
Canrenone Restores Vasorelaxation Impaired by Marinobufagenin in Human Preeclampsia

 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Methods
4.1. General
4.2. Preparation of the Placentae Sections
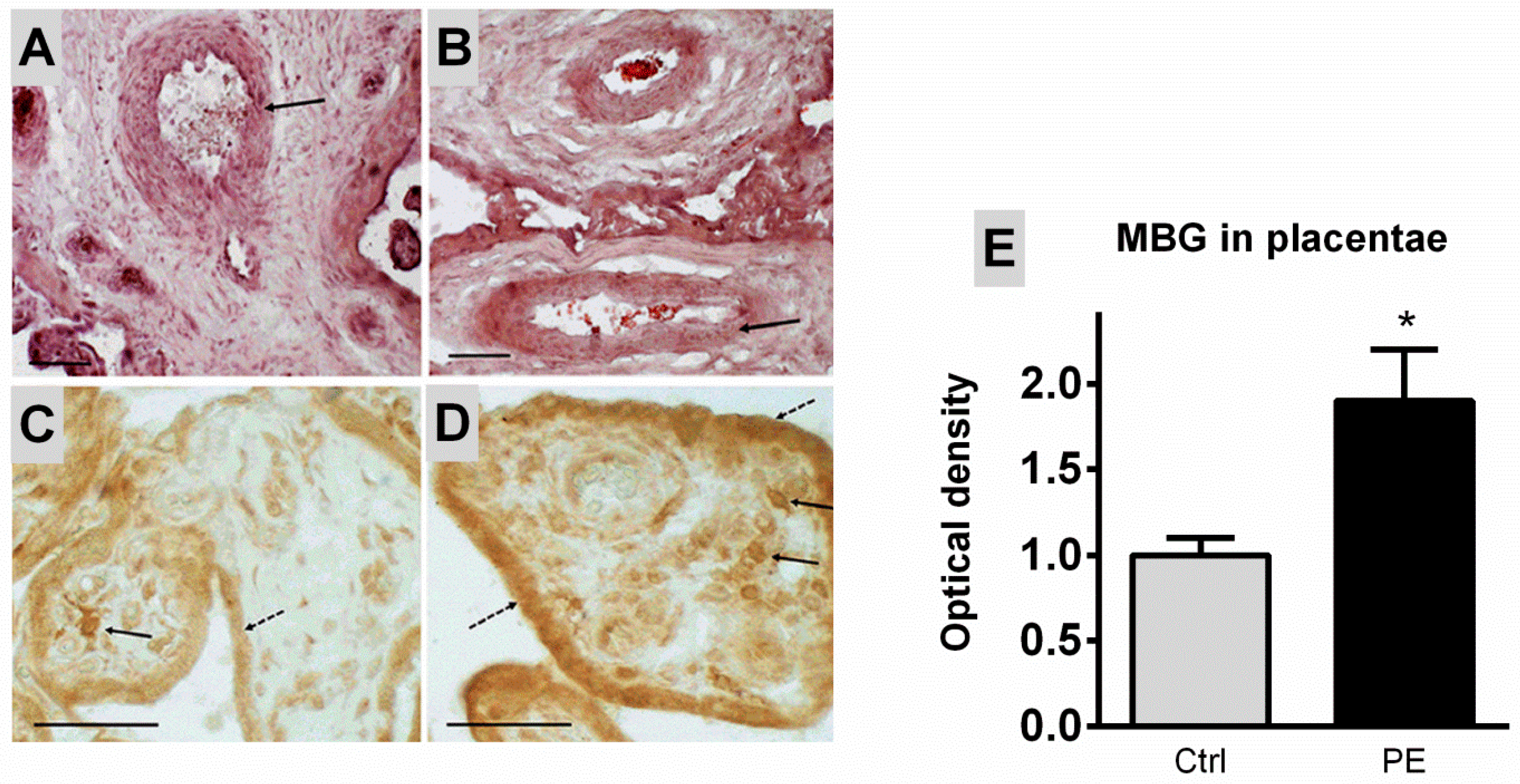
4.3. Histological Analysis and Immunohistochemical Identification of MBG in Placenta
4.4. Microscopy
4.5. Umbilical Arteries
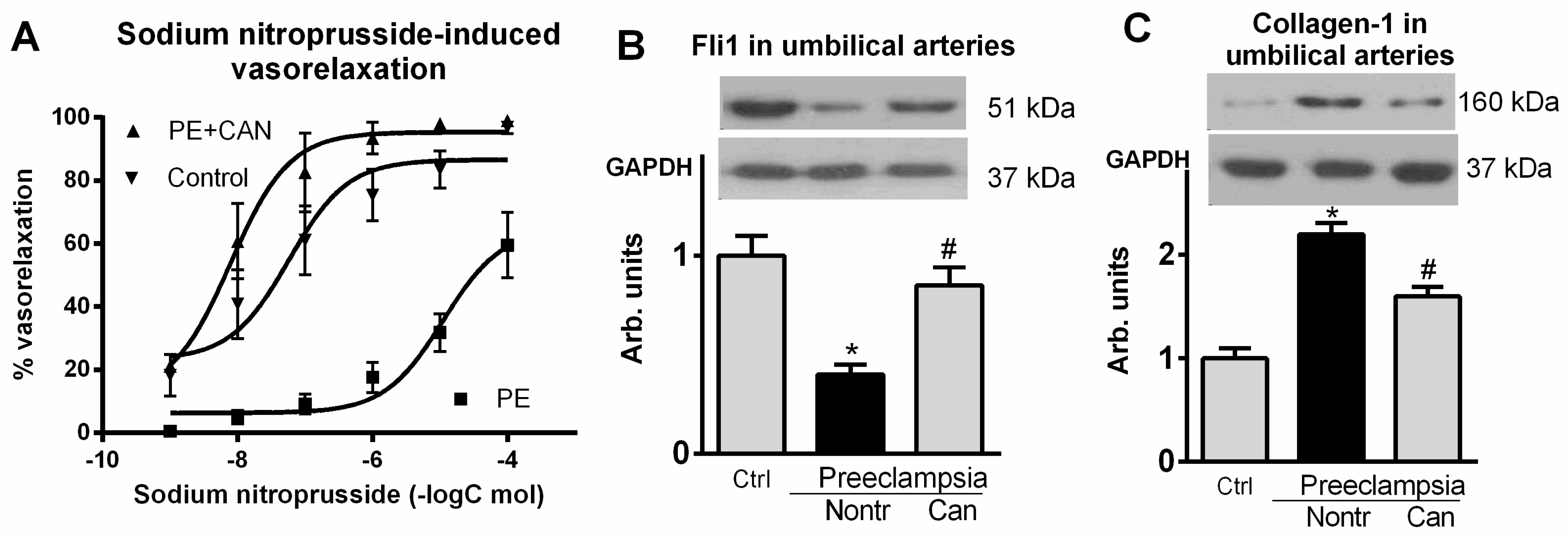
4.5.1. Isolated Umbilical Artery Contractile Studies
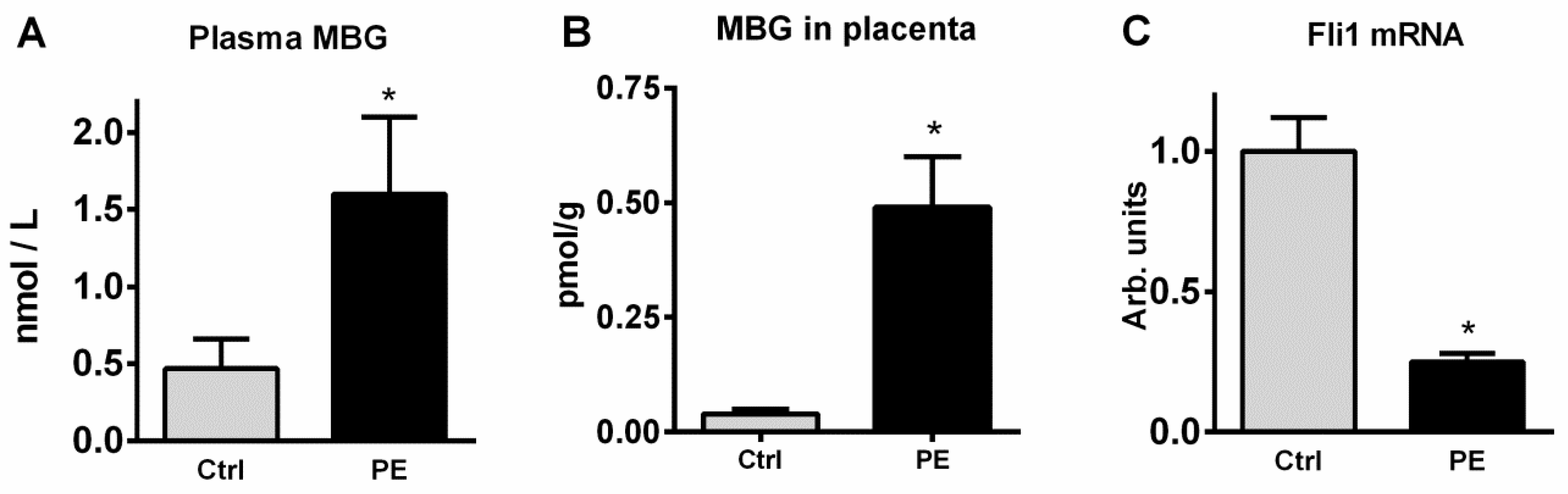
4.5.2. MBG Measurement
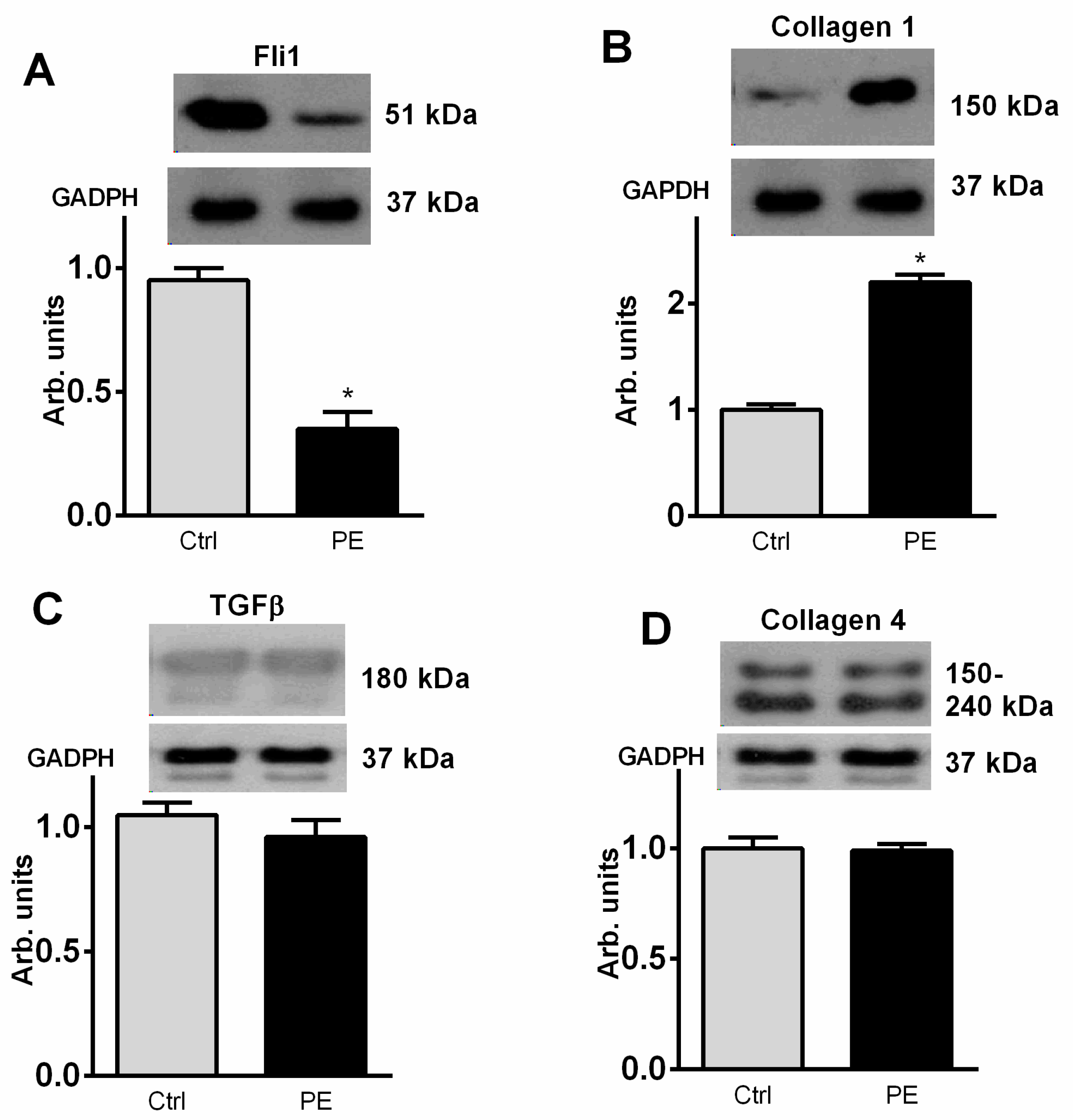
4.6. Western Blotting
4.7. The RNA Extraction, Reverse Transcription and Real-Time Quantitative PCR Analysis
4.8. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bagrov, A.Y.; Shapiro, J.I.; Fedorova, O.V. Endogenous cardiotonic steroids: Physiology, pharmacology and novel therapeutic targets. Pharmacol. Rev. 2009, 61, 9–38. [Google Scholar] [CrossRef]
- Fedorova, O.V.; Bagrov, A.Y. Inhibition of Na/K-ATPase from rat aorta by two endogenous Na/K pump inhibitors, ouabain and marinobufagenin. Evidence of interaction with different alpha-subinit isoforms. Am. J. Hypertens. 1997, 10, 929–993. [Google Scholar] [CrossRef] [Green Version]
