Skipping Breakfast and the Risk of Cardiovascular Disease and Death: A Systematic Review of Prospective Cohort Studies in Primary Prevention Settings

Abstract
:1. Background
2. Methods
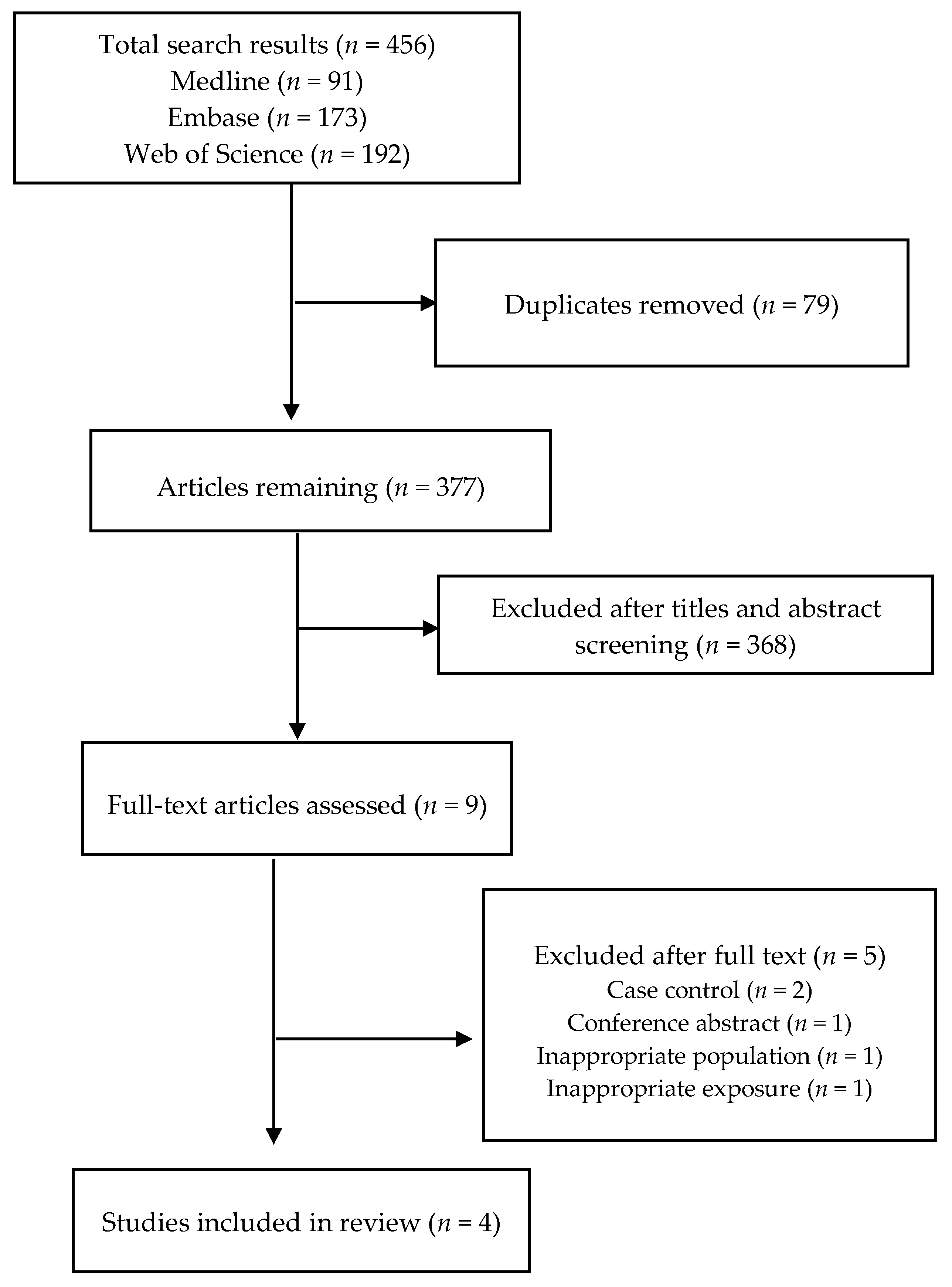
2.1. Search Strategy and Study Selection
2.2. Data Extraction, Quality Assessment, and Synthesis
3. Results
3.1. Search Results and Study Characteristics
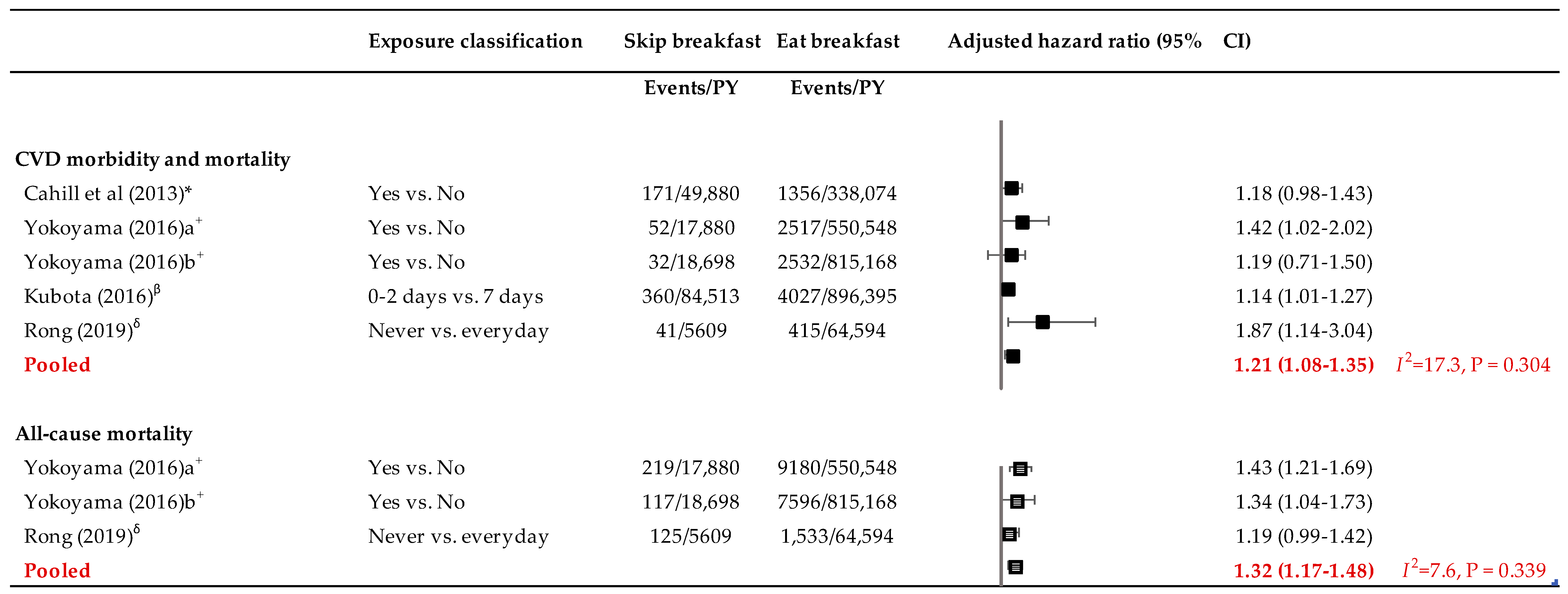
3.2. Association of Skipping Breakfast with CVD Morbidity and Mortality
3.3. Association of Skipping Breakfast with All-Cause Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Carnethon, M.R. Physical Activity and Cardiovascular Disease: How Much is Enough? Am. J. Lifestyle Med. 2009, 3, 44S–49S. [Google Scholar] [CrossRef] [PubMed]
- Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Available online: https://health.gov/dietaryguidelines/2015-scientific-report/ (accessed on 15 May 2019).
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010, 7th ed.; U.S. Government: Washington, DC, USA, 2010.
