zheng, F.; Xie, W. High-sensitivity C-reactive protein and cognitive decline: The English Longitudinal Study of Ageing. Psychol. Med. 2018, 48, 1381–1389. [Google Scholar] [CrossRef]
- Fiocco, A.J.; Krieger, L.; D’Amico, D.; Parrott, M.D.; Laurin, D.; Gaudreau, P.; Greenwood, C.; Ferland, G. A systematic review of existing peripheral biomarkers of cognitive aging: Is there enough evidence for biomarker proxies in behavioral modification interventions? An initiative in association with the nutrition, exercise and lifestyle team of the Canadian Consortium on Neurodegeneration in Aging. Ageing Res. Rev. 2019, 52, 72–119. [Google Scholar]
- Kuo, H.K.; Yen, C.J.; Chang, C.H.; Kuo, C.K.; Chen, J.H.; Sorond, F. Relation of C-reactive protein to stroke, cognitive disorders, and depression in the general population: Systematic review and meta-analysis. Lancet Neurol. 2005, 4, 371–380. [Google Scholar] [CrossRef]
- Koyama, A.; O’Brien, J.; Weuve, J.; Blacker, D.; Metti, A.L.; Yaffe, K. The role of peripheral inflammatory markers in dementia and Alzheimer’s disease: A meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, T. Systemic inflammatory markers and risk of dementia. Am. J. Alzheimers Dis. Other Demen. 2006, 21, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.; Trollor, J.N.; Crawford, J.; Brown, D.A.; Baune, B.T.; Samaras, K.; Campbell, L.; Breit, S.N.; Brodaty, H.; Sachdev, P.; et al. Macrophage inhibitory cytokine-1 is associated with cognitive impairment and predicts cognitive decline–the Sydney Memory and Aging Study. Aging Cell 2013, 12, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y.; Clements, M.S.; Roberts, R.O.; Vassilaki, M.; Druliner, B.R.; Boardman, L.A.; Petersen, R.C.; Reynolds, C.A.; Pedersen, N.L.; Hagg, S. Association of telomere length with general cognitive trajectories: A meta-analysis of four prospective cohort studies. Neurobiol. Aging 2018, 69, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Colicino, E.; Wilson, A.; Frisardi, M.C.; Prada, D.; Power, M.C.; Hoxha, M.; Dioni, L.; Spiro, A.; Vokonas, P.S.; Weisskopf, M.G.; et al. Telomere Length, Long-Term Black Carbon Exposure, and Cognitive Function in a Cohort of Older Men: The VA Normative Aging Study. Environ. Health Perspect. 2017, 125, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, S.E.; Marioni, R.E.; Martin-Ruiz, C.; Pattie, A.; Gow, A.J.; Cox, S.R.; Corley, J.; von Zglinicki, T.; Starr, J.M.; Deary, I.J. Longitudinal telomere length shortening and cognitive and physical decline in later life: The Lothian Birth Cohorts 1936 and 1921. Mech. Ageing Dev. 2016, 154, 43–48. [Google Scholar] [CrossRef]
- Legdeur, N.; Heymans, M.W.; Comijs, H.C.; Huisman, M.; Maier, A.B.; Visser, P.J. Age dependency of risk factors for cognitive decline. BMC Geriatr. 2018, 18, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karasek, R. Job-demands, job decision latitude, and mental strain: Implications for job redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Johnson, J.V. Theoretical developments in psychosocial work environment research. Int. J. Health Serv. 1989, 19, 457–458. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Gilbert-Ouimet, M.; Trudel, X.; Brisson, C.; Milot, A.; Vézina, M. Adverse effects of psychosocial work factors on blood pressure: Systematic review of studies on demand-control-support and effort-reward imbalance models. Scand. J. Work Environ. Health 2014, 40, 109–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sara, J.D.; Prasad, M.; Eleid, M.F.; Zhang, M.; Widmer, R.J.; Lerman, A. Association Between Work-Related Stress and Coronary Heart Disease: A Review of Prospective Studies Through the Job Strain, Effort-Reward Balance, and Organizational Justice Models. J. Am. Heart Assoc. 2018, 7, e008073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Xu, S.; Hua, J.; Zhu, D.; Liu, C.; Hu, Y.; Liu, T.; Xu, D. Association between job strain and risk of incident stroke: A meta-analysis. Neurology 2015, 85, 1648–1654. [Google Scholar] [CrossRef]
