
Overview of MicroRNAs as Diagnostic and Prognostic Biomarkers for High-Incidence Cancers in 2021
 and
and
Abstract
:1. Introduction
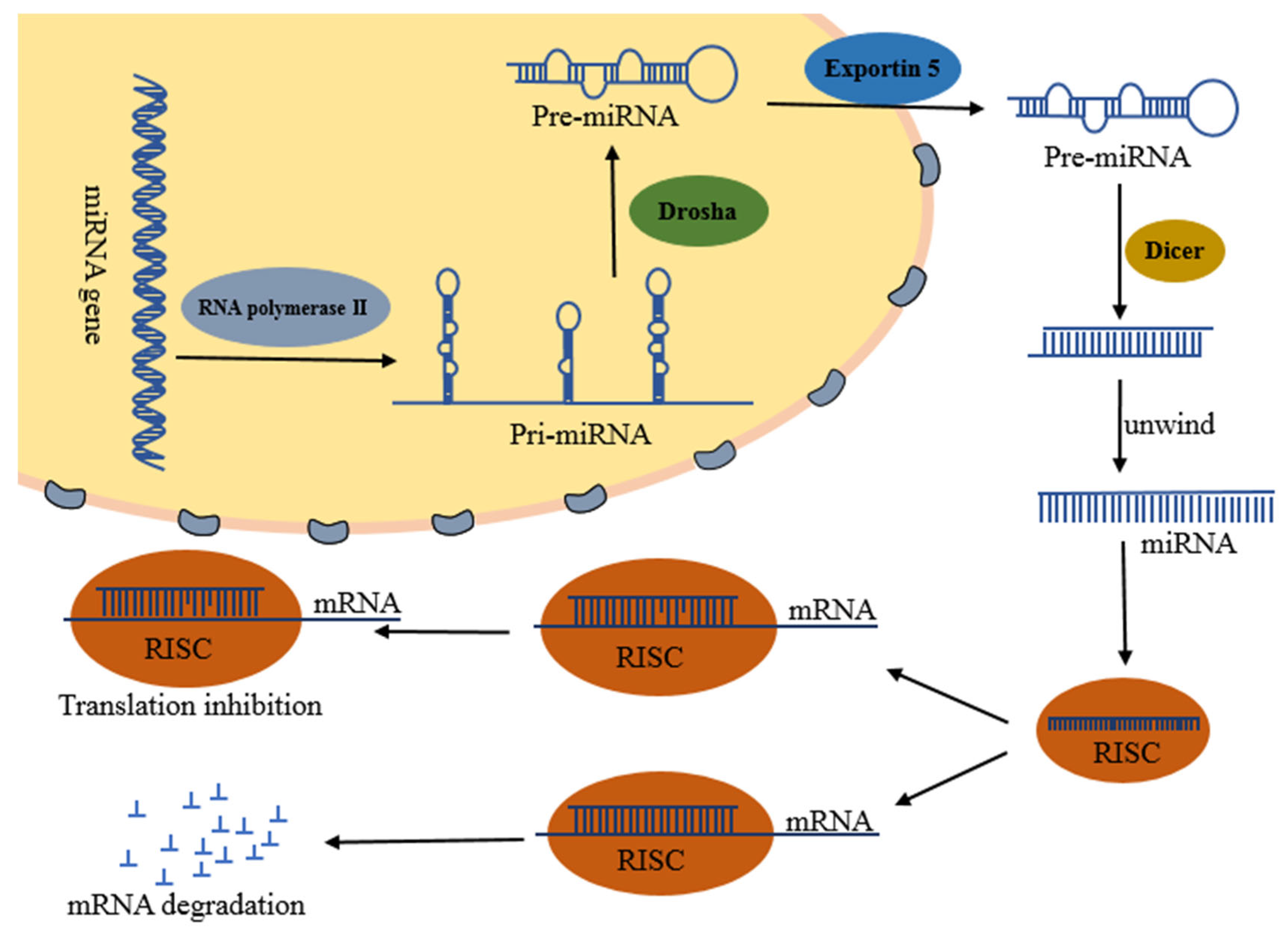
2. Biosynthesis and Functions of miRNAs
3. miRNAs and Cancer Diagnosis and Prognosis
3.1. Lung Cancer

{kind=link}
{kind=link}
{kind=link}
| miRNA | Sample | Expression | AUC | Biomarker | Reference |
|---|---|---|---|---|---|
| miR-708-5p | Tissue | ↑ | 0.925 | Diagnosis | [40] |
| miR-1247-5p | Serum | ↑ | 0.812 | Diagnosis | [41] |
| miR-301b-3p | Serum | ↑ | 0.788 | Diagnosis | [41] |
| miR-105-5p | Serum | ↑ | 0.793 | Diagnosis | [41] |
| miR-492 | Plasma | ↑ | 3-miR:0.828 | Diagnosis | [49] |
| miR-590-3p | Plasma | ↑ | 3-miR:0.828 | Diagnosis | [49] |
| miR-4507 | EBC | ↑ | 3-miR:0.837 | Diagnosis | [50] |
| miR-451a | EBC | ↑ | 3-miR:0.837 | Diagnosis | [50] |
| miR-483-5p | exosomes | ↑ | / | Diagnosis | [39] |
| miR-342-5p | exosomes | ↑ | / | Diagnosis | [39] |
| miR-520c-3p | exosomes | ↑ | 2-miR:0.857 | Diagnosis | [51] |
| miR-1274b | exosomes | ↑ | 2-miR:0.857 | Diagnosis | [51] |
| miR-96 | exosomes | ↑ | 0.9735 | Diagnosis/Prognosis | [52] |
| miR-1276 | Tissue | ↑ | / | Prognosis | [46] |
| miR-767-3p | Tissue | ↑ | / | Prognosis | [46] |
| miR-767-5p | Tissue | ↑ | / | Prognosis | [46] |
| miR-10b | Tissue | ↑ | / | Prognosis | [53] |
| miR-135b | Tissue | ↑ | / | Prognosis | [54] |
| miR-142-3p | Tissue | ↑ | / | Prognosis | [55] |
| miR-196a | Tissue | ↑ | / | Prognosis | [56] |
| miR-202 | Plasma | ↑ | / | Prognosis | [57] |
| miR-17 | Tissue | ↓ | 0.692 | Diagnosis | [38] |
| miR-125b-5p | Tissue | ↓ | 0.768 | Diagnosis/Prognosis | [44] |
| miR-631 | Plasma | ↓ | 3-miR:0.828 | Diagnosis | [49] |
| miR-6777-5p | EBC | ↓ | 3-miR:0.837 | Diagnosis | [50] |
| miR-23a | exosomes | ↓ | 0.744 | Diagnosis | [58] |
| miR-let7i | exosomes | ↓ | 0.733 | Diagnosis | [58] |
| miR-203 | Tissue | ↓ | / | Prognosis | [53] |
| miR-320a | Serum | ↓ | / | Prognosis | [47] |
3.2. Liver Cancer
| miRNA | Sample | Expression | AUC | Biomarker | Reference |
|---|---|---|---|---|---|
| miR-452-5p | Tissue | ↑ | 0.83 | Diagnosis/Prognosis | [62] |
| miR-4661-5p | Tissue | ↑ | 0.725 | Diagnosis/Prognosis | [62] |
| miR-760 | Tissue/Serum | ↑ | 0.707 | Diagnosis/Prognosis | [66] |
| miR-7-5p | Tissue/Serum | ↑ | 0.641 | Diagnosis/Prognosis | [66] |
| miR-27a | exosomes/Tissue | ↑ | 0.8282 | Diagnosis/Prognosis | [63] |
| miR-18a | exosomes/Tissue | ↑ | 3-miR:0.904 | Diagnosis/Prognosis | [63] |
| miR-20b | exosomes/Tissue | ↑ | 3-miR:0.904 | Diagnosis/Prognosis | [63] |
| miR-221 | exosomes/Tissue | ↑ | 3-miR:0.904 | Diagnosis/Prognosis | [63] |
| miR-184 | Serum | ↑ | 6-miR:0.9535 | Diagnosis | [64] |
| miR-532-5p | Serum | ↑ | 6-miR:0.9535 | Diagnosis | [64] |
| miR-221-3p | Serum | ↑ | 6-miR:0.9535 | Diagnosis | [64] |
| miR-200 | Serum | ↑ | 4-miR:0.92 | Diagnosis | [65] |
| miR-21 | Serum | ↑ | 4-miR:0.92 | Diagnosis | [65] |
| miR-355 | Serum | ↑ | 4-miR:0.92 | Diagnosis | [65] |
| miR-1293 | TEP miRNA | ↑ | 0.78 | Diagnosis | [70] |
| miR-3200-3p | Tissue | ↑ | / | Prognosis | [67] |
| miR-3690 | Tissue | ↑ | / | Prognosis | [67] |
| miR-1269a | Tissue | ↑ | / | Prognosis | [69] |
| miR-421 | Tissue | ↑ | / | Prognosis | [69] |
| miR-326 | Tissue | ↑ | / | Prognosis | [71] |
| miR-21 | Tissue | ↑ | / | Prognosis | [71] |
| miR-212-3p | Tissue | ↑ | / | Prognosis | [72] |
| miR-25 | Tissue | ↑ | / | Prognosis | [73] |
| let-7e | Tissue/Cell | ↑ | / | Prognosis | [74] |
| let-7e | exosomes/Tissue | ↑ | / | Prognosis | [63] |
| miR-652 | exosomes/Tissue | ↑ | / | Prognosis | [63] |
| miR-638 | Cell/exosomes | ↑ | / | Prognosis | [68] |
| miR-5589-3p | Tissue | ↓ | 0.838 | Diagnosis/Prognosis | [62] |
| miR-5589-5p | Tissue | ↓ | 0.879 | Diagnosis/Prognosis | [62] |
| miR-139-3p | Tissue/Serum | ↓ | 0.706 | Diagnosis/Prognosis | [66] |
| miR-5589-5p | Serum | ↓ | 6-miR:0.9535 | Diagnosis | [64] |
| miR-26b-3p | Serum | ↓ | 6-miR:0.9535 | Diagnosis | [64] |
| let-7b-3p | Serum | ↓ | 6-miR:0.9535 | Diagnosis | [64] |
| miR-29a | Serum | ↓ | 4-miR:0.92 | Diagnosis | [65] |
| miR-495-3p | TEP miRNA | ↓ | 0.76 | Diagnosis | [70] |
| miR-125b | exosomes | ↓ | / | Diagnosis | [75] |
| miR-144/451a cluster | Tissue | ↓ | / | Prognosis | [76] |
| miR-140 | Tissue | ↓ | / | Prognosis | [77] |
| mir-150-3p | Tissue/exosomes | ↓ | / | Prognosis | [78] |
3.3. Gastric Cancer
| miRNA | Sample | Expression | AUC | Biomarker | Reference |
|---|---|---|---|---|---|
| miR-455-3p | Tissue | ↑ | 3-miR:0.91 | Diagnosis | [88] |
| miR-135b-5p | Tissue | ↑ | 3-miR:0.91 | Diagnosis | [88] |
| let-7a-3p | Tissue | ↑ | 3-miR:0.91 | Diagnosis | [88] |
| miR-3185 | Tissue/Plasma | ↑ | 4-miR:0.825 | Diagnosis | [83] |
| miR-6083 | Tissue/Plasma | ↑ | 4-miR:0.825 | Diagnosis | [83] |
| miR-6792-3p | Tissue/Plasma | ↑ | 4-miR:0.825 | Diagnosis | [83] |
| miR-659-3p | Tissue/Plasma | ↑ | 4-miR:0.825 | Diagnosis | [83] |
| miR-140 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-183 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-30e | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-103a | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-93 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-142 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-21 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-29c | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-424 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-340 | Serum | ↑ | 12-miR:0.848 | Diagnosis | [84] |
| miR-1290 | Serum | ↑ | 0.6576 | Diagnosis | [89] |
| miR-320a | Serum | ↑ | ≥0.95 | Diagnosis | [90] |
| miR-1260b | Serum | ↑ | ≥0.95 | Diagnosis | [90] |
| miR-6515-5p | Serum | ↑ | ≥0.95 | Diagnosis | [90] |
| miR-130b | Plasma | ↑ | 0.911 | Diagnosis | [79] |
| miR-10a-5p | exosomes | ↑ | 0.801 | Diagnosis | [82] |
| miR-19b-3p | exosomes | ↑ | 0.721 | Diagnosis | [82] |
| miR-215-5p | exosomes | ↑ | 0.78 | Diagnosis | [82] |
| miR-18a-5p | exosomes | ↑ | 0.736 | Diagnosis | [82] |
| miR-145-3p | Tissue | ↑ | / | Prognosis | [85] |
| miR-328-3p | Tissue | ↑ | / | Prognosis | [85] |
| miR-125b-5p | Tissue | ↑ | / | Prognosis | [85] |
| miR-99a-3p | Tissue | ↑ | / | Prognosis | [85] |
| miR-133a-5p | Tissue | ↑ | / | Prognosis | [85] |
| miR-1292-5p | Tissue | ↑ | / | Prognosis | [85] |
| miR-196b-3p | Tissue | ↑ | / | Prognosis | [86] |
| miR-548v | Tissue | ↑ | / | Prognosis | [86] |
| miR-380-3p | Tissue | ↑ | / | Prognosis | [86] |
| miR-1275 | Tissue | ↑ | / | Prognosis | [86] |
| miR126-3p | Tissue | ↑ | / | Prognosis | [87] |
| miR-143-5p | Tissue | ↑ | / | Prognosis | [87] |
| miR-424-5p | Tissue | ↑ | / | Prognosis | [91] |
| let-7a-5p | Tissue | ↑ | / | Prognosis | [91] |
| miR-27a-3p | Tissue | ↑ | / | Prognosis | [91] |
| miR-126-5p | Tissue | ↑ | / | Prognosis | [91] |
| miR-182 | / | ↑ | / | Prognosis | [92] |
| miR-204-5p | Tissue | ↓ | 4-miR:0.94 | Diagnosis | [88] |
| miR-149-5p | Tissue | ↓ | 4-miR:0.94 | Diagnosis | [88] |
| miR-143-3p | Tissue | ↓ | 4-miR:0.94 | Diagnosis | [88] |
| miR-195-5p | Tissue | ↓ | 4-miR:0.94 | Diagnosis | [88] |
| miR-936 | Tissue/Plasma | ↓ | 2-miR:0.73 | Diagnosis | [83] |
| miR-1306-3p | Tissue/Plasma | ↓ | 2-miR:0.73 | Diagnosis | [83] |
| miR-181a | Serum | ↓ | 12-miR:0.848 | Diagnosis | [84] |
| miR-126 | Serum | ↓ | 12-miR:0.848 | Diagnosis | [84] |