- Gibney, M.J.; Barr, S.I.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Livingstone, B.; Masset, G.; Moreiras, G.V.; Moreno, L.A.; Smith, J.; et al. Breakfast in Human Nutrition: The International Breakfast Research Initiative. Nutrients 2018, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Spence, C. Breakfast: The most important meal of the day? Int. J. Gastron. Food Sci. 2017, 8, 1–6. [Google Scholar] [CrossRef]
- Leidy, H. The Benefits of Breakfast Consumption to Combat Obesity and Diabetes in Young People. Am. J. Lifestyle Med. 2012, 7, 99–103. [Google Scholar] [CrossRef]
- Haines, P.S.; Guilkey, D.K.; Popkin, B.M. Trends in breakfast consumption of US adults between 1965 and 1991. J. Am. Diet. Assoc. 1996, 96, 464–470. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Secular trends in patterns of self-reported food consumption of adult Americans: NHANES 1971–1975 to NHANES 1999–2002. Am. J. Clin. Nutr. 2006, 84, 1215–1223. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C.D.; Vieux, F. Breakfast in the United States: Food and Nutrient Intakes in Relation to Diet Quality in National Health and Examination Survey 2011–2014. A Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1200. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; McConnell, A.; Cassettari, T.; Petocz, P. Breakfast choice is associated with nutrient, food group and discretionary intakes in australian adults at both breakfast and the rest of the day. Nutrients 2019, 11, 175. [Google Scholar] [CrossRef]
- Lovell, G.P.; Nash, K.; Sharman, R.; Lane, B.R. A cross-sectional investigation of depressive, anxiety, and stress symptoms and health-behavior participation in Australian university students. Nurs. Health Sci. 2015, 17, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Lowden, A.; Moreno, C.; Holmback, U.; Lennernas, M.; Tucker, P. Eating and shift work—Effects on habits, metabolism and performance. Scand. J. Work Environ. Health 2010, 36, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Ballon, A.; Neuenschwander, M.; Schlesinger, S. Breakfast Skipping Is Associated with Increased Risk of Type 2 Diabetes among Adults: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. J. Nutr. 2019, 149, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Odegaard, A.O.; Jacobs, D.R., Jr.; Steffen, L.M.; Van Horn, L.; Ludwig, D.S.; Pereira, M.A. Breakfast frequency and development of metabolic risk. Diabetes Care 2013, 36, 3100–3106. [Google Scholar] [CrossRef] [PubMed]
- Geliebter, A.; Astbury, N.M.; Aviram-Friedman, R.; Yahav, E.; Hashim, S. Skipping breakfast leads to weight loss but also elevated cholesterol compared with consuming daily breakfasts of oat porridge or frosted cornflakes in overweight individuals: A randomised controlled trial. J. Nutr. Sci. 2014, 3, e56. [Google Scholar] [CrossRef] [PubMed]
- Uzhova, I.; Fuster, V.; Fernandez-Ortiz, A.; Ordovas, J.M.; Sanz, J.; Fernandez-Friera, L.; Lopez-Melgar, B.; Mendiguren, J.M.; Ibanez, B.; Bueno, H.; et al. The Importance of Breakfast in Atherosclerosis Disease: Insights From the PESA Study. J. Am. Coll. Cardiol. 2017, 70, 1833–1842. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 May 2019).