- Pena-Gralle, A.P.B.; Talbot, D.; Duchaine, C.S.; Lavigne-Robichaud, M.; Trudel, X.; Aubé, K.; Gralle, M.; Gilbert-Ouimet, M.; Milot, A.; Brisson, C. Job strain and effort-reward imbalance as risk factors for type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Scand. J. Work Environ. Health 2022, 48, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.Y.; Xu, W.; Mangialasche, F.; Dekhtyar, S.; Fratiglioni, L.; Wang, H.X. Working Life Psychosocial Conditions in Relation to Late-Life Cognitive Decline: A Population-Based Cohort Study. J. Alzheimers Dis. 2019, 67, 315–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andel, R.; Crowe, M.; Kareholt, I.; Wastesson, J.; Parker, M.G. Indicators of job strain at midlife and cognitive functioning in advanced old age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duchaine, C.S.; Brisson, C.; Talbot, D.; Gilbert-Ouimet, M.; Trudel, X.; Vézina, M.; Milot, A.; Diorio, C.; Ndjaboué, R.; Giguère, Y.; et al. Cumulative exposure to psychosocial stressors at work and global cognitive function: The PROspective Quebec Study on Work and Health. Occup. Environ. Med. 2021, 78, 884–892. [Google Scholar] [CrossRef]
- Dong, L.; Eaton, W.W.; Spira, A.P.; Agnew, J.; Surkan, P.J.; Mojtabai, R. Job strain and cognitive change: The Baltimore Epidemiologic Catchment Area follow-up study. Occup. Environ. Med. 2018, 75, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, C.; Andel, R.; Fors, S.; Meinow, B.; Darin Mattsson, A.; Kareholt, I. Associations between work-related stress in late midlife, educational attainment, and serious health problems in old age: A longitudinal study with over 20 years of follow-up. BMC Public Health 2014, 14, 878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnusson Hanson, L.L.; Virtanen, M.; Rod, N.H.; Steptoe, A.; Head, J.; David Batty, G.; Kivimaki, M.; Westerlund, H. Does inflammation provide a link between psychosocial work characteristics and diabetes? Analysis of the role of interleukin-6 and C-reactive protein in the Whitehall II cohort study. Brain Behav. Immun. 2019, 78, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Shirom, A.; Toker, S.; Berliner, S.; Shapira, I. The Job Demand-Control-Support Model and stress-related low-grade inflammatory responses among healthy employees: A longitudinal study. Work Stress 2008, 22, 138–152. [Google Scholar] [CrossRef]
- Coronado, J.I.C.; Chandola, T.; Steptoe, A. Allostatic Load and Effort-Reward Imbalance: Associations over the Working-Career. Int. J. Environ. Res. Public Health 2018, 15, 191. [Google Scholar] [CrossRef] [Green Version]
- Duchaine, C.S.; Brisson, C.; Talbot, D.; Gilbert-Ouimet, M.; Trudel, X.; Vézina, M.; Milot, A.; Diorio, C.; Ndjaboué, R.; Giguère, Y.; et al. Psychosocial stressors at work and inflammatory biomarkers: PROspective Quebec Study on Work and Health. Psychoneuroendocrinology 2021, 133, 105400. [Google Scholar] [CrossRef] [PubMed]
- Hoven, H.; Siegrist, J. Work characteristics, socioeconomic position and health: A systematic review of mediation and moderation effects in prospective studies. Occup. Environ. Med. 2013, 70, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Bekhbat, M.; Neigh, G.N. Sex differences in the neuro-immune consequences of stress: Focus on depression and anxiety. Brain Behav. Immun. 2018, 67, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gardner, M.; Bann, D.; Wiley, L.; Cooper, R.; Hardy, R.; Nitsch, D.; Martin-Ruiz, C.; Shiels, P.; Sayer, A.A.; Barbieri, M.; et al. Gender and telomere length: Systematic review and meta-analysis. Exp. Gerontol. 2014, 51, 15–27. [Google Scholar] [CrossRef]
- Li, R.; Singh, M. Sex differences in cognitive impairment and Alzheimer’s disease. Front. Neuroendocrinol. 2014, 35, 385–403. [Google Scholar] [CrossRef] [Green Version]
