
Erythema Increase Predicts Psoriasis Improvement after Phototherapy


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
2.3. Study Population
- Controls were healthy volunteers, gender- and age-matched (±3 years) with psoriasis patients. These volunteers were people who attended the Dermatology Department for trivial conditions such as melanocytic nevi or seborrheic keratoses. The same criteria were used to select the non-exposed group in the prospective study.
- For psoriasis patients, currently having non-plaque forms of psoriasis.
- For healthy volunteers, having previous personal or family history of any inflammatory skin disease.
- Clinical infection on the treatment area.
- History of cancer or an immunocompromised disease.
- Not signing the informed consent form.
2.4. Follow-Up and Exposure
2.5. Variables
- Clinical and sociodemographic variables. Gender, age, smoking and alcohol habit, psoriasis family history, and use of emollients were gathered by means of clinical interview. Psoriasis severity was assessed by the PASI and the body surface area (BSA). Every study patient was also evaluated with the Dermatology Life Quality Index (DLQI). Information about disease duration, previous treatment, the previous number of phototherapy sessions, session dose, and total cumulative dose was also collected.
- Epidermal barrier function variables. Homeostasis parameters related to epidermal barrier function and skin homeostasis were measured. SCH (in arbitrary units, using Corneometer®CM825), TEWL (in g·m−2·h−1, using Tewameter®TM300), pH (using Skin-pH-Meter®PH905), erythema index (in arbitrary units, using Mexameter®MX18), sebum (in arbitrary units, usingSebumeter®SM815), and skin temperature (in °C, using Skin-ThermometerST500) were measured by a Multi Probe Adapter (MPA, Courage + Khazaka electronic GmbH, Köln, Germany). Total antioxidant capacity (TAC) was measured using eBQC® electrochemical method (Bioquochem S.L. (BQCkit), Asturias, Spain), and expressed in microcoulombs. TAC is divided into two sections: fast antioxidants (Q1), which have a lower oxidation potential, and slow antioxidants (Q2) [26]. All variables were measured at a psoriatic plaque on the elbow and at an uninvolved skin area near the elbow in psoriatic patients, while healthy subjects were measured at a skin area on their elbows. All parameters were measured ten times for each area, using their average for analysis. The measurements were taken in the same room. The average ambient air temperature at the time of the study was 22 ± 1°C, and the average ambient air humidity was 45% ± 3%.