- Cahill, L.E.; Chiuve, S.E.; Mekary, R.A.; Jensen, M.K.; Flint, A.J.; Hu, F.B.; Rimm, E.B. Prospective study of breakfast eating and incident coronary heart disease in a cohort of male US health professionals. Circulation 2013, 128, 337–343. [Google Scholar] [CrossRef]
- Kubota, Y.; Iso, H.; Sawada, N.; Tsugane, S. Association of Breakfast Intake with Incident Stroke and Coronary Heart Disease: The Japan Public Health Center-Based Study. Stroke 2016, 47, 477–481. [Google Scholar] [CrossRef]
- Rong, S.; Snetselaar, L.G.; Xu, G.; Sun, Y.; Liu, B.; Wallace, R.B.; Bao, W. Association of Skipping Breakfast With Cardiovascular and All-Cause Mortality. J. Am. Coll. Cardiol. 2019, 73, 2025–2032. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Onishi, K.; Hosoda, T.; Amano, H.; Otani, S.; Kurozawa, Y.; Tamakoshi, A. Skipping Breakfast and Risk of Mortality from Cancer, Circulatory Diseases and All Causes: Findings from the Japan Collaborative Cohort Study. Yonago Acta Med. 2016, 59, 55–60. [Google Scholar] [PubMed]
- Rassool, G.H. Expert report on diet, nutrition and prevention of chronic diseases. J. Adv. Nurs. 2003, 43, 544–545. [Google Scholar] [CrossRef] [PubMed]
- Nishida, C.; Uauy, R.; Kumanyika, S.; Shetty, P. The joint WHO/FAO expert consultation on diet, nutrition and the prevention of chronic diseases: Process, product and policy implications. Public Health Nutr. 2004, 7, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C.; Probst, Y.C. Nutrition in the prevention of chronic diseases. World Rev. Nutr. Diet. 2008, 98, 94–105. [Google Scholar] [PubMed]
- St-Onge, M.P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; et al. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [PubMed]
- Kaplan, G.A.; Seeman, T.E.; Cohen, R.D.; Knudsen, L.P.; Guralnik, J. Mortality among the elderly in the Alameda County Study: Behavioral and demographic risk factors. Am. J. Public Health 1987, 77, 307–312. [Google Scholar] [CrossRef]
- Vieira Musse, G.N.; Moreira, T.; Ayumi Kimura, M.; Pereira, F.W.L.; Okoshi, K.; Garcia Zanati, S.; Schmidt Azevedo, P.; Furlan Polegato, B.; de Paiva, S.A.R.; Mamede Zornoff, L.A.; et al. Skipping breakfast concomitant with late-night dinner eating is associated with worse outcomes following ST-segment elevation myocardial infarction. Eur. J. Prev. Cardiol. 2019, 17, 2047487319839546. [Google Scholar] [CrossRef]
- Nakajima, K.; Suwa, K.; Oda, E. Atrial fibrillation may be prevalent in individuals who report late-night dinner eating and concomitant breakfast skipping, a complex abnormal eating behavior around sleep. Int. J. Cardiol. 2014, 177, 1124–1126. [Google Scholar] [CrossRef]
- Maki, K.C.; Phillips-Eakley, A.K.; Smith, K.N. The Effects of Breakfast Consumption and Composition on Metabolic Wellness with a Focus on Carbohydrate Metabolism. Adv. Nutr. 2016, 7, 613S–621S. [Google Scholar] [CrossRef]
- Oikonomou, E.; Lazaros, G.; Christoforatou, E.; Chasikidis, C.; Vavouranaki, G.; Vogiatzi, G.; Papamikroulis, G.A.; Tsalamandris, S.; Gergiopoulos, G.; Mazaris, S.; et al. Breakfast association with arterial stiffness and carotid atherosclerotic burden: Insights from the ‘Corinthia’ study. Nutr. Metab. Carbiovasc. Dis. 2019, 29, 744–750. [Google Scholar] [CrossRef]
- Shibata, S.; Tahara, Y.; Hirao, A. The adjustment and manipulation of biological rhythms by light, nutrition, and abused drugs. Adv. Drug Deliv. Rev. 2010, 62, 918–927. [Google Scholar] [CrossRef]
- Weinrauch, L.A.; D’Elia, J.A. Is Skipping Breakfast a Marker for Current Smoking? J. Am. Coll. Cardiol. 2018, 71, 707–708. [Google Scholar] [CrossRef]
- Chen, J.; Cheng, J.; Liu, Y.; Tang, Y.; Sun, X.; Wang, T.; Xiao, Y.; Li, F.; Xiang, L.; Jiang, P.; et al. Associations between breakfast eating habits and health-promoting lifestyle, suboptimal health status in Southern China: A population based, cross sectional study. J. Transl. Med. 2014, 12, 348. [Google Scholar] [CrossRef]
