
Affected Others Responsivity to Gambling Harm: An International Taxonomy of Consumer-Derived Behaviour Change Techniques
 , , , and
, , , and
Abstract
:1. Introduction
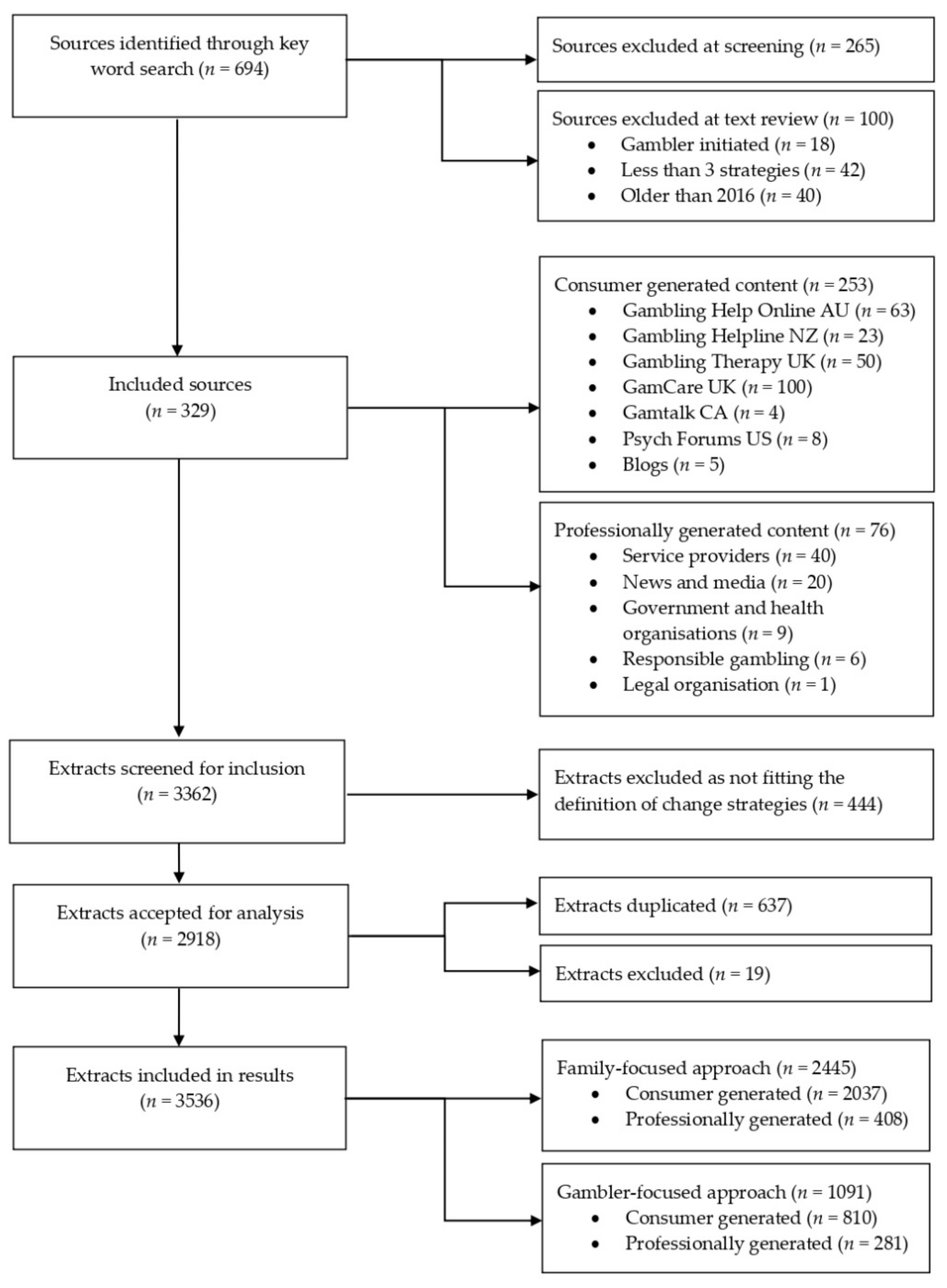
2. Methods
2.1. Sample and Procedure
2.2. Data Extraction and Preparation
2.3. Development of the Taxonomy
2.4. Data Coding and Analysis
3. Results
3.1. Aim 1. Development of the Taxonomy
3.2. Aim 2: Consumer-Derived Behaviour Change Strategies—Family-Focused
3.2.1. Family-Focused: Pre-Decisional
I’m in a no-win situation. If I stay, he gambles, and the misery continues. If I go, I’m on my own, but at least there is a more promising future.
