
GamblingLess: A Randomised Trial Comparing Guided and Unguided Internet-Based Gambling Interventions

 , , , , ,
, , , , ,
Abstract
:1. Introduction
1.1. Internet-Based Interventions
1.2. Internet-Based Gambling Interventions
1.3. Characteristics of Gamblers Accessing Internet-Based Interventions
1.4. Factors Associated with Internet-Based Gambling Intervention Outcomes
1.5. Aims and Hypotheses
2. Methods
2.1. Trial Design
2.2. Participant Recruitment and Registration
2.3. Interventions
2.3.1. The GamblingLess Program
2.3.2. Guidance in the GSD condition
2.4. Data Collection
2.4.1. Outcome Measures
2.4.2. Descriptive and Diagnostic Measures
2.4.3. Process Measures
2.5. Randomisation
2.6. Statistical Analyses
2.7. Sample Size
3. Results
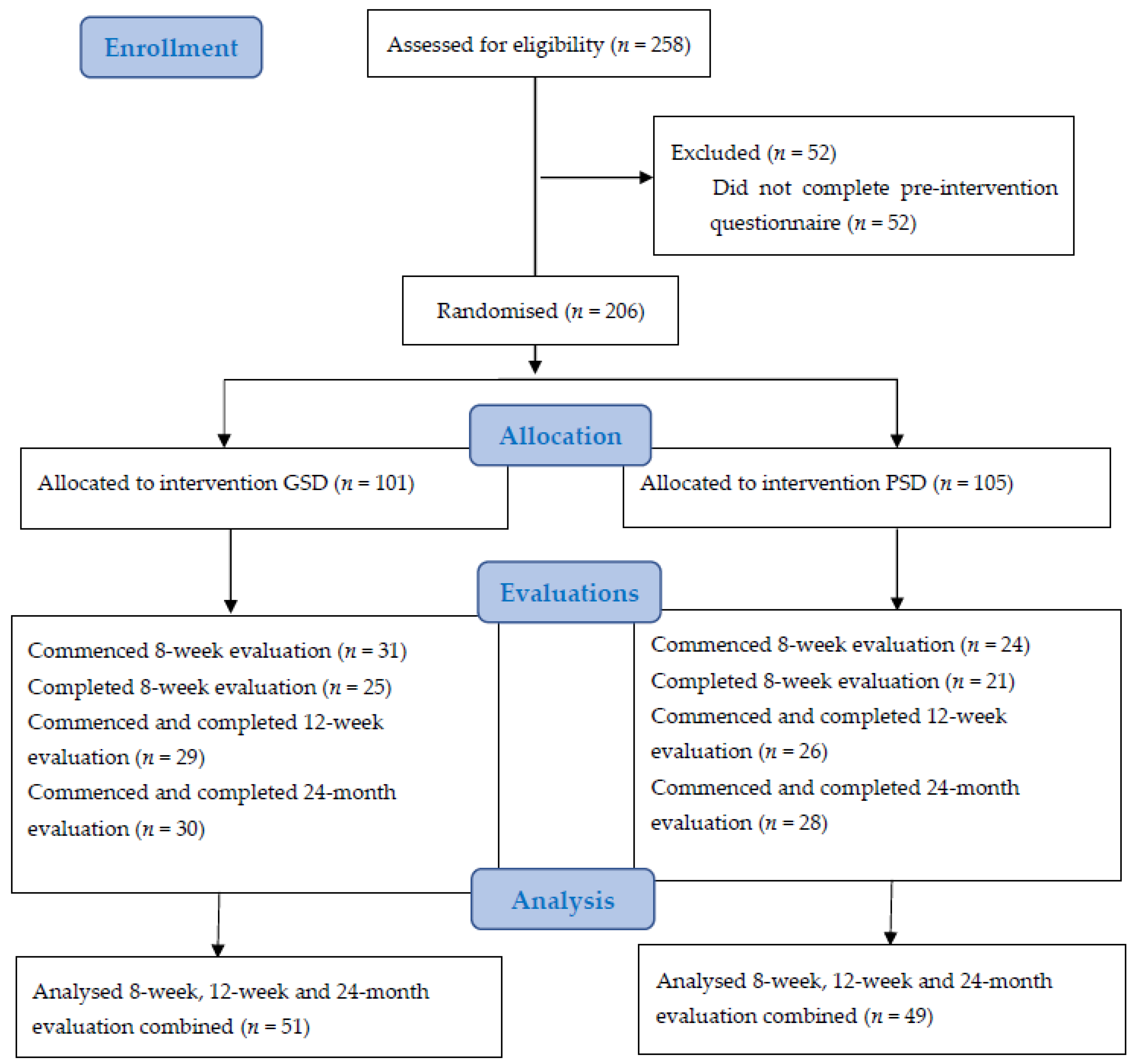
3.1. Participants
3.2. Profile of GamblingLess Users
3.2.1. Socio-Demographic Characteristics
3.2.2. Gambling Behaviour Characteristics
3.2.3. Psychological Characteristics
3.2.4. Treatment Characteristics
3.3. Effectiveness of the GamblingLess Program
3.3.1. Primary Outcome: G-SAS Gambling Symptom Severity
3.3.2. Secondary Outcomes
3.4. Subgroups Benefiting Most from the GamblingLess Program
3.4.1. Predictors of Short-Term Treatment Outcomes
3.4.2. Predictors of Long-Term Treatment Outcomes
3.4.3. Predictors of Treatment Engagement
3.4.4. Predictors of Post-Baseline Evaluation Completion
4. Discussion
4.1. Effectiveness of the GamblingLess Program
4.2. Profile of GamblingLess Users
4.3. Subgroups Benefiting Most from the GamblingLess Program
4.4. Study Limitations
4.5. Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cowlishaw, S.; Merkouris, S.; Dowling, N.; Anderson, C.; Jackson, A.; Thomas, S. Psychological therapies for pathological and problem gambling. Cochrane Database Syst. Rev. 2012, 11, CD008937. [Google Scholar] [CrossRef]
- Gooding, P.; Tarrier, N. A systematic review and meta-analysis of cognitive-behavioural interventions to reduce problem gambling: Hedging our bets? Behav. Res. Ther. 2009, 47, 592–607. [Google Scholar] [CrossRef]
- Thomas, S.A.; Merkouris, S.S.; Radermacher, H.L.; Dowling, N.A.; Misso, M.L.; Anderson, C.J.; Jackson, A.C. Australian guideline for treatment of problem gambling: An abridged outline. Med. J. Aust. 2011, 195, 664–665. [Google Scholar] [CrossRef] [Green Version]
- Yakovenko, I.; Quigley, L.; Hemmelgarn, B.R.; Hodgins, D.C.; Ronksley, P. The efficacy of motivational interviewing for disordered gambling: Systematic review and meta-analysis. Addict. Behav. 2015, 43, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Productivity Commission. Gambling, Report No. 50; Australian Government Productivity Comission: Canberra, Australia, 2010. [Google Scholar]
- Wilson, G.T.; Zandberg, L.J. Cognitive–behavioral guided self-help for eating disorders: Effectiveness and scalability. Clin. Psychol. Rev. 2012, 32, 343–357. [Google Scholar] [CrossRef]
- Suurvali, H.; Cordingley, J.; Hodgins, D.C.; Cunningham, J. Barriers to Seeking Help for Gambling Problems: A Review of the Empirical Literature. J. Gambl. Stud. 2009, 25, 407–424. [Google Scholar] [CrossRef] [PubMed]
- Goslar, M.; Leibetseder, M.; Muench, H.M.; Hofmann, S.G.; Laireiter, A.-R. Efficacy of face-to-face versus self-guided treatments for disordered gambling: A meta-analysis. J. Behav. Addict. 2017, 6, 142–162. [Google Scholar] [CrossRef] [PubMed]
- Bakker, D.; Kazantzis, N.; Rickwood, D.; Rickard, N. Mental Health Smartphone Apps: Review and Evidence-Based Recommendations for Future Developments. JMIR Ment. Health 2016, 3, e7. [Google Scholar] [CrossRef] [Green Version]
- Heron, K.E.; Smyth, J.M. Ecological momentary interventions: Incorporating mobile technology into psychosocial and health behaviour treatments. Br. J. Health Psychol. 2010, 15, 1–39. [Google Scholar] [CrossRef]
- Kim, J.; Marcusson-Clavertz, D.; Yoshiuchi, K.; Smyth, J.M. Potential benefits of integrating ecological momentary assessment data into mHealth care systems. Biopsychosoc. Med. 2019, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Barak, A.; Klein, B.; Proudfoot, J.G. Defining Internet-Supported Therapeutic Interventions. Ann. Behav. Med. 2009, 38, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Barak, A.; Hen, L.; Boniel-Nissim, M.; Shapira, N. A Comprehensive Review and a Meta-Analysis of the Effectiveness of Internet-Based Psychotherapeutic Interventions. J. Technol. Hum. Serv. 2008, 26, 109–160. [Google Scholar] [CrossRef]
