Clinical and Molecular Comparative Study of Colorectal Cancer Based on Age-of-Onset and Tumor Location: Two Main Criteria for Subclassifying Colorectal Cancer

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Results
2.1. EOCRC: Global Group Features and Comparative Analysis According to Colon Location
2.1.1. Clinicopathological and Familial Features
2.1.2. Molecular Features
2.2. LOCRC: Global Group Features and Comparative Analysis According to Colon Location
2.2.1. Clinico-Pathological and Familial Features
2.2.2. Molecular Features
2.3. Right Colon Cancers: Comparison between EOCC and LOCC
2.3.1. Clinico-Pathological and Familial Features
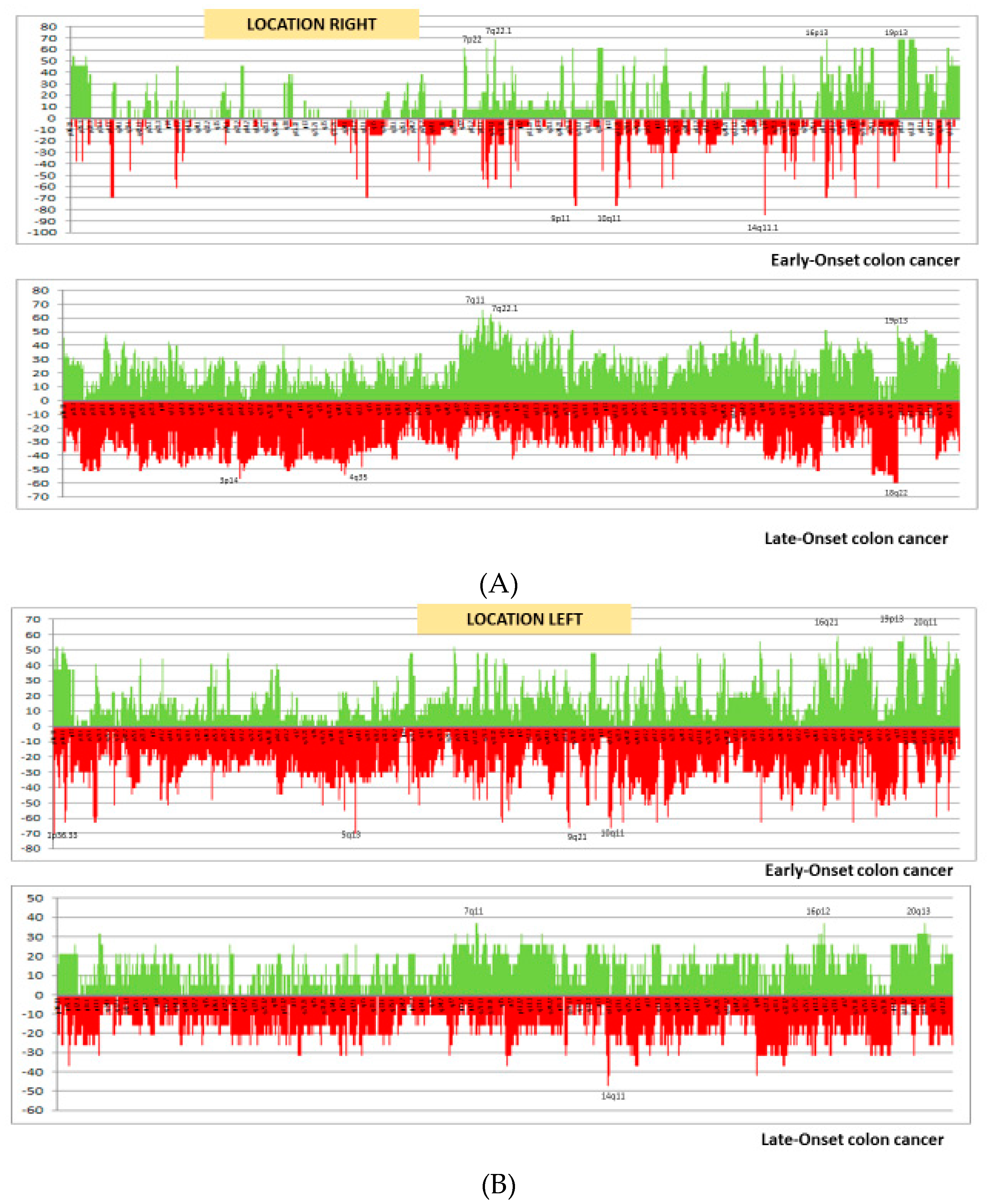
2.3.2. Molecular Features
2.4. Left Colon Cancers: Comparison between EOCC and LOCC
2.4.1. Clinico-Pathological and Familial Features
2.4.2. Molecular Features
2.5. Rectal Cancers: Comparison between EORC and LORC
2.5.1. Clinicopathological and Familial Features
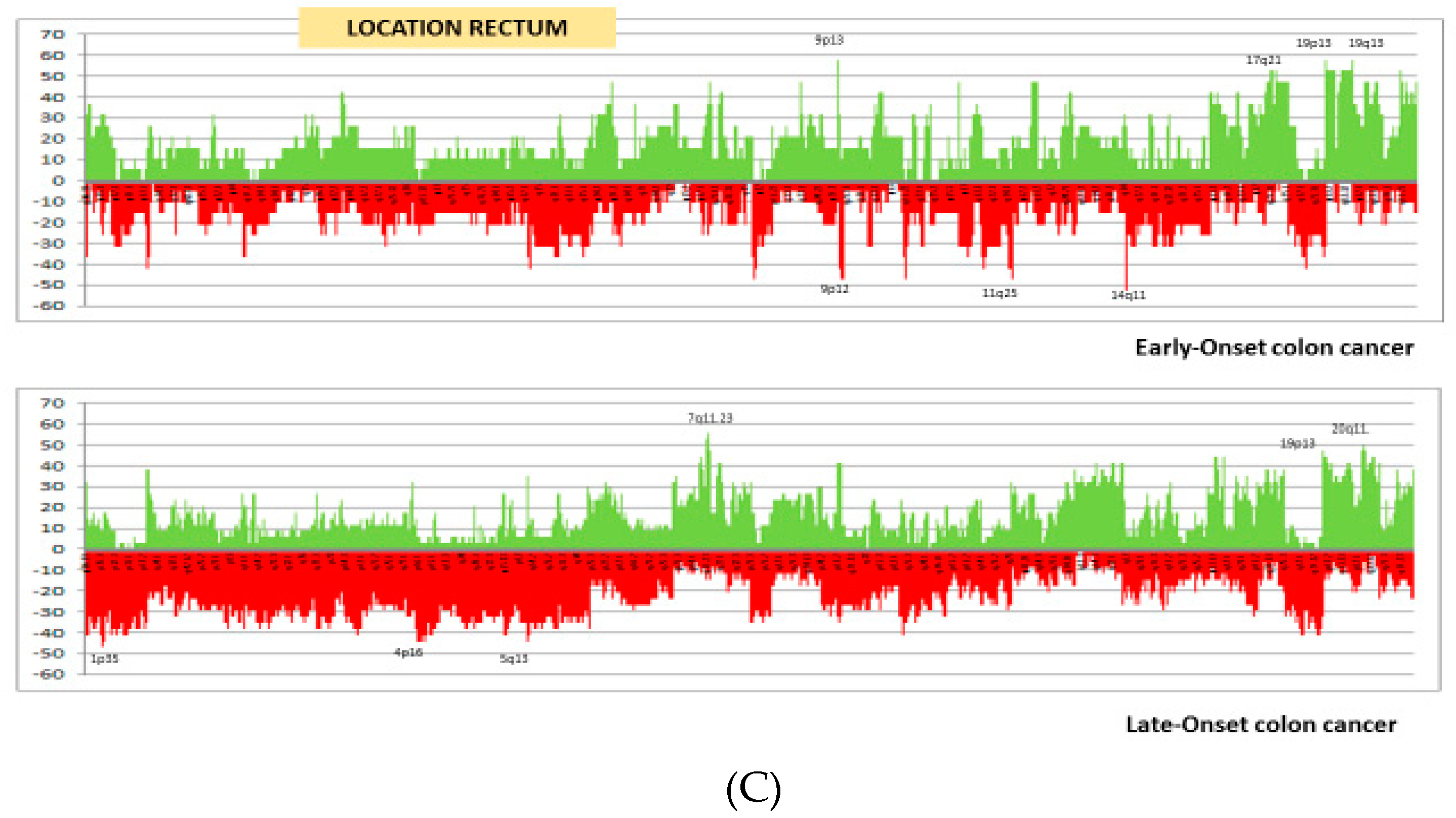
2.5.2. Molecular Features
3. Discussion
4. Materials and Methods
4.1. Families, Samples and Data Collection
4.2. Microsatellite Instability and Mutational Analysis
4.3. Analysis of CpG Island Methylation Phenotype Panel
4.4. Molecular Classification
4.5. Chromosomal Instability. Array Comparative Genomic Hybridization (aCGH)
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| aCGH | array of Comparative Genomic Hybridization |
| CIMP | CpG Island Methylator Phenotype |
| CIN | Chromosomal Instability |
| CRC | Colorectal cancer |
| CMS | Consensus Molecular subtype |
| CNA | Copy Number Alterations |
| DFS | Disease-Free survival |
| EOCC | Early-onset colon cancer |
| EOCRC | Early-onset colorectal cancer |
| EORC | Early-onset rectal cancer |
| GEO | Gene Expression Omnibus |
| LOCC | Late-onset colon cancer |
| LOCRC | Late-onset colorectal cancer |
| LORC | Late-onset rectal cancer |
| LS | Lynch syndrome |
| MCRC | Metachronous colorectal cancer |
| MMR | Mismatch Repair |
| MSI | Microsatellite instability |
| MSS | Microsatellite stability |
| OS | Overall survival |
| SCNA | somatic copy number alterations |
| SCRC | Synchronous colorectal cancer |
| SD | Standard Deviation |
References
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer Oxf. Engl. 1990 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Ahnen, D.J.; Wade, S.W.; Jones, W.F.; Sifri, R.; Mendoza Silveiras, J.; Greenamyer, J.; Guiffre, S.; Axilbund, J.; Spiegel, A.; You, Y.N. The increasing incidence of young-onset colorectal cancer: A call to action. Mayo Clin. Proc. 2014, 89, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Perea, J.; Alvaro, E.; Rodríguez, Y.; Gravalos, C.; Sánchez-Tomé, E.; Rivera, B.; Colina, F.; Carbonell, P.; González-Sarmiento, R.; Hidalgo, M.; et al. Approach to early-onset colorectal cancer: Clinicopathological, familial, molecular and immunohistochemical characteristics. World J. Gastroenterol. 2010, 16, 3697–3703. [Google Scholar] [CrossRef]