Get informed. If you think your loved one might have a problem, try to learn what you can about gambling addiction, including its warning signs, negative impacts, and options for help and recovery in the community.
My wife and I need to build trust. It’s terrible to be in a relationship with no trust. Is there anyone else out there that has some advice on how to rebuild trust?
If you look around the forums you will find many other people with similar stories to yourself. Have a talk with a few and see what sorts of things have helped them.
I feel like a fool for being so naive and not realising what was happening. I’d just accepted that my husband had changed personality and let him carry on. I really needed help.
I was foolish and accompanied her into casinos where she’d play a couple hundred then I’d say time to go. I should have never condoned this because it just allowed her to gamble.
All those endless promises that he will change, and not do it again...I now realise they don’t mean anything...I am just a means to an end to him at the moment.
3.2.2. Family-Focused: Post-Decisional
Set boundaries—know your limits by considering what you are willing to accept and what you will no longer tolerate.
Emotionally prepare yourself to deny his requests. For example, remind yourself daily that having money for bills and food is far more important than feeding your husband’s addiction.
I suffer from depression, anxiety disorder and OCD—I’ve tried to support him before but now I need to put myself first and I don’t feel like I should have a further burden upon my own mental health.
Try and resist the urge to lecture him, but rather express that you’re coming from a place of concern. Gambling can often be a tough topic for people to open up about.
I threatened I would go to the police. He broke down and confessed to his parents and mine that he had pawned my jewellery.
Managing addiction is a work in progress. There might come a time when my partner backslides. But if she remains committed to her recovery and treatment, I will remain committed to my vows.
But I know it’s a long road ahead. Trying really hard to stay strong…It’s just so hard on top of all of the other life stresses we have going on at the moment. For now, I’ll just keep putting one foot in front of the other.
I have a couple of stories with happy endings my friends shared with me, so I just keep them in my mind to strive. Hope our story will end up happily too.
3.2.3. Family-Focused: Actional
I am exhausted and feel like I am living with a stranger. I have an appointment booked with my Doctor to get plugged into a counsellor to help work through some of my emotions.
I went to counselling for myself for a while, but then I realised that it was of no use if we don’t both attend.
Don’t forget to look after yourself, you can be there for you partner, support him, but you also need support. Someone you can talk too, confide in, someone who can help you ride the roller coaster, hold your hand when things get tough.
It took me a long time to start talking but once I did, I was amazed by how supportive everyone was and still is.
I wanted desperately to phone a friend to come get me, but I couldn’t stand the thought of having to explain why I was in tears and everything else.
I have decided that enough is enough. I do love him, but not as a gambler, and I don’t have any energy left for the arguments, lies, deception that comes from this horrible infliction. Time to move on, I guess.
I have constantly thoughts about separating from my husband as the only possible way, honestly, I don’t know how it may affect kids’ and our lives either and it scares me.
I know I need to look after myself and am doing a mindfulness course at the moment which helps a bit.
A healthy diet, regular exercise and adequate rest can improve your wellbeing, and increase your resilience to stress.
Take time every day to engage in hobbies, interests, friends, family, things that do not include gambling thoughts of any kind.
I’ve now got every single card and have requested to become power of attorney over his and my mother’s accounts.
He had gone into my car, got my wallet and used my card. Luckily, I have learnt to only keep a small amount on my card.
It can help to write down your feelings, even if just to get them off your chest and see how the feelings are changing over time.
I am letting him make the mistakes he needs to make. At the end of the day, it is his money and me holding it causes a lot of conflict.
I wish I could go back in time and never lend you money, never bail you out, never enable the problem. Then maybe you’d hit a smaller rock bottom than we’re now about to hit, maybe a smaller rock bottom back then would be enough for you to want to change.
