
Clinical and Cytokine Profile in Patients with Early and Late Onset Meniere Disease

 , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Experimental Section
2.1. Patient Assessment and Selection
2.2. Peripheral Blood Mononuclear Cell (PBMC) Isolation and Incubation
2.3. Cytokine Measurement
2.4. Statistic and Data Analysis
3. Results
3.1. Clinical Profile in Early and Late Onset MD
3.2. EOMD Has a Higher Prevalence of Migraine Than LOMD Patients
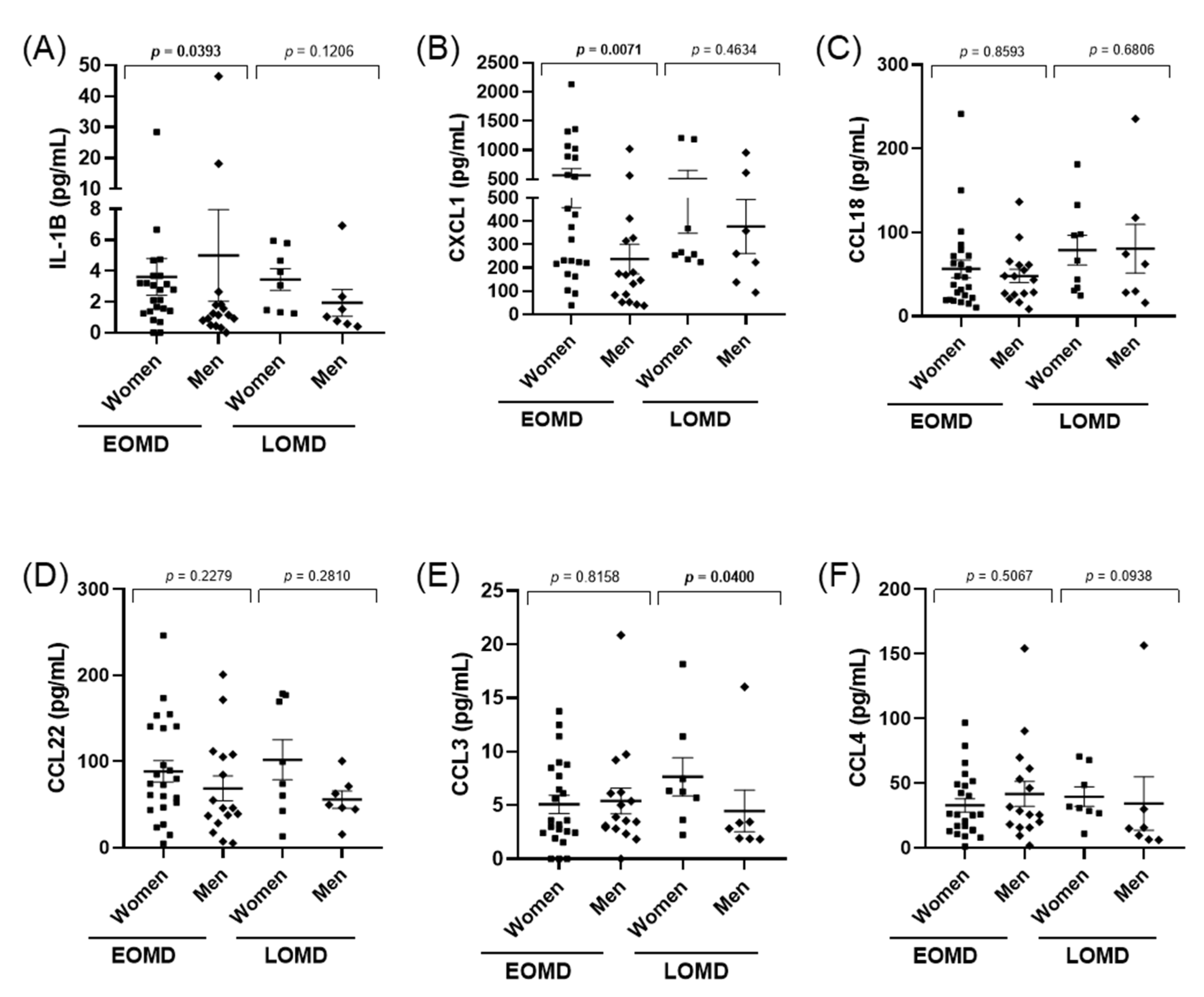
3.3. Cytokine Levels Do Not Allow to Distinguish between EOMD and LOMD Patients
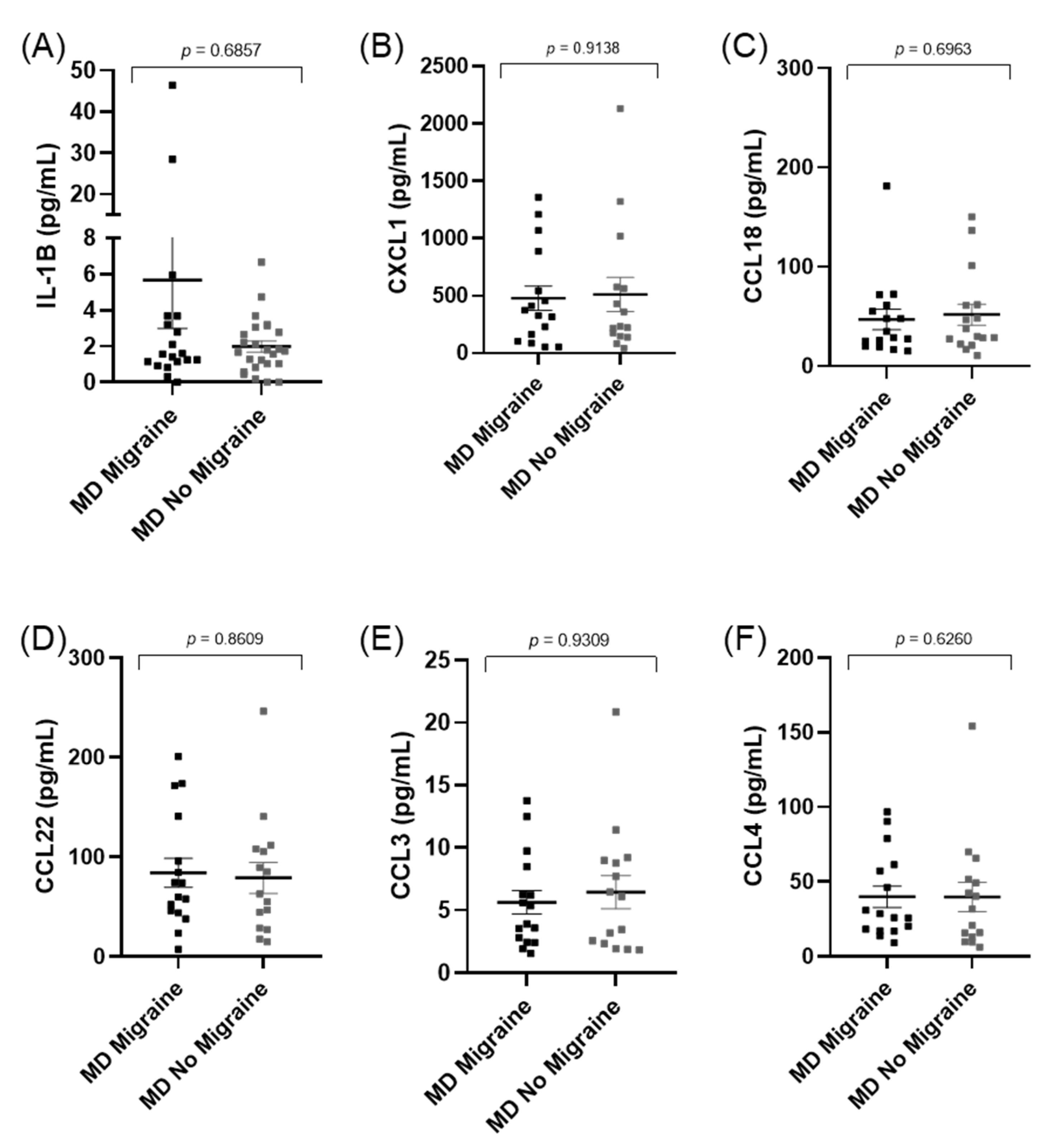