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Skin Homeostasis Parameters between Healthy Participants and Psoriatic Patients
3.2. Differences in Skin Homeostasis Parameters after One Phototherapy Session
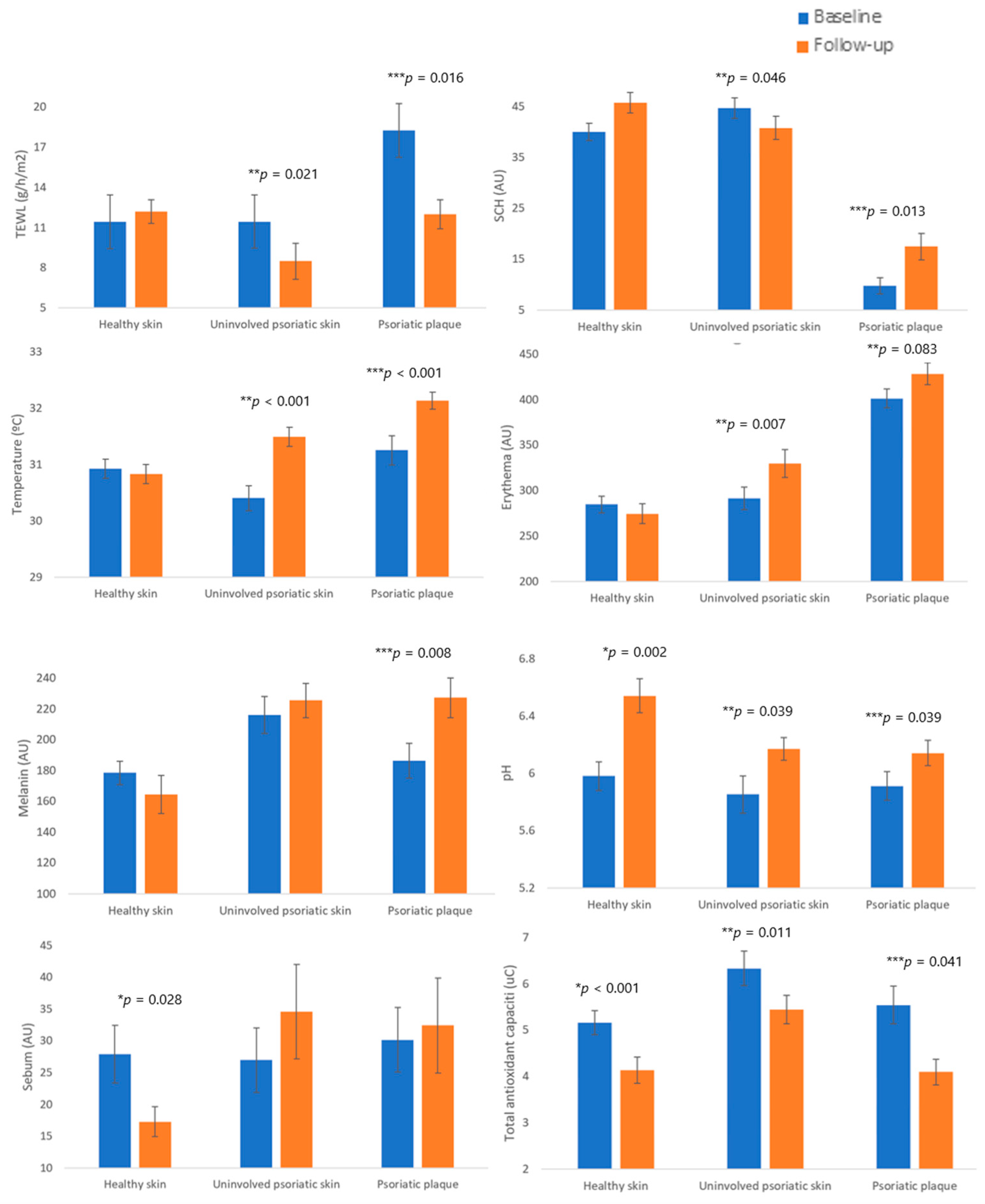
3.3. Skin Homeostasis Changes after Follow-Up
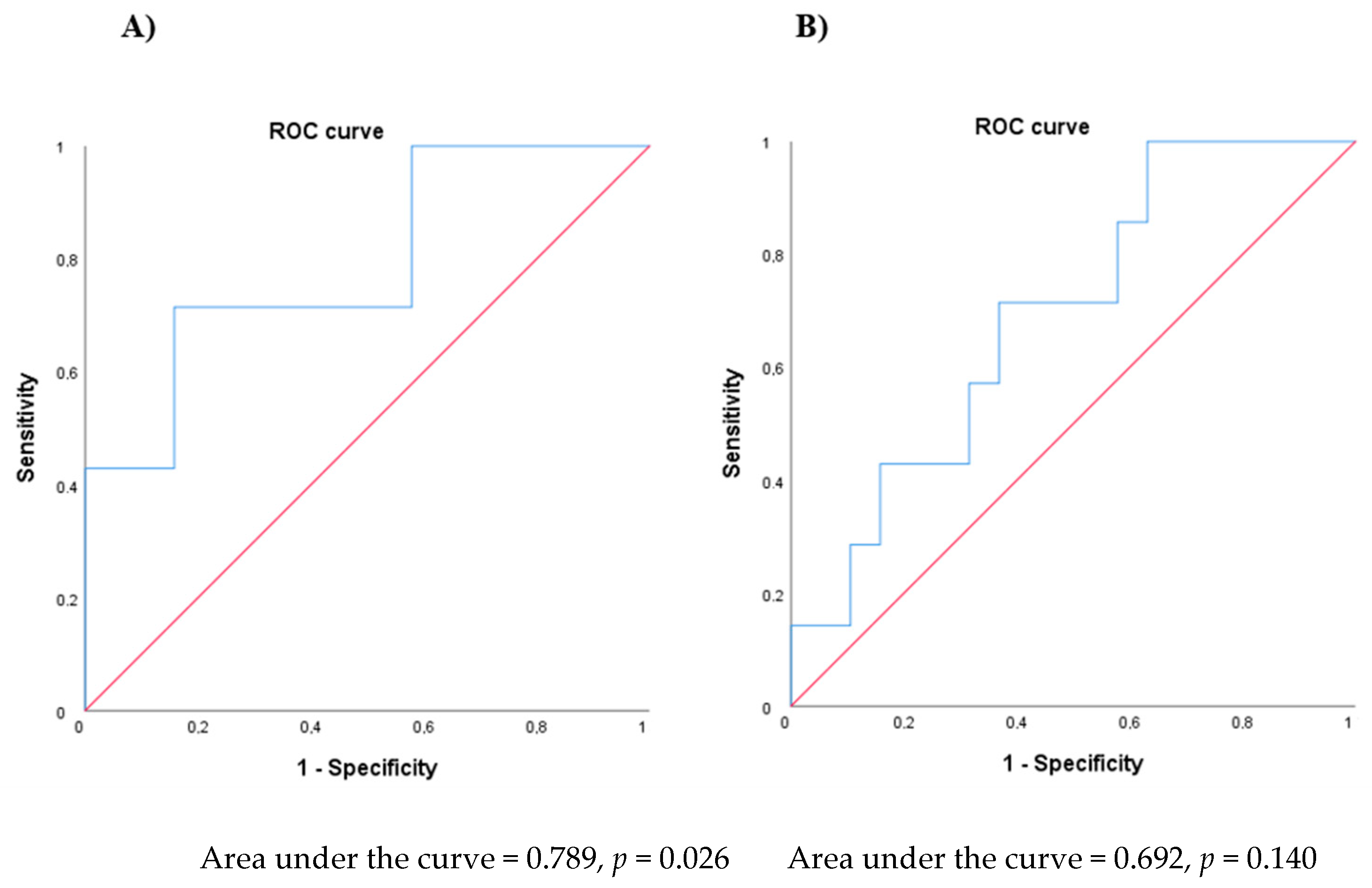
3.4. Skin Homeostasis Predicts PASI Improvement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boehncke, W.H.; Schon, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Frischknecht, L.; Vecellio, M.; Selmi, C. The role of epigenetics and immunological imbalance in the etiopathogenesis of psoriasis and psoriatic arthritis. Ther. Adv. Musculoskelet Dis. 2019, 11, 1759720X19886505. [Google Scholar] [CrossRef]
- Michalek, I.M.; Loring, B.; John, S.M. A systematic review of worldwide epidemiology of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 205–212. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Organization. EXECUTIVE BOARD. EB133/5. 133rd Session. 5 April 2013. Provisional Agenda Item 6.2. Psoriasis. 2013. Available online: https://apps.who.int/gb/ebwha/pdf_files/EB133/B133_5-en.pdf (accessed on 13 May 2020).
