3.2. Synthesis and Characterization of the Dendronized Hyperbranched Polymer DHP-bMPA
The
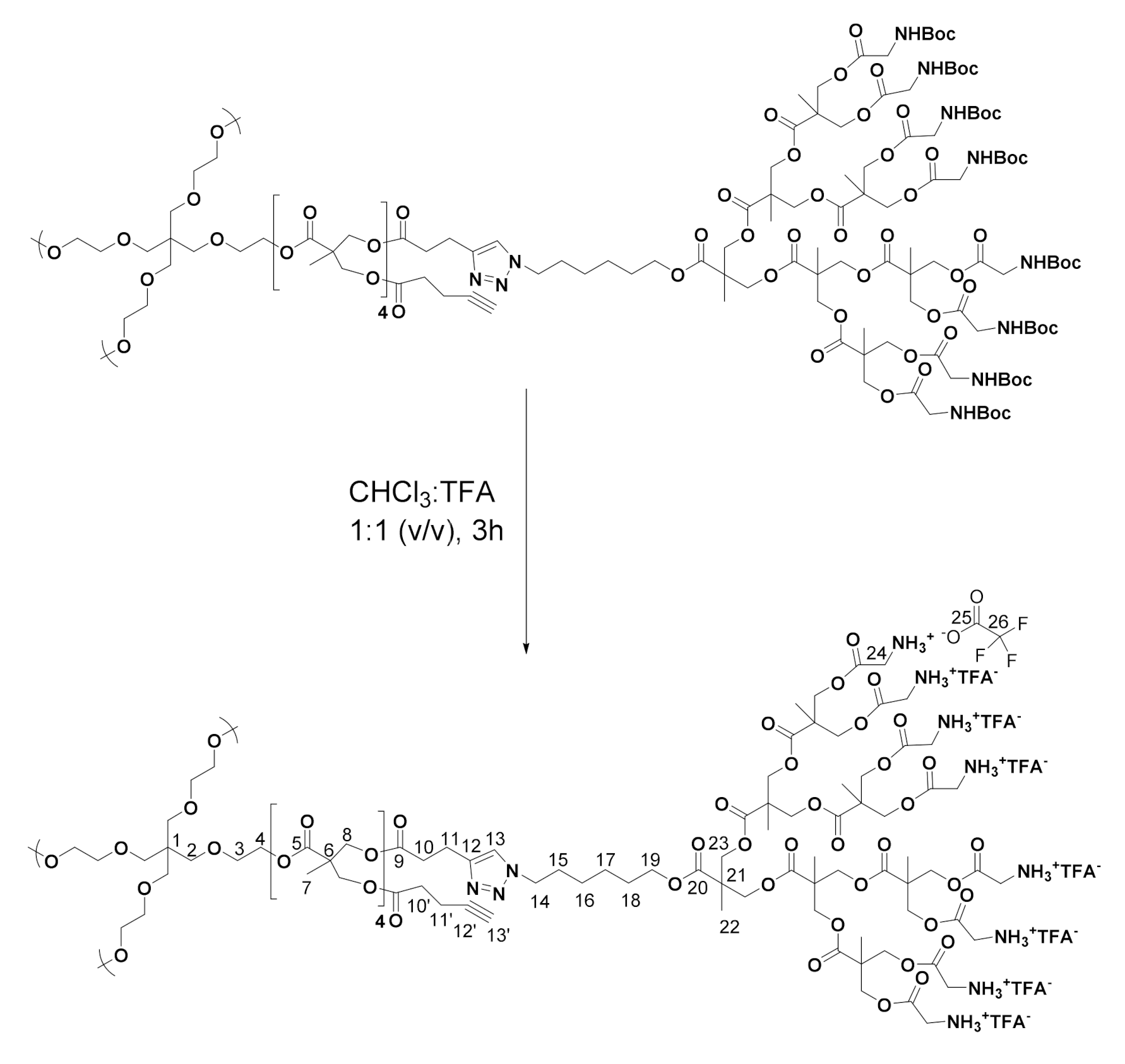
t-Boc-protected dendronized hyperbranched polymer (DHP-bMPA) was synthesized as previously reported by us [
47]. Terminal amines were deprotected as depicted in
Scheme 1, by dissolving
t-Boc protected DHP-bMPA (1.00 eq.) in a mixture of chloroform and trifluoroacetic acid (5 mL, 1:1 volume/v). The reaction mixture was stirred at room temperature for 3 h. The solvent and the excess of trifluoroacetic acid were removed under vacuum. Then, the product was dissolved in methanol and precipitated in cold ether. After decanting, the remaining solvent traces were removed under reduced pressure and the product was obtained as a white solid.
1H NMR (400 MHz, CD3OD) δ (ppm): 1.32 (1293H, m, H-7 and H-22), 1.42 (212H, m, H-16 and H-17), 1.70 (106H, m, H-18), 1.92 (106H, m, H-15), 2.73 (106H, m, H-10) 3.00 (106H, m, H-11), 3.67 (16H, m, H-2 and H-3), 3.95 (848H, m, H-24), 4.16 (106H, m, H-19), 4.32 (884H, m, H-4, H-8 and H-23[1,2G]), 4.44 (954H, H-14 and H-23[3G]), 7.80 (53H, s, H-13).
13C NMR (100 MHz, C2D6SO) δ (ppm): 16.9, 17.1 (C-7 and C-22), 20.5 (C-11), 24.8 (C-17), 25.7 (C-16), 28.0 (C-18), 29.8 (C-15), 32.8 (C-10), 46.0 (C-24), 46.3 (C-6, and C-21), 49.3 (C-14), 52.7, 63.7, 65.7 (C-8, C-19, C-23), 117.0 (JC-F = 300 Hz, C-26), 122.0 (C-12), 145.2 (C-13), 158.7 (JC-C-F = 31.5 Hz, C-25), 167.4 (C-20[G3]), 167.6, 168.2, 169.1, 171.5, 172.8 (C-5, C-9 and C-20[G0,1,2]).