- Peñate, W.; Fumero, A. A meta-review of Internet computer-based psychological treatments for anxiety disorders. J. Telemed. Telecare 2016, 22, 3–11. [Google Scholar] [CrossRef]
- White, A.; Kavanagh, D.J.; Stallman, H.M.; Klein, B.; Kay-Lambkin, F.; Proudfoot, J.; Drennan, J.; Connor, J.; Baker, A.; Hines, E.; et al. Online Alcohol Interventions: A Systematic Review. J. Med. Internet Res. 2010, 12, e62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovell, K.; Bower, P.; Richards, D.; Barkham, M.; Sibbald, B.; Roberts, C.; Davies, L.; Rogers, A.; Gellatly, J.; Hennessy, S. Developing guided self-help for depression using the Medical Research Council complex interventions framework: A description of the modelling phase and results of an exploratory randomised controlled trial. BMC Psychiatry 2008, 8, 91. [Google Scholar] [CrossRef] [Green Version]
- Andersson, G.; Carlbring, P.; Berger, T.; Almlöv, J.; Cuijpers, P. What Makes Internet Therapy Work? Cogn. Behav. Ther. 2009, 38, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Donker, T.; Van Straten, A.; Li, J.; Andersson, G. Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychol. Med. 2010, 40, 1943–1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, G.; Penelo, E.; Wanner, C.; Gwinner, P.; Trofaier, M.-L.; Imgart, H.; Waldherr, K.; Wöber-Bingöl, Ç.; Karwautz, A.F.K. Internet-delivered cognitive-behavioural therapy v. conventional guided self-help for bulimia nervosa: Long-term evaluation of a randomised controlled trial. Br. J. Psychiatry 2013, 202, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Wojtowicz, M.; Day, V.; McGrath, P.J. Predictors of Participant Retention in a Guided Online Self-Help Program for University Students: Prospective Cohort Study. J. Med. Internet Res. 2013, 15, e96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karyotaki, E.; Ebert, D.D.; Donkin, L.; Riper, H.; Twisk, J.; Burger, S.; Rozental, A.; Lange, A.; Williams, A.D.; Zarski, A.C.; et al. Do guided internet-based interventions result in clinically relevant changes for patients with depression? An individual participant data meta-analysis. Clin. Psychol. Rev. 2018, 63, 80–92. [Google Scholar] [CrossRef]
- Baumeister, H.; Reichler, L.; Munzinger, M.; Lin, J. The impact of guidance on Internet-based mental health interventions—A systematic review. Internet Interv. 2014, 1, 205–215. [Google Scholar] [CrossRef] [Green Version]
- Bailer, U.; De Zwaan, M.; Leisch, F.; Strnad, A.; Lennkh-Wolfsberg, C.; El-Giamal, N.; Hornik, K.; Kasper, S. Guided self-help versus cognitive-behavioral group therapy in the treatment of bulimia nervosa. Int. J. Eat. Disord. 2004, 35, 522–537. [Google Scholar] [CrossRef] [PubMed]
- Hirai, M.; Clum, G.A. A Meta-Analytic Study of Self-Help Interventions for Anxiety Problems. Behav. Ther. 2006, 37, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.; Schmidt, U.; Treasure, J.; Garthe, R.; Troop, N. Guided Self-Change for Bulimia Nervosa Incorporating Use of a Self-Care Manual. Am. J. Psychiatry 1998, 155, 947–953. [Google Scholar] [CrossRef]
- Isabelle, C.; Christelle, C.; Patrick, R.; Tony, L.; Martial, V.D.L.; Alain, G. Acceptance and Efficacy of a Guided Internet Self-Help Treatment Program for Obese Patients with Binge Eating Disorder. Clin. Pract. Epidemiol. Ment. Health 2011, 7, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Nordgreen, T.; Havik, O.; Öst, L.; Furmark, T.; Carlbring, P.; Andersson, G. Outcome predictors in guided and unguided self-help for social anxiety disorder. Behav. Res. Ther. 2012, 50, 13–21. [Google Scholar] [CrossRef]
- Lynch, F.L.; Striegel-Moore, R.H.; Dickerson, J.F.; Perrin, N.; DeBar, L.; Wilson, G.T.; Kraemer, H.C. Cost-effectiveness of guided self-help treatment for recurrent binge eating. J. Consult. Clin. Psychol. 2010, 78, 322–333. [Google Scholar] [CrossRef]
- Bucker, L.; Bierbrodt, J.; Hand, I.; Wittekind, C.; Moritz, S. Effects of a depression-focused internet intervention in slot machine gamblers: A randomized controlled trial. PLoS ONE 2018, 13, e0198859. [Google Scholar]
- Casey, L.M.; Oei, T.P.S.; Raylu, N.; Horrigan, K.; Day, J.; Ireland, M.; Clough, B.A. Internet-Based Delivery of Cognitive Behaviour Therapy Compared to Monitoring, Feedback and Support for Problem Gambling: A Randomised Controlled Trial. J. Gambl. Stud. 2017, 33, 993–1010. [Google Scholar] [CrossRef]