- Levine, D.A.; Gross, A.L.; Briceño, E.M.; Tilton, N.; Giordani, B.J.; Sussman, J.B.; Hayward, R.A.; Burke, J.F.; Hingtgen, S.; Elkind, M.S.V.; et al. Sex Differences in Cognitive Decline Among US Adults. JAMA Netw. Open 2021, 4, e210169. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2022 Alzheimer’s disease facts and figures. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2022, 18, 700–789. [Google Scholar] [CrossRef]
- Trudel, X.; Gilbert-Ouimet, M.; Milot, A.; Duchaine, C.S.; Vézina, M.; Laurin, D.; Sultan-Taieb, H.; Brisson, C. Cohort Profile: The PROspective Quebec (PROQ) Study on Work and Health. Int. J. Epidemiol. 2018, 47, 693–693i. [Google Scholar] [CrossRef] [Green Version]
- Brisson, C.; Blanchette, C.; Guimont, C.; Dion, J.; Moisan, J.; Vézina, M. Reliability and Validity of the French Version of the 18-item Karasek Job Content Questionnaire. Work Stress 1998, 12, 322–336. [Google Scholar] [CrossRef]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef]
- Niedhammer, I. Psychometric properties of the French version of the Karasek Job Content Questionnaire: A study of the scales of decision latitude, psychological demands, social support, and physical demands in the GAZEL cohort. Int. Arch. Occup. Environ. Health 2002, 75, 129–144. [Google Scholar] [CrossRef]
- Niedhammer, I.; Siegrist, J.; Landre, M.F.; Goldberg, M.; Leclerc, A. Psychometric properties of the French version of the Effort-Reward Imbalance model. Rev. Epidemiol. Sante Pub. 2000, 48, 419–437. [Google Scholar]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The measurement of effort-reward imbalance at work: European comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Santé Québec. Et votre coeur, ça va? In Rapport de L’enquête Québécoise sur la Santé Cardiovasculaire; Gouvernement du Québec: Québec, QC, Canada, 1990. [Google Scholar]
- Aboa-Éboulé, C.; Brisson, C.; Blanchette, C.; Maunsell, E.; Bourbonnais, R.; Abdous, B.; Vézina, M.; Milot, A.; Dagenais, G.R. Effort-reward imbalance at work and psychological distress: A validation study of post-myocardial infarction patients. Psychosom Med. 2011, 73, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Dong, Y.; Lee, W.Y.; Basri, N.A.; Collinson, S.L.; Merchant, R.A.; Venketasubramanian, N.; Chen, C.L. The Montreal Cognitive Assessment is superior to the Mini-Mental State Examination in detecting patients at higher risk of dementia. Int. Psychogeriatr. 2012, 24, 1749–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, T.C.C.; Machado, L.; Bulgacov, T.M.; Rodrigues-Junior, A.L.; Costa, M.L.G.; Ximenes, R.C.C.; Sougey, E.B. Is the Montreal Cognitive Assessment (MoCA) screening superior to the Mini-Mental State Examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer’s Disease (AD) in the elderly? Int. Psychogeriatr. 2018, 31, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Ennour-Idrissi, K.; Tetu, B.; Maunsell, E.; Poirier, B.; Montoni, A.; Rochette, P.J.; Diorio, C. Association of Telomere Length with Breast Cancer Prognostic Factors. PLoS ONE 2016, 11, e0161903. [Google Scholar] [CrossRef] [Green Version]
- Cawthon, R.M. Telomere length measurement by a novel monochrome multiplex quantitative PCR method. Nucleic Acids Res. 2009, 37, e21. [Google Scholar] [CrossRef] [Green Version]
- Yang, I.V.; Chen, E.; Hasseman, J.P.; Liang, W.; Frank, B.C.; Wang, S.; Sharov, V.; Saeed, A.I.; White, J.; Li, J.; et al. Within the fold: Assessing differential expression measures and reproducibility in microarray assays. Genome Biol. 2002, 3, research0062. [Google Scholar] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- The Joint National Committee on Prevention Detection Evaluation and Treatment of High Blood Pressure. The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch. Intern. Med. 1997, 157, 2413–2446.