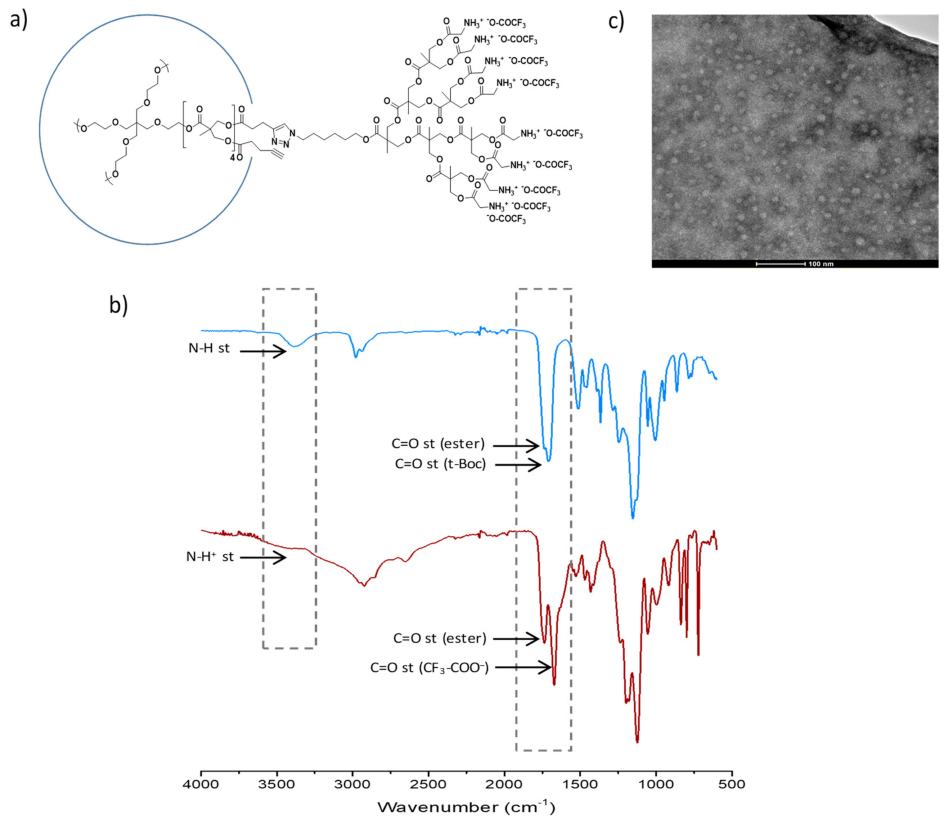
FTIR (νmax/cm−1, ATR): 3450 (bs, N-H+ st), 2930, 2860 (C-H st), 1737 (C = O st ester), 1670 (C = O st CF3-COO−), 1520 (N-H+ δ), 1432 (CH2, CH3 δ), 1193 (CO-O st), 1122 (O-C-C st).
3.3. Dendrimer Characterization Techniques
1H and 13C Nuclear Magnetic Resonance (NMR) experiments were performed using an AV-400 (1H: 400 MHz, 13C: 100 MHz) spectrometer (Bruker, Billerica, MA, USA) employing deuterated methanol (CD3OD) or deuterated dimethyl sulfoxide ((CD3)2SO) as solvents. The chemical shifts are given relative to tetramethylsilane (TMS) in ppm and the coupling constants in Hz; as internal standard, the solvent residual peak was used for spectrum calibration. Infrared spectra were recorded between 4000 and 600 cm–1 on a Vertex 70 spectrophotometer (Bruker, Billerica, MA, USA), which worked in attenuated total reflection (ATR) mode.
Transmission electron microscopy (TEM) images were recorded on a TECNAI T20 system (FEITM, Hillsboro, OR, USA) with a beam power of 200 kV. A droplet of a solution of the sample at 0.5 mg mL−1 in PBS was deposited on a holey carbon film 300 mesh coppered grids (Electron Microscopy Sciences, Hatfield, PA, USA) and a 3% w/v aqueous solution of phosphotungstic acid was used as negative stain.
3.4. Subjects and Samples
Experimental blood samples were obtained from four different sets, grouped two by two with the appropriate controls (diseased vs. controls): pancreatic cancer patients (PDAC) vs. blood donors (BD); ovarian cancer patients (OV) vs. benign ovarian cyst patients (OC). All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of CEICA (PI16/0228).
3.4.1. Pancreatic Cancer (PDAC): Patients (PDAC Diseased Group) and Blood Donor Subjects (BD Control Group) Cohort Sample Description
Samples and data from blood donor subjects as control group patients included in this study were obtained from blood donors at Blood and Tissue Bank of Aragon and provided by the Biobank of the Aragon Health System, integrated in the Spanish National Biobanks Network (PT20/00112). They were processed following standard operating procedures with the appropriate approval of the Ethics and Scientific Committees. The cohort consisted of 25 serum samples from Spanish Caucasian subjects, apparently diseased-free.
A total of 20 serum samples from patients diagnosed with pancreatic cancer at the oncology service at Hospital Universitario Miguel Servet in Zaragoza (Spain) were used in this study. Samples were collected after histopathological confirmation and prior to treatment. They were handled, stored, and provided by Biobank of the Aragon Health System.
Regarding disease/health, 55.6% of the samples were blood donor controls (BD) and 44.4% were patients diagnosed of pancreatic cancer (PDAC). According to the gender, 27/45 (60.0%) were males and 17/45 (37.8%) were females (there was only one missing demographic data in BD group). In the BD group, 16/25 (64.0%) were males and 8/25 (32.0%) were females, while in the PDAC group, 11/20 (55.0%) were males and 9/20 (45.0%) were females.
The age from PDAC group is statiscally higher than the age from BD group (
p < 0.001, Wilcoxon test,
Table 7). In the BD group, the age from males was statistically higher than the age from females (
p = 0.036,
t-test,
Table 8). In the PDAC group, there were no statistically significant differences in age depending on gender (
p = 0.703, Wilcoxon test,
Table 8).