| miR-1343-3p | Serum | ↓ | 1.000 | Diagnosis | [93] |
| miR-590-5p | exosomes | ↓ | 0.81 | Diagnosis/Prognosis | [94] |
| miR-92b-5p | Tissue | ↓ | / | Prognosis | [85] |
| miR-942-3p | Tissue | ↓ | / | Prognosis | [85] |
| miR-675-3p | Tissue | ↓ | / | Prognosis | [85] |
| miR-125b-5p | Tissue | ↓ | / | Prognosis | [86] |
| miR-99a-3p | Tissue | ↓ | / | Prognosis | [86] |
| miR-100-5p | Tissue | ↓ | / | Prognosis | [86] |
| miR-363-3p | Tissue | ↓ | / | Prognosis | [86] |
| miR-1275 | Tissue | ↓ | / | Prognosis | [87] |
| miR-23b | Tissue | ↓ | / | Prognosis | [95] |
| miR-194 | Tissue/Cell | ↓ | / | Prognosis | [96] |
| miR-339 | Tissue/Cell | ↓ | / | Prognosis | [97] |
| miR-148a | Plasma | ↓ | / | Prognosis | [98] |
3.4. Colorectal Cancer
| miRNA | Sample | Expression | AUC | Biomarker | Reference |
|---|---|---|---|---|---|
| miR-1290 | Serum | ↑ | 0.7852 | Diagnosis | [89] |
| miR-19a-3p | Serum | ↑ | 0.84 | Diagnosis | [104] |
| miR-203-3p | Serum | ↑ | 0.83 | Diagnosis | [104] |
| miR-221-3p | Serum | ↑ | 0.88 | Diagnosis | [104] |
| let-7f-5p | Serum | ↑ | 0.73 | Diagnosis | [104] |
| miR-21 | Serum/Plasma | ↑ | 0.87 | Diagnosis | [109] |
| let-7e-5p | Plasma/Tissue | ↑ | 4-miR: | Diagnosis | [101] |
| miR-106a-5p | Plasma/Tissue | ↑ | 0.716(Plasma); | Diagnosis | [101] |
| miR-28-3p | Plasma/Tissue | ↑ | 0.998(Tissue) | Diagnosis | [101] |
| miR-542-5p | Plasma/Tissue | ↑ | Diagnosis | [101] | |
| miR-210 | Plasma | ↑ | 2-miR:0.731 | Diagnosis | [103] |
| miR-21 | Plasma | ↑ | 2-miR:0.731 | Diagnosis | [103] |
| miR-203 | Plasma | ↑ | 2-miR:0.833 | Diagnosis | [103] |
| miR-210 | Plasma | ↑ | 2-miR:0.833 | Diagnosis | [103] |
| miR-15b | exosomes | ↑ | 0.82 | Diagnosis | [100] |
| miR-16 | exosomes | ↑ | 0.58 | Diagnosis | [100] |
| miR-21 | exosomes | ↑ | 0.75 | Diagnosis | [100] |
| miR-31 | exosomes | ↑ | 0.75 | Diagnosis | [100] |
| miR-183 | Tissue | ↑ | / | Prognosis | [99] |
| miR-20a | Tissue | ↑ | / | Prognosis | [99] |
| miR-21 | Tissue | ↑ | / | Prognosis | [99] |
| miR-216a-5p | Tissue | ↑ | / | Prognosis | [105] |
| let-7c | Tissue | ↑ | / | Prognosis | [110] |
| let-7e | Tissue | ↑ | / | Prognosis | [110] |
| miR-34c | Tissue | ↑ | / | Prognosis | [110] |
| miR-133b | Tissue | ↑ | / | Prognosis | [110] |
| miR-21-5p | Plasma | ↑ | / | Prognosis | [108] |
| let-7g | exosomes | ↑ | / | Prognosis | [107] |
| miR-96 | Plasma | ↑ | 2-miR:0.93 | Diagnosis/Prognosis | [102] |
| miR-99b | Plasma | ↓ | 2-miR:0.93 | Diagnosis/Prognosis | [102] |
| miR-381-3p | exosomes | ↓ | 2-miR:0.807 | Diagnosis | [111] |
| miR-377-3p | exosomes | ↓ | 2-miR:0.807 | Diagnosis | [111] |
| miR-195 | Tissue | ↓ | / | Prognosis | [99] |
| miRN-139 | Tissue | ↓ | / | Prognosis | [99] |
| miR-145 | Tissue | ↓ | / | Prognosis | [99] |
| miR-194-3p | Tissue | ↓ | / | Prognosis | [105] |
| miR-3677-3p | Tissue | ↓ | / | Prognosis | [105] |
| miR-449a | Tissue | ↓ | / | Prognosis | [106] |
| miR-106a | Tissue | ↓ | / | Prognosis | [110] |
| miR-144 | Tissue | ↓ | / | Prognosis | [110] |
| miR-100 | Tissue | ↓ | / | Prognosis | [112] |
| miR-99a | Tissue | ↓ | / | Prognosis | [112] |
| miR-33b-5p | Tissue | ↓ | / | Prognosis | [113] |
| miR-193a | exosomes | ↓ | / | Prognosis | [107] |
3.5. Breast Cancer
| miRNA | Sample | Expression | AUC | Biomarker | Reference |
|---|---|---|---|---|---|
| let-7b-5p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-106a-5p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-19a-3p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-19b-3p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-20a-5p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-223-3p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-25-3p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-425-5p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-451a | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-92a-3p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-93-5p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-16-5p | Serum/Tissue/exosomes | ↑ | >0.94 | Diagnosis | [125] |
| miR-451a | Serum | ↑ | 6-miR:0.881 | Diagnosis | [126] |
| miR-195-5p | Serum | ↑ | 6-miR:0.881 | Diagnosis | [126] |
| miR-126-5p | Serum | ↑ | 6-miR:0.881 | Diagnosis | [126] |
| miR-30b-5p | Plasma | ↑ | 2-miR:0.9273 | Diagnosis | [116] |
| miR-99a-5p | Plasma | ↑ | 2-miR:0.9273 | Diagnosis | [116] |
| miR-145 | Plasma | ↑ | 4-miR:0.97 | Diagnosis | [117] |
| miR-139-5p | Plasma | ↑ | 4-miR:0.97 | Diagnosis | [117] |
| miR-130a | Plasma | ↑ | 4-miR:0.97 | Diagnosis | [117] |
| miR-425-5p | Plasma | ↑ | 4-miR:0.97 | Diagnosis | [117] |
| pri-miR-526b | Plasma | ↑ | 0.7273 | Diagnosis | [118] |
| miR-19a | Plasma | ↑ | 4-miR:0.802 | Diagnosis | [127] |
| miR-20a | Plasma | ↑ | 4-miR:0.802 | Diagnosis | [127] |
| miR-421 | exosomes | ↑ | 0.835 | Diagnosis | [128] |
| miR-128 | exosomes | ↑ | 0.825 | Diagnosis | [128] |
| miR-16 | EV | ↑ | 4-miR:0.88 | Diagnosis | [119] |
| miR-21 | EV | ↑ | 4-miR:0.88 | Diagnosis | [119] |
| miR-9 | EV | ↑ | 4-miR:0.88 | Diagnosis | [119] |
| miR-429 | EV | ↑ | 4-miR:0.88 | Diagnosis | [119] |
| miR-10b | Tissue | ↑ | / | Prognosis | [53] |
| miR-210 | Tissue | ↑ | / | Prognosis | [121] |
| miR-378c | Tissue | ↑ | / | Prognosis | [122] |
| let-7f-5p | Tissue | ↑ | / | Prognosis | [122] |
| miR-1268b | Tissue | ↑ | / | Prognosis | [122] |
| miR-200c-3p | Tissue | ↑ | / | Prognosis | [122] |
| miR-1271-3p | Tissue | ↑ | / | Prognosis | [122] |
| miR-200c-3p | Tissue | ↑ | / | Prognosis | [123] |
| miR-214-3p | Tissue | ↑ | / | Prognosis | [123] |
| miR-23a-3p | Tissue | ↑ | / | Prognosis | [123] |
| miR-106b-5p | Tissue | ↑ | / | Prognosis | [128] |
| miR-93 | Serum | ↑ | / | Prognosis | [129] |
| miR-210 | Serum | ↑ | / | Prognosis | [129] |
| miR-19a | Serum | ↑ | / | Prognosis | [129] |
| miR-19b | Serum | ↑ | / | Prognosis | [129] |
| miR379/656 cluster | Tissue | ↓ | 0.9843 | Diagnosis/ Prognosis | [120] |
| miR-423-3p | Serum | ↓ | 6-miR:0.881 | Diagnosis | [126] |
| miR-192-5p | Serum | ↓ | 6-miR:0.881 | Diagnosis | [126] |
| miR-17-5p | Serum | ↓ | 6-miR:0.881 | Diagnosis | [126] |
| miR-126 | Plasma | ↓ | 4-miR:0.802 | Diagnosis | [127] |
| miR-155 | Plasma | ↓ | 4-miR:0.802 | Diagnosis | [127] |
| miR-203 | Tissue | ↓ | / | Prognosis | [53] |
| miR-574 | Tissue | ↓ | / | Prognosis | [121] |
| miR-224 | Tissue | ↓ | / | Prognosis | [121] |
| miR-30b | Tissue | ↓ | / | Prognosis | [121] |
| miR-130a | Tissue | ↓ | / | Prognosis | [121] |
| miR-1200 | Tissue | ↓ | / | Prognosis | [122] |
| miR-1249-3p | Tissue | ↓ | / | Prognosis | [122] |
| miR-1255b-5p | Tissue | ↓ | / | Prognosis | [122] |
| miR-520d | Tissue | ↓ | / | Prognosis | [122] |
| miR-527 | Tissue | ↓ | / | Prognosis | [122] |
| miR-518a-5p | Tissue | ↓ | / | Prognosis | [122] |
| miR-2117 | Tissue | ↓ | / | Prognosis | [122] |
| miR-638 | Tissue | ↓ | / | Prognosis | [123] |
| miR-451a | Tissue | ↓ | / | Prognosis | [123] |
| miR-495-3p | Tissue | ↓ | / | Prognosis | [124] |
| miR-223 | Tissue | ↓ | / | Prognosis | [130] |
| miR-34a | Tissue | ↓ | / | Prognosis | [131] |
| miR-200c | Tissue | ↓ | / | Prognosis | [131] |
| miR-363-5p | Tissue/exosomes | ↓ | / | Prognosis | [132] |
3.6. Prostate Cancer
| miRNA | Sample | Expression | AUC | Biomarker | Reference |
|---|---|---|---|---|---|