- Cunningham, J.A.; Godinho, A.; Hodgins, D.C. Pilot randomized controlled trial of an online intervention for problem gamblers. Addict. Behav. Rep. 2019, 9, 100175. [Google Scholar] [CrossRef]
- Cunningham, J.A.; Hodgins, D.C.; Keough, M.; Hendershot, C.S.; Schell, C.; Godinho, A. Online interventions for problem gamblers with and without co-occurring unhealthy alcohol use: Randomized controlled trial. Internet Interv. 2020, 19, 100307. [Google Scholar] [CrossRef]
- Cunningham, J.A.; Hodgins, D.C.; MacKenzie, C.S.; Godinho, A.; Schell, C.; Kushnir, V.; Hendershot, C.S. Randomized controlled trial of an Internet intervention for problem gambling provided with or without access to an Internet intervention for co-occurring mental health distress. Internet Interv. 2019, 17, 100239. [Google Scholar] [CrossRef]
- Hodgins, D.C.; Cunningham, J.A.; Murray, R.; Hagopian, S. Online Self-Directed Interventions for Gambling Disorder: Randomized Controlled Trial. J. Gambl. Stud. 2019, 35, 635–651. [Google Scholar] [CrossRef]
- Carlbring, P.; Degerman, N.; Jonsson, J.; Andersson, G. Internet-Based Treatment of Pathological Gambling with a Three-Year Follow-Up. Cogn. Behav. Ther. 2012, 41, 321–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castrén, S.; Pankakoski, M.; Tamminen, M.; Lipsanen, J.; Ladouceur, R.; Lahti, T. Internet-based CBT intervention for gamblers in Finland: Experiences from the field. Scand. J. Psychol. 2013, 54, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Erevik, E.K.; Pallesen, S.; Mohn, M.; Aspeland, T.; Vedaa, Ø.; Torsheim, T. The Norwegian remote intervention programme for problem gambling: Short- and long-term outcomes. Nord. Stud. Alcohol Drugs 2020, 37, 365–383. [Google Scholar] [CrossRef]
- Myrseth, H.; Brunborg, G.S.; Eidem, M.; Pallesen, S. Description and pre-post evaluation of a telephone and Internet based treatment programme for pathological gambling in Norway: A pilot study. Int. Gambl. Stud. 2013, 13, 205–220. [Google Scholar] [CrossRef]
- Carlbring, P.; Smit, F. Randomized trial of internet-delivered self-help with telephone support for pathological gamblers. J. Consult. Clin. Psychol. 2008, 76, 1090. [Google Scholar] [CrossRef]
- Nilsson, A.; Magnusson, K.; Carlbring, P.; Andersson, G.; Gumpert, C.H. The Development of an Internet-Based Treatment for Problem Gamblers and Concerned Significant Others: A Pilot Randomized Controlled Trial. J. Gambl. Stud. 2018, 34, 539–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, A.; Magnusson, K.; Carlbring, P.; Andersson, G.; Hellner, C. Behavioral couples therapy versus cognitive behavioral therapy for problem gambling: A randomized controlled trial. Addiction 2020, 115, 1330–1342. [Google Scholar] [CrossRef] [Green Version]
- Luquiens, A.; Tanguy, M.-L.; Lagadec, M.; Benyamina, A.; Aubin, H.-J.; Reynaud, M. The Efficacy of Three Modalities of Internet-Based Psychotherapy for Non–Treatment-Seeking Online Problem Gamblers: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e36. [Google Scholar] [CrossRef]
- Rodda, S.; Lubman, D.; Dowling, N.A. Examining the Impact of E-Mental Health in Problem Gambling; Victorian Responsible Gambling Foundation: Melbourne, Australia, 2017. [Google Scholar]
- Rodda, S.; Lubman, D.I. Characteristics of Gamblers Using a National Online Counselling Service for Problem Gambling. J. Gambl. Stud. 2013, 30, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Merkouris, S.; Thomas, S.; Browning, C.; Dowling, N. Predictors of outcomes of psychological treatments for disordered gambling: A systematic review. Clin. Psychol. Rev. 2016, 48, 7–31. [Google Scholar] [CrossRef] [Green Version]
- Beatty, L.; Binnion, C. A Systematic Review of Predictors of, and Reasons for, Adherence to Online Psychological Interventions. Int. J. Behav. Med. 2016, 23, 776–794. [Google Scholar] [CrossRef]
- Melville, K.M.; Casey, L.M.; Kavanagh, D.J. Psychological treatment dropout among pathological gamblers. Clin. Psychol. Rev. 2007, 27, 944–958. [Google Scholar] [CrossRef] [Green Version]
- Rodda, S.; Merkouris, S.; Lavis, T.; Smith, D.; Lubman, D.; Austin, D.; Harvey, P.; Battersby, M.; Dowling, N. The therapist experience of internet delivered CBT for problem gambling: Service integration considerations. Internet Interv. 2019, 18, 100264. [Google Scholar] [CrossRef]