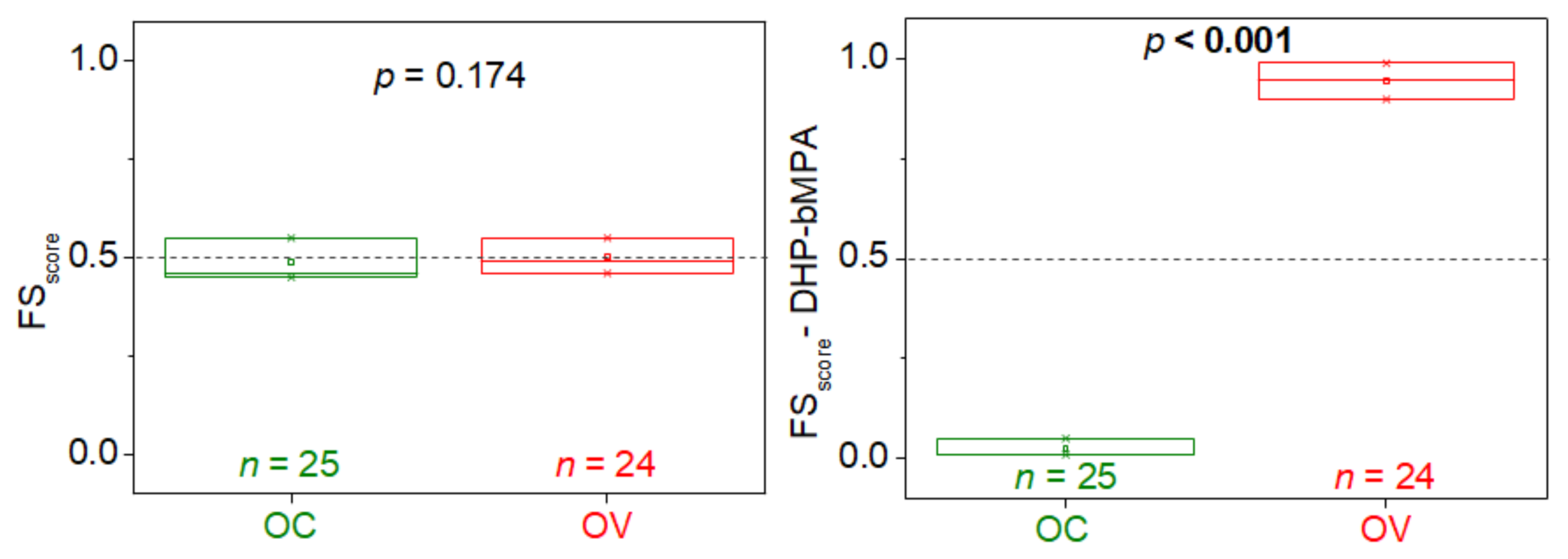
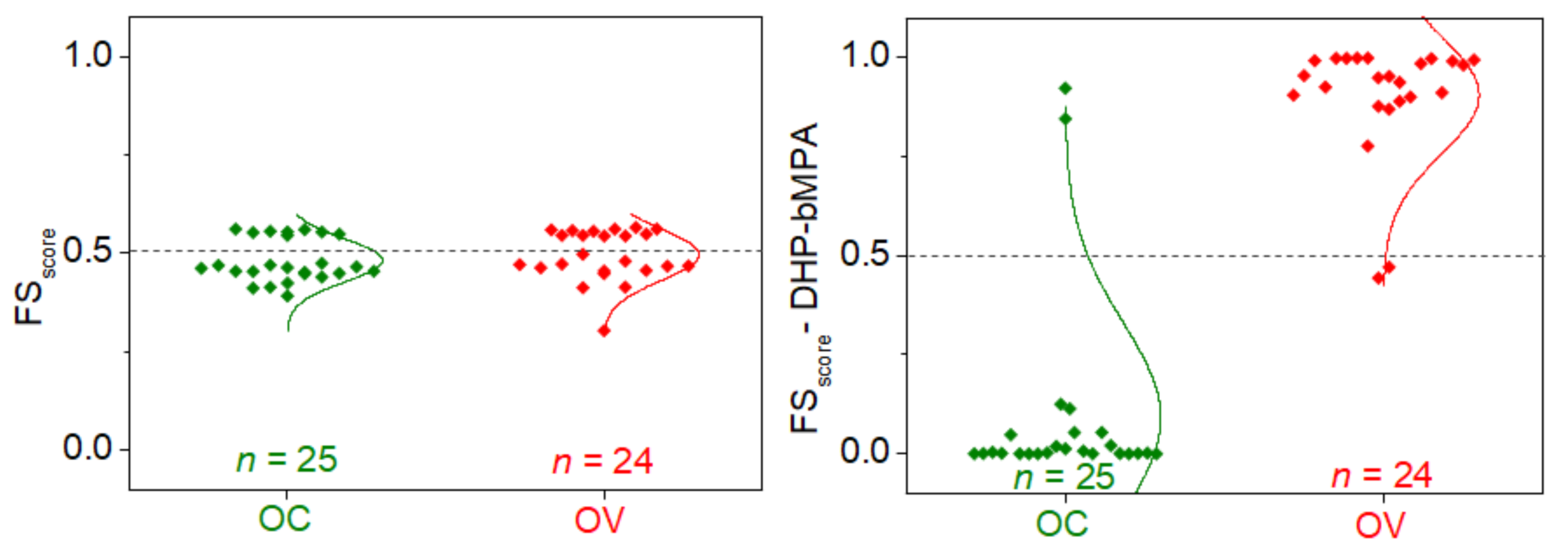
3.4.2. Ovarian Cancer (OV): Ovarian Cancer Patients (OV Diseased Group) and Benign Cyst Patients (OC Control Group) Cohort Sample Description
Samples from ovarian cancer (24) and benign cysts (25) patients diagnosed at the gynecology service at Hospital Virgen del Camino in Pamplona (Spain) were included in this study. Serum samples were collected before surgery, handled, stored, and provided by the Biobank Navarrabiomed integrated in the Spanish National Biobanks Network (PT17/0015/0007). They were processed following standard operating procedures with the appropriate approval of the Ethics and Scientific Committees.
We recruited 49 samples, 24/49 (49.0%) were from female patients diagnosed of ovarian cancer (OV), and 25/49 (51.0%) were from female patients with initially suspected ovarian cancer, but finally diagnosed as benign (OC). There was only one missing age data in the OV group.
The age from OC group is statistically higher than age from OC group (
p = 0.011, Wilcoxon test,
Table 9).