- Perea, J.; Rueda, D.; Canal, A.; Rodríguez, Y.; Álvaro, E.; Osorio, I.; Alegre, C.; Rivera, B.; Martínez, J.; Benítez, J.; et al. Age at onset should be a major criterion for subclassification of colorectal cancer. J. Mol. Diagn. 2014, 16, 116–126. [Google Scholar] [CrossRef]
- Boardman, L.A.; Johnson, R.A.; Viker, K.B.; Hafner, K.A.; Jenkins, R.B.; Riegert-Johnson, D.L.; Smyrk, T.C.; Litzelman, K.; Seo, S.; Gangnon, R.E.; et al. Correlation of chromosomal instability, telomere length and telomere maintenance in microsatellite stable rectal cancer: A molecular subclass of rectal cancer. PLoS ONE 2013, 8, e80015. [Google Scholar] [CrossRef] [PubMed]
- Iacopetta, B. Are there two sides to colorectal cancer? Int. J. Cancer 2002, 101, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Glebov, O.K.; Rodriguez, L.M.; Nakahara, K.; Jenkins, J.; Cliatt, J.; Humbyrd, C.-J.; DeNobile, J.; Soballe, P.; Simon, R.; Wright, G.; et al. Distinguishing right from left colon by the pattern of gene expression. Cancer Epidemiol. Biomark. Prev. 2003, 12, 755–762. [Google Scholar]
- Snaebjornsson, P.; Jonasson, L.; Jonsson, T.; Möller, P.H.; Theodors, A.; Jonasson, J.G. Colon cancer in Iceland—A nationwide comparative study on various pathology parameters with respect to right and left tumor location and patients age. Int. J. Cancer 2010, 127, 2645–2653. [Google Scholar] [CrossRef]
- Perea, J.; Cano, J.M.; Rueda, D.; García, J.L.; Inglada, L.; Osorio, I.; Arriba, M.; Pérez, J.; Gaspar, M.; Fernández-Miguel, T.; et al. Classifying early-onset colorectal cancer according to tumor location: New potential subcategories to explore. Am. J. Cancer Res. 2015, 5, 2308–2313. [Google Scholar]
- Arriba, M.; García, J.L.; Inglada-Pérez, L.; Rueda, D.; Osorio, I.; Rodríguez, Y.; Álvaro, E.; Sánchez, R.; Fernández, T.; Pérez, J.; et al. DNA copy number profiling reveals different patterns of chromosomal instability within colorectal cancer according to the age of onset. Mol. Carcinog. 2016, 55, 705–716. [Google Scholar] [CrossRef]