- Mehrmal, S.; Uppal, P.; Nedley, N.; Giesey, R.L.; Delost, G.R. The global, regional, and national burden of psoriasis in 195 countries and territories, 1990 to 2017: A systematic analysis from the Global Burden of Disease Study 2017. J. Am. Acad. Dermatol. 2021, 84, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Arias-Santiago, S.; Orgaz-Molina, J.; Castellote-Caballero, L.; Arrabal-Polo, M.A.; Garcia-Rodriguez, S.; Perandres-Lopez, R. Atheroma plaque, metabolic syndrome and inflammation in patients with psoriasis. Eur. J. Dermatol. 2012, 22, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Lopez, A.; Blasco-Morente, G.; Giron-Prieto, M.S.; Arrabal-Polo, M.A.; Luque-Valenzuela, M.; Luna-Del Castillo, J.D. Linking of psoriasis with osteopenia and osteoporosis: A cross-sectional study. Indian J. Dermatol. Venereol. Leprol. 2019, 85, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Oliveira Mde, F.; Rocha Bde, O.; Duarte, G.V. Psoriasis: Classical and emerging comorbidities. An. Bras. Dermatol. 2015, 90, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Orgaz-Molina, J.; Buendia-Eisman, A.; Arrabal-Polo, M.A.; Ruiz, J.C.; Arias-Santiago, S. Deficiency of serum concentration of 25-hydroxyvitamin D in psoriatic patients: A case-control study. J. Am. Acad. Dermatol. 2012, 67, 931–938. [Google Scholar] [CrossRef]
- Martinez-Garcia, E.; Arias-Santiago, S.; Valenzuela-Salas, I.; Garrido-Colmenero, C.; Garcia-Mellado, V.; Buendia-Eisman, A. Quality of life in persons living with psoriasis patients. J. Am. Acad. Dermatol. 2014, 71, 302–307. [Google Scholar] [CrossRef]
- Feldman, S.R.; Burudpakdee, C.; Gala, S.; Nanavaty, M.; Mallya, U.G. The economic burden of psoriasis: A systematic literature review. Expert Rev. Pharmacoecon. Outcomes Res. 2014, 14, 685–705. [Google Scholar] [CrossRef]
- Stiff, K.M.; Glines, K.R.; Porter, C.L.; Cline, A.; Feldman, S.R. Current pharmacological treatment guidelines for psoriasis and psoriatic arthritis. Expert Rev. Clin. Pharmacol. 2018, 11, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Florek, A.G.; Wang, C.J.; Armstrong, A.W. Treatment preferences and treatment satisfaction among psoriasis patients: A systematic review. Arch. Dermatol. Res. 2018, 310, 271–319. [Google Scholar] [CrossRef] [PubMed]
- Bozek, A.; Reich, A. The reliability of three psoriasis assessment tools: Psoriasis area and severity index, body surface area and physician global assessment. Adv. Clin. Exp. Med. 2017, 26, 851–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albaghdadi, A. Current and Under Development Treatment Modalities of Psoriasis: A Review. Endocr. Metab. Immune Disord. Drug Targets 2017, 17, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Yanovsky, R.L.; Huang, K.P.; Buzney, E.A. Optimizing Narrowband UVB Phototherapy Regimens for Psoriasis. Dermatol. Clin. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Elmets, C.A.; Lim, H.W.; Stoff, B.; Connor, C.; Cordoro, K.M.; Lebwohl, M. Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management and treatment of psoriasis with phototherapy. J. Am. Acad. Dermatol. 2019, 81, 775–804. [Google Scholar] [CrossRef] [Green Version]