3.6. Fluorescence Spectroscopy
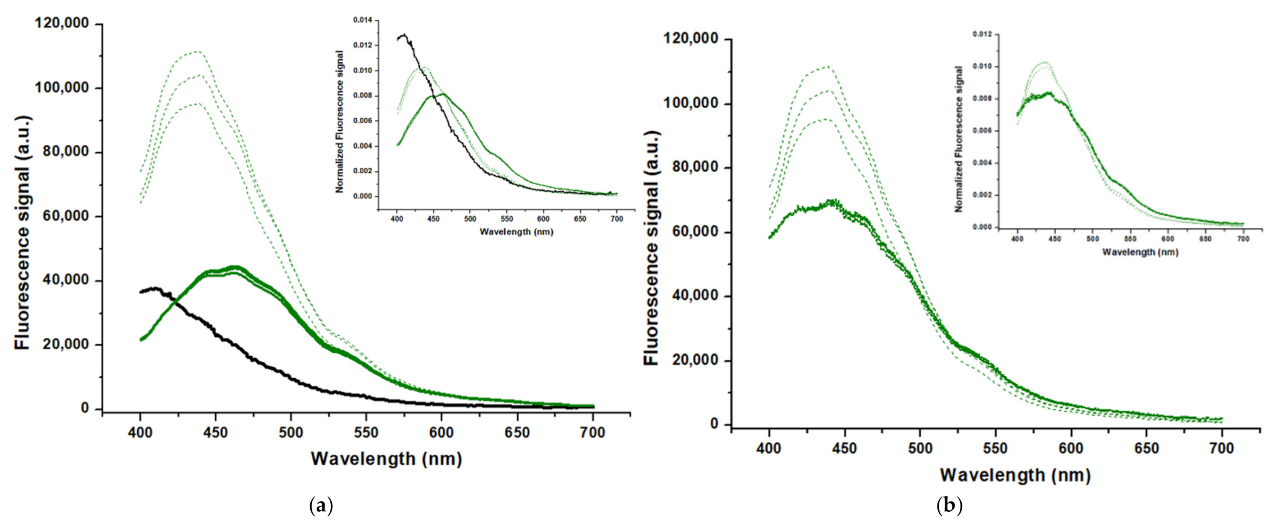
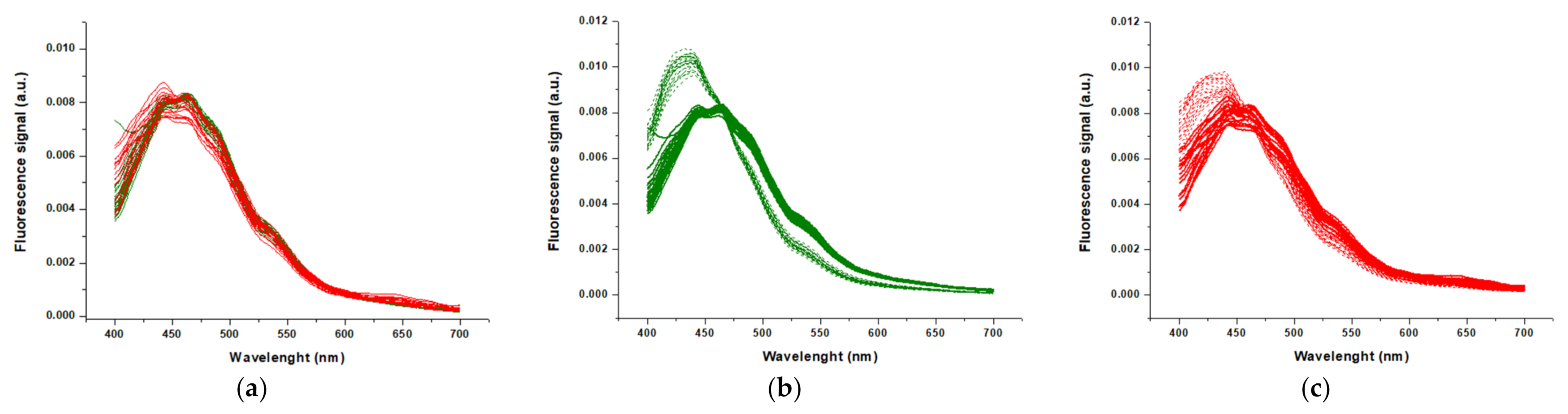
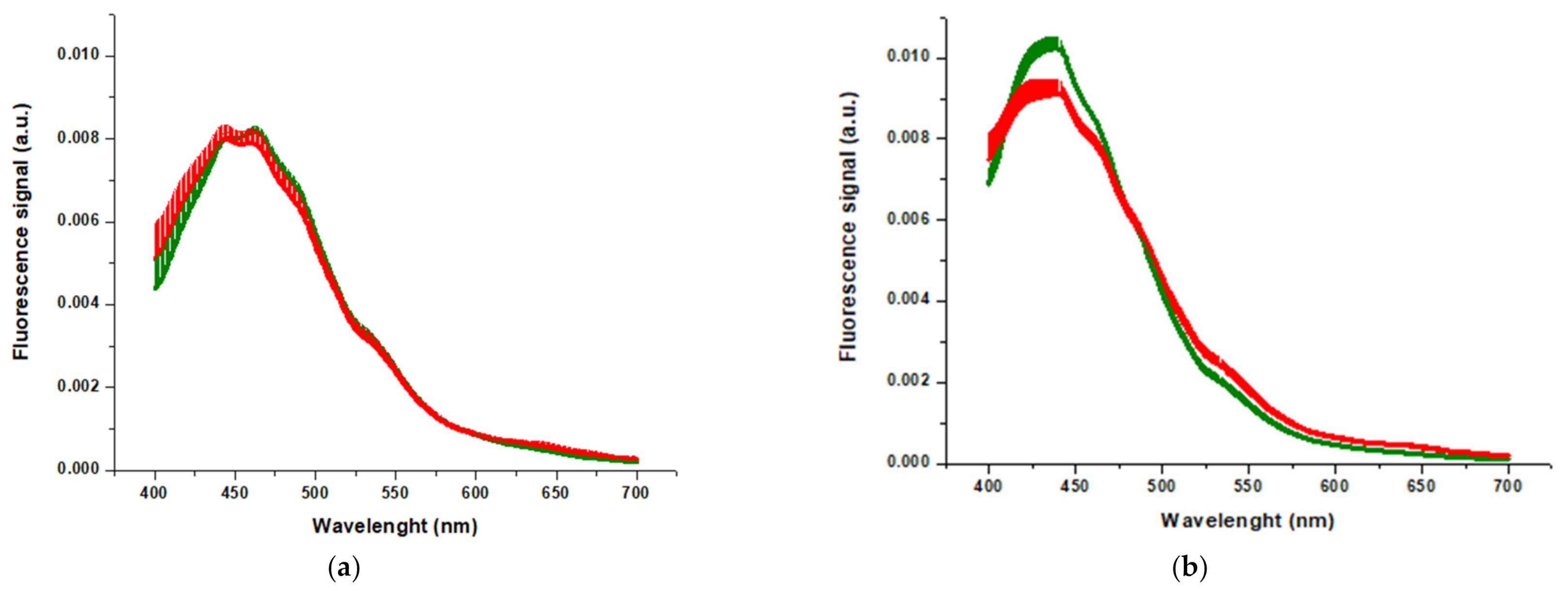
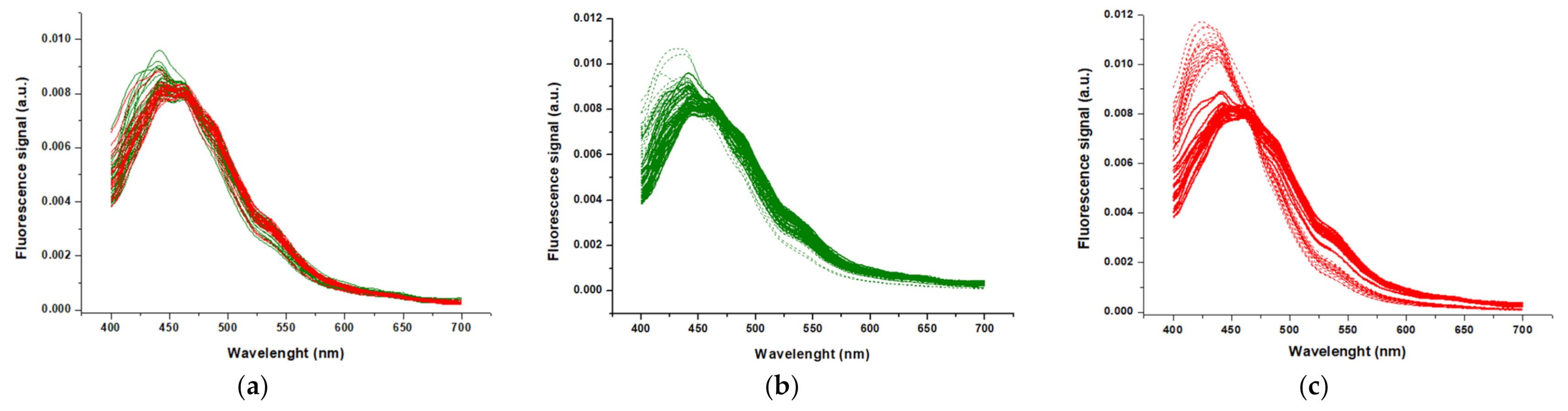
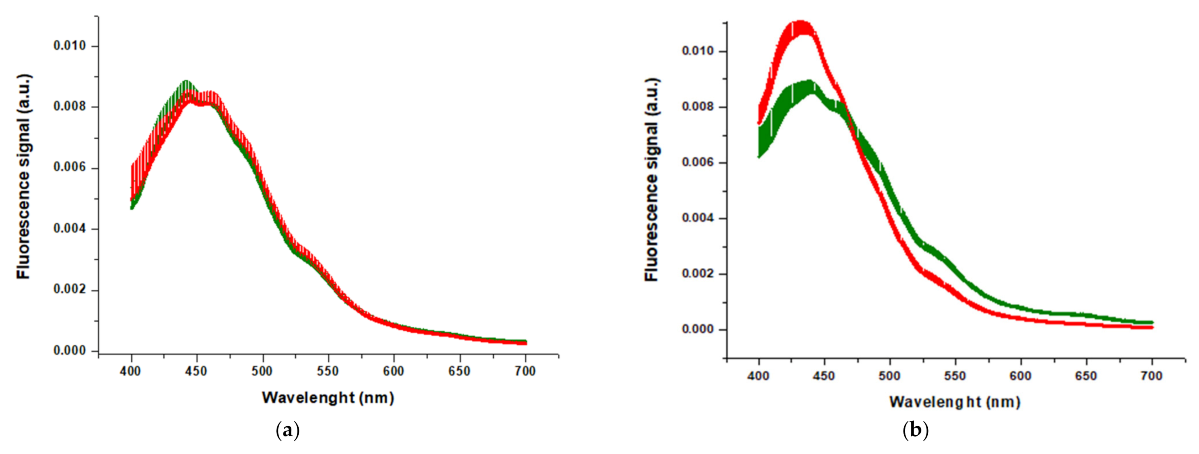
Serum samples were diluted 1:25 in PBS and, when appropriate, mixed with DHP-bMPA nanoparticles to a final concentration of 500 µg mL−1 prior data acquisition. A total volume of 80 µL was transferred into 96-well microplates (96-well PCR plate, non-skirted, from 4titude, Surrey, UK). Fluorescence measurements were performed in a CLARIOstar plate reader (BMG Labtech, Germany) selecting an