| miR-3195 | Tissue | ↑ | 3-miR:0.994 | Diagnosis | [139] |
| miR-4417 | Tissue | ↑ | 3-miR:0.994 | Diagnosis | [139] |
| miR-301a | Serum/Tissue | ↑ | / | Diagnosis | [144] |
| miR-4732-3p | Plasma | ↑ | 2-miR:0.8 | Diagnosis | [136] |
| miR-5100 | Plasma | ↑ | / | Diagnosis | [135] |
| miR-1255-5p | Plasma | ↑ | 0.885 | Diagnosis | [145] |
| miR-181a-5p | exosomes | ↑ | 0.738 | Diagnosis | [138] |
| miR-451a | Urine exosomes | ↑ | 0.757 | Diagnosis | [146] |
| miR-486-3p | Urine exosomes | ↑ | 0.704 | Diagnosis | [146] |
| miR-486-5p | Urine exosomes | ↑ | 0.796 | Diagnosis | [146] |
| miR-6078 | Urine | ↑ | 0.7 | Diagnosis | [137] |
| miR-1913 | Urine | ↑ | 2-miR:0.821 | Diagnosis | [147] |
| miR-3659 | Urine | ↑ | 2-miR:0.821 | Diagnosis | [147] |
| miR-451a | SEVs | ↑ | 0.65 | Diagnosis | [148] |
| miR-141 | SEVs | ↑ | 0.64 | Diagnosis | [148] |
| miR-145 | SEVs | ↑ | 0.76 | Diagnosis | [148] |
| miR-221 | SEVs | ↑ | 0.7 | Diagnosis | [148] |
| miR-17-5p | Tissue | ↑ | / | Prognosis | [140] |
| miR-222-3p | Tissue | ↑ | / | Prognosis | [142] |
| miR-582-5p | Tissue | ↑ | / | Prognosis | [142] |
| miR-582-3p | Tissue | ↑ | / | Prognosis | [142] |
| miR-505-3p | Tissue | ↑ | / | Prognosis | [142] |
| miR-326 | Tissue | ↑ | / | Prognosis | [142] |
| miR-212-3p | Tissue | ↑ | / | Prognosis | [142] |
| miR-296-5p | Tissue | ↑ | / | Prognosis | [142] |
| miR-144-3p | Tissue | ↑ | / | Prognosis | [142] |
| miR-532-5p | Urine exosomes | ↑ | / | Prognosis | [143] |
| miR-425-5p | Cell exosomes | ↑ | / | Prognosis | [149] |
| miR-205 | Tissue | ↓ | 3-miR:0.994 | Diagnosis | [139] |
| miR-26b-5p | Plasma | ↓ | 2-miR:0.944 | Diagnosis | [136] |
| miR-98-5p | Plasma | ↓ | 2-miR:0.944 | Diagnosis | [136] |
| miR-26b-5p | Plasma | ↓ | 2-miR:0.8 | Diagnosis | [136] |
| miR-15a-5p | Urine | ↓ | 0.71 | Diagnosis | [137] |
| miR-3126-3p | Urine | ↓ | 0.76 | Diagnosis | [137] |
| miR-324-5p | Urine | ↓ | 0.74 | Diagnosis | [137] |
| miR-150-5p | Urine | ↓ | 0.76 | Diagnosis | [137] |
| miR-425-3p | Urine | ↓ | 0.71 | Diagnosis | [137] |
| miR-375 | Urine exosomes | ↓ | 0.788 | Diagnosis | [146] |
| miR-199b-3p | Tissue | ↓ | / | Prognosis | [141] |
| miR-21-5p | Tissue | ↓ | / | Prognosis | [142] |
| miR-192-5p | Tissue | ↓ | / | Prognosis | [142] |
| miR-15b-5p | Tissue | ↓ | / | Prognosis | [142] |
| miR-106b-5p | Tissue | ↓ | / | Prognosis | [142] |
| miR181a-5p | Tissue | ↓ | / | Prognosis | [142] |
| miR-18a-5p | Tissue | ↓ | / | Prognosis | [142] |
| miR-301a-3p | Tissue | ↓ | / | Prognosis | [142] |
4. Conclusions and Prospects
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| miRNAs(miR) | MicroRNAs |
| ncRNAs | non-coding RNAs |
| IARC | International Agency for Research on Cancer |
| NCC | National Cancer Center of China |
| CT | Computed Tomography |
| MRI | magnetic resonance |
| PET | Positron emission computed tomography |
| CEA | carcinoembryonic antigen |
| AFP | alpha-fetoprotein |
| PSA | Prostate cancer specific antigen |
| CTC | circulating tumor cells |
| NSCLC | non-small cell lung cancer |
| RISC | RNA induced silencing complex |
| pri-miRNA | primary miRNA |
| pre-miRNA | precursor miRNA |
| UTR | untranslated region |
| PTGES3 | prostaglandin E synthase 3 |
| FAP | ibroblast activation protein |
| PD1 | programmed cell death 1 |
| PDL1 | programmed death ligand 1 |
| LUAD | lung adenocarcinoma |
| LUSC | lung squamous cell carcinoma |
| CSF | cerebrospinal fluid |
| ROC | receiver operating characteristic |
| AUC | area under the curve |
| PTEN | phosphatase and tensin homolog |
| HCC | hepatocellular carcinoma |
| DFS | disease-free survival |
| GC | Gastric cancer |
| ImmiRSig | immune-related nine-miRNA signature |
| GIMiSig | GI-related miRNA signature |
| CRC | Colorectal cancer |
| IAMIPS | immune-associated miRNA prognostic signature |
| PTM | peritoneal metastasis |
| LM | Leptomeningeal metastasis |
| BC | breast cancer |
| TCGA | The Cancer Genome Atlas |
| GEO | Gene Expression Omnibus |
| PCa | Prostatic cancer |
| BPH | benign prostatic hyperplasia |
| PSA | prostate specific antigen |
| ADT | androgen-deprivation therapy |
| CRPC | castration-resistant prostate cancer |
| BF | biochemical disorder |
| CF | clinical failure |
| PFS | progression-free survival |
| RFS | relapse free survival |
| BRC | biochemical relapse |
| RP | radical prostatectomy |
| SERS-LFA | surface-enhanced Raman scattering-lateral flow assay |
| TEP | tumor-educated platelet |
| SEVs | small extracellular vesicles |
| EV | extracellular vesicles |
| EBC | exhaled breath condensate |
| ACP | acid phosphatase |
| ER | estrogen receptor |
| PR | progesterone receptor |
| DRE | digital rectal examination |
| FOBT | fecal occult blood test |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Dong, X.; Li, H.; Cao, M.; Sun, D.; He, S.; Yang, F.; Yan, X.; Zhang, S.; Li, N.; et al. Cancer statistics in China and United States, 2022: Profiles, trends, and determinants. Chin. Med. J. 2022, 135, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef] [PubMed]
- Jafari, S.H.; Saadatpour, Z.; Salmaninejad, A.; Momeni, F.; Mokhtari, M.; Nahand, J.S.; Rahmati, M.; Mirzaei, H.; Kianmehr, M. Breast cancer diagnosis: Imaging techniques and biochemical markers. J. Cell. Physiol. 2018, 233, 5200–5213. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.K.; Ganeshan, D.; Jensen, C.T.; Devine, C.E. Imaging and Management of Bladder Cancer. Cancers 2021, 13, 1396. [Google Scholar] [CrossRef]
- Li, C.; Zhang, D.; Pang, X.; Pu, H.; Lei, M.; Fan, B.; Lv, J.; You, D.; Li, Z.; Zhang, T. Trajectories of Perioperative Serum Tumor Markers and Colorectal Cancer Outcomes: A Retrospective, Multicenter Longitudinal Cohort Study. EBioMedicine 2021, 74, 103706. [Google Scholar] [CrossRef]
- Sarwar, S.; Adil, M.A.; Nyamath, P.; Ishaq, M. Biomarkers of Prostatic Cancer: An Attempt to Categorize Patients into Prostatic Carcinoma, Benign Prostatic Hyperplasia, or Prostatitis Based on Serum Prostate Specific Antigen, Prostatic Acid Phosphatase, Calcium, and Phosphorus. Prost. Cancer 2017, 2017, 5687212. [Google Scholar] [CrossRef]
- Wang, W.; Xu, X.; Tian, B.; Wang, Y.; Du, L.; Sun, T.; Shi, Y.; Zhao, X.; Jing, J. The diagnostic value of serum tumor markers CEA, CA19-9, CA125, CA15-3, and TPS in metastatic breast cancer. Clin. Chim. Acta Int. J. Clin. Chem. 2017, 470, 51–55. [Google Scholar] [CrossRef]
- Xia, Y.; Hu, X.; Di, K.; Liu, C.; Tan, T.; Lin, Y.; Xu, H.; Xie, H.; Wang, S.; Yang, Z.; et al. Combined Detection of Exosome Concentration and Tumor Markers in Gastric Cancer. J. Biomed. Nanotechnol. 2020, 16, 252–258. [Google Scholar] [CrossRef]
- Broggi, G.; Salvatorelli, L. Bio-Pathological Markers in the Diagnosis and Therapy of Cancer. Cancers 2020, 12, 3113. [Google Scholar] [CrossRef]
- Yang, Q.Z.; Qi, C.B.; Xu, M.L.; Yue, J.Q.; Guo, F. Easily misdiagnosed pulmonary benign metastasizing leiomyoma with rich-mucus degeneration in intraoperative pathological section: Report of a case. Zhonghua Bing Li Xue Za Zhi Chin. J. Pathol. 2021, 50, 1177–1179. [Google Scholar] [CrossRef]