Don’t even entertain that thought one bit. You are not responsible for his gambling. It is all his own doing, his choice.
You might consider not lending money if he continues to gamble, however, if he cuts back or stop gambling you might offer to conditionally help to pay off a bill.
3.2.4. Family-Focused: Post-Actional Phase
I’ve tried different strategies on how to help him, but he somehow manages to find his way around everything.
I can honestly say I am now thinking about myself. I’ve been on holiday, got my own place, socialise and buy myself things if the notion takes me...things I haven’t done in years and they make me feel good!
3.3. Aim 2: Consumer-Derived Behaviour Change Strategies—Gambler-Focused
3.3.1. Gambler-Focused: Pre-Decisional
I try to ask questions to make him think about his gambling and its effect. I can’t say it’s actually working but he is at least talking every now and again and sometimes I can see something I have asked ticking in his head.
Tell the person how his or her gambling affects you and the family—Partners of gamblers often feel confused, angry and helpless. Don’t be afraid to tell them how their gambling affects you but remain calm.
We went to the Bank and printed out all the statements and highlighted the amounts that had been spent on gambling. It came to $47,000.
Download the GA 20-questions and show them to him—maybe he doesn’t realise his problem is a recognised addiction and that there is support for him.
Ask him what he thinks would be helpful and offer to support him by getting more information or seeking external assistance.
I leave gambling pamphlets where he can see them in the hope he may pick it up when no-one is looking.
3.3.2. Gambler-Focused: Post-Decisional
Make an action plan if you are helping someone close to you recover from problem gambling, it can be useful to have a plan in place to help keep them headed in the right direction.
Work with the person to agree on acceptable behaviours, e.g., talking to a professional, staying within agreed spending limits.
I am setting little goals (like deleting online accounts) with dates for it to be done by to make it more manageable. Are there any other suggestions I can to do to make this easier for him?
Help the person identify their triggers. This can help them know what to avoid or allow them to learn how to cope when faced with these triggers.
Let him know that he can call you when he’s having an urge to gamble—sometimes that can be really powerful, as it helps the gambler realise that the urge will pass by talking to someone or doing something to distract themselves.
Don’t get angry or frustrated with them if they slip from time to time—this is normal and you can encourage them to learn from these mistakes.
We identified the underlying issues that have triggered this—we lost a baby and his mum, and he hasn’t dealt with this.
I’m also happy to share that yesterday was his two-week anniversary of giving up gambling. He’s having trouble celebrating his anniversaries so far I think so I’m trying to hold the hope for him until he feels it himself.
3.3.3. Gambler-Focused Approach: Actional Phase
I went to counselling sessions with my husband a couple of times and I believe it helped both of us to understand each other a bit better.
When I feel the time is right again, I’ll suggest he calls the helpline. I think talking helps my dad immensely. He’s probably just terrified to do it in a public forum.
My mum still has a few issues to work out and we will always be here to help her. We are slowly working out how best to do that as a family.
I got an awful text from my boyfriend who is an addict and has been for a long time. He was saying goodbye. That he needed to be free and this (suicide) was the only way. Thank god I managed to get him to come home and talked to him. I think I managed to save him today. And I’m terrified about tomorrow and the days to come.
Fortunately, Sue has a real talent with eBay. I’ve got a business friend of mine who wants her to create a shop there. This will keep Sue busy with other stuff thereby cutting down on the spare time she has to play the pokies.
I have helped her create and stick to a budget, rang and arranged payment plans with finance companies, tracked her spending via internet banking, and held on to her ATM card.
Discuss with the person how they can limit their access to cash or credit. This will remove a major gambling trigger.
I took care of all expenditure of the house including food, bills, house, everything, I also gave her a bit of money every month to make her feel life is still happy. But the situation was worsening since she kept asking for more money.
He is terrible with his spending and will also gamble online. I have deleted the gambling apps off his phone and said I never want to see them on your phone again.
I would pretend I was him and self-exclude him from the sites he played.
Sit with him and make a list of all online gambling sites and self-exclude. Then do the same with all bookmakers he could possibly go to.