- Hung, R.; Ungureanu, S.; Edwards, C.; Gambles, B.; Anstey, A.V. Home phototherapy for psoriasis: A review and update. Clin. Exp. Dermatol. 2015, 40, 827–833, quiz 32-3. [Google Scholar] [CrossRef]
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. N. Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef]
- Yu, Z.; Wolf, P. How It Works: The Immunology Underlying Phototherapy. Dermatol. Clin. 2020, 38, 37–53. [Google Scholar] [CrossRef]
- Takahashi, H.; Tsuji, H.; Minami-Hori, M.; Miyauchi, Y.; Iizuka, H. Defective barrier function accompanied by structural changes of psoriatic stratum corneum. J. Dermatol. 2014, 41, 144–148. [Google Scholar] [CrossRef]
- Nikam, V.N.; Monteiro, R.C.; Dandakeri, S.; Bhat, R.M. Transepidermal Water Loss in Psoriasis: A Case-control Study. Indian Dermatol. Online J. 2019, 10, 267–271. [Google Scholar]
- Brazzelli, V.; Barbagallo, T.; Prestinari, F.; Rona, C.; De Silvestri, A.; Trevisan, V. Non-invasive evaluation of tacalcitol plus puva versus tacalcitol plus UVB-NB in the treatment of psoriasis: “Right-left intra-individual pre/post comparison design”. Int. J. Immunopathol. Pharmacol. 2005, 18, 755–760. [Google Scholar] [CrossRef] [Green Version]
- Darlenski, R.; Hristakieva, E.; Aydin, U.; Gancheva, D.; Gancheva, T.; Zheleva, A. Epidermal barrier and oxidative stress parameters improve during in 311nm narrow band UVB phototherapy of plaque type psoriasis. J. Dermatol. Sci. 2018, 91, 28–34. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Soler-Gongora, M.; Martinez-Lopez, A.; Ana, F.G.; Buendia-Eisman, A.; Molina-Leyva, A. Epidermal barrier changes in patients with psoriasis: The role of phototherapy. Photodermatol. Photoimmunol. Photomed. 2021, 37, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Rey, S.; Gómez, E.; Muñoz-Cimadevilla, H.; Hevia, D. Fast and Accurate Electrochemical Measurement of Total Antioxidant Capacity as an Alternative to Spectrophotometrical Methods. Biomed. J. Sci. Tech. Res. 2018, 11, 8376. [Google Scholar]
- Montero-Vilchez, T.; Segura-Fernandez-Nogueras, M.V.; Perez-Rodriguez, I.; Soler-Gongora, M.; Martinez-Lopez, A.; Fernandez-Gonzalez, A. Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity. J. Clin. Med. 2021, 10, 359. [Google Scholar] [CrossRef]
- Cannavo, S.P.; Guarneri, F.; Giuffrida, R.; Aragona, E.; Guarneri, C. Evaluation of cutaneous surface parameters in psoriatic patients. Skin Res. Technol. 2017, 23, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Je, Y.J.; Lee, S.S.; Li, Z.J.; Choi, D.K.; Kwon, Y.B. Changes in transepidermal water loss and skin hydration according to expression of aquaporin-3 in psoriasis. Ann. Dermatol. 2012, 24, 168–174. [Google Scholar] [CrossRef]
- Gran, F.; Kerstan, A.; Serfling, E.; Goebeler, M.; Muhammad, K. Current Developments in the Immunology of Psoriasis. Yale J. Biol. Med. 2020, 93, 97–110. [Google Scholar]
- Mehta, D.; Lim, H.W. Ultraviolet B Phototherapy for Psoriasis: Review of Practical Guidelines. Am. J. Clin. Dermatol. 2016, 17, 125–133. [Google Scholar] [CrossRef]