excitation wavelength of 330 nm, with excitation and emission bandwidths of 10 nm, and recording the fluorescence emission spectra in the range 400–700 nm. The excitation wavelength was slightly higher than optimal for tryptophan excitation (295 nm), but was a constraint from the instrument. Multimode plate readers with fluorescence capabilities very seldom offer the possibility to use lower excitation wavelengths.
All the fluorescence spectra,
F(
λ), where
F is the fluorescence emission intensity and
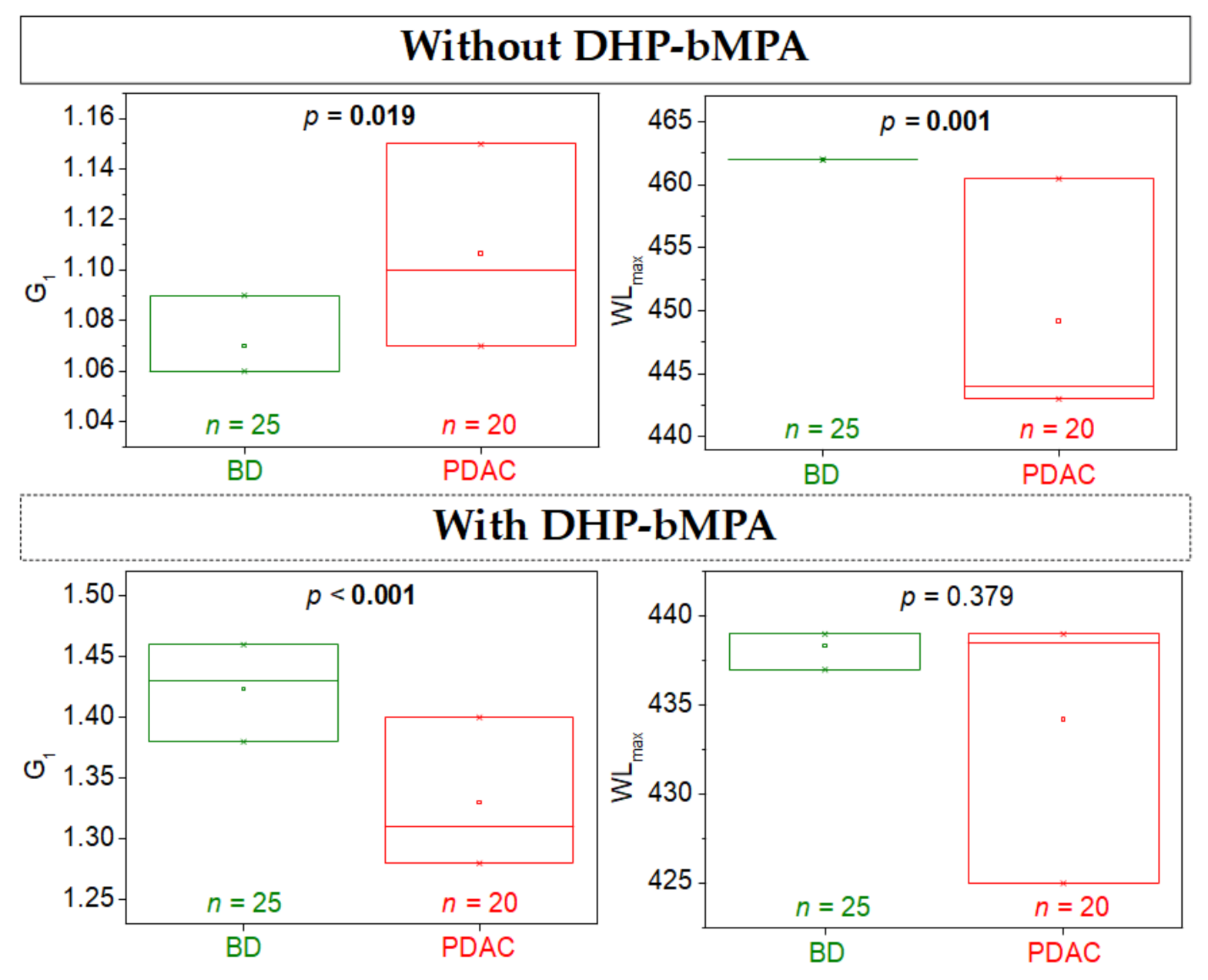
λ is the wavelength, were normalized to an area equal to 1, and two parameters (