- Merkouris, S.S.; Rodda, S.N.; Austin, D.; Lubman, D.I.; Harvey, P.W.; Battersby, M.W.; Cunningham, J.; Lavis, T.; Smith, D.; Dowling, N.A. GAMBLINGLESS: FOR LIFE study protocol: A pragmatic randomised trial of an online cognitive–behavioural programme for disordered gambling. BMJ Open 2017, 7, e014226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treweek, S.; Zwarenstein, M. Making trials matter: Pragmatic and explanatory trials and the problem of applicability. Trials 2009, 10, 37. [Google Scholar] [CrossRef] [Green Version]
- Riper, H.; Kramer, J.; Smit, F.; Conijn, B.; Schippers, G.; Cuijpers, P. Web-based self-help for problem drinkers: A pragmatic randomized trial. Addiction 2008, 103, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G.; Estling, F.; Jakobsson, E.; Cuijpers, P.; Carlbring, P. Can the Patient Decide Which Modules to Endorse? An Open Trial of Tailored Internet Treatment of Anxiety Disorders. Cogn. Behav. Ther. 2011, 40, 57–64. [Google Scholar] [CrossRef]
- Kim, S.W.; Grant, J.E.; Potenza, M.N.; Blanco, C.; Hollander, E. The Gambling Symptom Assessment Scale (G-SAS): A reliability and validity study. Psychiatry Res. 2009, 166, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Schmidt, S.; Mühlan, H.; Power, M. The EUROHIS-QOL 8-item index: Psychometric results of a cross-cultural field study. Eur. J. Public Health 2005, 16, 420–428. [Google Scholar] [CrossRef]
- Power, M.J. Development of a common instrument for quality of life. In Developing Common Instruments for Health Surveys; Nosikov, A., Gudex, C., Eds.; IOS Press: Amsterdam, The Netherlands, 2003; pp. 145–163. [Google Scholar]
- Rodda, S.; Dowling, N.; Lubman, D. Gamblers seeking online help are active help-seekers: Time to support autonomy and competence. Addict. Behav. 2018, 87, 272–275. [Google Scholar] [CrossRef]
- Ferris, J.; Wynne, H. The Canadian Problem Gambling Index: Final Report; Canadian Centre on Substance Abuse: Ottawa, ON, Canada, 2001. [Google Scholar]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT Alcohol Consumption Questions (AUDIT-C): An Effective Brief Screening Test for Problem Drinking. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.C.; Schmidt, S.M.; Allensworth-Davies, D.; Saitz, R. A Single-Question Screening Test for Drug Use in Primary Care. Arch. Intern. Med. 2010, 170, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Rodda, S.N.; Lubman, D.I.; Iyer, R.; Gao, C.X.; Dowling, N.A. Subtyping based on readiness and confidence: The identification of help-seeking profiles for gamblers accessing web-based counselling. Addiction 2015, 110, 494–501. [Google Scholar] [CrossRef]
- Breslin, F.; Sobell, L.C.; Sobell, M.B.; Agrawal, S. A comparison of a brief and long version of the Situational Confidence Questionnaire. Behav. Res. Ther. 2000, 38, 1211–1220. [Google Scholar] [CrossRef]
- Statistical Software. StataCorp Stata: Release 15; StataCorp LP: College Station, TX, USA, 2017. [Google Scholar]
- Cro, S.; Morris, T.P.; Kenward, M.G.; Carpenter, J.R. Reference-based Sensitivity Analysis via Multiple Imputation for Longitudinal Trials with Protocol Deviation. Stata J. Promot. Commun. Stat. Stata 2016, 16, 443–463. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12. [Google Scholar] [CrossRef]
- Hosmer, D.; Lemeshow, S. Applied Logistic Regression; Johns Wiley & Sons: Hoboken, NJ, USA, 1992. [Google Scholar]
- Milton, S.; Crino, R.; Hunt, C.; Prosser, E. The effect of compliance-improving interventions on the cognitive-behavioural treatment of pathological gambling. J. Gambl. Stud. 2002, 18, 207–229. [Google Scholar] [CrossRef]
- Petry, N.M.; Weinstock, J.; Ledgerwood, D.M.; Morasco, B. A randomized trial of brief interventions for problem and pathological gamblers. J. Consult. Clin. Psychol. 2008, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Coull, G.; Morris, P.G. The clinical effectiveness of CBT-based guided self-help interventions for anxiety and depressive disorders: A systematic review. Psychol. Med. 2011, 41, 2239–2252. [Google Scholar] [CrossRef]
- Browne, M.; Langham, E.; Rawat, V.; Greer, N.; Li, E.; Rose, J.; Rockloff, M.; Donaldson, P.; Thorne, H.; Goodwin, B.; et al. Assessing Gambling-Related Harm in Victoria: A Public Health Perspective; Victorian Responsible Gambling Foundation: Melbourne, Australia, 2016. [Google Scholar]