- Periyasamy, S.M.; Liu, J.; Tanta, F.; Kabak, B.; Wakefield, B.; Malhotra, D.; Kennedy, D.J.; Nadoor, A.; Fedorova, O.V.; Gunning, W.; et al. Salt loading induces redistribution of the plasmalemmal Na/K-ATPase in proximal tubule cells. Kidney Int. 2005, 67, 1868–1877. [Google Scholar] [CrossRef] [Green Version]
- Bagrov, A.Y.; Fedorova, O.V.; Dmitrieva, R.I.; French, A.W.; Anderson, D.E. Plasma marinobufagenin-like and ouabain-like immunorecativity during acute saline volume expansion in anesthetized dogs. Cardiovasc. Res. 1996, 206, 296–305. [Google Scholar] [CrossRef] [Green Version]
- Nikitina, E.R.; Mikhailov, A.V.; Nikandrova, E.S.; Frolova, E.V.; Fadeev, A.V.; Shman, V.V.; Shilova, V.Y.; Tapilskaya, N.I.; Shapiro, J.I.; Fedorova, O.V.; et al. In preeclampsia endogenous cardiotonic steroids induce vascular fibrosis and impair relaxation of umbilical arteries. J. Hypertens. 2011, 29, 769–776. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, D.J.; Vetteth, S.; Periyasamy, S.M.; Kanj, M.; Fedorova, L.; Khouri, S.; Kahaleh, B.; Xie, Z.; Malhotra, D.; Kolodkin, N.I.; et al. Central role for the cardiotonic steroid marinobufagenin in the pathogenesis of experimental uremic cardiomyopathy. Hypertension 2006, 47, 488–495. [Google Scholar] [CrossRef]