Part of me thinks I should come to an agreement with her on how often and how much she can spend per week. So that she can be happy, and I can learn to deal with the occasional gamble.
We figured into our budget $50.00 a week each, which we may do whatever we like with. I don’t mind if he wishes to gamble that $50.00 a week—it is his discretionary spending and he is free to decide how to spend it.
4. Discussion
4.1. Limitations
4.2. Clinical Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Association: Philadelphia, PA, USA, 2013. [Google Scholar]
- Di Nicola, M.; De Crescenzo, F.; D’Alò, G.L.; Remondi, C.; Panaccione, I.; Moccia, L.; Molinaro, M.; Dattoli, L.; Lauriola, A.; Martinelli, S. Pharmacological and psychosocial treatment of adults with gambling disorder: A meta-review. J. Addict. Med. 2020, 14, e15–e23. [Google Scholar] [CrossRef]
- Langham, E.; Thorne, H.; Browne, M.; Donaldson, P.; Rose, J.; Rockloff, M. Understanding gambling related harm: A proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health 2016, 16, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kourgiantakis, T.; Saint-Jacques, M.-C.; Tremblay, J. Problem gambling and families: A systematic review. J. Soc. Work Pract. Addict. 2013, 13, 353–372. [Google Scholar] [CrossRef]
- Riley, B.J.; Harvey, P.; Crisp, B.R.; Battersby, M.; Lawn, S. Gambling-Related harm as reported by concerned significant others: A systematic review and meta-synthesis of empirical studies. J. Fam. Stud. 2018, 1–17. [Google Scholar] [CrossRef]
- Browne, M.; Bellringer, M.; Greer, N.; Kolandai-Matchett, K.; Langham, E.; Rockloff, M.; Du Preez, K.; Abbott, M. Measuring the Burden of Gambling Harm in New Zealand; Ministry of Health: Wellington, New Zealand, 2017.
- Goodwin, B.C.; Browne, M.; Rockloff, M.; Rose, J. A typical problem gambler affects six others. Int. Gambl. Stud. 2017, 17, 276–289. [Google Scholar] [CrossRef]
- Rockloff, M.J.; Browne, M.; Russell, A.M.T.; Merkouris, S.S.; Dowling, N.A. A quantification of the net consumer surplus from gambling participation. J. Gambl. Stud. 2019, 35, 1147–1162. [Google Scholar] [CrossRef]
- Salonen, A.H.; Alho, H.; Castrén, S. Gambling frequency, gambling problems and concerned significant others of problem gamblers in Finland: Cross-sectional population studies in 2007 and 2011. Scand. J. Public Health 2015, 43, 229–235. [Google Scholar] [CrossRef]
- Salonen, A.H.; Alho, H.; Castren, S. The extent and type of gambling harms for concerned significant others: A cross-sectional population study in Finland. Scand. J. Public Health 2016, 44, 799–804. [Google Scholar] [CrossRef] [Green Version]
- Salonen, A.H.; Castrén, S.; Alho, H.; Lahti, T. Concerned significant others of people with gambling problems in Finland: A cross-sectional population study. BMC Public Health 2014, 14, 398. [Google Scholar] [CrossRef] [Green Version]
- Shiue, I. Self and environmental exposures to drinking, smoking, gambling or video game addiction are associated with adult hypertension, heart and cerebrovascular diseases, allergy, self-rated health and happiness: Japanese General Social Survey, 2010. Int. J. Cardiol. 2015, 181, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Svensson, J.; Romild, U.; Shepherdson, E. The concerned significant others of people with gambling problems in a national representative sample in Sweden—A 1 year follow-up study. BMC Public Health 2013, 13, 1087. [Google Scholar] [CrossRef] [Green Version]
- Wenzel, H.G.; Øren, A.; Bakken, I.J. Gambling problems in the family—A stratified probability sample study of prevalence and reported consequences. BMC Public Health 2008, 8, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowling, N.A.; Rodda, S.N.; Lubman, D.I.; Jackson, A.C. The impacts of problem gambling on concerned significant others accessing web-based counselling. Addict. Behav. 2014, 39, 1253–1257. [Google Scholar] [CrossRef] [PubMed]
- Rodda, S.N.; Dowling, N.A.; Thomas, A.C.; Bagot, K.L.; Lubman, D.I. Treatment for Family Members of People Experiencing Gambling Problems: Family Members Want Both Gambler-Focused and Family-Focused Options. Int. J. Ment. Health Addict. 2019, 18. [Google Scholar] [CrossRef]