- Brandariz, L.; Arriba, M.; García, J.L.; Cano, J.M.; Rueda, D.; Rubio, E.; Rodríguez, Y.; Pérez, J.; Vivas, A.; Sánchez, C.; et al. Differential clinicopathological and molecular features within late-onset colorectal cancer according to tumor location. Oncotarget 2018, 9, 15302–15311. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Goel, A. Molecular classification and correlates in colorectal cancer. J. Mol. Diagn. 2008, 10, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Berg, M.; Agesen, T.H.; Thiis-Evensen, E.; INFAC-Study Group; Merok, M.A.; Teixeira, M.R.; Vatn, M.H.; Nesbakken, A.; Skotheim, R.I.; Lothe, R.A. Distinct high resolution genome profiles of early onset and late onset colorectal cancer integrated with gene expression data identify candidate susceptibility loci. Mol. Cancer 2010, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Ishizaka, Y.; Itoh, F.; Tahira, T.; Ikeda, I.; Sugimura, T.; Tucker, J.; Fertitta, A.; Carrano, A.V.; Nagao, M. Human ret proto-oncogene mapped to chromosome 10q11.2. Oncogene 1989, 4, 1519–1521. [Google Scholar] [PubMed]
- Xu, X.; Li, J.; Sun, X.; Guo, Y.; Chu, D.; Wei, L.; Li, X.; Yang, G.; Liu, X.; Yao, L.; et al. Tumor suppressor NDRG2 inhibits glycolysis and glutaminolysis in colorectal cancer cells by repressing c-Myc expression. Oncotarget 2015, 6, 26161–26176. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Qu, X.; Ma, Y.; Zheng, J.; Chu, D.; Liu, B.; Li, X.; Wang, M.; Xu, C.; Liu, N.; et al. Tumor suppressor NDRG2 tips the balance of oncogenic TGF-β via EMT inhibition in colorectal cancer. Oncogenesis 2014, 3, e86. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.N.; Kim, S.J.; Kim, E.-R.; Chang, D.K.; Kim, Y.-H. Epigenetic silencing of NDRG2 promotes colorectal cancer proliferation and invasion. J. Gastroenterol. Hepatol. 2016, 31, 164–171. [Google Scholar] [CrossRef]
- Schaid, D.J.; Stanford, J.L.; McDonnell, S.K.; Suuriniemi, M.; McIntosh, L.; Karyadi, D.M.; Carlson, E.E.; Deutsch, K.; Janer, M.; Hood, L.; et al. Genome-wide linkage scan of prostate cancer Gleason score and confirmation of chromosome 19q. Hum. Genet. 2007, 121, 729–735. [Google Scholar] [CrossRef]
- Blaumueller, C.M.; Qi, H.; Zagouras, P.; Artavanis-Tsakonas, S. Intracellular cleavage of Notch leads to a heterodimeric receptor on the plasma membrane. Cell 1997, 90, 281–291. [Google Scholar] [CrossRef]
- Ding, C.; Luo, J.; Li, L.; Li, S.; Yang, L.; Pan, H.; Liu, Q.; Qin, H.; Chen, C.; Feng, J. Gab2 facilitates epithelial-to-mesenchymal transition via the MEK/ERK/MMP signaling in colorectal cancer. J. Exp. Clin. Cancer Res. 2016, 35, 5. [Google Scholar] [CrossRef]