- Strugo, V.; Glew, F.J.; Davis, J.; Opie, L.H. Update: Recommendations for human blood pressure determination by sphygmomanometers. Hypertension 1990, 16, 594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vansteelandt, S.; Daniel, R.M. Interventional Effects for Mediation Analysis with Multiple Mediators. Epidemiology 2017, 28, 258–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Hernán, M.A.; Robins, J.M. Causal Inference: What If. 2020. Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/1268/2020/02/ci_hernanrobins_21feb20.pdf (accessed on 12 October 2022).
- Almadi, T.; Cathers, I.; Chow, C.M. Associations among work-related stress, cortisol, inflammation, and metabolic syndrome. Psychophysiology 2013, 50, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Misiak, B.; Leszek, J.; Kiejna, A. Metabolic syndrome, mild cognitive impairment and Alzheimer’s disease—The emerging role of systemic low-grade inflammation and adiposity. Brain Res. Bull. 2012, 89, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [Green Version]
- Zhuo, L.B.; Pei, J.J.; Yan, Z.; Yao, W.; Hao, C.F.; Wang, H.X. Working life job strain status and cognitive aging in Europe: A 12-year follow-up study. J. Affect. Disord. 2021, 295, 1177–1183. [Google Scholar] [CrossRef]
- Sabbath, E.L.; Andel, R.; Zins, M.; Goldberg, M.; Berr, C. Domains of cognitive function in early old age: Which ones are predicted by pre-retirement psychosocial work characteristics? Occup. Environ. Med. 2016, 73, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.Y.; Xu, W.; Mangialasche, F.; Grande, G.; Fratiglioni, L.; Wang, H.X. The role of Apolipoprotein E epsilon4 in the association between psychosocial working conditions and dementia. Aging 2020, 12, 3730–3746. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.X.; Wahlberg, M.; Karp, A.; Winblad, B.; Fratiglioni, L. Psychosocial stress at work is associated with increased dementia risk in late life. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2012, 8, 114–120. [Google Scholar]
- Kivimäki, M.; Walker, K.A.; Pentti, J.; Nyberg, S.T.; Mars, N.; Vahtera, J.; Suominen, S.B.; Lallukka, T.; Rahkonen, O.; Pietiläinen, O.; et al. Cognitive stimulation in the workplace, plasma proteins, and risk of dementia: Three analyses of population cohort studies. BMJ 2021, 374, n1804. [Google Scholar] [CrossRef] [PubMed]
- Agbenyikey, W.; Karasek, R.; Cifuentes, M.; Wolf, P.A.; Seshadri, S.; Taylor, J.A.; Beiser, A.S.; Au, R. Job strain and cognitive decline: A prospective study of the framingham offspring cohort. Int. J. Occup. Environ. Med. 2015, 6, 79–94. [Google Scholar] [CrossRef] [Green Version]
- Fujishiro, K.; Diez-Roux, A.V.; Landsbergis, P.A.; Jenny, N.S.; Seeman, T. Current employment status, occupational category, occupational hazard exposure and job stress in relation to telomere length: The Multiethnic Study of Atherosclerosis (MESA). Occup. Environ. Med. 2013, 70, 552–560. [Google Scholar] [CrossRef]