- Reeves, S.; Halsey, L.G.; McMeel, Y.; Huber, J.W. Breakfast habits, beliefs and measures of health and wellbeing in a nationally representative UK sample. Appetite 2013, 60, 51–57. [Google Scholar] [CrossRef]
- Patte, K.A.; Leatherdale, S.T. A cross-sectional analysis examining the association between dieting behaviours and alcohol use among secondary school students in the COMPASS study. J. Public Health 2017, 39, 321–329. [Google Scholar] [CrossRef]
- Souza, R.V.; Sarmento, R.A.; de Almeida, J.C.; Canuto, R. The effect of shift work on eating habits: A systematic review. Scand. J. Work Environ. Health 2019, 45, 7–21. [Google Scholar] [CrossRef]
- Nagai, M.; Hoshide, S.; Kario, K. Sleep duration as a risk factor for cardiovascular disease—A review of the recent literature. Curr. Cardiol. Rev. 2010, 6, 54–61. [Google Scholar] [CrossRef]
- Fewell, Z.; Davey Smith, G.; Sterne, J.A. The impact of residual and unmeasured confounding in epidemiologic studies: A simulation study. Am. J. Epidemiol. 2007, 166, 646–655. [Google Scholar] [CrossRef]
- Garde, A.H.; Hansen, A.M.; Holtermann, A.; Gyntelberg, F.; Suadicani, P. Sleep duration and ischemic heart disease and all-cause mortality: Prospective cohort study on effects of tranquilizers/hypnotics and perceived stress. Scand. J. Work Environ. Health 2013, 39, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Cahill, L.; Chiuve, S.; Mekary, R.; Jensen, M.; Flint, A.; Hu, F.; Mukamal, K.; Rexrode, K.; Rimm, E. Breakfast eating and incident coronary heart disease in a large prospective cohort of American women. FASEB J. 2015, 29, 906.3. [Google Scholar]
- Ruiz, E.; Avila, J.M.; Valero, T.; Rodriguez, P.; Varela-Moreiras, G. Breakfast Consumption in Spain: Patterns, Nutrient Intake and Quality. Findings from the ANIBES Study, a Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1324. [Google Scholar] [CrossRef]
- Li, K.K.; Concepcion, R.Y.; Lee, H.; Cardinal, B.J.; Ebbeck, V.; Woekel, E.; Readdy, R.T. An examination of sex differences in relation to the eating habits and nutrient intakes of university students. J. Nutr. Educ. Behav. 2012, 44, 246–250. [Google Scholar] [CrossRef]
- Levine, C.S.; Miyamoto, Y.; Markus, H.R.; Rigotti, A.; Boylan, J.M.; Park, J.; Kitayama, S.; Karasawa, M.; Kawakami, N.; Coe, C.L.; et al. Culture and Healthy Eating: The Role of Independence and Interdependence in the United States and Japan. Personal. Soc. Psychol. Bull. 2016, 42, 1335–1348. [Google Scholar] [CrossRef]
- Gabriel, A.S.; Ninomiya, K.; Uneyama, H. The Role of the Japanese Traditional Diet in Healthy and Sustainable Dietary Patterns around the World. Nutrients 2018, 10, 173. [Google Scholar] [CrossRef]
- Marmot, M.G.; Syme, S.L.; Kagan, A.; Kato, H.; Cohen, J.B.; Belsky, J. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: Prevalence of coronary and hypertensive heart disease and associated risk factors. Am. J. Epidemiol. 1975, 102, 514–525. [Google Scholar] [CrossRef]
- Suzuki, N.; Goto, Y.; Ota, H.; Kito, K.; Mano, F.; Joo, E.; Ikeda, K.; Inagaki, N.; Nakayama, T. Characteristics of the Japanese Diet Described in Epidemiologic Publications: A Qualitative Systematic Review. J. Nutr. Sci. Vitaminol. 2018, 64, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003–2015: Continuous Westernization of the Japanese Diet. Nutrients 2018, 10, 994. [Google Scholar] [CrossRef]
- Morinaka, T.; Wozniewicz, M.; Jeszka, J.; Bajerska, J.; Nowaczyk, P.; Sone, Y. Westernization of dietary patterns among young Japanese and Polish females—A comparison study. Ann. Agric. Environ. Med. AAEM 2013, 20, 122–130. [Google Scholar]