- Zhou, H.-T.; Shi, Z.-Z.; Zhou, Z.-X.; Jiang, Y.-Y.; Hao, J.-J.; Zhang, T.-T.; Shi, F.; Xu, X.; Wang, M.-R.; Zhang, Y. Genomic changes in rectal adenocarcinoma associated with liver metastasis. Cancer Biomark. Sect. Dis. Markers 2013, 13, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.; Kopetz, S.; Tie, J.; Gibbs, P.; Jiang, Z.-Q.; Lieu, C.H.; Agarwal, A.; Maru, D.M.; Sieber, O.; Desai, J. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer 2011, 117, 4623–4632. [Google Scholar] [CrossRef] [PubMed]
- Gavin, P.G.; Colangelo, L.H.; Fumagalli, D.; Tanaka, N.; Remillard, M.Y.; Yothers, G.; Kim, C.; Taniyama, Y.; Kim, S.I.; Choi, H.J.; et al. Mutation profiling and microsatellite instability in stage II and III colon cancer: An assessment of their prognostic and oxaliplatin predictive value. Clin. Cancer Res. 2012, 18, 6531–6541. [Google Scholar] [CrossRef] [PubMed]
- Popovici, V.; Budinska, E.; Bosman, F.T.; Tejpar, S.; Roth, A.D.; Delorenzi, M. Context-dependent interpretation of the prognostic value of BRAF and KRAS mutations in colorectal cancer. BMC Cancer 2013, 13, 439. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.E.; Hu, C.-Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.G.; Ahnen, D.J. Colorectal Cancer in the Young. Curr. Gastroenterol. Rep. 2018, 20, 15. [Google Scholar] [CrossRef] [PubMed]
- Tamas, K.; Walenkamp, A.M.; de Vries, E.G.; van Vugt, M.A.; Beets-Tan, R.G.; van Etten, B.; de Groot, D.J.; Hospers, G.A. Rectal and colon cancer: Not just a different anatomic site. Cancer Treat. Rev. 2015, 41, 671–679. [Google Scholar] [CrossRef]
- Al-Barrak, J.; Gill, S. Presentation and outcomes of patients aged 30 years and younger with colorectal cancer: A 20-year retrospective review. Med. Oncol. Northwood Lond. Engl. 2011, 28, 1058–1061. [Google Scholar] [CrossRef]
- Fazeli, M.S.; Adel, M.G.; Lebaschi, A.H. Colorectal carcinoma: A retrospective, descriptive study of age, gender, subsite, stage, and differentiation in Iran from 1995 to 2001 as observed in Tehran University. Dis. Colon Rectum 2007, 50, 990–995. [Google Scholar] [CrossRef]
- Campos, F.G. Colorectal cancer in young adults: A difficult challenge. World J. Gastroenterol. 2017, 23, 5041–5044. [Google Scholar] [CrossRef] [PubMed]
- Ziogas, A.; Anton-Culver, H. Validation of family history data in cancer family registries. Am. J. Prev. Med. 2003, 24, 190–198. [Google Scholar] [CrossRef]
- Aaltonen, L.A.; Peltomäki, P.; Mecklin, J.P.; Järvinen, H.; Jass, J.R.; Green, J.S.; Lynch, H.T.; Watson, P.; Tallqvist, G.; Juhola, M. Replication errors in benign and malignant tumors from hereditary nonpolyposis colorectal cancer patients. Cancer Res. 1994, 54, 1645–1648. [Google Scholar] [PubMed]