- Dowling, N.A.; Cowlishaw, S.; Jackson, A.C.; Merkouris, S.S.; Francis, K.L.; Christensen, D.R. Prevalence of psychiatric co-morbidity in treatment-seeking problem gamblers: A systematic review and meta-analysis. Aust. N. Z. J. Psychiatry 2015, 49, 519–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, J.E.; Kim, S.W. Quality of life in kleptomania and pathological gambling. Compr. Psychiatry 2005, 46, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Ledgerwood, D.M.; Petry, N.M. Gambling and Suicidality in Treatment-Seeking Pathological Gamblers. J. Nerv. Ment. Dis. 2004, 192, 711–714. [Google Scholar] [CrossRef]
- Ledgerwood, D.M.; Steinberg, M.A.; Wu, R.; Potenza, M.N. Self-reported gambling-related suicidality among gambling helpline callers. Psychol. Addict. Behav. 2005, 19, 175–183. [Google Scholar] [CrossRef]
- Dowling, N.A.; Cowlishaw, S.; Jackson, A.C.; Merkouris, S.S.; Francis, K.L.; Christensen, D.R. The Prevalence of Comorbid Personality Disorders in Treatment-Seeking Problem Gamblers: A Systematic Review and Meta-Analysis. J. Pers. Disord. 2015, 29, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.; Jackson, A.; Suomi, A.; Lavis, T.; Thomas, S.; Patford, J.; Harvey, P.; Battersby, M.; Koziol-McLain, J.; Abbott, M.; et al. Problem gambling and family violence: Prevalence and patterns in treatment-seekers. Addict. Behav. 2014, 39, 1713–1717. [Google Scholar] [CrossRef] [Green Version]
- Petry, N.M. Pathological Gambling: Etiology, Comorbidity, and Treatment; American Psychological Association (APA): Washington, DC, USA, 2005; Volume 2. [Google Scholar]
- Westphal, J.R.; Johnson, L.J. Multiple Co-occurring Behaviours among Gamblers in Treatment: Implications and Assessment. Int. Gambl. Stud. 2007, 7, 73–99. [Google Scholar] [CrossRef]
- Dowling, N.; Smith, D. Treatment Goal Selection for Female Pathological Gambling: A Comparison of Abstinence and Controlled Gambling. J. Gambl. Stud. 2007, 23, 335–345. [Google Scholar] [CrossRef]
- Ladouceur, R. Controlled Gambling for Pathological Gamblers. J. Gambl. Stud. 2005, 21, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Robson, E.; Edwards, J.; Smith, G.; Colman, I. Gambling decisions: An early intervention program for problem gamblers. J. Gambl. Stud. 2002, 18, 235–255. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.A. The selection of controlled gambling in Australian problem gambling treatment services. In Proceedings of the 42nd Australian Psychological Society, Brisbane, QLD, Australia, 25–29 September 2007. [Google Scholar]
- Murray, E.; Khadjesari, Z.; White, I.R.; Kalaitzaki, E.; Godfrey, C.; McCambridge, J.; Thompson, S.G.; Wallace, P.; Riper, M.; Eapen, B.; et al. Methodological Challenges in Online Trials. J. Med. Internet Res. 2009, 11, e9. [Google Scholar] [CrossRef] [PubMed]
- Donkin, L.; Christensen, H.; Naismith, S.L.; Neal, B.; Hickie, I.B.; Glozier, N. A Systematic Review of the Impact of Adherence on the Effectiveness of e-Therapies. J. Med. Internet Res. 2011, 13, e52. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. The Law of Attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef] [PubMed]
- Melville, K.M.; Casey, L.M.; Kavanagh, D.J. Dropout from Internet-based treatment for psychological disorders. Br. J. Clin. Psychol. 2010, 49, 455–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verheijden, M.W.; Jans, M.P.; Hildebrandt, V.H.; Hopman-Rock, M. Rates and Determinants of Repeated Participation in a Web-Based Behavior Change Program for Healthy Body Weight and Healthy Lifestyle. J. Med. Internet Res. 2007, 9, e1. [Google Scholar] [CrossRef] [Green Version]
- Christensen, H.; Griffiths, K.M.; Farrer, L. Adherence in internet interventions for anxiety and depression: Systematic review. J. Med. Internet Res. 2009, 11, e13. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.A.; Cosic, S. Client Engagement Characteristics Associated with Problem Gambling Treatment Outcomes. Int. J. Ment. Health Addict. 2010, 9, 656–671. [Google Scholar] [CrossRef]