- Ning, D.; Cui, K.; Liu, M.; Ou, Y.; Wang, Z.; Zou, B.; Shen, Y.; Lu, X.; Li, S.; Li, P. Comparison of CellSearch and Circulating Tumor Cells (CTC)-Biopsy Systems in Detecting Peripheral Blood Circulating Tumor Cells in Patients with Gastric Cancer. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e926565. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.; Nedosekin, D.A.; Galanzha, E.I.; Zharov, V.P. Detection of Apoptotic Circulating Tumor Cells Using in vivo Fluorescence Flow Cytometry. Cytom. Part A J. Int. Soc. Anal. Cytol. 2019, 95, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Bizzarro, T.; Bernardi, L.; Buda, R.; Rossi, G. Cytological diagnosis of a rare synchronous non-small cell lung cancer metastatic to the thyroid gland. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2020, 31, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Wang, P.; Shang, D.; Liu, Y. Spatial-domain low-coherence quantitative phase microscopy to improve the cytological diagnosis of pancreatic cancer. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2020, 68, 60–67. [Google Scholar] [CrossRef]
- Halpern, J.A.; Shoag, J.E.; Mittal, S.; Oromendia, C.; Ballman, K.V.; Hershman, D.L.; Wright, J.D.; Shih, Y.T.; Nguyen, P.L.; Hu, J.C. Prognostic Significance of Digital Rectal Examination and Prostate Specific Antigen in the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Arm. J. Urol. 2017, 197, 363–368. [Google Scholar] [CrossRef]
- Ladabaum, U.; Dominitz, J.A.; Kahi, C.; Schoen, R.E. Strategies for Colorectal Cancer Screening. Gastroenterology 2020, 158, 418–432. [Google Scholar] [CrossRef]
- He, J.; Wu, F.; Han, Z.; Hu, M.; Lin, W.; Li, Y.; Cao, M. Biomarkers (mRNAs and Non-Coding RNAs) for the Diagnosis and Prognosis of Colorectal Cancer—From the Body Fluid to Tissue Level. Front. Oncol. 2021, 11, 632834. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Amin Mahdian, S.M.; Ebrahimi, M.S.; Taghizadieh, M.; Vosough, M.; Sadri Nahand, J.; Hosseindoost, S.; Vousooghi, N.; Javar, H.A.; Larijani, B.; et al. Microfluidics for detection of exosomes and microRNAs in cancer: State of the art. Mol. Ther. Nucleic Acids 2022, 28, 758–791. [Google Scholar] [CrossRef]
- Raza, A.; Khan, A.Q.; Inchakalody, V.P.; Mestiri, S.; Yoosuf, Z.; Bedhiafi, T.; El-Ella, D.M.A.; Taib, N.; Hydrose, S.; Akbar, S.; et al. Dynamic liquid biopsy components as predictive and prognostic biomarkers in colorectal cancer. J. Exp. Clin. Cancer Res. 2022, 41, 99. [Google Scholar] [CrossRef]
- Zhong, C.; Xie, Z.; Zeng, L.H.; Yuan, C.; Duan, S. MIR4435-2HG Is a Potential Pan-Cancer Biomarker for Diagnosis and Prognosis. Front. Immunol. 2022, 13, 855078. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef]
- Jet, T.; Gines, G.; Rondelez, Y.; Taly, V. Advances in multiplexed techniques for the detection and quantification of microRNAs. Chem. Soc. Rev. 2021, 50, 4141–4161. [Google Scholar] [CrossRef]
- Tang, L. Recapitulating miRNA biogenesis in cells. Nat. Methods 2022, 19, 35. [Google Scholar] [CrossRef]
- Ho, P.T.B.; Clark, I.M.; Le, L.T.T. MicroRNA-Based Diagnosis and Therapy. Int. J. Mol. Sci. 2022, 23, 7167. [Google Scholar] [CrossRef]
- Xuan, J.; Liu, Y.; Zeng, X.; Wang, H. Sequence Requirements for miR-424-5p Regulating and Function in Cancers. Int. J. Mol. Sci. 2022, 23, 4037. [Google Scholar] [CrossRef]
- Bazzini, A.A.; Lee, M.T.; Giraldez, A.J. Ribosome profiling shows that miR-430 reduces translation before causing mRNA decay in zebrafish. Science 2012, 336, 233–237. [Google Scholar] [CrossRef]
- Huntzinger, E.; Izaurralde, E. Gene silencing by microRNAs: Contributions of translational repression and mRNA decay. Nat. Rev. Genet. 2011, 12, 99–110. [Google Scholar] [CrossRef]
- Park, J.H.; Shin, C. MicroRNA-directed cleavage of targets: Mechanism and experimental approaches. BMB Rep. 2014, 47, 417–423. [Google Scholar] [CrossRef]
- Subtelny, A.O.; Eichhorn, S.W.; Chen, G.R.; Sive, H.; Bartel, D.P. Poly(A)-tail profiling reveals an embryonic switch in translational control. Nature 2014, 508, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; Dandona, L.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef]
- Ding, H.; Wang, Y.; Cui, Y.; Chen, Z.; Li, Y.; Yang, J.; Yang, Y.; Chen, T.; Xia, D.; Li, C.; et al. Comprehensive analysis of the expression and prognosis for RBR E3 ubiquitin ligases in lung adenocarcinoma. Thorac. Cancer 2022, 13, 2459–2472. [Google Scholar] [CrossRef]
- Gao, P.; Zou, K.; Xiao, L.; Zhou, H.; Xu, X.; Zeng, Z.; Zhang, W. High expression of PTGES3 is an independent predictive poor prognostic biomarker and correlates with immune infiltrates in lung adenocarcinoma. Int. Immunopharmacol. 2022, 110, 108954. [Google Scholar] [CrossRef]
- Yanagawa, N.; Sugai, M.; Shikanai, S.; Sugimoto, R.; Osakabe, M.; Uesugi, N.; Saito, H.; Maemondo, M.; Sugai, T. High expression of fibroblast-activating protein is a prognostic marker in non-small cell lung carcinoma. Thorac. Cancer 2022, 13, 2377–2384. [Google Scholar] [CrossRef]
- Wang, Y.; He, H. Prognostic value of soluble programmed cell death ligand-1 in patients with non-small-cell lung cancer: A meta-analysis. Immunotherapy 2022, 14, 945–956. [Google Scholar] [CrossRef]
- Yamaguchi, O.; Kaira, K.; Naruse, I.; Umeda, Y.; Honda, T.; Watanabe, S.; Ichikawa, K.; Tateishi, K.; Kasahara, N.; Higuchi, T.; et al. Prospective assessment using (18)F-FDG PET/CT as a novel predictor for early response to PD-1 blockade in non-small-cell lung cancer. Sci. Rep. 2022, 12, 11832. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Migdalska-Sęk, M.; Modrzewska, B.; Kordiak, J.; Pastuszak-Lewandoska, D.; Kiszałkiewicz, J.M.; Bielec, F.; Antczak, A.; Brzeziańska-Lasota, E. Diagnostic value of PPARδ and miRNA-17 expression levels in patients with non-small cell lung cancer. Sci. Rep. 2021, 11, 24136. [Google Scholar] [CrossRef]
- Xu, Q.; Ye, L.; Huang, L.; Zhou, L.; Chen, X.; Ye, M.; Wu, G.; Zhan, P.; Lv, T.; Song, Y. Serum Exosomal miRNA Might Be a Novel Liquid Biopsy to Identify Leptomeningeal Metastasis in Non-Small Cell Lung Cancer. OncoTargets Ther. 2021, 14, 2327–2335. [Google Scholar] [CrossRef]
- Nie, R.; Niu, W.; Tang, T.; Zhang, J.; Zhang, X. Integrating microRNA expression, miRNA-mRNA regulation network and signal pathway: A novel strategy for lung cancer biomarker discovery. PeerJ 2021, 9, e12369. [Google Scholar] [CrossRef]
- Dong, X.; Chang, M.; Song, X.; Ding, S.; Xie, L.; Song, X. Plasma miR-1247-5p, miR-301b-3p and miR-105-5p as potential biomarkers for early diagnosis of non-small cell lung cancer. Thorac. Cancer 2021, 12, 539–548. [Google Scholar] [CrossRef]
- Klotz, L.V.; Courty, Y.; Lindner, M.; Petit-Courty, A.; Stowasser, A.; Koch, I.; Eichhorn, M.E.; Lilis, I.; Morresi-Hauf, A.; Arendt, K.A.M.; et al. Comprehensive clinical profiling of the Gauting locoregional lung adenocarcinoma donors. Cancer Med. 2019, 8, 1486–1499. [Google Scholar] [CrossRef]
- Jiang, X.; Yuan, Y.; Tang, L.; Wang, J.; Zhang, D.; Duan, L. Systematic Analysis and Validation of the Prognosis, Immunological Role and Biology Function of the Ferroptosis-Related lncRNA GSEC/miRNA-101-3p/CISD1 Axis in Lung Adenocarcinoma. Front. Mol. Biosci. 2021, 8, 793732. [Google Scholar] [CrossRef]
- Tang, L.; Yuan, Y.; Zhai, H.; Wang, J.; Zhang, D.; Liang, H.; Shi, Y.; Duan, L.; Jiang, X. MicroRNA-125b-5p Correlates with Prognosis and Lung Adenocarcinoma Progression. Front. Mol. Biosci. 2021, 8, 788690. [Google Scholar] [CrossRef]