- Boland, C.R.; Thibodeau, S.N.; Hamilton, S.R.; Sidransky, D.; Eshleman, J.R.; Burt, R.W.; Meltzer, S.J.; Rodriguez-Bigas, M.A.; Fodde, R.; Ranzani, G.N.; et al. A National Cancer Institute Workshop on Microsatellite Instability for cancer detection and familial predisposition: Development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998, 58, 5248–5257. [Google Scholar] [PubMed]
- Perea, J.; Rodríguez, Y.; Rueda, D.; Marín, J.C.; Díaz-Tasende, J.; Álvaro, E.; Alegre, C.; Osorio, I.; Colina, F.; Lomas, M.; et al. Early-onset colorectal cancer is an easy and effective tool to identify retrospectively Lynch syndrome. Ann. Surg. Oncol. 2011, 18, 3285–3291. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2012; ISBN 3-900051-07-0. Available online: http://www.R-project.org/ (accessed on 1 April 2014).



{kind=link}
{kind=link}
| RIGHT COLON | n/N EOCRC | EARLY-ONSET n/Right-sided EOCC (%) | n/N LOCRC | LATE-ONSET n/ Right-sided LOCC (%) | p(χ2) |
|---|---|---|---|---|---|
| Number of cases (%) | 20/82 | 24% | 38/97 | 39% | |
| Age of Onset (mean (SD), years) 1 | - | 39.1 (6) | - | 79.08 (5) | NS |
| Gender | 10/82 | Female 10/20 (50%) | 25/97 | Female 25/38 (66%) | NS |
| Grade of tumor differentiation (%) 2 | 5/82 | Poor 5/20 (25%) | 24/97 | Medium 24/38 (63%) | NS |
| Mucosecretion2 | 7/82 | 7/20 (35%) | 13/97 | 13/38 (34%) | NS |
| Presence of “Signet-ring” cells 2 | 0/82 | 0/20 (0%) | 0/97 | 0/38 (0%) | NS |
| TNM (UICC) Stage (%) | 16/82 | I-II: 16/20 (80%) | 30/97 | II-III: 30/38 (79%) | NS |
| Associated Polyps | 7/82 | 14/20 (70%) | 19/97 | 24/38 (63%) | NS |
| Mean number of associated polyps 1 | - | 3 | - | 1.8 | 0.021 |
| Type of associated polyps (%) | 10/82 | Mixed: 10/20 (50%) | 21/97 | Adenomatous: 21/38 (54%) | NS |
| S- and/or MCRC | 4/82 | 4/20 (20%) | 9/97 | 9/38 (24%) | NS |
| Amsterdam criteria for LS | 8/82 | 8/20 (40%) | 1/97 | 1/38 (3%) | <0.001 |
| Familial aggregation for LS-related neoplasms | 7/82 | 7/20 (35%) | 6/97 | 6/38 (16%) | 0.008 |
| Familial aggregation for LS-unrelated neoplasms | 1/82 | 1/20 (5%) | 1/97 | 1/38 (3%) | NS |
| Sporadic cases | 4/82 | 4/20 (20%) | 28/97 | 28/38 (74%) | <0.001 |
| Disease-Free Survival (mean; months) 1 | - | 72.4 | - | 20.16 | 0.002 |
| Global Survival (mean; months) 1 | - | 81.06 | - | 45.94 | 0.003 |
| MSI | 6/82 | 6/20 (30%) | 7/38 | 7/38 (18%) | NS |
| MMR genes germline mutations | 6/82 | 6/20 (30%) | 5/97 | 5/ 38 (13%) | NS |
| BRAF mutation | 0/82 | 0/82 (0%) | 5/97 | 5/38 (13%) | NS |
| CIMP Classification (%) 2 | 0.025 | ||||
| High | 8/78 | 8/16 (50%) | 7/90 | 7/36 (20%) | |
| Low | 6/78 | 6/16 (37.5%) | 12/90 | 12/36 (33%) | |
| 0 | 2/78 | 2/16 (12.5%) | 17/90 | 17/36 (47%) | |
| Molecular Classification (%) 2 | |||||