- Strauss, M.; Smith, W.; Wei, W.; Bagrov, A.Y.; Fedorova, O.V.; Schutte, A.E. Large artery stiffness is associated with marinobufagenin in young adults: The African- PREDICT study. J. Hypertens. 2018, 36, 2333–2339. [Google Scholar] [CrossRef] [PubMed]
- Strauss, M.; Smith, W.; Fedorova, O.V.; Schutte, A.E. The Na+K+-ATPase Inhibitor Marinobufagenin and Early Cardiovascular Risk in Humans: A Review of Recent Evidence. Curr. Hypertens. Rep. 2019, 21, 38. [Google Scholar] [CrossRef] [PubMed]
- Lopatin, D.A.; Ailamazian, E.K.; Dmitrieva, R.I.; Shpen, V.M.; Fedorova, O.V.; Doris, P.A.; Bagrov, A.Y. Circulating bufodienolide and cardenolide sodium pump inhibitors in preeclampsia. J. Hypertens. 1999, 17, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Fedorova, O.V.; Kolodkin, N.I.; Agalakova, N.I.; Namikas, A.R.; Bzhelyansky, A.; St-Louis, J.; Lakatta, E.G.; Bagrov, A.Y. Antibody to marinobufagenin lowers blood pressure in pregnant rats on a high NaCl intake. J. Hypertens. 2005, 23, 835–842. [Google Scholar] [CrossRef]
- Fedorova, O.V.; Simbirtsev, A.S.; Kolodkin, N.I.; Kotov, A.Y.; Agalakova, N.I.; Kashkin, V.A.; Tapilskaya, N.I.; Bzhelyansky, A.M.; Reznik, V.A.; Nikitina, E.R.; et al. Monoclonal antibody to an endogenous bufadienolide, marinobufagenin, reverses preeclampsia-induced Na/K-ATPase inhibition in lowers blood pressure in NaCl-sensitive hypertension. J. Hypertens. 