G1 and
WLmax) were calculated according to the following equations:
where <
λ> is the average wavelength (or first moment) considering the spectrum as a probability density function:
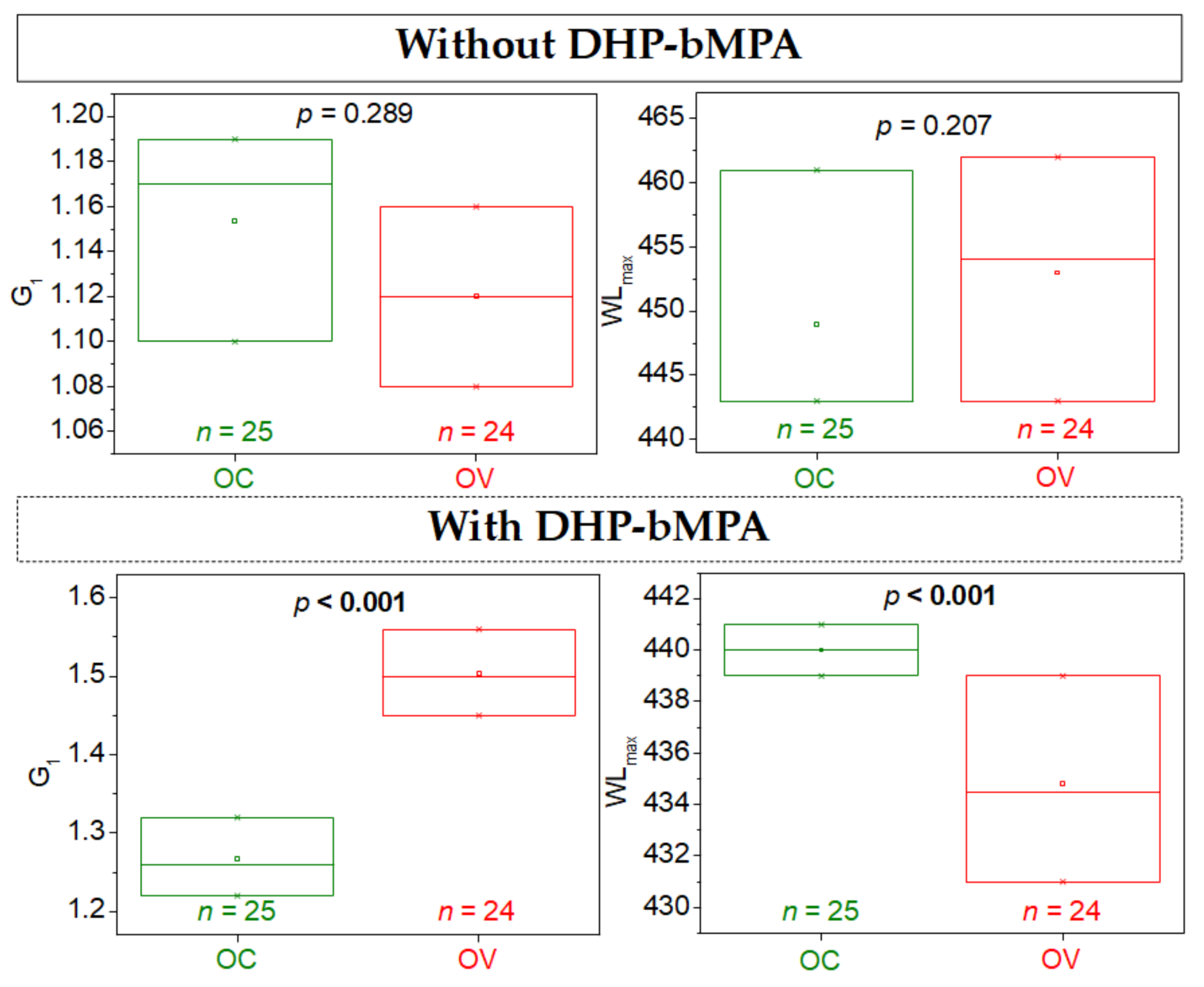
m2 and m3 are the second and third moments of that density distribution, G1 is the parameter that provides a measure of the asymmetry or skewness of the spectrum. In addition, the wavelength corresponding to the maximal fluorescence intensity of the spectrum (mode of the probability density function), WLmax, is a central measure providing information about the location of the main region of the spectrum.