| MSI-CIMP-High | 3/82 | 3/16 (19%) | 5/90 | 5/36 (14%) | 0.019 |
| MSI-CIMP0 | 2/82 | 2/16 (12.5%) | 2/90 | 2/36 (5%) | |
| MSS-CIMP-High | 5/82 | 5/16 (31%) | 2/90 | 2/36 (5%) | |
| MSS-CIMP0 | 6/82 | 6/16 (37.5%) | 27/90 | 27/36 (75%) | |
| Genomic instability1 | |||||
| GII Gain | 0.144296 | 0.183649 | NS | ||
| GII Loss | 0.058762 | 0.249820 | 0.003 | ||
| GII Normal | 0.796933 | 0.566522 | 0.03 | ||
| Mean Gained Chromosomes | 1.38 | 1.80 | NS | ||
| Mean Lost Chromosomes | 0.08 | 2.20 | 0.18 |
| LEFT COLON | n/N EOCRC | EARLY-ONSET n/Left colon EOCC (%) | n/N LOCR | LATE-ONSET n/ Left colon EOCC (%) | p(χ2) |
|---|---|---|---|---|---|
| Number of cases (%) | 35/82 | 43% | 22/97 | 22.7% | |
| Age of Onset (mean (SD), years) 1 | - | 39.3 (4.2) | - | 74.86 (5) | NS |
| Gender (%) | 22/82 | Male 22/35 (63%) | 14/97 | Male 14/22 (64%) | NS |
| Grade of tumor differentiation (%) 2 | 24/82 | Medium 24/35 (68.5%) | 17/97 | Medium 17/22 (77%) | NS |
| Mucosecretion 2 | 8/82 | 8/24 (33%) | 2/97 | 2/22 (9.1%) | NS |
| Presence of “Signet-ring” cells 2 | 2/82 | 2/24 (8%) | 0/97 | 0/22 (0%) | NS |
| TNM Stage (%) | 27/82 | I/II 27/35 (77%) | 18/97 | II-III 18/22 (82%) | 0.003 |
| Associated polyps | 21/82 | 21/35 (60%) | 13/97 | 13/22 (59.1%) | NS |
| Mean number of associated polyps 1 | - | 1.6 | - | 5.41 | <0.001 |
| Type of associated polyps (%) | 10/82 | Adenomatous 10/21 (48%) | 7/97 | Adenomatous 7/13 (54%) | NS |
| S- and/or MCRC | 0/82 | 0/35 | 8/97 | 8/22 (36%) | <0.001 |
| Amsterdam criteria for LS | 6/82 | 6/35 (17%) | 0/97 | 0/22 (0%) | NS |
| Familial aggregation for LS-related neoplasms | 6/82 | 6/35 (17%) | 6/97 | 6/22 (27%) | NS |
| Familial aggregation for LS-unrelated neoplasms | 6/82 | 6/35 (17%) | 2/97 | 2/22 (9%) | NS |
| Sporadic cases | 17/82 | 17/35 (48%) | 12/97 | 12/22 (55%) | NS |
| Disease-Free Survival (mean; months) 1 | - | 48.70 | - | 31.68 | NS |
| Global Survival (mean; months) 1 | - | 76.67 | - | 96.95 | NS |
| MSI | 6/82 | 6/35 (17%) | 2/97 | 2/22 (9%) | NS |
| MMR gene germline mutations | 4/82 | 4/35 (11%) | 0/97 | 0/22 (0%) | NS |
| BRAF mutation | 1/82 | 1/35 (3%) | 1/97 | 1/22 (4.5%) | NS |
| CIMP Classification (%) 2 | |||||
| High | 3/78 | 3/31 (10%) | 3/96 | 3/21 (14%) | NS |
| Low | 14/78 | 14/31 (45%) | 4/96 | 4/21 (19%) | |
| 0 | 14/78 | 14/31 (45%) | 14/96 | 14/21 (67%) | |
| Molecular Classification (%) 2 | |||||
| MSI-CIMP-High | 1/78 | 1/31 (3%) | 2/96 | 2/21 (9.5%) | NS |
| MSI-CIMP0 | 4/78 | 4/31 (13%) | 0/96 | 0/21 (0%) | |
| MSS-CIMP-High | 2/78 | 2/31 (6.5%) | 1/96 | 1/21 (5%) | |
| MSS-CIMP0 | 24/78 | 24/31 (77.5%) | 18/96 | 18/21 (86%) | |
| Genomic instability 1 | |||||