- Chmelar, C.; Jorres, R.A.; Kronseder, A.; Muller, A.; Nowak, D.; Weigl, M. Associations Between Age, Psychosocial Work Conditions, Occupational Well-Being, and Telomere Length in Geriatric Care Professionals: A Mixed-Methods Study. J. Occup. Environ. Med. 2017, 59, 949–955. [Google Scholar] [CrossRef]
- Meier, H.C.S.; Hussein, M.; Needham, B.; Barber, S.; Lin, J.; Seeman, T.; Diez Roux, A. Cellular response to chronic psychosocial stress: Ten-year longitudinal changes in telomere length in the Multi-Ethnic Study of Atherosclerosis. Psychoneuroendocrinology 2019, 107, 70–81. [Google Scholar] [CrossRef]
- Cohen-Manheim, I.; Doniger, G.M.; Sinnreich, R.; Simon, E.S.; Pinchas, R.; Aviv, A.; Kark, J.D. Increased attrition of leukocyte telomere length in young adults is associated with poorer cognitive function in midlife. Eur. J. Epidemiol. 2016, 31, 147–157. [Google Scholar] [CrossRef] [Green Version]
- Massamba, V.K.; Talbot, D.; Milot, A.; Pearce, N.; Trudel, X.; Brisson, C. Assessment of the healthy worker survivor effect in the relationship between psychosocial work-related factors and hypertension. Occup. Environ. Med. 2019, 76, 414–421. [Google Scholar] [CrossRef] [Green Version]
- Pearce, N.; Checkoway, H.; Kriebel, D. Bias in occupational epidemiology studies. Occup. Environ. Med. 2007, 64, 562–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, J.P.; Keil, A.P.; McGrath, L.J.; Edwards, J.K. Evolving methods for inference in the presence of healthy worker survivor bias. Epidemiology 2015, 26, 204–212. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall c N = 2219 Mean ± SD or n (%) | Females N = 1133 (51%) Mean ± SD or n (%) | Males N = 1086 (49%) Mean ± SD or n (%) | |
|---|---|---|---|
| Age (y) | |||
| At T1 (1991–1993) | 38.9 ± 7.9 | 37.4 ± 7.4 | 40.4 ± 8.0 |
| At T2 (1999–2001) | 46.5 ± 7.9 | 45.0 ± 7.4 | 48.0 ± 8.1 |
| At T3 (2015–2018) | 63.2 ± 7.4 | 61.8 ± 7.0 | 64.7 ± 7.6 |
| Education at T3 (y) | 15.3 ± 2.9 | 14.3 ± 2.7 | 16.3 ± 2.7 |
| Smoking status | |||
| Never smoked regularly | 1012 (46.0) | 546 (48.5) | 466 (43.4) |
| Former regular smoker | 735 (33.4) | 330 (29.3) | 405 (37.7) |
| Current occasional smoker d | 101 (4.6) | 55 (4.9) | 46 (4.3) |
| Current regular smoker d | 351 (16.0) | 195 (17.3) | 156 (14.5) |
| Alcohol intake (drinks/week) | 3.5 ± 4.5 | 2.3 ± 2.9 | 4.7 ± 5.4 |
| Physical activity (times/month) | 5.3 ± 4.3 | 4.7 ± 4.2 | 6.0 ± 4.4 |
| Body mass index (kg/m2) | 24.5 ± 3.8 | 23.5 ± 3.9 | 25.5 ± 3.5 |
| Waist-to-hip ratio | 0.84 ± 0.1 | 0.76 ± 0.07 | 0.92 ± 0.05 |
| Diabetes (yes) | 34 (1.5) | 22 (1.9) | 12 (1.1) |
| Hypertension (yes) | 347 (15.6) | 120 (10.6) | 227 (20.9) |
| Cardiovascular diseases (yes) | 52 (2.3) | 26 (2.3) | 26 (2.4) |
| Confidants (number) | 2.1 ± 1.5 | 2.3 ± 1.4 | 1.9 ± 1.5 |
| Helpers (number) | 3.0 ± 1.6 | 3.1 ± 1.5 | 2.9 ± 1.7 |
| Relationship with spouse | |||