2008, 26, 2414–2425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorova, O.V.; Ishkaraeva, V.V.; Grigorova, Y.N.; Reznik, V.A.; Kolodkin, N.I.; Zazerskaya, I.E.; Zernetkina, V.; Agalakova, N.I.; Tapilskaya, N.I.; Adair, C.D.; et al. Antibody to Marinobufagenin Reverses Placenta-Induced Fibrosis of Umbilical Arteries in Preeclampsia. Int. J. Mol. Sci. 2018, 19, 2377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agalakova, N.I.; Reznik, V.A.; Nadei, O.V.; Ershov, I.A.; Rassokha, O.S.; Vasyutina, M.L.; Ivanov, D.O.; Adair, E.D.; Galagudza, M.M.; Bagrov, A.Y. Antibody against Na/K-ATPase inhibitor lowers blood pressure and increases vascular Fli1 in experimental preeclampsia. Am. J. Hypertens. 2020, 33, 514–519. [Google Scholar] [CrossRef]
- Agalakova, N.I.; Kolodkin, N.I.; Adair, C.D.; Trashkov, A.P.; Bagrov, A.Y. Preeclampsia: Cardiotonic Steroids, Fibrosis, Fli1 and Hint to Carcinogenesis. Int. J. Mol. Sci. 2021, 22, 1941. [Google Scholar] [CrossRef] [PubMed]
- Haller, S.T.; Kennedy, D.J.; Shidyak, A.; Budny, G.V.; Malhotra, D.; Fedorova, O.V.; Shapiro, J.I.; Bagrov, A.Y. Monoclonal antibody against marinobufagenin reverses cardiac fibrosis in rats with chronic renal failure. Am. J. Hypertens. 