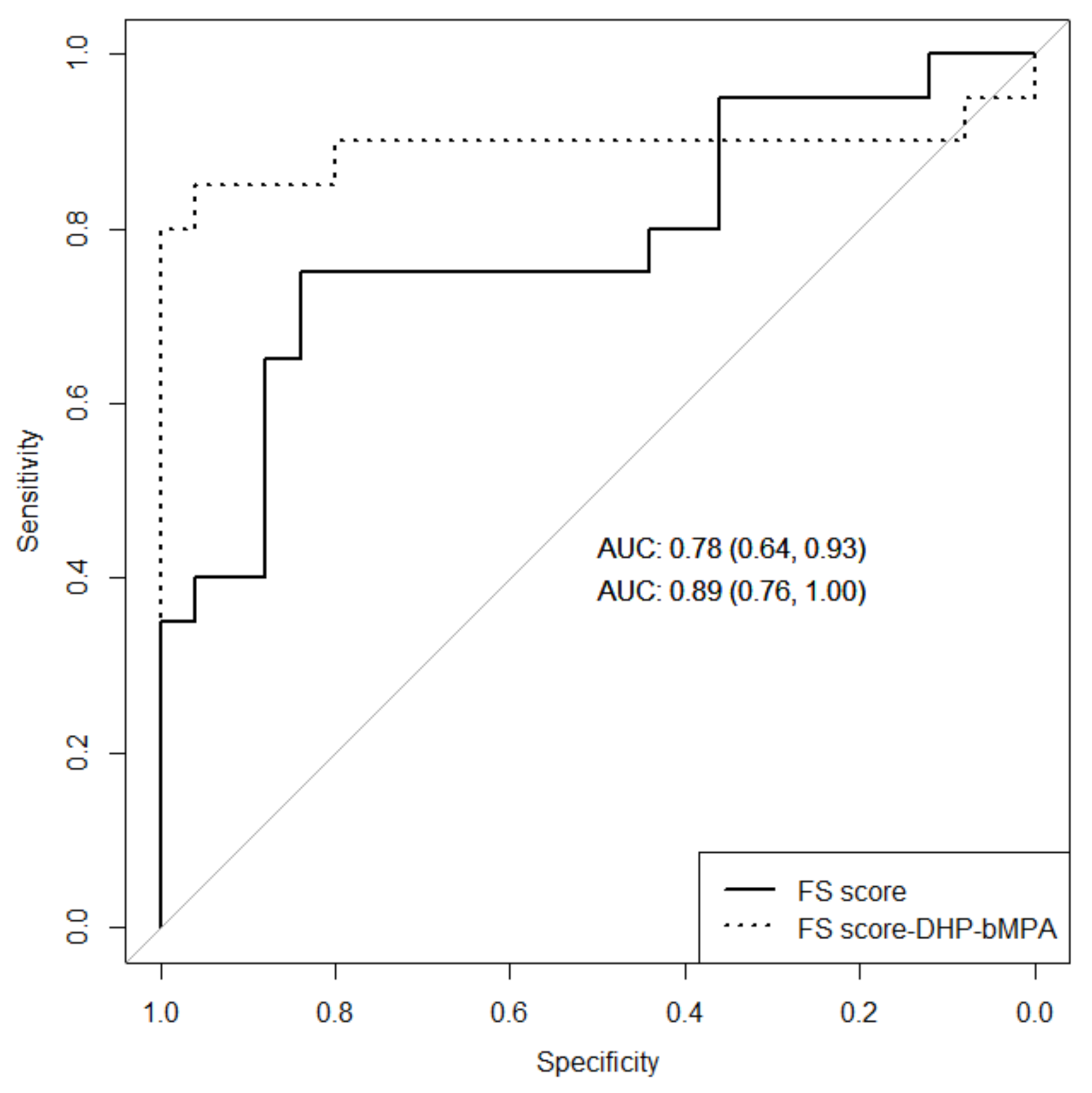
3.7. Statistical Analysis
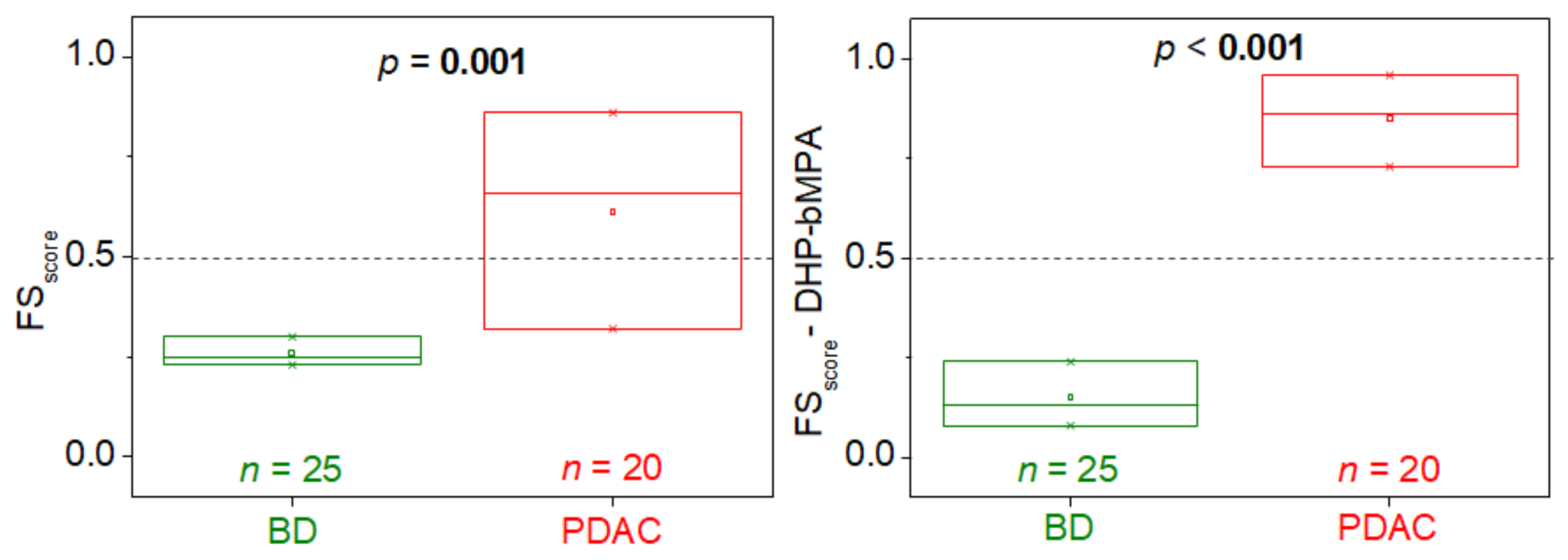
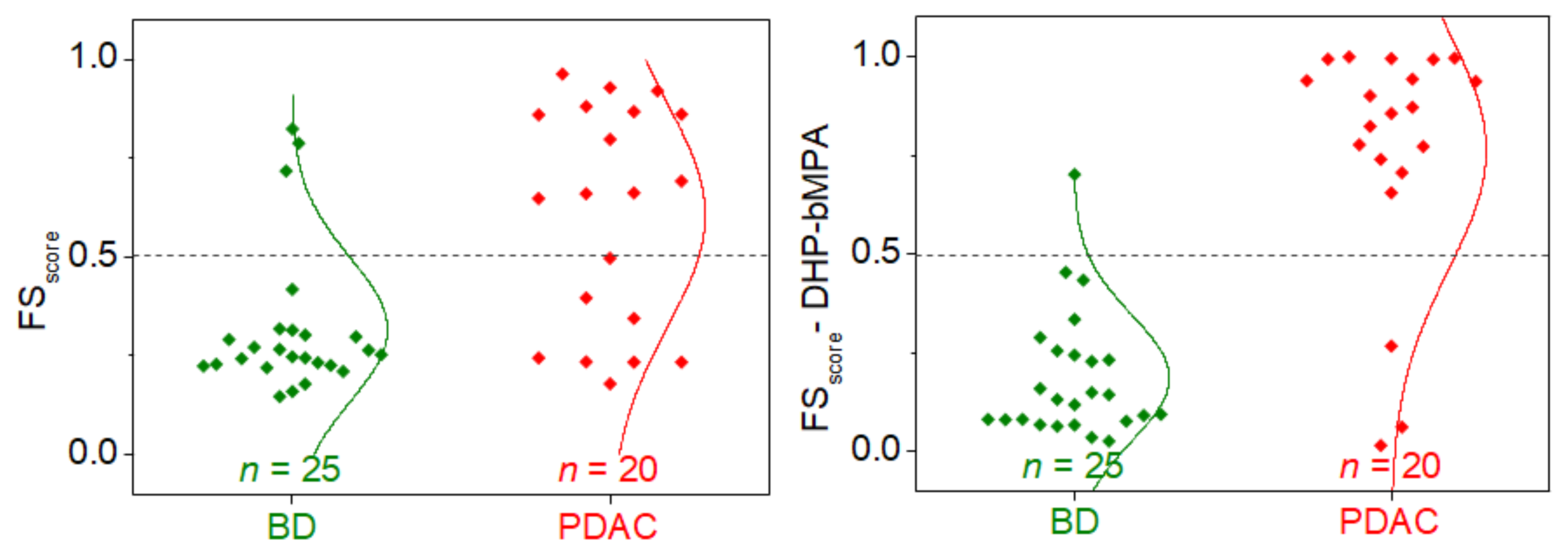
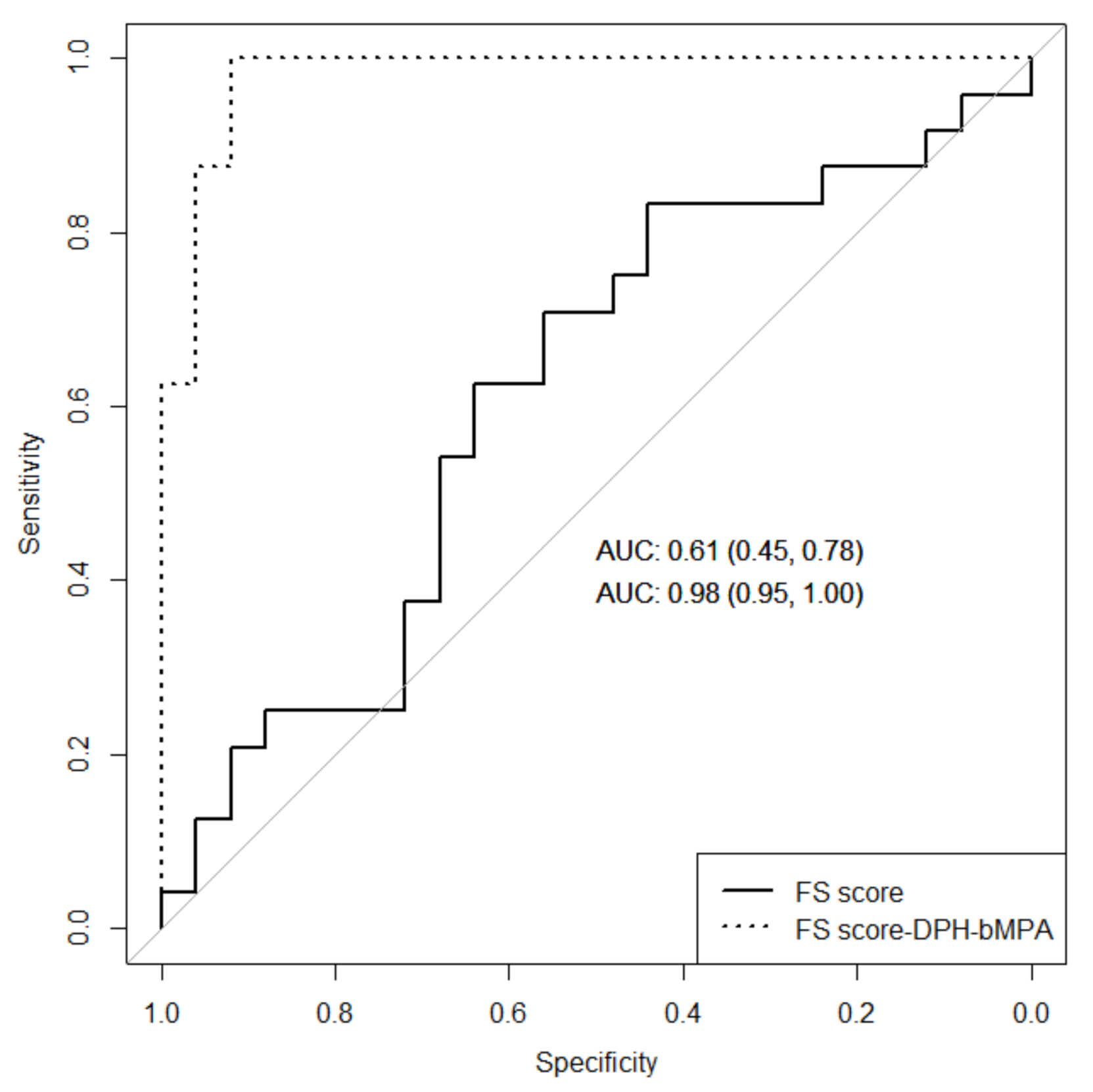
Fluorescence raw data were processed using Origin software (OriginLab, Northampton, MA). Two parameters summarizing the essential geometric features of each fluorescence spectrum were directly calculated, G1 and WLmax, and were used for calculating the FSscore to compare fluorescence spectra and build the classification model by using a generalized linear model (GLM). FSscore provides the probability of an individual fluorescence spectrum for reflecting serum alterations. Such FSscore is a single value employed for classifying a given subject as control or diseased. As any probability, the FSscore ranges between 0 and 1: the model classifies the subjects with FSscore values > 0.5 as individuals with high probability of having serum alterations (i.e., diseased status), and the subjects with FSscore values < 0.5 as individuals with low probability of having serum alterations (i.e., healthy status). The performance of the diagnostic test was evaluated by calculating common statistical performance indexes (e.g., sensitivity, specificity) and the receiver operating characteristic (ROC) curve. Net Reclassification Index (NRI) of Pencina and/or Delong test were performed to compare area under curve (AUC) ROC.
The Kolmogorov–Smirnov test was performed to assess the normal distribution of the variables. Averages between two independent groups were compared with the t-test in normal distributions. Medians between two independent groups were compared with the Wilcoxon test in non-normal distributions. Comparisons between groups for qualitative variables were made using a chi-squared test.
The statistical analyses were performed using Rstudio, R version 3.6.1 (RStudio, PBC, Boston, MA, USA) (2019-07-05). For all tests, a two-sided p-value of less than 0.050 was considered statistically significant.


 ,
, 















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}