| Satisfying | 1370 (64.8) | 647 (59.6) | 723 (70.3) |
| Unsatisfying | 215 (10.2) | 112 (10.3) | 103 (10.0) |
| No spouse | 528 (25.0) | 326 (30.1) | 202 (19.7) |
| Relationship with children | |||
| Satisfying | 1311 (61.1) | 611 (55.4) | 310 (29.7) |
| Unsatisfying | 64 (3.0) | 30 (2.7) | 700 (67.1) |
| No children | 771 (35.9) | 461 (41.8) | 34 (3.3) |
| Passive work at T2 | 722 (34.4) | 423 (40.0) | 299 (28.7) |
| High job strain at T2 | 396 (18.9) | 239 (22.6) | 157 (15.1) |
| High psychological demands at T2 | 991 (46.9) | 482 (45.2) | 509 (48.5) |
| Low job control at T2 | 1120 (53.3) | 664 (62.7) | 456 (43.7) |
| Low social support at work at T2 | 1152 (55.2) | 584 (55.6) | 568 (54.8) |
| Effort–reward imbalance at T2 | 497 (24.3) | 255 (24.7) | 242 (23.8) |
| Low reward at T2 | 954 (46.6) | 491 (47.5) | 463 (45.6) |
| Iso-strain at T2 | 275 (13.3) | 156 (15.0) | 119 (11.5) |
| CRP concentration at T3, mg/L, median, interquartile range | 1.15 (0.43;2.65) | 1.34 (0.48;3.20) | 0.99 (0.41;2.15) |
| IL-6 concentration at T3, pg/mL, median, interquartile range | 2.05 (1.38;3.20) | 2.01 (1.35;3.18) | 2.09 (1.41;3.2) |
| Telomere length at T3, ratio T/S median, interquartile range | 0.75 (0.63;0.89) | 0.76 (0.64;0.92) | 0.74 (0.61;0.86) |
| Inflammatory index, mean, min, max | 0.00 (−4.87;5.22) | 0.03 (−4.87;5.22) | −0.03 (−2.95;5.02) |
| MoCA score (out of 30) at T3 | 25.6 ± 2.6 | 25.8 ± 2.6 | 25.4 ± 2.5 |
| Telomere Length a β (95% CI) p-Value | |||
|---|---|---|---|
| Overall | Females | Males | |
| Passive work | −0.04 (−0.08;−0.00) p = 0.0263 | −0.08 (−0.13;−0.03) p = 0.0026 | 0.01 (−0.05;0.06) p = 0.8237 |
| High job strain | 0.01 (−0.04;0.05) p = 0.7839 | 0.01 (−0.05;0.07) p = 0.7218 | 0.00 (−0.07;0.07) p = 0.9921 |
| High psychological demand | 0.02 (−0.02;0.05) p = 0.3770 | 0.04 (−0.01;0.09) p = 0.1103 | −0.01 (−0.06;0.04) p = 0.6403 |
| Low job control | −0.04 (−0.07;0.00) p = 0.0533 | −0.08 (−0.13;−0.02) p = 0.0051 | 0.01 (−0.04;0.05) p = 0.8351 |
| Low social support | −0.01 (−0.04;0.03 p = 0.7626) | −0.01 (−0.06;0.04) p = 0.7497 | −0.00 (−0.05;0.04) p = 0.8895 |
| Effort–reward imbalance | 0.02 (−0.01;0.06) p = 0.2232 | 0.03 (−0.02;0.08) p = 0.2987 | 0.01 (−0.04;0.06) p = 0.6262 |
| Low reward | −0.03 (−0.06;0.01) p = 0.1166 | −0.04 (−0.09;0.01) p = 0.1021 | −0.02 (−0.07;0.03) p = 0.4544 |
| Iso-strain | 0.00 (−0.05;0.05) p = 0.9624 | −0.07 (−0.07;0.06) p = 0.9325 | 0.00 (−0.08;0.08) p = 0.9393 |
| Inflammatory index a β (95% CI) p-value | |||
| Passive work | −0.01 (−0.11;0.10) p = 0.8809 | 0.04 (−0.11;0.19) p = 0.6134 | −0.07 (−0.22;0.08) p = 0.3633 |
| High job strain | 0.07 (−0.06;0.20) p = 0.2588 | 0.02 (−0.15;0.19) p = 0.7898 | 0.18 (−0.02;0.38) p = 0.0759 |
| High psychological demand | −0.01 (−0.11;0.09) p = 0.9126 | −0.03 (−0.18;0.11) p = 0.6610 | 0.04 (−0.09;0.18) p = 0.5506 |
| Low job control | 0.04 (−0.06;0.14) p = 0.4275 | 0.06 (−0.09;0.21) p = 0.4380 | 0.04 (−0.10;0.17) p = 0.6049 |