2012, 25, 690–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorova, O.V.; Emelianov, I.V.; Bagrov, K.A.; Grigorova, Y.N.; Wei, W.; Juhasz, O.; Frolova, E.V.; Marshall, C.A.; Lakatta, E.G.; Konradi, A.O.; et al. Marinobufagenin-induced vascular fibrosis is a likely target for mineralocorticoid antagonists. J. Hypertens. 2015, 33, 1602–1610. [Google Scholar] [CrossRef] [Green Version]
- Eschalier, R.; McMurray, J.J.; Swedberg, K.; van Veldhuisen, D.J.; Krum, H.; Pocock, S.J.; Shi, H.; Vincent, J.; Rossignol, P.; Zannad, F.; et al. Safety and efficacy of eplerenone in patients at high risk for hyperkalemia and/or worsening renal function: Analyses of the EMPHASIS-HF study subgroups (Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure). J. Am. Coll. Cardiol. 2013, 62, 1585–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakris, G.; Yang, Y.F.; Pitt, B. Mineralocorticoid Receptor Antagonists for Hypertension Management in Advanced Chronic Kidney Disease: BLOCK-CKD Trial. Hypertension 2020, 76, 144–149. [Google Scholar] [CrossRef]
- National Institutes of Health Working Group on Hypertension in Pregnancy. Classification of Hypertensive Disorders of Pregnancy; US Department of Health and Human Services: Bethesda, MD, USA, 1991.