- Orford, J.; Copello, A.; Velleman, R.; Templeton, L. Family members affected by a close relative’s addiction: The stress-strain-coping-support model. Drugs Educ. Prev. Policy 2010, 17, 36–43. [Google Scholar] [CrossRef] [Green Version]
- Copello, A.; Templeton, L.; Orford, J.; Velleman, R. The 5-Step Method: Principles and practice. Drugs Educ. Prev. Policy 2010, 17, 86–99. [Google Scholar] [CrossRef]
- Orford, J.; Cousins, J.; Smith, N.; Bowden-Jones, H. Stress, strain, coping and social support for affected family members attending the National Problem Gambling Clinic, London. Int. Gambl. Stud. 2017, 17, 259–275. [Google Scholar] [CrossRef]
- Rychtarik, R.G.; McGillicuddy, N.B. Preliminary evaluation of a coping skills training program for those with a pathological-gambling partner. J. Gambl. Stud. 2006, 22, 165–178. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Spielberger, C.D. Family stress: Integrating theory and measurement. J. Fam. Psychol. 1992, 6, 99. [Google Scholar] [CrossRef]
- Moos, R.H.; Finney, J.W.; Cronkite, R.C. Alcoholism Treatment: Context, Process, and Outcome; Oxford University Press: Oxford, UK, 1990. [Google Scholar]
- Rychtarik, R.G.; McGillicuddy, N.B. Coping skills training and 12-step facilitation for women whose partner has alcoholism: Effects on depression, the partner’s drinking, and partner physical violence. J. Consult. Clin. Psychol. 2005, 73, 249. [Google Scholar] [CrossRef] [Green Version]
- Buchner, U.G.; Koytek, A.; Wodarz, N.; Wolstein, J. Is an e-mental health programme a viable way to reach affected others of disordered gamblers? A feasibility study focusing on access and retention. Int. Gambl. Stud. 2019, 19, 85–105. [Google Scholar] [CrossRef]
- Côté, M.; Tremblay, J.; Jiménez-Murcia, S.; Fernàndez-Aranda, F.; Brunelle, N. How Can Partners Influence the Gambling Habits of Their Gambler Spouse? J. Gambl. Stud. 2019, 1–26. [Google Scholar] [CrossRef]
- Bond, K.S.; Jorm, A.F.; Miller, H.E.; Rodda, S.N.; Reavley, N.J.; Kelly, C.M.; Kitchener, B.A. How a concerned family member, friend or member of the public can help someone with gambling problems: A Delphi consensus study. BMC Psychol. 2016, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Hodgins, D.C.; Toneatto, T.; Makarchuk, K.; Skinner, W.; Vincent, S. Minimal treatment approaches for concerned significant others of problem gamblers: A randomized controlled trial. J. Gambl. Stud. 2007, 23, 215–230. [Google Scholar] [CrossRef]
- Magnusson, K.; Nilsson, A.; Gumpert, C.H.; Andersson, G.; Carlbring, P. Internet-Delivered cognitive-behavioural therapy for concerned significant others of people with problem gambling: Study protocol for a randomised wait-list controlled trial. BMJ Open 2015, 2, e008724. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, K.; Nilsson, A.; Andersson, G.; Hellner, C.; Carlbring, P. Internet-Delivered cognitive-behavioral therapy for significant others of treatment-refusing problem gamblers: A randomized wait-list controlled trial. J. Consult. Clin. Psychol. 2019, 87, 802–814. [Google Scholar] [CrossRef] [Green Version]
- Nayoski, N.; Hodgins, D.C. The efficacy of individual community reinforcement and family training (CRAFT) for concerned significant others of problem gamblers. J. Gambl. Issues 2016, 33. [Google Scholar] [CrossRef] [Green Version]
- Hing, N.; Tiyce, M.; Holdsworth, L.; Nuske, E. All in the family: Help-Seeking by significant others of problem gamblers. Int. J. Ment. Health Addict. 2013, 11, 396–408. [Google Scholar] [CrossRef]
- Archer, M.; Harwood, H.; Stevelink, S.; Rafferty, L.; Greenberg, N. Community reinforcement and family training and rates of treatment entry: A systematic review. Addiction 2019, 115. [Google Scholar] [CrossRef]
- Makarchuk, K.; Hodgins, D.C.; Peden, N. Development of a brief intervention for concerned significant others of problem gamblers. Addict. Disord. Treat. 2002, 1, 126–134. [Google Scholar] [CrossRef]
- Merkouris, S.S.; Dowling, N.A.; Rodda, S.N. Affected Other Treatments: Systematic Review and Meta-Analysis Across Addictions; NSW Office of Responsible Gambling: Sydney, Australia, 2020.