| GII Gain | 0.1462817 | 0.101056 | NS | ||
| GII Loss | 0.2294307 | 0.114539 | 0.06 | ||
| GII Normal | 0.6247970 | 0.784362 | NS | ||
| Mean Gained Chromosomes | 2.00 | 0.78 | 0.03 | ||
| Mean Lost Chromosomes | 1.93 | 0.61 | 0.03 |
| RECTUM | n/N EOCRC | EARLY-ONSET n/ EORC (%) | n/N LOCRC | LATE-ONSET n/ LORC (%) | p(χ2) |
|---|---|---|---|---|---|
| Number of cases (%) | 27/82 | 33% | 37/97 | 38.1% | |
| Age of Onset (mean (SD), years) 1 | - | 40.2 (5) | - | 78.54 (5) | NS |
| Gender (%) | 17/82 | Male 17/27 (63%) | 23/97 | Male 23/37 (62%) | NS |
| Grade of tumoral differentiation (%)2 | 18/82 | Medium 18/27 (68%) | 29/97 | Medium 29/37 (79%) | NS |
| Mucosecretion2 | 5/75 | 5/20 (25%) | 4/97 | 4/34 (11.8%) | NS |
| Presence of Signet-ring cells2 | 2/75 | 2/20 (10%) | 0/97 | 0/37 (0%) | NS |
| TNM Stage (%) | 10/82 | IV 10/27 (37%) | 18/97 | II 18/37 (49%) | 0.002 |
| Associated Polyps | 11/82 | 11/27 (41%) | 25/97 | 25/37 (68%) | 0.04 |
| Mean number of associated polyps1 | - | 1.22 | - | 2.00 | NS |
| Type of associated polyps (%) | 7/66 | Adenomatous: 7/11 (64%) | 18/85 | Adenomatous: 18/25 (72%) | NS |
| S- and/or MCRC | 0/82 | 0/27 (0) | 4/97 | 4/37 (11%) | NS |
| Amsterdam criteria for LS | 1/82 | 1/27 (4%) | 0/97 | 0/37 (0) | NS |
| Familial aggregation for LS-related neoplasms | 14/82 | 14/ 27 (52%) | 0/97 | 0/37 (0) | <0.001 |
| Familial aggregation for LS-unrelated neoplasms | 2/82 | 2/27 (7%) | 3/97 | 3/37 (8%) | NS |
| Sporadic Cases | 10/82 | 10/27 (37%) | 34/97 | 34/37 (92%) | <0.001 |
| Disease-Free Survival (mean; months)1 | - | 35.85 | - | 16.25 | <0.001 |
| Global Survival (mean; months)1 | - | 64.79 | - | 31.67 | <0.001 |
| Microsatellite stability: | 0/82 | 0/27 | 0/97 | 0/37 | NS |
| MMR gene germline mutations | 0/82 | 0/27 | 0/97 | 0/27 | NS |
| BRAF mutation | 0/82 | 0/27 | 1/97 | 1/37 (2.7%) | NS |
| CIMP Classification (%)2 | NS | ||||
| High | 2/76 | 2/21 (10%) | 12/93 | 12/33 (36%) | |
| Low | 8/76 | 8/21 (38%) | 9/93 | 8/33 (24%) | |
| 0 | 11/76 | 11/21 (52%) | 13/93 | 13/33 (40%) | |
| Molecular Classification (%)2 | 0.035 | ||||
| MSI-CIMP-High | 0/76 | 0/21 | 0/93 | 0/33 | |
| MSI-CIMP0 | 0/76 | 0/21 | 0/93 | 0/33 | |
| MSS-CIMP-High | 2/76 | 2/21 (9%) | 12/93 | 12/33 (36%) | |
| MSS-CIMP0 | 19/76 | 19/21 (90.5%) | 21/93 | 21/33 (64%) | |
| Genomic instability 1 | |||||
| GII Gain | 0.1627359 | 0.133332 | NS | ||
| GII Loss | 0.1441914 | 0.194276 | NS | ||
| GII Normal | 0.6930648 | 0.672383 | NS | ||
| Mean Gained Chromosomes | 2.37 | 1.67 | NS | ||
| Mean Lost Chromosomes | 1.26 | 2.09 | NS |
| Chromosomal Segment | RIGHT-SIDED | LEFT-SIDED COLON | RECTUM | |||||