- Ozawa, M.; Ferenczi, K.; Kikuchi, T.; Cardinale, I.; Austin, L.M.; Coven, T.R. 312-nanometer ultraviolet B light (narrow-band UVB) induces apoptosis of T cells within psoriatic lesions. J. Exp. Med. 1999, 189, 711–718. [Google Scholar] [CrossRef]
- Van de Kerkhof, P.C.M.; de Gruijl, F.R. Phototherapy in the perspective of the chronicity of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 926–931. [Google Scholar] [CrossRef]
- Chen, H.K.; Waite, G.N.; Miller, P.L.; Hughes, E.F.; Waite, L.R. Monitoring temperature and light exposure of biosamples exposed to ultraviolet and low energy radiation. Biomed. Sci. Instrum. 2007, 43, 312–317. [Google Scholar]
- Kwon, I.H.; Kwon, H.H.; Na, S.J.; Youn, J.I. Could colorimetric method replace the individual minimal erythemal dose (MED) measurements in determining the initial dose of narrow-band UVB treatment for psoriasis patients with skin phototype III-V? J. Eur. Acad. Dermatol. Venereol. 2013, 27, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Kwon, I.H.; Woo, S.M.; Choi, J.W.; Kwon, H.H.; Youn, J.I. Recovery from tanning induced by narrow-band UVB phototherapy in brown-skinned individuals with psoriasis: Twelve-month follow-up. J. Dermatol. Sci. 2010, 57, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Pektas, S.D.; Akoglu, G.; Metin, A.; Neselioglu, S.; Erel, O. Evaluation of systemic oxidant/antioxidant status and paraoxonase 1 enzyme activities in psoriatic patients treated by narrow band ultraviolet B phototherapy. Redox Rep. 2013, 18, 200–204. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthy Skin at Baseline (n = 38) | Uninvolved Psoriatic Skin at Baseline (n = 38) | Psoriatic Plaques at Baseline (n = 38) | p * | p ** | p *** | |
|---|---|---|---|---|---|---|
| TEWL (g·m−2h−1) | 11.41 (6.63) | 11.44 (8.11) | 18.23 (9.46) | 0.792 | <0.001 ** | <0.001 *** |
| SCH (AU) | 40.00 (10.50) | 44.64 (12.49) | 9.71 (9.81) | 0.073 | <0.001 ** | <0.001 *** |
| Temperature (°C) | 30.92 (1.04) | 30.40 (1.34) | 31.25 (1.59) | 0.080 | 0.280 | <0.001 *** |
| Erythema (AU) | 284.52 (55.54) | 291.12 (75.43) | 401.09 (64.51) | 0.574 | <0.001 ** | <0.001 *** |
| pH | 5.98 (0.63) | 5.86 (0.64) | 5.91 (0.47) | 0.321 | 0.301 | 0.728 |
| Sebum (AU) | 27.91 (26.95) | 26.97 (30.50) | 30.14 (30.38) | 0.957 | 0.056 | 0.386 |
| Q1 (uC) | 0.86 (0.2) | 1.15 (0.46) | 0.96 (0.45) | 0.001 * | 0.176 | 0.001 *** |
| Q2 (uC) | 4.30 (1.37) | 5.20 (1.85) | 4.57 (2.16) | 0.028 * | 0.565 | 0.026 *** |
| QT (uC) | 5.16 (1.53) | 6.33 (2.26) | 5.54 (2.53) | 0.015 * | 0.474 | 0.014 *** |
| Uninvolved Psoriatic Skin after One Phototherapy Session (n = 38) | Psoriatic Plaques after One Phototherapy Session (n = 38) | Mean Difference in Uninvolved Skin after vs. before Phototherapy | Mean Difference at Psoriatic Plaques after vs. before Phototherapy | p * | p ** | p *** | |
|---|---|---|---|---|---|---|---|
| TEWL (g·m−2h−1) | 10.78 (8.84) | 17.72 (8.46) | −0.66 (0.87) | −0.52 (0.94) | <0.001 * | 0.45 | 0.568 |
| SCH (AU) | 42.78 (11.26) | 12.16 (10.77) | −1.86 (1.19) | 2.45 (0.72) | <0.001 * | 0.126 | 0.002 *** |
| Temperature (°C) | 30.54 (1.54) | 31.49 (1.42) | 0.14 (0.13) | 0.24 (0.1) | <0.001 * | 0.297 | 0.016 *** |