- Rodda, S.N.; Lubman, D.; Dowling, N.; McCann, T. Reasons for using web-based counselling among family and friends impacted by problem gambling. Asian J. Gambl. Issues Public Health 2013, 3, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Côté, M.; Tremblay, J.; Brunelle, N. A new look at the coping strategies used by the partners of pathological gamblers. J. Gambl. Issues 2018, 38. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; West, R.; Sheals, K.; Godinho, C.A. Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Transl. Behav. Med. 2018, 8, 212–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Cane, J.; Richardson, M.; Johnston, M.; Ladha, R.; Michie, S. From lists of behaviour change techniques (BCT s) to structured hierarchies: Comparison of two methods of developing a hierarchy of BCT s. Br. J. Health Psychol. 2015, 20, 130–150. [Google Scholar] [CrossRef]
- Gong, L.; Rodda, S.N. An Exploratory Study of Individual and Parental Techniques for Limiting Loot Box Consumption. Int. J. Ment. Health Addict. 2020, 1–28. [Google Scholar] [CrossRef]
- Rodda, S.N.; Booth, N.; McKean, J.; Chung, A.; Park, J.; Ware, P. Mechanisms for the reduction of caffeine consumption: What, how and why. Drug Alcohol Depend. 2020, 108024. [Google Scholar] [CrossRef] [PubMed]
- Rodda, S.N.; Hing, N.; Hodgins, D.C.; Cheetham, A.; Dickins, M.; Lubman, D.I. Behaviour change strategies for problem gambling: An analysis of online posts. Int. Gambl. Stud. 2018, 18, 420–438. [Google Scholar] [CrossRef]
- Rodda, S.N.; Booth, N.; Brittain, M.; McKean, J.; Thornley, S. I was truly addicted to sugar: A consumer-focused classification system of behaviour change strategies for sugar reduction. Appetite 2020, 144, 104456. [Google Scholar] [CrossRef]
- Rodda, S.N.; Booth, N.; Vacaru, M.; Knaebe, B.; Hodgins, D. Behaviour change strategies for internet, pornography and gaming addiction: A taxonomy and content analysis of professional and consumer websites. Comput. Hum. Behav. 2018, 84, 467–476. [Google Scholar] [CrossRef]
- Newell, R. Research for Evidence-Based Practice in Healthcare, 2nd ed.; Wiley-Blackwell: Chichester, UK, 2011. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V.; Hayfield, N.; Terry, G. Thematic analysis. In Handbook of Research Methods in Health Social Sciences; Liamputtong, P., Ed.; Springer: Singapore, 2019; pp. 843–860. [Google Scholar]
- Heckhausen, H.; Gollwitzer, P.M. Thought contents and cognitive functioning in motivational versus volitional states of mind. Motiv. Emot. 1987, 11, 101–120. [Google Scholar] [CrossRef]
- Michie, S.; Whittington, C.; Hamoudi, Z.; Zarnani, F.; Tober, G.; West, R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction 2012, 107, 1431–1440. [Google Scholar] [CrossRef] [PubMed]
- Rodda, S.N.; Hing, N.; Hodgins, D.C.; Cheetham, A.; Dickins, M.; Lubman, D.I. Change strategies and associated implementation challenges: An analysis of online counselling sessions. J. Gambl. Stud. 2017, 33, 955–973. [Google Scholar] [CrossRef] [PubMed]
- Rodda, S.N.; Bagot, K.; Cheetham, A.; Hodgins, D.C.; Hing, N.; Lubman, D.I. Types of change strategies for limiting or reducing gambling behaviours and their perceived helpfulness: A factor analysis. Psychol. Addict. Behav. 2018, 32, 679–688. [Google Scholar] [CrossRef]


{kind=link}
| BCT Category | Description of Consumer-Derived BCT | Number and % | |
|---|---|---|---|
| Pre-decisional phase | |||
| Pros and cons | Weigh the available evidence for and against taking action. Pros and cons were focused predominantly on the degree of involvement in the gambling problem and whether to initiate, maintain or avoid engagement. | 148 | 6.1% |
| Realisation | Come to realise, accept or acknowledge the development or presence of gambling harm. Realise the extent of harm and burden on the family. Realise that an action may be required. | 126 | 5.2% |
| Seek knowledge and information | Understand the nature of gambling problems and addiction and possible harm to the family. Information was sought from a wide range of sources including peer-to-peer forums, books and gambling harm reduction websites. | 133 | 5.4% |