- Yuan, Y.; Jiang, X.; Tang, L.; Wang, J.; Zhang, D.; Cho, W.C.; Duan, L. FOXM1/lncRNA TYMSOS/miR-214-3p-Mediated High Expression of NCAPG Correlates with Poor Prognosis and Cell Proliferation in Non-Small Cell Lung Carcinoma. Front. Mol. Biosci. 2021, 8, 785767. [Google Scholar] [CrossRef]
- Yang, J.; Hao, R.; Zhang, Y.; Deng, H.; Teng, W.; Wang, Z. Construction of circRNA-miRNA-mRNA network and identification of novel potential biomarkers for non-small cell lung cancer. Cancer Cell Int. 2021, 21, 611. [Google Scholar] [CrossRef]
- Khandelwal, A.; Sharma, U.; Barwal, T.S.; Seam, R.K.; Gupta, M.; Rana, M.K.; Vasquez, K.M.; Jain, A. Circulating miR-320a Acts as a Tumor Suppressor and Prognostic Factor in Non-small Cell Lung Cancer. Front. Oncol. 2021, 11, 645475. [Google Scholar] [CrossRef]
- Boldrini, L.; Giordano, M.; Melfi, F.; Lucchi, M.; Fontanini, G. Expression of miRNA-25 in young and old lung adenocarcinoma. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2021, 26, 132. [Google Scholar] [CrossRef]
- Duan, X.; Qiao, S.; Li, D.; Li, S.; Zheng, Z.; Wang, Q.; Zhu, X. Circulating miRNAs in Serum as Biomarkers for Early Diagnosis of Non-small Cell Lung Cancer. Front. Genet. 2021, 12, 673926. [Google Scholar] [CrossRef]
- Pérez-Sánchez, C.; Barbarroja, N.; Pantaleão, L.C.; López-Sánchez, L.M.; Ozanne, S.E.; Jurado-Gámez, B.; Aranda, E.; Lopez-Pedrera, C.; Rodríguez-Ariza, A. Clinical Utility of microRNAs in Exhaled Breath Condensate as Biomarkers for Lung Cancer. J. Pers. Med. 2021, 11, 111. [Google Scholar] [CrossRef]
- Zhong, Y.; Ding, X.; Bian, Y.; Wang, J.; Zhou, W.; Wang, X.; Li, P.; Shen, Y.; Wang, J.J.; Li, J.; et al. Discovery and validation of extracellular vesicle-associated miRNAs as noninvasive detection biomarkers for early-stage non-small-cell lung cancer. Mol. Oncol. 2021, 15, 2439–2452. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Ding, H.; Wang, L.; Yan, Y.; Wan, Y.; Yi, Y.; Tao, L.; Zhu, C. Circulating Exosomal miR-96 as a Novel Biomarker for Radioresistant Non-Small-Cell Lung Cancer. J. Oncol. 2021, 2021, 5893981. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.B.; Fan, R.H.; Qin, X.; Han, R.M. microRNA Prognostic Signature for Postoperative Success of Metastatic Orthopedic Cancers: Implications for Precision Microsurgery. Front. Cell Dev. Biol. 2021, 9, 704505. [Google Scholar] [CrossRef]
- Zhao, J.; Wang, X.; Mi, Z.; Jiang, X.; Sun, L.; Zheng, B.; Wang, J.; Meng, M.; Zhang, L.; Wang, Z.; et al. STAT3/miR-135b/NF-κB axis confers aggressiveness and unfavorable prognosis in non-small-cell lung cancer. Cell Death Dis. 2021, 12, 493. [Google Scholar] [CrossRef]
- Ye, Q.; Putila, J.; Raese, R.; Dong, C.; Qian, Y.; Dowlati, A.; Guo, N.L. Identification of Prognostic and Chemopredictive microRNAs for Non-Small-Cell Lung Cancer by Integrating SEER-Medicare Data. Int. J. Mol. Sci. 2021, 22, 7658. [Google Scholar] [CrossRef]
- Lee, S.; Hong, J.H.; Kim, J.S.; Yoon, J.S.; Chun, S.H.; Hong, S.A.; Kim, E.J.; Kang, K.; Lee Kang, J.; Ko, Y.H.; et al. Cancer-associated fibroblasts activated by miR-196a promote the migration and invasion of lung cancer cells. Cancer Lett. 2021, 508, 92–103. [Google Scholar] [CrossRef]
- Monastirioti, A.; Papadaki, C.; Rounis, K.; Kalapanida, D.; Mavroudis, D.; Agelaki, S. A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer. Cells 2021, 10, 1988. [Google Scholar] [CrossRef]
- Kryczka, J.; Migdalska-Sęk, M.; Kordiak, J.; Kiszałkiewicz, J.M.; Pastuszak-Lewandoska, D.; Antczak, A.; Brzeziańska-Lasota, E. Serum Extracellular Vesicle-Derived miRNAs in Patients with Non-Small Cell Lung Cancer-Search for Non-Invasive Diagnostic Biomarkers. Diagnostics 2021, 11, 425. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Yang, J.; Pan, G.; Guan, L.; Liu, Z.; Wu, Y.; Liu, Z.; Lu, W.; Li, S.; Xu, H.; Ouyang, G. The burden of primary liver cancer caused by specific etiologies from 1990 to 2019 at the global, regional, and national levels. Cancer Med. 2022, 11, 1357–1370. [Google Scholar] [CrossRef]
- Oura, K.; Morishita, A.; Masaki, T. Molecular and Functional Roles of MicroRNAs in the Progression of Hepatocellular Carcinoma-A Review. Int. J. Mol. Sci. 2020, 21, 8362. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xu, J.; Yi, Y.; Jiang, S.; Jin, P.; Xia, X.; Ma, F. Transcription Factors and Methylation Drive Prognostic miRNA Dysregulation in Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 691115. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Tang, S.; Shen, D.; Li, X.; Liang, L.; Ding, Y.; Xu, B. Circulating plasma exosomal miRNA profiles serve as potential metastasis-related biomarkers for hepatocellular carcinoma. Oncol. Lett. 2021, 21, 168. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Zhou, S.; Liang, H.; Ye, Q.; Wang, Y. Development and Validation of a Novel Circulating miRNA-Based Diagnostic Score for Early Detection of Hepatocellular Carcinoma. Dig. Dis. Sci. 2022, 67, 2283–2292. [Google Scholar] [CrossRef]
- Fouda, M.S.; Omran, M.M.; Tarek, G.; Hady, A.A.W.A. Development of a novel panel based on micro-RNAs (21, 29a, 200 and 335) and alpha-fetoprotein as diagnostic biomarkers for hepatocellular carcinoma associated with hepatitis C infection. Arab J. Gastroenterol. Off. Publ. Pan-Arab Assoc. Gastroenterol. 2021, 22, 28–33. [Google Scholar] [CrossRef]
- Zhang, X.; Ma, L.; Zhai, L.; Chen, D.; Li, Y.; Shang, Z.; Zhang, Z.; Gao, Y.; Yang, W.; Li, Y.; et al. Construction and validation of a three-microRNA signature as prognostic biomarker in patients with hepatocellular carcinoma. Int. J. Med. Sci. 2021, 18, 984–999. [Google Scholar] [CrossRef]
- Huang, X.C.; Pang, F.X.; Ou, S.S.; Wei, X.J.; Xu, Y.J.; Lai, Y.H. Risk Score Based on Two microRNAs as a Prognostic Marker of Hepatocellular Carcinoma and the Corresponding Competitive Endogenous RNA Network. Int. J. Gen. Med. 2021, 14, 3377–3385. [Google Scholar] [CrossRef]
- Yokota, Y.; Noda, T.; Okumura, Y.; Kobayashi, S.; Iwagami, Y.; Yamada, D.; Tomimaru, Y.; Akita, H.; Gotoh, K.; Takeda, Y.; et al. Serum exosomal miR-638 is a prognostic marker of HCC via downregulation of VE-cadherin and ZO-1 of endothelial cells. Cancer Sci. 2021, 112, 1275–1288. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, Y.; Xue, W.; Zou, H.; Li, K.; Liu, K.; Zhao, W.; Zhu, C.; Cao, J. Profiling and Integrated Analysis of Differentially Expressed MicroRNAs as Novel Biomarkers of Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 770918. [Google Scholar] [CrossRef]
- Zhu, B.; Gu, S.; Wu, X.; He, W.; Zhou, H. Bioinformatics analysis of tumor-educated platelet microRNAs in patients with hepatocellular carcinoma. Biosci. Rep. 2021, 41, BSR20211420. [Google Scholar] [CrossRef]
- Hu, B.; Ma, X.; Fu, P.; Sun, Q.; Tang, W.; Sun, H.; Yang, Z.; Yu, M.; Zhou, J.; Fan, J.; et al. miRNA-mRNA Regulatory Network and Factors Associated with Prediction of Prognosis in Hepatocellular Carcinoma. Genom. Proteom. Bioinform. 2021, 19, 913. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.D.; Wang, W.E.; Ma, Y.S.; Shi, Y.; Yin, J.; Liu, J.B.; Yang, X.L.; Xin, R.; Fu, D.; Zhang, W.J. A miR-212-3p/SLC6A1 Regulatory Sub-Network for the Prognosis of Hepatocellular Carcinoma. Cancer Manag. Res. 2021, 13, 5063–5075. [Google Scholar] [CrossRef] [PubMed]