- Ghaderi, A. Attrition and outcome in self-help treatment for bulimia nervosa and binge eating disorder: A constructive replication. Eat. Behav. 2006, 7, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Walker, M.; Toneatto, T.; Potenza, M.N.; Petry, N.; Ladouceur, R.; Hodgins, D.C.; El-Guebaly, N.; Echeburúa, E.; Blaszczynski, A. A framework for reporting outcomes in problem gambling treatment research: The Banff, Alberta Consensus. Addiction 2006, 101, 504–511. [Google Scholar] [CrossRef]
- Barak, A.; Buchanan, T. Internet-based psychological testing and assessment. In Online Counseling: A Handbook for Mental Health Professionals; Kraus, R., Stricker, G., Speyer, C., Eds.; Elsevier Academic Press: London, UK, 2004. [Google Scholar]
- Wangberg, S.C.; Bergmo, T.S.; Johnsen, J.-A.K. Adherence in Internet-based interventions. Patient Prefer. Adherence 2008, 2, 57–65. [Google Scholar]
- Holtrop, J.S.; Wadland, W.C.; Vansen, S.; Weismatel, D.; Fadel, H. Recruting health plan members receiving pharcotherapy into smoking cessation counseling. Am. J. Manag. Care 2005, 11, 501–507. [Google Scholar] [PubMed]
- Rodondi, N.; Humair, J.-P.; Ghali, W.A.; Ruffieux, C.; Stoianov, R.; Seematter-Bagnoud, L.; Stalder, H.; Pecoud, A.; Cornuz, J. Counselling overweight and obese patients in primary care: A prospective cohort study. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 222–228. [Google Scholar] [CrossRef]
- Topolovec-Vranic, J.; Cullen, N.; Michalak, A.; Ouchterlony, D.; Bhalerao, S.; Masanic, C.; Cusimano, M.D. Evaluation of an online cognitive behavioural therapy program by patients with traumatic brain injury and depression. Brain Inj. 2010, 24, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Postel, M.G.; de Haan, H.A.; ter Huurne, E.D.; Becker, E.S.; de Jong, C.A. Effectiveness of a web-based intervention for problem drinkers and reasons for dropout: Randomized controlled trial. J. Med. Internet Res. 2010, 12, e68. [Google Scholar] [CrossRef]
- Andersson, G.; Strömgren, T.; Ström, L.; Lyttkens, L. Randomized Controlled Trial of Internet-Based Cognitive Behavior Therapy for Distress Associated with Tinnitus. Psychosom. Med. 2002, 64, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Bagot, K.L.; Dowling, N.A.; Merkouris, S.S.; Youssef, G.J.; Portogallo, H.; Lubman, D.I.; Hawker, C.O.; Rodda, S.N. Gambling Habit Hacker: Protocol for a micro-randomised trial of a gambling Just-In-Time Adaptive Intervention. 2021, in press. [Google Scholar]
- Dowling, N.A.; Merkouris, S.S.; Rodda, S.N.; Youssef, G.J.; Bagot, K.L.; Hawker, C.O.; Portogallo, H.; Lubman, D.I. GAMBLINGLESS IN-THE-MOMENT: Protocol for a micro-randomised trial of a gambling Just-In-Time Adaptive Intervention. 2021, in press. [Google Scholar]
- Dowling, N.A.; Rodda, S.N.; Merkouris, S.S.; Youssef, G.J.; Bagot, K.L.; Hawker, C.O.; POrtogallo, H.; Lubman, D.I. Applying the Just-In-Time Adaptive Intervention framework to the development of gambling interventions. 2021, in press. [Google Scholar]
- Hawker, C.O.; Merkouris, S.S.; Youssef, G.J.; Dowling, N.A. GAMBLINGLESS: CURB YOUR URGE: An acceptability and feasibility trial of a smartphone-delivered ecological momentary intervention for problem gambling (Preprint). J. Med. Internet Res. 2021, 33, e25786. [Google Scholar] [CrossRef]
- Humphrey, G.; Chu, J.; Dowling, N.; Rodda, S.; Merkouris, S.; Parag, V.; Newcombe, D.; Ho, E.; Nosa, V.; Ruwhui-Collins, R. Manaaki–A cognitive behavioral therapy mobile health app to support people experiencing gambling problems: A randomized control trial protocol. BMC Public Health 2020, 20, 191. [Google Scholar] [CrossRef]
- Merkouris, S.S.; Hawker, C.O.; Rodda, S.N.; Youssef, G.J.; Dowling, N.A. GamblingLess: Curb Your Urge: Development and usability testing of a smartphone-delivered ecological momentary intervention for problem gambling. Int. Gambl. Stud. 2020, 20, 515–538. [Google Scholar] [CrossRef]
- Proudfoot, J.; Parker, G.; Manicavasagar, V.; Hadzi-Pavlovic, D.; Whitton, A.; Nicholas, J.; Smith, M.; Burckhardt, R. Effects of adjunctive peer support on perceptions of illness control and understanding in an online psychoeducation program for bipolar disorder: A randomised controlled trial. J. Affect. Disord. 2012, 142, 98–105. [Google Scholar] [CrossRef]
- Simon, G.E.; Ludman, E.J.; Goodale, L.C.; Dykstra, D.M.; Stone, E.; Cutsogeorge, D.; Operskalski, B.; Savarino, J.; Pabiniak, C. An online recovery plan program: Can peer coaching increase participation? Psychiatr. Serv. 2011, 62, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Johansson, R.; Andersson, G. Internet-based psychological treatments for depression. Expert Rev. Neurother. 2012, 12, 861–870. [Google Scholar] [CrossRef] [Green Version]