| Post-decisional phase | |||
| Goals and plans | Set priorities and goals that are focused on the self or children and other affected others. Establish expectations and convey boundaries for own behaviour on gambling-related issues (e.g., moral but not financial support). | 75 | 3.1% |
| Communication | Establish communication patterns that involve being prepared, enhanced listening skills and methods to communicate own needs. Strategies include communication that is viewed by consumers as unhelpful (accusations, threats, ultimatums, nagging, lecturing or prompting guilt or blame) and helpful (focus on gambling behaviours as being unacceptable rather than the person). | 137 | 5.6% |
| Coping planning | Plan for barriers that might get in the way of behaviour change. Barriers were predominately related to pressure from a gambler requesting money or family member’s pre-existing conditions such as depression or anxiety. | 53 | 2.2% |
| Maintain momentum | Maintain family member’s change in response to general barriers such as shifting readiness, importance and priorities. Families do this through practicing patience, willpower, determination and renewing commitment. | 34 | 1.4% |
| Actional phase | |||
| Avoidance | Distance from the person with the gambling problem. Distance may be physical or psychological. It may involve temporary or permanent separation. Prepare for distancing by establishing financial independence and organising social support, housing and a safety plan. | 160 | 6.5% |
| Behavioural substitution | Refocus away from gambling harm and towards new or improved habits. For family, this included habits that are enjoyable, good for personal development, and can be performed jointly or separately. | 7 | 0.3% |
| Financial management | Act to investigate, audit, assess and address financial harm. Arrange for the repayment of debt and ensure processes in place to stem the flow of cash for gambling. Install safeguards to protect current and future assets. | 334 | 13.7% |
| Planned consequences | Reinforce desired behaviour of the gambler through selective rewards and exposure to negative consequences. Look at role of affected others in current and past reinforcement (e.g., enabling behaviours). | 289 | 11.8% |
| Professional support | Seek support, advice or treatment from professionals or treatment services. This includes seeking expertise from peer support groups and in psychology, psychiatry, medicine, finances, law, housing, and family violence. Reasons are to learn new skills, build confidence and increase support network. | 547 | 22.4% |
| Social support | Identify the different types of social support such as practical or emotional. Develop a willingness and skills to ask and receive support. Be a support person for others, as well as share information and updates with family. Get and give inspiration to other people. | 117 | 4.8% |
| Stress management | Identify the signs of stress and how stress can make it difficult to respond to gambling harm. Enact strategies to manage stress including self-care, self-talk, and relaxation. Improve resilience through healthy diet, exercise and adequate sleep. Learn to notice and name emotions and respond in a way that is helpful. | 138 | 5.6% |
| Self-monitoring | Establish the focus and methods to monitor behaviours against goals and plans. Monitoring was mostly focused on tracking the gambler’s behaviours against the goals of affected others. This involved regular checking of banking transactions, physical location and questioning the person on their movements. Monitoring was also used to increase gambler’s accountability. | 140 | 5.7% |
| Post-actional phase | |||
| Self-evaluation | Assess attempts of behaviour change to learn from them and decide what to do next. Notice the difference the change in the behaviour have created (e.g., what has improved). | 7 | 0.3% |
| Total | 2445 | 100% | |
| BCT Category | Description of Consumer-Derived BCT | Number and % | |
|---|---|---|---|
| Pre-decisional phase | |||