- Selye, H.; Jelinek, J.; Krajny, M. Prevention of digitoxin poisoning by various steroids. J. Pharm. Sci. 1969, 58, 1055–1059. [Google Scholar] [CrossRef]
- Selye, H.; Krajny, M.; Savoie, L. Digitoxin poisoning: Prevention by spironolactone. Science 1969, 164, 842–843. [Google Scholar] [CrossRef]
- de Mendonça, M.; Grichois, M.L.; Pernollet, M.G.; Wauquier, I.; Trouillet-Thormann, B.; Meyer, P.; Devynck, M.A.; Garay, R. Antihypertensive effect of canrenone in a model where endogenous ouabain-like factors are present. J. Cardiovasc. Pharmacol. 1988, 11, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Semplicini, A.; Serena, L.; Valle, R.; Ceolotto, G.; Felice, M.; Fontebasso, A.; Pessina, A.C. Ouabain-inhibiting activity of aldosterone antagonists. Steroids 1995, 60, 110–113. [Google Scholar] [CrossRef]
- Buckalew, V.M. Role of endogenous digitalis-like factors in the clinical manifestations of severe preeclampsia: A systematic review. Clin. Sci. 2018, 132, 1215–1242. [Google Scholar] [CrossRef] [PubMed]
- Sibai, B.; Dekker, G.; Kupferminc, M. Pre-eclampsia. Lancet 2005, 365, 785–799. [Google Scholar] [CrossRef]
- Burton, G.J.; Redman, C.W.; Roberts, J.M.; Moffett, A. Pre-eclampsia: Pathophysiology and clinical implications. BMJ 2019, 366, l2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorova, O.V.; Zernetkina, V.I.; Shilova, V.Y.; Grigorova, Y.N.; Juhasz, O.; Wei, W.; Marshall, C.A.; Lakatta, E.G.; Bagrov, A.Y. Synthesis of an endogenous steroidal Na pump inhibitor marinobufagenin, implicated in human cardiovascular diseases, is initiated by CYP27A1 via bile acid pathway. Circ. Cardiovasc. Genet. 2015, 8, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Fedorova, O.V.; Fadeev, A.V.; Grigorova, Y.N.; Agalakova, N.I.; Konradi, A.O.; Bagrov, A.Y. Marinobufagenin induces vascular fibrosis via a pressure-independent mechanism in NaCl-loaded diabetic rats. J. Cardiovasc. Pharmacol. 2019, 74, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Elkareh, J.; Periyasamy, S.M.; Shidyak, A.; Vetteth, S.; Schroeder, J.; Raju, V.; Hariri, I.M.; El-Okdi, N.; Gupta, S.; Fedorova, L.; et al. Marinobufagenin induces increases in procollagen expression in a process involving protein kinase C and Fli-1: Implications for uremic cardiomyopathy. Am. J. Physiol. Renal Physiol. 2009, 296, F1219–F1226. [Google Scholar] [CrossRef] [PubMed]
- Asano, Y.; Stawski, L.; Hant, F.; Highland, K.; Silver, R.; Szalai, G.; Watson, D.K.; Trojanowska, M. Endothelial Fli1 deficiency impairs vascular homeostasis: A role in scleroderma vasculopathy. Am. J. Pathol. 2010, 176, 1983–1998. [Google Scholar] [CrossRef] [PubMed]
- Carracedo, S.; Sacher, F.; Brandes, G.; Braun, U.; Leitges, M. Redundant role of protein kinase C delta and epsilon during mouse embryonic development. PLoS ONE 2014, 9, e103686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keskin, T.; Bakaric, A.; Waszyk, P.; Boulay, G.; Torsello, M.; Cornaz-Buros, S.; Chevalier, N.; Geiser, T.; Martin, P.; Volorio, A.; et al. LIN28B Underlies the Pathogenesis of a Subclass of Ewing Sarcoma LIN28B Control of EWS-FLI1 Stability. Cell Rep. 2020, 30, 4567–4583.e5. [Google Scholar] [CrossRef] [PubMed]