- Palmqvist, B.; Carlbring, P.; Andersson, G. Internet-delivered treatments with or without therapist input: Does the therapist factor have implications for efficacy and cost? Expert Rev. Pharm. Outcomes Res. 2007, 7, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Choudhury, T.; Patrick, K.; Michie, S. Current Issues and Future Directions for Research into Digital Behavior Change Interventions. Am. J. Prev. Med. 2016, 51, 814–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Socio-Demographic Characteristic | Pure Self-Directed (n = 105) | Guided Self-Directed (n = 101) | Total (n = 206) |
|---|---|---|---|
| Sex (n, % male) | 67 (63.8) | 66 (65.3) | 133 (64.6) |
| Age group in years (n, %) | |||
| 18–24 | 17 (16.2) | 24 (23.8) | 41 (19.9) |
| 25–29 | 17 (16.2) | 20 (19.8) | 37 (18.0) |
| 30–34 | 15 (14.3) | 9 (8.9) | 24 (11.7) |
| 35–39 | 18 (17.1) | 11 (10.9) | 29 (14.1) |
| 40–44 | 11 (10.5) | 9 (8.9) | 20 (9.7) |
| 45–49 | 6 (5.7) | 10 (9.9) | 16 (7.8) |
| 50–54 | 10 (9.5) | 10 (9.9) | 20 (9.7) |
| 55+ | 11 (10.5) | 8 (7.9) | 19 (9.2) |
| Country of birth (n, % Australia) | 81 (77.1) | 76 (75.3) | 157 (76.2) |
| Employment (n, %) | |||
| Work full time | 77 (73.3) | 70 (69.3) | 147 (71.4) |
| Work part time/casual | 13 (12.4) | 22 (21.8) | 35 (17.0) |
| Unemployed | 5 (4.8) | 2 (2.0) | 7 (3.4) |
| Full time student | 3 (2.9) | 1 (1.0) | 4 (1.9) |
| Full-time home duties | 1 (1.0) | 1 (1.0) | 2 (1.0) |
| Retired | 3 (2.9) | 0 (0) | 3 (1.5) |
| Sick or disability pension | 2 (1.9) | 4 (4.0) | 6 (2.9) |
| Other | 1 (1.0) | 1 (1.0) | 2 (1.0) |
| Annual personal net income (n, %) | |||
| <AUD$25,000 | 13 (12.4) | 10 (9.9) | 23 (11.2) |
| AUD$25,000–$39,999 | 18 (17.1) | 14 (13.9) | 32 (15.5) |
| AUD$40,000–$64,999 | 28 (26.7) | 41 (40.6) | 69 (33.5) |
| AUD$65,000–$79,999 | 20 (19.1) | 17 (16.8) | 37 (18.0) |
| AUD$80,000–$129,999 | 18 (17.1) | 15 (14.9) | 33 (16.0) |
| AUD$130,000+ | 8 (7.6) | 4 (4.0) | 12 (5.8) |
| Internet use (hours) (n, %) a | |||
| Less than 1 | 6 (5.7) | 2 (2.0) | 8 (3.9) |
| 1–7 | 25 (23.8) | 19 (18.8) | 44 (21.4) |
| 8–14 | 29 (27.6) | 28 (27.7) | 57 (27.7) |
| 15–21 | 15 (14.3) | 22 (21.8) | 37 (18.0) |
| 22–28 | 7 (6.7) | 7 (6.9) | 14 (6.8) |
| 29–35 | 8 (7.6) | 6 (5.9) | 14 (6.8) |
| 36–42 | 3 (2.9) | 9 (8.9) | 12 (5.8) |
| More than 42 | 12 (11.4) | 8 (7.9) | 20 (9.7) |
| Outcome | Baseline | 8 Weeks | 12 Weeks | 24 Months | ||||
|---|---|---|---|---|---|---|---|---|
| PSD (n = 50) | GSD (n = 51) | PSD (n = 22) | GSD (n = 28) | PSD (n = 26) | GSD (n = 29) | PSD (n = 28) | GSD (n = 30) | |
| G-SAS gambling symptom severity a | 30.12 (7.92) | 27.94 (7.97) | 17.50 (11.91) | 19.45 (11.82) | 20.42 (10.63) | 15.14 (9.91) | 19.79 (10.90) | 13.87 (10.88) |
| G-SAS gambling urges a | 10.18 (2.84) | 9.06 (2.77) | 6.13 (4.71) | 6.94 (4.17) | 7.15 (4.10) | 5.14 (3.54) | 6.89 (3.95) | 3.93 (3.94) |
| Gambling frequency b | 13.20 (11.57) | 14.43 (19.64) | 6.14 (7.89) | 6.82 (8.58) | 7.88 (8.50) | 3.72 (4.71) | 14.89 (17.58) | 11.57 (21.23) |
| Gambling expenditure (AUD$) b | 3590 (6923) | 2579 (5096) | 511 (1123) | 664 (1037) | 747 (973) | 272 (352) | 1511 (2497) | 1027 (1657) |
| K6 psychological distress a | 16.74 (5.92) | 17.24 (5.56) | 12.50 (4.98 | 13.93 (5.96) | 14.00 (6.01) | 12.66 (6.30) | 13.64 (4.98) | 12.17 (4.57) |
| EUROHIS quality of life a | 3.32 (1.15) | 3.35 (1.04) | 3.68 (0.84) | 3.57 (1.00) | 3.31 (1.01) | 3.79 (0.90) | 3.43 (1.03) | 3.83 (0.79) |
| HSQ high-intensity help-seeking a,b | 0.32 (0.68) | 0.31 (0.73) | 0.32 (0.57) | 0.32 (0.72) | 0.58 (0.95) | 0.52 (0.78) | 0.46 (0.88) | 0.20 (0.41) |
| HSQ low-intensity help-seeking a,b | 0.14 (0.40) | 0.20 (0.57) | 0.05 (0.21) | 0.32 (0.48) | 0.27 (0.53) | 0.28 (0.59) | 0.18 (0.55) | 0.10 (0.55) |
| Outcome | Unadjusted Estimate (SE) | Estimated Between-Group Difference (95% CI) | p | |||
|---|---|---|---|---|---|---|
| Baseline | 8 Weeks | 12 Weeks | 24 Months | |||
| G-SAS gambling symptom severity b | - | −0.32 (0.19) | −0.47 (0.29) | −3.78 (2.29) | −0.16 (−0.34, 0.03) c | 0.098 |
| G-SAS gambling urges b | - | −0.18 (0.07) | −0.27 (0.10) | −2.17 (0.84) | −0.09 (−0.16, −0.02) c | 0.010 |