| Feedback on behaviour | Provide evidence (e.g., bank statements) on how gambling behaviours are causing harm to the family with the intention of prompting increased awareness. Harms can include finances as well as relational, emotional, and physical health. Prompt gambler to take a test to assess their gambling. | 250 | 22.9% |
| Provide information | Provide information on gambling problems and how gambling works. Provide the information in a respectful and direct way, e.g., make it available for the person without pressuring them to read it. | 26 | 2.4% |
| Post-decisional phase | |||
| Coping planning | Help the gambler to plan for lapses and relapses and to manage barriers to change. This focused on identifying and responding to gambling triggers, cravings and urges in a goal-consistent manner. Triggers included underlying causes and/or co-occurring substance use or mental health concerns. Help included practical support such as being a distraction in the moment of an urge. | 39 | 3.6% |
| Goals and plans | Support gambler’s goal setting and planning by offering to jointly construct or discuss the content of goals and plans. Encourage those involved to agree to the outcome of discussion. | 16 | 1.5% |
| Maintain momentum | Support gambler to maintain behaviour change in response to general barriers such as shifting priorities and readiness to change. Understand the nature and pace of behaviour change to support the current level of readiness. Provide encouragement and praise, recognise and celebrate gambler’s achievements. | 24 | 2.2% |
| Actional phase | |||
| Avoidance | Support the person to avoid gambling or gambling triggers through discussion on different options (e.g., self-exclusion). Offer to help with self-exclusion, change passwords, remove betting apps or install blocking software. | 77 | 7.1% |
| Behavioural substitution | Support the gambler to develop interests and hobbies away from gambling. Assist the person to refocus their attention towards family or life without gambling. | 19 | 1.7% |
| Consumption planning | Support the person to reach a goal of gambling reduction through a focus on preparation for a gambling episode. This includes setting a limit for the frequency, time, and amount of expenditure. It also includes enacting strategies during and post-gambling for sticking to these limits. | 12 | 1.1% |
| Finances and cash control | Offer advice, assistance or information on options for financial management and budgeting. This includes debt and bill management. Agree on a method to manage access to cash that may involve affected others offering to oversee the finances for a period of time. | 208 | 19.1% |
| Professional support | Encourage and support treatment seeking. This may involve getting information, offering support to make an appointment, attending an appointment or offering post-appointment support. Professional support includes psychological, psychiatric, medical, or financial advice. Support can involve individual or group, and online, telephone or face-to-face support. | 240 | 22.0% |
| Social support | Families can provide support to the person who gambles and help them to get more support from others. Support can be about helping the gambler to open up about their gambling or during a crisis. | 180 | 16.5% |
| Total | 1091 | 100% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Booth, N.; Dowling, N.A.; Landon, J.; Lubman, D.I.; Merkouris, S.S.; Rodda, S.N. Affected Others Responsivity to Gambling Harm: An International Taxonomy of Consumer-Derived Behaviour Change Techniques. J. Clin. Med. 2021, 10, 583. https://doi.org/10.3390/jcm10040583
Booth N, Dowling NA, Landon J, Lubman DI, Merkouris SS, Rodda SN. Affected Others Responsivity to Gambling Harm: An International Taxonomy of Consumer-Derived Behaviour Change Techniques. Journal of Clinical Medicine. 2021; 10(4):583. https://doi.org/10.3390/jcm10040583
Chicago/Turabian StyleBooth, Natalia, Nicki A. Dowling, Jason Landon, Dan I. Lubman, Stephanie S. Merkouris, and Simone N. Rodda. 2021. "Affected Others Responsivity to Gambling Harm: An International Taxonomy of Consumer-Derived Behaviour Change Techniques" Journal of Clinical Medicine 10, no. 4: 583. https://doi.org/10.3390/jcm10040583