| Erythema (AU) | 294.11 (78.14) | 432.51 (81.91) | 2.98 (6.19) | 31.42 (8.30) | <0.001 * | 0.633 | 0.001 *** |
| pH | 5.84 (0.54) | 6.04 (0.51) | −0.03 (0.11) | 0.13 (0.18) | 0.081 | 0.815 | 0.1 |
| Sebum (AU) | 30.21 (27.40) | 27.71 (17.19) | 0.97 (3.65) | −3.41 (3.84) | 0.571 | 0.792 | 0.381 |
| Q1 (uC) | 1.09 (0.32) | 0.93 (0.39) | −0.05 (0.07) | −0.03 (0.06) | 0.010 * | 0.42 | 0.66 |
| Q2 (uC) | 5.00 (1.31) | 4.51 (1.57) | −0.18 (0.26) | −0.09 (0.24) | 0.026 * | 0.494 | 0.744 |
| QT (uC) | 6.09 (1.55) | 5.44 (1.91) | −0.21 (0.32) | −0.11 (0.28) | 0.013 * | 0.505 | 0.703 |
| Healthy Skin after Follow-Up (n = 26) | Uninvolved Psoriatic Skin after Phototherapy (n = 26) | Psoriatic Plaques after Phototherapy (n = 26) | Mean Difference in Healthy Skin after Follow-Up | Mean Difference in Uninvolved Skin after vs. before Phototherapy | Mean Difference at Psoriatic Plaques after vs. before Phototherapy | p * | p ** | p *** | |
|---|---|---|---|---|---|---|---|---|---|
| TEWL (g·m−2h−1) | 12.18 (4.5) | 8.48 (6.77) | 11.98 (5.45) | 0.30 (1.11) | −3.50 (1.41) | −5.19 (2.00) | 0.786 | 0.021 ** | 0.016 *** |
| SCH (AU) | 45.73 (10.13) | 40.78 (11.70) | 17.45 (13.41) | 4.18 (1.96) | −6.10 (2.91) | 7.01 (2.63) | 0.53 | 0.046 ** | 0.013 *** |
| Temperature (°C) | 30.93 (1.39) | 31.49 (0.88) | 32.13 (0.75) | −0.01 (0.25) | 1.5 (0.26) | 1.42 (0.28) | 0.537 | <0.00 1 ** | <0.001 *** |
| Erythema (AU) | 274.13 (55.65) | 329.57 (79.44) | 428.15 (61.82) | −13.50 (6.78) | 31.83 (17.06) | 30.82 (17.06) | 0.68 | 0.007 * | 0.083 |
| pH | 6.54 (0.59) | 6.20 (0.28) | 6.26 (0.36) | 0.65 (0.18) | 0.37 (0.16) | 0.37 (0.16) | 0.002 * | 0.039 ** | 0.039 *** |
| Sebum (AU) | 17.27 (11.90) | 35.00 (39.18) | 32.26 (38.78) | −10.38 (4.45) | 12.83 (9.51) | 7.17 (9.80) | 0.028 * | 0.190 | 0.472 |
| Q1 (uC) | 0.72 (0.27) | 0.87 (0.25) | 0.85 (0.30) | −0.17 (0.04) | −0.39 (0.09) | −0.22 (0.11) | <0.001 * | <0.001 ** | 0.059 |
| Q2 (uC) | 3.39 (1.20) | 4.32 (1.37) | 4.07 (1.20) | −1.03 (0.26) | −1.24 (0.43) | −1.01 (0.49) | 0.001 * | 0.009 * | 0.049 * |
| QT (uC) | 4.13 (1.42) | 5.44 (1.57) | 4.90 (1.43) | −1.18 (0.27) | −1.36 (0.49) | −1.23 (0.57) | <0.001 * | 0.011 * | 0.041 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montero-Vilchez, T.; Martinez-Lopez, A.; Sierra-Sanchez, A.; Soler-Gongora, M.; Jimenez-Mejias, E.; Molina-Leyva, A.; Buendia-Eisman, A.; Arias-Santiago, S. Erythema Increase Predicts Psoriasis Improvement after Phototherapy. J. Clin. Med. 2021, 10, 3897. https://doi.org/10.3390/jcm10173897
Montero-Vilchez T, Martinez-Lopez A, Sierra-Sanchez A, Soler-Gongora M, Jimenez-Mejias E, Molina-Leyva A, Buendia-Eisman A, Arias-Santiago S. Erythema Increase Predicts Psoriasis Improvement after Phototherapy. Journal of Clinical Medicine. 2021; 10(17):3897. https://doi.org/10.3390/jcm10173897
Chicago/Turabian StyleMontero-Vilchez, Trinidad, Antonio Martinez-Lopez, Alvaro Sierra-Sanchez, Miguel Soler-Gongora, Eladio Jimenez-Mejias, Alejandro Molina-Leyva, Agustin Buendia-Eisman, and Salvador Arias-Santiago. 2021. "Erythema Increase Predicts Psoriasis Improvement after Phototherapy" Journal of Clinical Medicine 10, no. 17: 3897. https://doi.org/10.3390/jcm10173897