| Gambling frequency | - | − | − | − | 0.95 (0.91, 1.00) d | 0.046 |
| Gambling expenditure | - | − | − | − | 0.99 (0.94, 1.04) d | 0.667 |
| K6 psychological distress b | - | −0.05 (0.10) | −0.08 (0.15) | −0.64 (1.18) | −0.03 (−0.12, 0.07) c | 0.585 |
| EUROHIS quality of life b | - | 0.02 (0.02) | 0.03 (0.03) | 0.26 (0.21) | 0.01 (−0.01, 0.03) c | 0.210 |
| HSQ high-intensity help-seeking b | - | − | − | − | 0.98 (0.91, 1.06) e | 0.660 |
| HSQ low-intensity help-seeking b | - | − | − | − | 0.93 (0.83, 1.03) e | 0.157 |
| Outcome | Treatment Group | Unadjusted Estimate (SE) | Estimated Within-Group Difference (95% CI) | p | |||
|---|---|---|---|---|---|---|---|
| Baseline | 8 Weeks | 12 Weeks | 24 Months | ||||
| G-SAS gambling symptom severity b | PSD | 29.69 (1.39) | 21.50 (1.32) | 17.90 (1.59) | 18.43 (1.85) | −4.42 (−5.70, −3.15) c | <0.001 |
| GSD | 27.92 (1.35) | 19.29 (1.22) | 15.48 (1.48) | 13.84 (1.68) | −4.66 (−5.90, −3.41) c | <0.001 | |
| G-SAS gambling urges b | PSD | 10.05 (0.52) | 7.55 (0.50) | 6.45 (0.60) | 6.54 (0.65) | −1.35 (−1.81, −0.88) c | <0.001 |
| GSD | 9.10 (0.47) | 6.63 (0.42) | 5.53 (0.52) | 3.95 (0.64) | −1.33 (−1.77, −0.89) c | <0.001 | |
| Gambling frequency | PSD | - | −0.82 (0.31) | −1.17 (0.44) | −0.89 (0.46) | 0.64 (0.46, 0.89) d | 0.007 |
| GSD | - | −1.76 (0.35) | −2.52 (0.50) | −1.38 (0.48) | 0.39 (0.27, 0.56) d | <0.001 | |
| Gambling expenditure | PSD | - | −1.91 (0.41) | −2.75 (0.58) | −1.77 (0.60) | 0.35 (0.23, 0.55) d | <0.001 |
| GSD | - | −1.84 (0.35) | −2.64 (0.50) | −1.70 (0.54) | 0.37 (0.25, 0.54) d | <0.001 | |
| K6 psychological distress b | PSD | 16.57 (0.77) | 14.36 (0.75) | 13.38 (0.85) | 12.39 (0.91) | −1.19 (−1.76, −0.62) c | <0.001 |
| GSD | 17.19 (0.76) | 13.89 (0.70) | 12.43 (0.85) | 12.11 (0.94) | −1.78 (−2.47, −1.09) c | <0.001 | |
| EUROHIS quality of life b | PSD | 3.35 (0.15) | 3.44 (0.14) | 3.48 (0.16) | 3.57 (0.18) | 0.05 (−0.07, 0.17) c | 0.423 |
| GSD | 3.35 (0.13) | 3.61 (0.12) | 3.73 (0.14) | 3.85 (0.16) | 0.14 (0.03, 0.25) c | 0.013 | |
| HSQ high-intensity help-seeking b | PSD | −2.12 (0.64) | −1.51 (0.57) | −1.24 (0.65) | −1.88 (0.75) | 1.39 (0.84, 2.31) e | 0.199 |
| GSD | −1.87 (0.52) | −1.38 (0.43) | −1.17 (0.51) | −1.96 (0.65) | 1.31 (0.84, 2.05) e | 0.239 | |
| HSQ low-intensity help-seeking b | PSD | −2.26 (0.55) | −1.88 (0.45) | −1.71 (0.55) | −2.27 (0.72) | 1.23 (0.74, 2.06) e | 0.422 |
| GSD | −1.84 (0.47) | −1.33 (0.37) | −1.12 (0.44) | −3.57 (1.11) | 1.33 (0.87, 2.04) e | 0.189 | |
| 8 weeks | PSD (n = 24) | GSD (n = 31) | Total (n = 55) |
| Recovered | 14 (58.3) | 12 (38.7) | 26 (47.3) |
| Improved | 2 (8.3) | 6 (19.4) | 8 (14.6) |
| Unchanged | 7 (29.2) | 12 (38.7) | 19 (34.6) |
| Deteriorated | 1 (4.2) | 1 (3.2) | 2 (3.6) |
| 12 weeks | PSD (n = 26) | GSD (n = 29) | Total (n = 55) |
| Recovered | 9 (34.6) | 18 (62.1) | 27 (49.1) |
| Improved | 8 (30.8) | 2 (6.9) | 10 (18.2) |
| Unchanged | 9 (34.6) | 8 (27.6) | 17 (30.9) |
| Deteriorated | 0 (0.0) | 1 (3.5) | 1 (1.8) |
| 24 months | PSD (n = 28) | GSD (n = 30) | Total (n = 58) |
| Recovered | 12 (42.9) | 21 (70.0) | 33 (56.9) |
| Improved | 5 (17.9) | 2 (6.7) | 7 (12.1) |
| Unchanged | 11 (39.3) | 7 (23.3) | 18 (31.0) |
| Deteriorated | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dowling, N.A.; Merkouris, S.S.; Rodda, S.N.; Smith, D.; Aarsman, S.; Lavis, T.; Lubman, D.I.; Austin, D.W.; Cunningham, J.A.; Battersby, M.W.; et al. GamblingLess: A Randomised Trial Comparing Guided and Unguided Internet-Based Gambling Interventions. J. Clin. Med. 2021, 10, 2224. https://doi.org/10.3390/jcm10112224
Dowling NA, Merkouris SS, Rodda SN, Smith D, Aarsman S, Lavis T, Lubman DI, Austin DW, Cunningham JA, Battersby MW, et al. GamblingLess: A Randomised Trial Comparing Guided and Unguided Internet-Based Gambling Interventions. Journal of Clinical Medicine. 2021; 10(11):2224. https://doi.org/10.3390/jcm10112224
Chicago/Turabian StyleDowling, Nicki A., Stephanie S. Merkouris, Simone N. Rodda, David Smith, Stephanie Aarsman, Tiffany Lavis, Dan I. Lubman, David W. Austin, John A. Cunningham, Malcolm W. Battersby, and et al. 2021. "GamblingLess: A Randomised Trial Comparing Guided and Unguided Internet-Based Gambling Interventions" Journal of Clinical Medicine 10, no. 11: 2224. https://doi.org/10.3390/jcm10112224