| Low social support | 0.07 (−0.03;0.017) p = 0.1579 | −0.01 (−0.15;0.14) p = 0.9263 | 0.17 (0.03;0.31) p = 0.0142 |
| Effort–reward imbalance | 0.06 (−0.04;0.16) p = 0.2482 | 0.00 (−0.15;0.15) p = 0.9939 | 0.14 (0.00;0.29) p = 0.0487 |
| Low reward | 0.07 (−0.03;0.17) p = 0.1962 | 0.02 (−0.12;0.16) p = 0.7419 | 0.13 (−0.01;0.27) p = 0.0603 |
| Iso-strain | 0.10 (−0.05;0.25) p = 0.1749 | −0.03 (−0.23;0.17) p = 0.7435 | 0.32 (0.10;0.55) p = 0.0038 |
| Overall β (95% CI) p-Value | Females β (95% CI) p-Value | Males β (95% CI) p-Value | |
|---|---|---|---|
| Telomere length a | 0.26 (-0.00;0.52) p = 0.0527 | 0.10 (−0.27;0.47) p = 0.5923 | 0.50 (0.15;0.86) p = 0.0058 |
| Inflammatory index a | −0.02 (-0.11;0.08) p = 0.7425 | 0.07 (−0.06;0.20) p = 0.2740 | −0.12 (−0.25;0.01) p = 0.0763 |
| OVERALL | Total b β (95% CI) | Direct c β (95% CI) | Indirect Telomere length b β (95% CI) | Indirect Inflammatory index b β (95% CI) |
|---|---|---|---|---|
| Passive work | −0.30 (−0.55;−0.06) p = 0.0163 | −0.29 (−0.54;−0.04) p = 0.0208 | −0.01 (−0.03;0.01) p = 0.2697 | −0.00 (−0.01;0.01) p = 0.9928 |
| High job strain | 0.24 (−0.03;0.50) p = 0.0764 | 0.23 (−0.04;0.49) p = 0.0911 | 0.00 (−0.01;0.02) p = 0.8171 | 0.00 (−0.01;0.02) p = 0.9236 |
| High psychological demand | 0.23 (0.03;0.44) p = 0.0280 | 0.23 (0.02;0.43) p = 0.0348 | 0.00 (−0.01;0.02) p = 0.5107 | −0.00 (−0.01;0.01) p = 0.9837 |
| Low job control | −0.13 (−0.36;0.10) p = 0.2571 | −0.13 (−0.36;0.10) p = 0.2726 | −0.01 (−0.02;0.01) p = 0.2422 | 0.00 (−0.01;0.02) p = 0.9497 |
| Low social support | −0.15 (−0.37;0.08) p = 0.2051 | −0.16 (−0.38;0.07) p = 0.1739 | −0.00 (−0.01;0.01) p = 0.7874 | 0.00 (−0.01;0.01) p = 0.8831 |
| Effort–reward imbalance | 0.12 (−0.10;0.34) p = 0.2904 | 0.11 (−0.11;0.34) p = 0.3247 | 0.01 (−0.01;0.02) p = 0.3969 | 0.00 (−0.01;0.01) p = 0.9483 |
| Low reward | −0.21 (−0.44;0.02) p = 0.0708 | −0.20 (−0.43;0.03) p = 0.0828 | −0.01 (−0.02;0.01) p = 0.2945 | 0.00 (−0.01;0.01) p = 0.8886 |
| Iso-strain | 0.19 (−0.12;0.51) p = 0.2343 | 0.19 (−0.13;0.50) p = 0.2529 | 0.00 (−0.01;0.02) p = 0.9705 | 0.00 (−0.02;0.02) p = 0.8834 |
| FEMALES | ||||
| Passive work | −0.22 (−0.54;0.10) p = 0.1833 | −0.21 (−0.54;0.11) p = 0.1943 | −0.01 (−0.06;0.04) p = 0.6926 | 0.00 (−0.02;0.03) p = 0.8117 |
| High job strain | 0.34 (0.01;0.68) p = 0.0449 | 0.34 (0.01;0.68) p = 0.0456 | 0.00 (−0.02;0.02) p = 0.8929 | 0.00 (−0.03;0.03) p = 0.8929 |
| High psychological demand | 0.11 (−0.19;0.40) p = 0.4763 | 0.10 (−0.20;0.39) p = 0.5100 | 0.01 (−0.02;0.04) p = 0.6855 | −0.00 (−0.03;0.02) p = 0.8380 |
| Low job control | 0.04 (−0.30;0.36) p = 0.8259 | 0.04 (−0.29;0.37) p = 0.8079 | −0.01 (−0.05;0.03) p = 0.5501 | 0.00 (−0.02;0.03) p = 0.7316 |
| Low social support | −0.02 (−0.33;0.29) p = 0.8968 | −0.03 (−0.35;0.28) p = 0.8378 | −0.00 (−0.02;0.01) p = 0.8465 | −0.00 (−0.03;0.03) p = 0.9883 |