- Brikou, D.; Zannidi, D.; Karfopoulou, E.; Anastasiou, C.A.; Yannakoulia, M. Breakfast consumption and weight-loss maintenance: Results from the MedWeight study. Br. J. Nutr. 2016, 115, 2246–2251. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The role of breakfast in health: Definition and criteria for a quality breakfast. J. Acad. Nutr. Diet. 2014, 114, S8–S26. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author Details | Country of Study | Study (Cohort) Name | Sample Size | Age (Years) | % Female | Duration of Follow-Up (Years) | Breakfast Evaluation Method | Exposure (Breakfast) Definition | Outcome(s) |
|---|---|---|---|---|---|---|---|---|---|
| Cahill et al., 2013 [21] | US | Health Professionals Follow-Up Study | 26,902 | 45–82 | 0.0 | 16.0 | Questionnaire (self-administered) | Breakfast was defined as a positive response to any of the first three eating times (‘before breakfast’, ‘breakfast’, ‘between breakfast and lunch’) | Incident coronary heart disease (CHD); defined as non-fatal myocardial infarction (MI) or fatal CHD |
| Kubota et al., 2016 [22] | Japan | The Japan Public Health Center-Based Prospective (JPHC) study | 82,772 | 45–74 | 53.3 | 12.7 | Questionnaire (self-administered) | Participants were classified into the following four groups; those who had breakfast 0 to 2 (subjects with almost never, those with 1–3 times/month, and those with 1–2 times/week were combined because of the small number of those with 1–3 times/month or 1–2 times/week), 3–4, 5–6, or 7 (everyday) times/week. Those who had breakfast 7 times/week were regarded as the reference group. | Stroke and CHD (i.e., myocardial infarction and sudden cardiac death) |
| Rong et al., 2019 [23] | US | National Health and Nutrition Examination Survey III | 6550 | 40–75 | 52.0 | 18.8 | Home-based interviews | Participants were asked “How often do you eat breakfast?” during the household interview, and the possible answers included “every day,” “some days,” “rarely,” “never,” and “weekends only.” The frequency of breakfast eating was classified as “never,” “rarely,” “some days,” or “every day.” | Death from cardiovascular disease (CVD) (defined as heart disease or stroke; ICD codes: (I00–09, I11, I13, I20–51, I60–69), heart disease, stroke, or all-cause death. |
| Yokoyama et al., 2016 [24] | Japan | The Japan Collaborative Cohort Study (JACC) Study | 83,410 | 40–79 | 59.1 | 19.4 | Questionnaire (self-administered) | The type of breakfast consumed was assessed according to the following five categories: Japanese style, Western style, Chagayu style (tea rice gruel), no or nearly no breakfast eaten, or other. Participants were classified into two groups, as those who eat breakfast (including Japanese style, Western style, Chagayu style (tea rice gruel), and other) and those who skip breakfast (no or nearly no breakfast eaten). | Deaths from circulatory diseases (I00–I99) or all-cause death. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ofori-Asenso, R.; Owen, A.J.; Liew, D. Skipping Breakfast and the Risk of Cardiovascular Disease and Death: A Systematic Review of Prospective Cohort Studies in Primary Prevention Settings. J. Cardiovasc. Dev. Dis. 2019, 6, 30. https://doi.org/10.3390/jcdd6030030
Ofori-Asenso R, Owen AJ, Liew D. Skipping Breakfast and the Risk of Cardiovascular Disease and Death: A Systematic Review of Prospective Cohort Studies in Primary Prevention Settings. Journal of Cardiovascular Development and Disease. 2019; 6(3):30. https://doi.org/10.3390/jcdd6030030
Chicago/Turabian StyleOfori-Asenso, Richard, Alice J. Owen, and Danny Liew. 2019. "Skipping Breakfast and the Risk of Cardiovascular Disease and Death: A Systematic Review of Prospective Cohort Studies in Primary Prevention Settings" Journal of Cardiovascular Development and Disease 6, no. 3: 30. https://doi.org/10.3390/jcdd6030030