- El-Mezayen, H.; Yamamura, K.; Yusa, T.; Nakao, Y.; Uemura, N.; Kitamura, F.; Itoyama, R.; Yamao, T.; Higashi, T.; Hayashi, H.; et al. MicroRNA-25 Exerts an Oncogenic Function by Regulating the Ubiquitin Ligase Fbxw7 in Hepatocellular Carcinoma. Ann. Surg. Oncol. 2021, 28, 7973–7982. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Xu, M.; Xiong, Z.; Hu, K.; Yang, J.; Cao, M.; Zhong, Z.; Yao, Z.; Deng, M.; Liu, B. Identification of miRNAs as diagnostic and prognostic markers in hepatocellular carcinoma. Aging 2021, 13, 6115–6133. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, J.S.; Park, N.R.; Nam, H.; Sung, P.S.; Bae, S.H.; Choi, J.Y.; Yoon, S.K.; Hur, W.; Jang, J.W. Exosomal miR-125b Exerts Anti-Metastatic Properties and Predicts Early Metastasis of Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 637247. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, H.; Zhao, S.; Wang, E.; Zhu, J.; Feng, D.; Zhu, Y.; Dou, W.; Fan, Q.; Hu, J.; et al. Epigenetic silencing of miR-144/451a cluster contributes to HCC progression via paracrine HGF/MIF-mediated TAM remodeling. Mol. Cancer 2021, 20, 46. [Google Scholar] [CrossRef]
- Kong, C.Q.; Chen, X.C.; Qiu, G.H.; Liang, J.C.; Wang, D.; Liu, X.Y.; Liu, J.J.; Han, Y.Q.; Fan, X.H. Effects of miRNA-140 on the Growth and Clinical Prognosis of SMMC-7721 Hepatocellular Carcinoma Cell Line. BioMed Res. Int. 2021, 2021, 6638915. [Google Scholar] [CrossRef]
- Yugawa, K.; Yoshizumi, T.; Mano, Y.; Itoh, S.; Harada, N.; Ikegami, T.; Kohashi, K.; Oda, Y.; Mori, M. Cancer-associated fibroblasts promote hepatocellular carcinoma progression through downregulation of exosomal miR-150-3p. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2021, 47, 384–393. [Google Scholar] [CrossRef]
- Chen, J.; Liu, Z.; Gao, G.; Mo, Y.; Zhou, H.; Huang, W.; Wu, L.; He, X.; Ding, J.; Luo, C.; et al. Efficacy of circulating microRNA-130b and blood routine parameters in the early diagnosis of gastric cancer. Oncol. Lett. 2021, 22, 725. [Google Scholar] [CrossRef]
- Matsuoka, T.; Yashiro, M. Biomarkers of gastric cancer: Current topics and future perspective. World J. Gastroenterol. 2018, 24, 2818–2832. [Google Scholar] [CrossRef]
- Necula, L.; Matei, L.; Dragu, D.; Neagu, A.I.; Mambet, C.; Nedeianu, S.; Bleotu, C.; Diaconu, C.C.; Chivu-Economescu, M. Recent advances in gastric cancer early diagnosis. World J. Gastroenterol. 2019, 25, 2029–2044. [Google Scholar] [CrossRef] [PubMed]
- Kahroba, H.; Samadi, N.; Mostafazadeh, M.; Hejazi, M.S.; Sadeghi, M.R.; Hashemzadeh, S.; Eftekhar Sadat, A.T.; Karimi, A. Evaluating the presence of deregulated tumoral onco-microRNAs in serum-derived exosomes of gastric cancer patients as noninvasive diagnostic biomarkers. BioImpacts 2022, 12, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Rong, Z.; Sheng, J.; Luo, Z.; Zhang, J.; Li, T.; Zhu, Z.; Fu, Z.; Qiu, Z.; Huang, C. Aberrant Non-Coding RNA Expressed in Gastric Cancer and Its Diagnostic Value. Front. Oncol. 2021, 11, 606764. [Google Scholar] [CrossRef] [PubMed]
- So, J.B.Y.; Kapoor, R.; Zhu, F.; Koh, C.; Zhou, L.; Zou, R.; Tang, Y.C.; Goo, P.C.K.; Rha, S.Y.; Chung, H.C.; et al. Development and validation of a serum microRNA biomarker panel for detecting gastric cancer in a high-risk population. Gut 2021, 70, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wen, J.; Li, S.; Shen, X.; You, T.; Huang, Y.; Xu, C.; Zhao, Y. Immune-Related Nine-MicroRNA Signature for Predicting the Prognosis of Gastric Cancer. Front. Genet. 2021, 12, 690598. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Cheng, L.; Huang, W.; Cheng, X.; Peng, W.; Shi, D. Genome Instability-Related miRNAs Predict Survival, Immune Landscape, and Immunotherapy Responses in Gastric Cancer. J. Immunol. Res. 2021, 2021, 2048833. [Google Scholar] [CrossRef]
- Qi, W.; Zhang, Q. Development and clinical validation of a 3-miRNA signature to predict prognosis of gastric cancer. PeerJ 2021, 9, e10462. [Google Scholar] [CrossRef]
- Liu, X.; Pu, K.; Wang, Y.; Chen, Y.; Zhou, Y. Gastric cancer-associated microRNA expression signatures: Integrated bioinformatics analysis, validation, and clinical significance. Ann. Transl. Med. 2021, 9, 797. [Google Scholar] [CrossRef]
- Xu, L.; Cai, Y.; Chen, X.; Zhu, Y.; Cai, J. Circulating MiR-1290 as a potential diagnostic and disease monitoring biomarker of human gastrointestinal tumors. BMC Cancer 2021, 21, 989. [Google Scholar] [CrossRef]
- Yao, Y.; Ding, Y.; Bai, Y.; Zhou, Q.; Lee, H.; Li, X.; Teng, L. Identification of Serum Circulating MicroRNAs as Novel Diagnostic Biomarkers of Gastric Cancer. Front. Genet. 2020, 11, 591515. [Google Scholar] [CrossRef]
- Liang, Y.; Zhao, Y.; Li, L.; Wei, H.; Huang, T.; Zhang, H.; Chen, X.; Yun, H.; Sun, W.; Wang, Y. MicroRNA profiles in five pairs of early gastric cancer tissues and adjacent non-cancerous tissues. Oncol. Lett. 2021, 22, 595. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Xie, J.; Wu, S. MicroRNA-182 is a potential biomarker for prognosis of gastric cancer: A protocol for meta-analysis and bioinformatics analysis. Medicine 2021, 100, e25830. [Google Scholar] [CrossRef] [PubMed]
- Gilani, N.; Arabi Belaghi, R.; Aftabi, Y.; Faramarzi, E.; Edgünlü, T.; Somi, M.H. Identifying Potential miRNA Biomarkers for Gastric Cancer Diagnosis Using Machine Learning Variable Selection Approach. Front. Genet. 2021, 12, 779455. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.D.; Xu, Z.Y.; Hu, C.; Lv, H.; Xie, H.X.; Huang, T.; Zhang, Y.Q.; Chen, G.P.; Fu, Y.F.; Cheng, X.D. Exosomal miR-590-5p in Serum as a Biomarker for the Diagnosis and Prognosis of Gastric Cancer. Front. Mol. Biosci. 2021, 8, 636566. [Google Scholar] [CrossRef]
- Mei, D.; Qi, Y.; Xia, Y.; Ma, J.; Hu, H.; Ai, J.; Chen, L.; Wu, N.; Liao, D. Microarray profile analysis identifies ETS1 as potential biomarker regulated by miR-23b and modulates TCF4 in gastric cancer. World J. Surg. Oncol. 2021, 19, 311. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, M.; Hu, X.; She, J.; Sun, R.; Qin, S.; Li, D. miRNA-194 predicts favorable prognosis in gastric cancer and inhibits gastric cancer cell growth by targeting CCND1. FEBS Open Bio 2021, 11, 1814–1826. [Google Scholar] [CrossRef]
- Jiang, H.; Liu, Y.; Hu, K.; Xia, Y.; Liang, L.; Zhu, X.; Cheng, X. MiRNA-339 targets and regulates ZNF689 to inhibit the proliferation and invasion of gastric cancer cells. Transl. Cancer Res. 2021, 10, 3516–3526. [Google Scholar] [CrossRef]
- Komatsu, S.; Imamura, T.; Kiuchi, J.; Takashima, Y.; Kamiya, H.; Ohashi, T.; Konishi, H.; Shiozaki, A.; Kubota, T.; Okamoto, K.; et al. Depletion of tumor suppressor miRNA-148a in plasma relates to tumor progression and poor outcomes in gastric cancer. Am. J. Cancer Res. 2021, 11, 6133–6146. [Google Scholar]
- Feng, J.; Wei, Q.; Yang, M.; Wang, X.; Liu, B.; Li, J. Development and validation of a novel miRNA classifier as a prognostic signature for stage II/III colorectal cancer. Ann. Transl. Med. 2021, 9, 747. [Google Scholar] [CrossRef]
- Han, L.; Shi, W.J.; Xie, Y.B.; Zhang, Z.G. Diagnostic value of four serum exosome microRNAs panel for the detection of colorectal cancer. World J. Gastrointest. Oncol. 2021, 13, 970–979. [Google Scholar] [CrossRef]
- Silva, C.M.S.; Barros-Filho, M.C.; Wong, D.V.T.; Mello, J.B.H.; Nobre, L.M.S.; Wanderley, C.W.S.; Lucetti, L.T.; Muniz, H.A.; Paiva, I.K.D.; Kuasne, H.; et al. Circulating let-7e-5p, miR-106a-5p, miR-28-3p, and miR-542-5p as a Promising microRNA Signature for the Detection of Colorectal Cancer. Cancers 2021, 13, 1493. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, H.; Ning, S.; Wei, C.; Li, J.; Wei, W.; Zhang, L. The High Ratio of the Plasma miR-96/miR-99b Correlated with Poor Prognosis in Patients with Metastatic Colorectal Cancer. Front. Mol. Biosci. 2021, 8, 799060. [Google Scholar] [CrossRef] [PubMed]