- Quan, Y.; Shan, X.; Hu, M.; Jin, P.; Ma, J.; Fan, J.; Yang, J.; Zhang, H.; Fan, X.; Gong, Y.; et al. YAP inhibition promotes endothelial cell differentiation from pluripotent stem cell through EC master transcription factor FLI1. J. Mol. Cell. Cardiol. 2021, 163, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Ferdous, A.; Singh, S.; Luo, Y.; Abedin, M.J.; Jiang, N.; Perry, C.E.; Evers, B.M.; Gillette, T.G.; Kyba, M.; Trojanowska, M.; et al. Fli1 Promotes Vascular Morphogenesis by Regulating Endothelial Potential of Multipotent Myogenic Progenitors. Circ. Res. 2021, 129, 949–964. [Google Scholar] [CrossRef] [PubMed]
- Matrone, G.; Xia, B.; Chen, K.; Denvir, M.A.; Baker, A.H.; Cooke, J.P. Fli1+ cells transcriptional analysis reveals an Lmo2-Prdm16 axis in angiogenesis. Proc. Natl. Acad. Sci. USA 2021, 118, e2008559118. [Google Scholar] [CrossRef] [PubMed]
- Kolmakova, E.V.; Haller, S.T.; Kennedy, D.J.; Isachkina, A.N.; Budny, G.V.; Frolova, E.V.; Nikitina, E.R.; Piecha, G.; Malhotra, D.; Fedorova, O.V.; et al. Endogenous cardiotonic steroids in chronic renal failure. Nephrol. Dial. Transplant. 2011, 26, 2912–2919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolignano, D.; De Rosa, S.; Greco, M.; Presta, P.; Patella, G.; Crugliano, G.; Sabatino, S.; Strangio, S.; Romano, L.R.; Comi, A.; et al. Marinobufagenin, left ventricular geometry and cardiac dysfunction in end-stage kidney disease patients. Int. Urol. Nephrol. 2022, in press.
- Emelyanov, I.V.; Fedorova, O.V.; Lakatta, E.G.; Konradi, A.O.; Bagrov, A.Y. In resistant hypertension NaCl-induced marinobufagenin-dependent Na/K-ATPase inhibition associates with vascular stiffness. Curr. Top. Membranes 2019, 83, 1–13. [Google Scholar] [CrossRef]
- Romanova, I.V.; Derkach, K.V.; Mikhrina, A.L.; Sukhov, I.B.; Mikhailova, E.V.; Shpakov, A.O. The Leptin, Dopamine and Serotonin Receptors in Hypothalamic POMC-Neurons of Normal and Obese Rodents. Neurochem. Res. 2018, 43, 821–837. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 12) | Patients with PE (n = 15) | |
|---|---|---|
| Age (years) | 34 ± 1 | 34 ± 2 |
| Gestational age (weeks) | 39 ± 0.5 | 37.9 ± 0.2 |
| Systolic BP (mmHg) | 116 ± 2 | 148 ± 4 * |
| Diastolic BP (mmHg) | 73 ± 1 | 94 ± 3 * |
| Protein excretion (g per 24 h) | n/d | 1.4 ± 0.3 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agalakova, N.I.; Grigorova, Y.N.; Ershov, I.A.; Reznik, V.A.; Mikhailova, E.V.; Nadei, O.V.; Samuilovskaya, L.; Romanova, L.A.; Adair, C.D.; Romanova, I.V.; et al. Canrenone Restores Vasorelaxation Impaired by Marinobufagenin in Human Preeclampsia. Int. J. Mol. Sci. 2022, 23, 3336. https://doi.org/10.3390/ijms23063336
Agalakova NI, Grigorova YN, Ershov IA, Reznik VA, Mikhailova EV, Nadei OV, Samuilovskaya L, Romanova LA, Adair CD, Romanova IV, et al. Canrenone Restores Vasorelaxation Impaired by Marinobufagenin in Human Preeclampsia. International Journal of Molecular Sciences. 2022; 23(6):3336. https://doi.org/10.3390/ijms23063336
Chicago/Turabian StyleAgalakova, Natalia I., Yulia N. Grigorova, Ivan A. Ershov, Vitaly A. Reznik, Elena V. Mikhailova, Olga V. Nadei, Leticia Samuilovskaya, Larisa A. Romanova, C. David Adair, Irina V. Romanova, and et al. 2022. "Canrenone Restores Vasorelaxation Impaired by Marinobufagenin in Human Preeclampsia" International Journal of Molecular Sciences 23, no. 6: 3336. https://doi.org/10.3390/ijms23063336