3.4. Cytokines Levels Do Not Differ between Patients with and without Migraine in MD
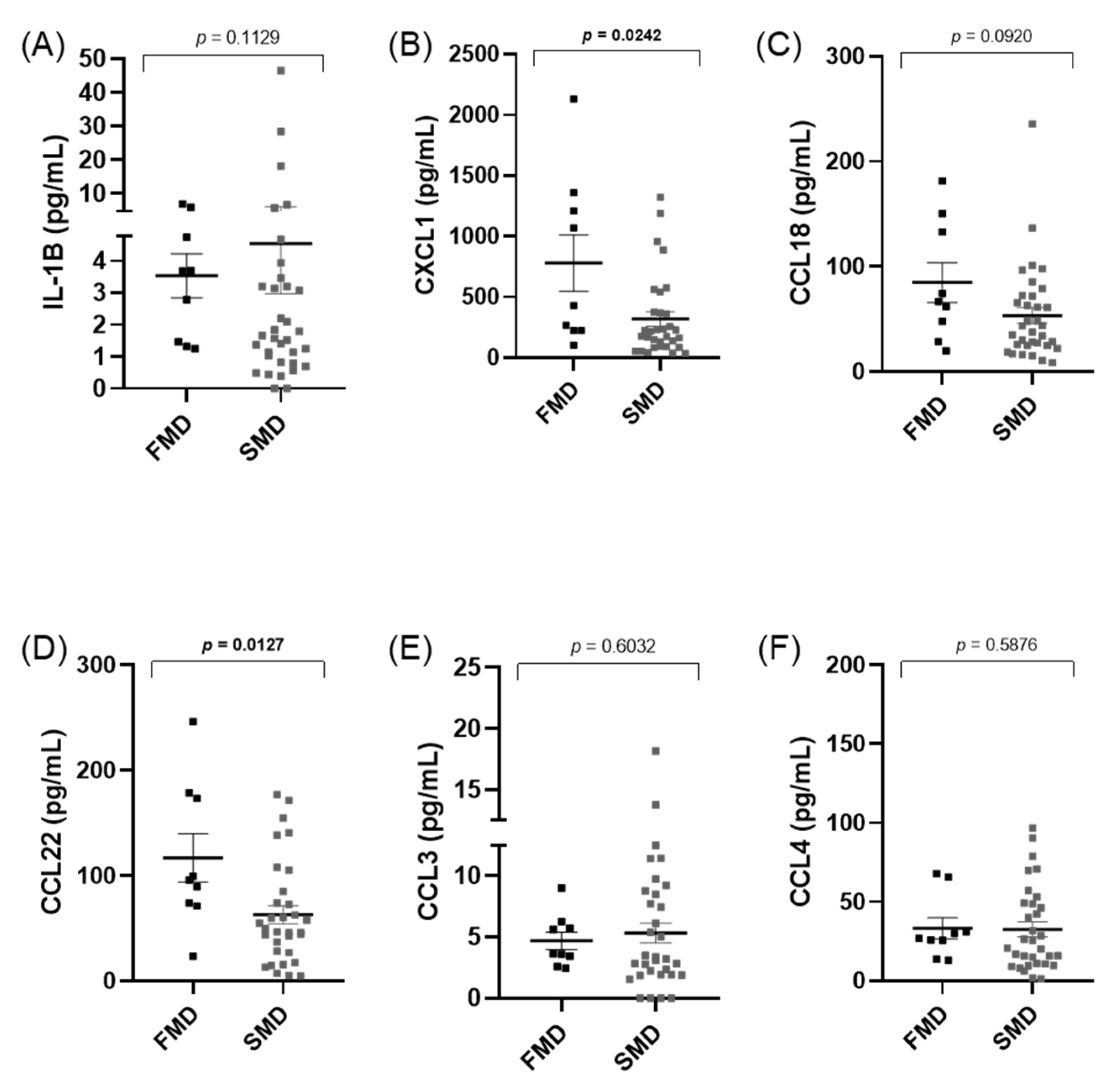
3.5. Cytokines Levels Do Not Differ between Familial (FMD) and Sporadic (SMD) MD Patients
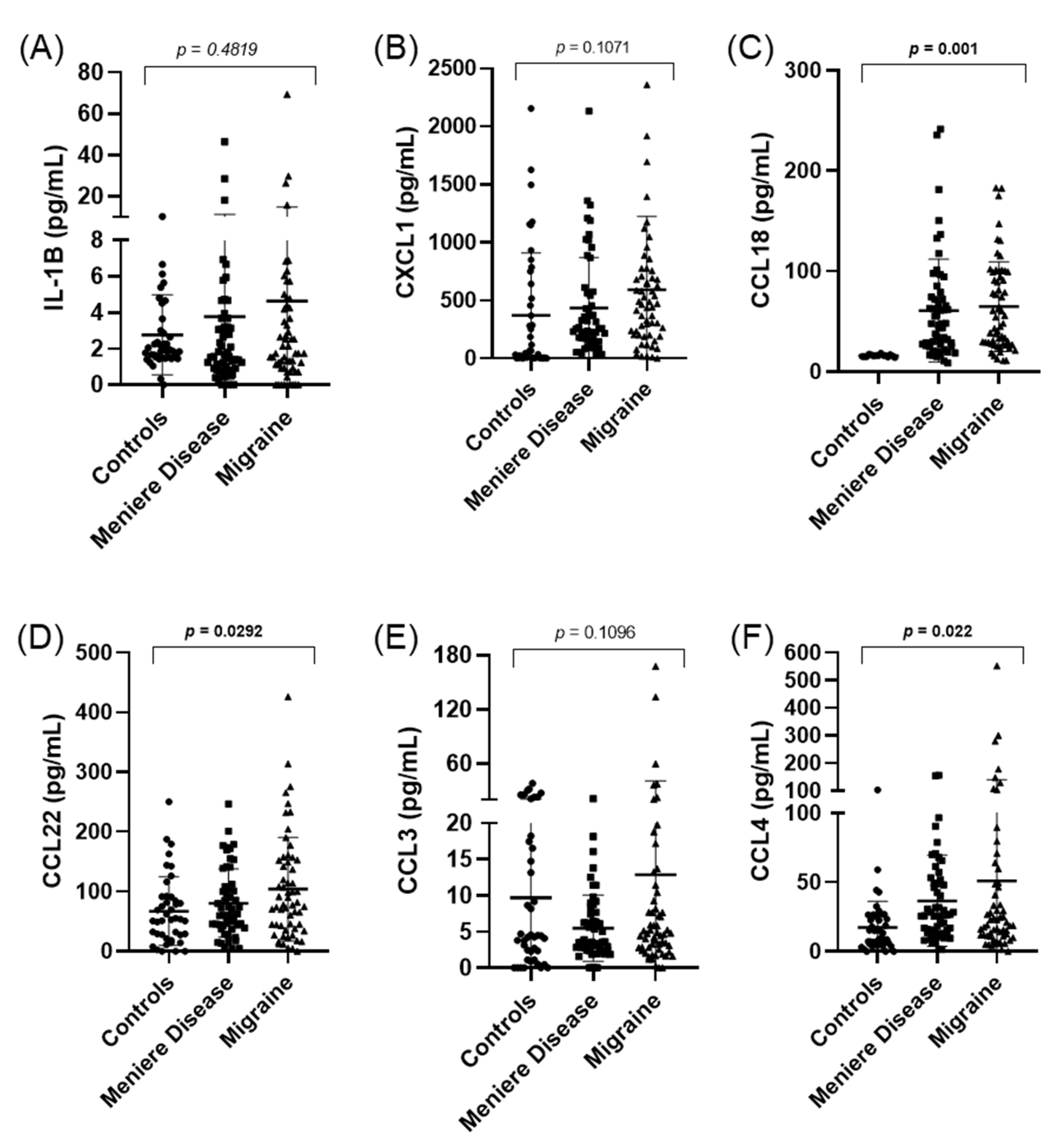
3.6. CCL18, CCL22, and CCL4 Levels Are Different between Patients with MD, Migraine, and Controls
4. Discussion
5. Limitations of the Study
6. Conclusions
- Patients with EOMD have a higher prevalence of migraine than patients with LOMD.
- The levels of IL-1β or chemokines were not dependent on the age of the individuals or the presence of migraine in patients with MD.