- Nassar, F.J.; Msheik, Z.S.; Itani, M.M.; Helou, R.E.; Hadla, R.; Kreidieh, F.; Bejjany, R.; Mukherji, D.; Shamseddine, A.; Nasr, R.R.; et al. Circulating miRNA as Biomarkers for Colorectal Cancer Diagnosis and Liver Metastasis. Diagnostics 2021, 11, 341. [Google Scholar] [CrossRef] [PubMed]
- Dokhanchi, M.; Pakravan, K.; Zareian, S.; Hussen, B.M.; Farid, M.; Razmara, E.; Mossahebi-Mohammadi, M.; Cho, W.C.; Babashah, S. Colorectal cancer cell-derived extracellular vesicles transfer miR-221-3p to promote endothelial cell angiogenesis via targeting suppressor of cytokine signaling 3. Life Sci. 2021, 285, 119937. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Lu, T.; Wang, Y.; Jiao, D.; Li, Z.; Wang, L.; Liu, L.; Guo, C.; Zhao, Y.; Han, X. Establishment and experimental validation of an immune miRNA signature for assessing prognosis and immune landscape of patients with colorectal cancer. J. Cell. Mol. Med. 2021, 25, 6874–6886. [Google Scholar] [CrossRef] [PubMed]
- Lan, S.H.; Lin, S.C.; Wang, W.C.; Yang, Y.C.; Lee, J.C.; Lin, P.W.; Chu, M.L.; Lan, K.Y.; Zuchini, R.; Liu, H.S.; et al. Autophagy Upregulates miR-449a Expression to Suppress Progression of Colorectal Cancer. Front. Oncol. 2021, 11, 738144. [Google Scholar] [CrossRef]
- Cho, W.C.; Kim, M.; Park, J.W.; Jeong, S.Y.; Ku, J.L. Exosomal miR-193a and let-7g accelerate cancer progression on primary colorectal cancer and paired peritoneal metastatic cancer. Transl. Oncol. 2021, 14, 101000. [Google Scholar] [CrossRef]
- Fukada, M.; Matsuhashi, N.; Takahashi, T.; Sugito, N.; Heishima, K.; Yoshida, K.; Akao, Y. Postoperative changes in plasma miR21-5p as a novel biomarker for colorectal cancer recurrence: A prospective study. Cancer Sci. 2021, 112, 4270–4280. [Google Scholar] [CrossRef]
- Liu, T.; Liu, D.; Guan, S.; Dong, M. Diagnostic role of circulating MiR-21 in colorectal cancer: A update meta-analysis. Ann. Med. 2021, 53, 87–102. [Google Scholar] [CrossRef]
- Song, H.; Ruan, C.; Xu, Y.; Xu, T.; Fan, R.; Jiang, T.; Cao, M.; Song, J. Survival stratification for colorectal cancer via multi-omics integration using an autoencoder-based model. Exp. Biol. Med. 2022, 247, 898–909. [Google Scholar] [CrossRef]
- Wang, L.; Song, X.; Yu, M.; Niu, L.; Zhao, Y.; Tang, Y.; Zheng, B.; Song, X.; Xie, L. Serum exosomal miR-377-3p and miR-381-3p as diagnostic biomarkers in colorectal cancer. Future Oncol. 2022, 18, 793–805. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gao, G.; Chen, Z.; Chen, Z.; Han, M.; Xie, X.; Jin, Q.; Du, H.; Cao, Z.; Zhang, H. Identification of the miRNA signature and key genes in colorectal cancer lymph node metastasis. Cancer Cell Int. 2021, 21, 358. [Google Scholar] [CrossRef] [PubMed]
- Cai, R.; Lu, Q.; Wang, D. Construction and prognostic analysis of miRNA-mRNA regulatory network in liver metastasis from colorectal cancer. World J. Surg. Oncol. 2021, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, O.; Yip, C.H.; Brooks, A.; Cabanes, A.; Caleffi, M.; Dunstan Yataco, J.A.; Gyawali, B.; McCormack, V.; McLaughlin de Anderson, M.; Mehrotra, R.; et al. Breast cancer early detection: A phased approach to implementation. Cancer 2020, 126 (Suppl. 10), 2379–2393. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef]
- Adam-Artigues, A.; Garrido-Cano, I.; Carbonell-Asins, J.A.; Lameirinhas, A.; Simón, S.; Ortega-Morillo, B.; Martínez, M.T.; Hernando, C.; Constâncio, V.; Burgues, O.; et al. Identification of a Two-MicroRNA Signature in Plasma as a Novel Biomarker for Very Early Diagnosis of Breast Cancer. Cancers 2021, 13, 2848. [Google Scholar] [CrossRef]
- Itani, M.M.; Nassar, F.J.; Tfayli, A.H.; Talhouk, R.S.; Chamandi, G.K.; Itani, A.R.S.; Makoukji, J.; Boustany, R.N.; Hou, L.; Zgheib, N.K.; et al. A Signature of Four Circulating microRNAs as Potential Biomarkers for Diagnosing Early-Stage Breast Cancer. Int. J. Mol. Sci. 2021, 22, 6121. [Google Scholar] [CrossRef]
- Majumder, M.; Ugwuagbo, K.C.; Maiti, S.; Lala, P.K.; Brackstone, M. Pri-miR526b and Pri-miR655 Are Potential Blood Biomarkers for Breast Cancer. Cancers 2021, 13, 3838. [Google Scholar] [CrossRef]
- Kim, M.W.; Park, S.; Lee, H.; Gwak, H.; Hyun, K.A.; Kim, J.Y.; Jung, H.I.; Il Kim, S. Multi-miRNA panel of tumor-derived extracellular vesicles as promising diagnostic biomarkers of early-stage breast cancer. Cancer Sci. 2021, 112, 5078–5087. [Google Scholar] [CrossRef]
- Lal, M.; Ansari, A.H.; Agrawal, A.; Mukhopadhyay, A. Diagnostic and Prognostic Potential of MiR-379/656 MicroRNA Cluster in Molecular Subtypes of Breast Cancer. J. Clin. Med. 2021, 10, 4071. [Google Scholar] [CrossRef]
- Tian, B.; Hou, M.; Zhou, K.; Qiu, X.; Du, Y.; Gu, Y.; Yin, X.; Wang, J. A Novel TCGA-Validated, MiRNA-Based Signature for Prediction of Breast Cancer Prognosis and Survival. Front. Cell Dev. Biol. 2021, 9, 717462. [Google Scholar] [CrossRef] [PubMed]
- Turkistani, S.; Sugita, B.M.; Fadda, P.; Marchi, R.; Afsari, A.; Naab, T.; Apprey, V.; Copeland, R.L., Jr.; Campbell, M.C.; Cavalli, L.R.; et al. A panel of miRNAs as prognostic markers for African-American patients with triple negative breast cancer. BMC Cancer 2021, 21, 861. [Google Scholar] [CrossRef] [PubMed]
- Xing, A.Y.; Wang, B.; Li, Y.H.; Chen, X.; Wang, Y.W.; Liu, H.T.; Gao, P. Identification of miRNA Signature in Breast Cancer to Predict Neoadjuvant Chemotherapy Response. Pathol. Oncol. Res. POR 2021, 27, 1609753. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zhao, M.; Lv, Y.; Mao, G.; Ding, S.; Peng, F. The lncRNA GATA3-AS1/miR-495-3p/CENPU axis predicts poor prognosis of breast cancer via the PLK1 signaling pathway. Aging 2021, 13, 13663–13679. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Xia, T.; Li, M.; Wang, T.; Liu, P.; Zhou, X.; Huang, Z.; Zhu, W. MicroRNA profiling in serum: Potential signatures for breast cancer diagnosis. Cancer Biomark. Sect. A Dis. Markers 2021, 30, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Zou, R.; Loke, S.Y.; Tan, V.K.; Quek, S.T.; Jagmohan, P.; Tang, Y.C.; Madhukumar, P.; Tan, B.K.; Yong, W.S.; Sim, Y.; et al. Development of a microRNA Panel for Classification of Abnormal Mammograms for Breast Cancer. Cancers 2021, 13, 2130. [Google Scholar] [CrossRef]
- Thomopoulou, K.; Papadaki, C.; Monastirioti, A.; Koronakis, G.; Mala, A.; Kalapanida, D.; Mavroudis, D.; Agelaki, S. MicroRNAs Regulating Tumor Immune Response in the Prediction of the Outcome in Patients with Breast Cancer. Front. Mol. Biosci. 2021, 8, 668534. [Google Scholar] [CrossRef]
- Bao, S.; Hu, T.; Liu, J.; Su, J.; Sun, J.; Ming, Y.; Li, J.; Wu, N.; Chen, H.; Zhou, M. Genomic instability-derived plasma extracellular vesicle-microRNA signature as a minimally invasive predictor of risk and unfavorable prognosis in breast cancer. J. Nanobiotechnol. 2021, 19, 22. [Google Scholar] [CrossRef]
- Qattan, A.; Al-Tweigeri, T.; Alkhayal, W.; Suleman, K.; Tulbah, A.; Amer, S. Clinical Identification of Dysregulated Circulating microRNAs and Their Implication in Drug Response in Triple Negative Breast Cancer (TNBC) by Target Gene Network and Meta-Analysis. Genes 2021, 12, 549. [Google Scholar] [CrossRef]