| EO (n = 13) | LO (n = 35) | EO (n = 27) | LO (n = 19) | EO (n =2 0) | LO (n = 32) | |||
| % | % | % | % | % | % | |||
| chr1 | p32.3-22.2 | 0 | 51 | |||||
| chr1 | p21.3-11.2 | 0 | 51 | |||||
| chr2 | p25.2 | 0 | 51 | RIGHT COLON | ||||
| chr2 | p11.2 | 54 | 20 | |||||
| chr10 | q11.21-11.22 | 70 | 23 | |||||
| chr14 | q11.1-11.2 | 85 | 37 | |||||
| chr16 | p13.12-13.11 | 54 | 11 | |||||
| chr17 | p11.2 | 62 | 29 | |||||
| chr18 | p11.32-11.21 | 0 | 54 | |||||
| chr18 | q21.1-21.1 | 8 | 51 | |||||
| chr18 | q21.31-21.33 | 8 | 54 | |||||
| chr7 | q11.22-21.11 | 15 | 63 | |||||
| chr7 | q22.1-31.33 | 15 | 57 | |||||
| chr7 | p12.2-11.2 | 15 | 54 | |||||
| chr7 | q11.21 | 15 | 54 | |||||
| chr9 | q12-13 | 0 | 51 | |||||
| chr9 | q33.3 | 62 | 29 | |||||
| chr9 | q34.12-34.13 | 62 | 29 | |||||
| chr13 | q11 | 8 | 51 | |||||
| chr21 | q22.3 | 62 | 26 | |||||
| chr1 | p12-q21.1 | 63 | 10 | LEFT COLON | ||||
| chr5 | q13.1-13.2 | 67 | 16 | |||||
| chr9 | p12-q24.22 | 59 | 21 | |||||
| chr9 | q31.3-33.1 | 52 | 16 | |||||
| chr11 | p11.12-q12.1 | 63 | 21 | |||||
| chr11 | q14.1-14.3 | 59 | 21 | |||||
| chr15 | p11.1-q11.2 | 0 | 26 | |||||
| chr19 | p13.12-12 | 59 | 26 | |||||
| chr1 | p36.32-36.13 | 5 | 41 | RECTUM | ||||
| chr1 | p36.23-36.22 | 37 | 12 | |||||
| chr3 | p21.31-21.1 | 42 | 32 | |||||
| chr5 | q13.2 | 5 | 53 | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvaro, E.; Cano, J.M.; García, J.L.; Brandáriz, L.; Olmedillas-López, S.; Arriba, M.; Rueda, D.; Rodríguez, Y.; Cañete, Á.; Arribas, J.; et al. Clinical and Molecular Comparative Study of Colorectal Cancer Based on Age-of-Onset and Tumor Location: Two Main Criteria for Subclassifying Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 968. https://doi.org/10.3390/ijms20040968
Álvaro E, Cano JM, García JL, Brandáriz L, Olmedillas-López S, Arriba M, Rueda D, Rodríguez Y, Cañete Á, Arribas J, et al. Clinical and Molecular Comparative Study of Colorectal Cancer Based on Age-of-Onset and Tumor Location: Two Main Criteria for Subclassifying Colorectal Cancer. International Journal of Molecular Sciences. 2019; 20(4):968. https://doi.org/10.3390/ijms20040968
Chicago/Turabian StyleÁlvaro, Edurne, Juana M. Cano, Juan L. García, Lorena Brandáriz, Susana Olmedillas-López, María Arriba, Daniel Rueda, Yolanda Rodríguez, Ángel Cañete, Julia Arribas, and et al. 2019. "Clinical and Molecular Comparative Study of Colorectal Cancer Based on Age-of-Onset and Tumor Location: Two Main Criteria for Subclassifying Colorectal Cancer" International Journal of Molecular Sciences 20, no. 4: 968. https://doi.org/10.3390/ijms20040968