| Effort–reward imbalance | 0.05 (−0.25;0.35) p = 0.7535 | 0.04 (−0.26;0.35) p = 0.7879 | 0.00 (−0.02;0.02) p = 0.6873 | 0.00 (−0.02;0.02) p = 0.9920 |
| Low reward | −0.09 (−0.39;0.21) p = 0.5472 | −0.10 (−0.40;0.21) p = 0.5367 | −0.01 (−0.16;0.14) p = 0.9303 | 0.00 (−0.01;0.01) p = 0.9788 |
| Iso-strain | 0.30 (−0.10;0.71) p = 0.1399 | 0.31 (−0.10;0.72) p = 0.1395 | −0.00 (−0.02;0.02) p = 0.9927 | −0.00 (−0.15;0.14) p = 0.9927 |
| MALES | ||||
| Passive work | −0.40 (−0.78;−0.02) p = 0.0368 | −0.40 (−0.78;−0.03) p = 0.0366 | 0.00 (−0.02;0.03) p = 0.8128 | 0.01 (−0.02;0.03) p = 0.5592 |
| High job strain | 0.11 (−0.29;0.51) p = 0.5883 | 0.12 (−0.29;0.52) p = 0.5630 | 0.00 (−0.03;0.03) p = 0.9985 | −0.02 (−0.06;0.03) p = 0.4314 |
| High psychological demand | 0.38 (0.09;0.67) p = 0.0104 | 0.39 (0.09;0.68) p = 0.0095 | −0.00 (−0.03;0.02) p = 0.7092 | −0.00 (−0.02;0.01) p = 0.6562 |
| Low job control | −0.28 (−0.61;0.05) p = 0.0981 | −0.27 (−0.60;0.05) p = 0.1020 | 0.00 (−0.02;0.03) p = 0.8299 | −0.00 (−0.02;0.01) p = 0.7254 |
| Low social support | −0.23 (−0.55;0.09) p = 0.1661 | −0.22 (−0.55;0.10) p = 0.9560 | 0.00 (−0.02;0.02) p = 0.9560 | −0.01 (−0.05;0.02) p = 0.4338 |
| Effort–reward imbalance | 0.17 (−0.14;0.49) p = 0.2773 | 0.18 (−0.13;0.50) p = 0.2561 | 0.01 (−0.02;0.03) p = 0.6217 | −0.01 (−0.04;0.02) p = 0.3853 |
| Low reward | −0.35 (−0.69;−0.01) p = 0.0459 | −0.32 (−0.67;0.03) p = 0.0702 | −0.01 (−0.03;0.02) p = 0.6116 | −0.01 (−0.04;0.02) p = 0.4543 |
| Iso-strain | 0.06 (−0.42;0.53) p = 0.8142 | 0.08 (−0.41;0.57) p = 0.7491 | 0.00 (−0.04;0.04) p = 0.8857 | −0.03 (−0.10;0.04) p = 0.3536 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duchaine, C.S.; Brisson, C.; Diorio, C.; Talbot, D.; Maunsell, E.; Carmichael, P.-H.; Giguère, Y.; Gilbert-Ouimet, M.; Trudel, X.; Ndjaboué, R.; et al. Work-Related Psychosocial Factors and Global Cognitive Function: Are Telomere Length and Low-Grade Inflammation Potential Mediators of This Association? Int. J. Environ. Res. Public Health 2023, 20, 4929. https://doi.org/10.3390/ijerph20064929
Duchaine CS, Brisson C, Diorio C, Talbot D, Maunsell E, Carmichael P-H, Giguère Y, Gilbert-Ouimet M, Trudel X, Ndjaboué R, et al. Work-Related Psychosocial Factors and Global Cognitive Function: Are Telomere Length and Low-Grade Inflammation Potential Mediators of This Association? International Journal of Environmental Research and Public Health. 2023; 20(6):4929. https://doi.org/10.3390/ijerph20064929
Chicago/Turabian StyleDuchaine, Caroline S., Chantal Brisson, Caroline Diorio, Denis Talbot, Elizabeth Maunsell, Pierre-Hugues Carmichael, Yves Giguère, Mahée Gilbert-Ouimet, Xavier Trudel, Ruth Ndjaboué, and et al. 2023. "Work-Related Psychosocial Factors and Global Cognitive Function: Are Telomere Length and Low-Grade Inflammation Potential Mediators of This Association?" International Journal of Environmental Research and Public Health 20, no. 6: 4929. https://doi.org/10.3390/ijerph20064929