- Chen, L.; Zhu, X.; Han, B.; Ji, L.; Yao, L.; Wang, Z. High Expression of microRNA-223 Indicates a Good Prognosis in Triple-Negative Breast Cancer. Front. Oncol. 2021, 11, 630432. [Google Scholar] [CrossRef]
- Mansoori, B.; Silvestris, N.; Mohammadi, A.; Khaze, V.; Baghbani, E.; Mokhtarzadeh, A.; Shanehbandi, D.; Derakhshani, A.; Duijf, P.H.G.; Baradaran, B. miR-34a and miR-200c Have an Additive Tumor-Suppressive Effect on Breast Cancer Cells and Patient Prognosis. Genes 2021, 12, 267. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Qian, T.; Bao, S.; Zhao, H.; Chen, H.; Xing, Z.; Li, Y.; Zhang, M.; Meng, X.; Wang, C.; et al. Circulating exosomal miR-363-5p inhibits lymph node metastasis by downregulating PDGFB and serves as a potential noninvasive biomarker for breast cancer. Mol. Oncol. 2021, 15, 2466–2479. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Koay, E.J.; Borowsky, A.D.; De Marzo, A.M.; Ghosh, S.; Wagner, P.D.; Kramer, B.S. Cancer overdiagnosis: A biological challenge and clinical dilemma. Nat. Rev. Cancer 2019, 19, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Albertsen, P.C. Reconsidering Prostate Cancer Mortality—The Future of PSA Screening. N. Engl. J. Med. 2020, 382, 1557–1563. [Google Scholar] [CrossRef]
- Mello-Grand, M.; Bruno, A.; Sacchetto, L.; Cristoni, S.; Gregnanin, I.; Dematteis, A.; Zitella, A.; Gontero, P.; Peraldo-Neia, C.; Ricotta, R.; et al. Two Novel Ceramide-Like Molecules and miR-5100 Levels as Biomarkers Improve Prediction of Prostate Cancer in Gray-Zone PSA. Front. Oncol. 2021, 11, 769158. [Google Scholar] [CrossRef]
- Giglio, S.; De Nunzio, C.; Cirombella, R.; Stoppacciaro, A.; Faruq, O.; Volinia, S.; Baldassarre, G.; Tubaro, A.; Ishii, H.; Croce, C.M.; et al. A preliminary study of micro-RNAs as minimally invasive biomarkers for the diagnosis of prostate cancer patients. J. Exp. Clin. Cancer Res. 2021, 40, 79. [Google Scholar] [CrossRef]
- Markert, L.; Holdmann, J.; Klinger, C.; Kaufmann, M.; Schork, K.; Turewicz, M.; Eisenacher, M.; Savelsbergh, A. Small RNAs as biomarkers to differentiate benign and malign prostate diseases: An alternative for transrectal punch biopsy of the prostate? PLoS ONE 2021, 16, e0247930. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, Y.X.; Dong, B.; Du, X.; Wang, J.; Wang, X.; Gao, W.Q.; Xue, W. Discovery of extracellular vesicles derived miR-181a-5p in patient’s serum as an indicator for bone-metastatic prostate cancer. Theranostics 2021, 11, 878–892. [Google Scholar] [CrossRef]
- Rönnau, C.G.H.; Fussek, S.; Smit, F.P.; Aalders, T.W.; van Hooij, O.; Pinto, P.M.C.; Burchardt, M.; Schalken, J.A.; Verhaegh, G.W. Upregulation of miR-3195, miR-3687 and miR-4417 is associated with castration-resistant prostate cancer. World J. Urol. 2021, 39, 3789–3797. [Google Scholar] [CrossRef]
- Stoen, M.J.; Andersen, S.; Rakaee, M.; Pedersen, M.I.; Ingebriktsen, L.M.; Bremnes, R.M.; Donnem, T.; Lombardi, A.P.G.; Kilvaer, T.K.; Busund, L.T.; et al. High expression of miR-17-5p in tumor epithelium is a predictor for poor prognosis for prostate cancer patients. Sci. Rep. 2021, 11, 13864. [Google Scholar] [CrossRef]
- Liu, J.; Quan, Z.; Gao, Y.; Wu, X.; Zheng, Y. MicroRNA-199b-3p suppresses malignant proliferation by targeting Phospholipase Cε and correlated with poor prognosis in prostate cancer. Biochem. Biophys. Res. Commun. 2021, 576, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Bian, Z.; Huang, X.; Chen, Y.; Meng, J.; Feng, X.; Zhang, M.; Zhang, L.; Zhou, J.; Liang, C. Fifteen-MiRNA-Based Signature Is a Reliable Prognosis-Predicting Tool for Prostate Cancer Patients. Int. J. Med. Sci. 2021, 18, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.Y.; Shin, H.; Moon, H.W.; Park, Y.H.; Park, J.; Lee, J.Y. Urinary exosomal microRNA profiling in intermediate-risk prostate cancer. Sci. Rep. 2021, 11, 7355. [Google Scholar] [CrossRef]
- Saran, U.; Chandrasekaran, B.; Kolluru, V.; Tyagi, A.; Nguyen, K.D.; Valadon, C.L.; Shaheen, S.P.; Kong, M.; Poddar, T.; Ankem, M.K.; et al. Diagnostic molecular markers predicting aggressive potential in low-grade prostate cancer. Transl. Res. J. Lab. Clin. Med. 2021, 231, 92–101. [Google Scholar] [CrossRef]
- Zhao, Y.; Tang, X.; Zhao, Y.; Yu, Y.; Liu, S. Diagnostic significance of microRNA-1255b-5p in prostate cancer patients and its effect on cancer cell function. Bioengineered 2021, 12, 11451–11460. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, L.X.; Diao, Y.J.; Wang, J.; Ye, Y.; Hao, X.K. Identification of Urinary Exosomal miRNAs for the Non-Invasive Diagnosis of Prostate Cancer. Cancer Manag. Res. 2021, 13, 25–35. [Google Scholar] [CrossRef]
- Byun, Y.J.; Piao, X.M.; Jeong, P.; Kang, H.W.; Seo, S.P.; Moon, S.K.; Lee, J.Y.; Choi, Y.H.; Lee, H.Y.; Kim, W.T.; et al. Urinary microRNA-1913 to microRNA-3659 expression ratio as a non-invasive diagnostic biomarker for prostate cancer. Investig. Clin. Urol. 2021, 62, 340–348. [Google Scholar] [CrossRef]
- Zabegina, L.; Nazarova, I.; Nikiforova, N.; Slyusarenko, M.; Sidina, E.; Knyazeva, M.; Tsyrlina, E.; Novikov, S.; Reva, S.; Malek, A. A New Approach for Prostate Cancer Diagnosis by miRNA Profiling of Prostate-Derived Plasma Small Extracellular Vesicles. Cells 2021, 10, 2372. [Google Scholar] [CrossRef]
- Rode, M.P.; Silva, A.H.; Cisilotto, J.; Rosolen, D.; Creczynski-Pasa, T.B. miR-425-5p as an exosomal biomarker for metastatic prostate cancer. Cell. Signal. 2021, 87, 110113. [Google Scholar] [CrossRef]
- Zhou, P.; Gong, S.; Liu, B.; Shi, M.; Lu, F.; Li, N.; Tang, B. A hybridization-based dual-colorimetric kit for circulating cancer miRNA detection. Chem. Commun. 2021, 57, 6058–6061. [Google Scholar] [CrossRef]
- Mao, Y.; Sun, Y.; Xue, J.; Lu, W.; Cao, X. Ultra-sensitive and high efficiency detection of multiple non-small cell lung cancer-related miRNAs on a single test line in catalytic hairpin assembly-based SERS-LFA strip. Anal. Chim. Acta 2021, 1178, 338800. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, J.; Wan, H.; Zhang, X. Electrochemical detection of miRNA-100 in the sera of gastric cancer patients based on DSN-assisted amplification. Talanta 2021, 225, 121981. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Liang, Y.; Li, J.; Yu, Y.; Xiao, M.M.; Ni, W.; Zhang, Z.; Zhang, G.J. Carbon Nanotube Field-Effect Transistor Biosensor for Ultrasensitive and Label-Free Detection of Breast Cancer Exosomal miRNA21. Anal. Chem. 2021, 93, 15501–15507. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.; Sun, C.; Zhao, Y.; Wang, Q.; Guo, J.; Ye, B.; Yu, G. Overview of MicroRNAs as Diagnostic and Prognostic Biomarkers for High-Incidence Cancers in 2021. Int. J. Mol. Sci. 2022, 23, 11389. https://doi.org/10.3390/ijms231911389
Zhang C, Sun C, Zhao Y, Wang Q, Guo J, Ye B, Yu G. Overview of MicroRNAs as Diagnostic and Prognostic Biomarkers for High-Incidence Cancers in 2021. International Journal of Molecular Sciences. 2022; 23(19):11389. https://doi.org/10.3390/ijms231911389
Chicago/Turabian StyleZhang, Chunyan, Caifang Sun, Yabin Zhao, Qiwen Wang, Jianlin Guo, Bingyu Ye, and Guoying Yu. 2022. "Overview of MicroRNAs as Diagnostic and Prognostic Biomarkers for High-Incidence Cancers in 2021" International Journal of Molecular Sciences 23, no. 19: 11389. https://doi.org/10.3390/ijms231911389