- The levels of CCL18, CCL22, and CCL4 were different between patients with MD or migraine and controls.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teggi, R.; Colombo, B.; Albera, R.; Libonati, G.A.; Balzanelli, C.; Caletrio, A.B.; Casani, A.; Espinoza-Sanchez, J.M.; Gamba, P.; Lopez-Escamez, J.A.; et al. Clinical Features, Familial History, and Migraine Precursors in Patients with Definite Vestibular Migraine: The VM-Phenotypes Projects. Headache J. Head Face Pain 2018, 58, 534–544. [Google Scholar] [CrossRef]
- Seemungal, B.; Kaski, D.; Lopez-Escamez, J.A. Early Diagnosis and Management of Acute Vertigo from Vestibular Migraine and Ménière’s Disease. Neurol. Clin. 2015, 33, 619–628. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.H.; Goebel, J.A.; Magnusson, M.; Mandala, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Menière’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Frejo, L.; Soto-Varela, A.; Santos-Perez, S.; Aran, I.; Caletrio, A.B.; Perez-Guillen, V.; Perez-Garrigues, H.; Fraile, J.; Martin-Sanz, E.; Tapia, M.C.; et al. Clinical Subgroups in Bilateral Meniere Disease. Front. Neurol. 2016, 7, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frejo, L.; Martin-Sanz, E.; Teggi, R.; Trinidad-Ruiz, G.; Soto-Varela, A.; Santos-Perez, S.; Manrique, R.; Perez, N.; Aran, I.; Almeida-Branco, M.S.; et al. Extended phenotype and clinical subgroups in unilateral Meniere disease: A cross-sectional study with cluster analysis. Clin. Otolaryngol. 2017, 42, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Requena, T.; Espinosa-Sanchez, J.M.; Cabrera, S.; Trinidad-Ruiz, G.; Soto-Varela, A.; Santos-Perez, S.; Teggi, R.; Perez, P.; Caletrio, A.B.; Fraile, J.; et al. Familial clustering and genetic heterogeneity in Meniere’s disease. Clin. Genet. 2014, 85, 245–252. [Google Scholar] [CrossRef]
- Lee, J.M.; Kim, M.J.; Jung, J.; Kim, H.J.; Seo, Y.J.; Kim, S.H. Genetic aspects and clinical characteristics of familial meniere’s disease in a South Korean population. Laryngoscope 2015, 125, 2175–2180. [Google Scholar] [CrossRef]
- Roman-Naranjo, P.; Gallego-Martinez, A.; Soto-Varela, A.; Aran, I.; Moleon, M.D.C.; Espinosa-Sanchez, J.M.; Amor-Dorado, J.C.; Batuecas-Caletrio, A.; Vázquez, P.P.; Lopez-Escamez, J.A. Burden of Rare Variants in the OTOG Gene in Familial Meniere’s Disease. Ear Hear. 2020, 41, 1598–1605. [Google Scholar] [CrossRef]
- Frejo, L.; Gallego-Martinez, A.; Requena, T.; Martin-Sanz, E.; Amor-Dorado, J.C.; Soto-Varela, A.; Santos-Perez, S.; Espinosa-Sanchez, J.M.; Batuecas-Caletrio, A.; Aran, I.; et al. Proinflammatory cytokines and response to molds in mononuclear cells of patients with Meniere disease. Sci. Rep. 2018, 8, 5974. [Google Scholar] [CrossRef] [PubMed]
- Flook, M.; Frejo, L.; Gallego-Martinez, A.; Martin-Sanz, E.; Rossi-Izquierdo, M.; Amor-Dorado, J.C.; Soto-Varela, A.; Santos-Perez, S.; Batuecas-Caletrio, A.; Espinosa-Sanchez, J.M.; et al. Differential Proinflammatory Signature in Vestibular Migraine and Meniere Disease. Front. Immunol. 2019, 10, 1229. [Google Scholar] [CrossRef]
- Flook, M.; Escamez, J.A.L. Meniere’s Disease: Genetics and the Immune System. Curr. Otorhinolaryngol. Rep. 2018, 6, 24–31. [Google Scholar] [CrossRef]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) the International Classification of Headache Disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Lempert, T.; Olesen, J.; Furman, J.; Waterston, J.; Seemungal, B.; Carey, J.; Bisdorff, A.; Versino, M.; Evers, S.; Newman-Toker, D. Vestibular migraine: Diagnostic criteria. J. Vestib. Res. 2012, 22, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Moore, D.S.; McCabe, G.P. Introduction to the Practice of Statistics, 5th ed.; W.H. Freeman & Company: New York, NY, USA, 2005. [Google Scholar]
- Strupp, M.; Thurtell, M.; Shaikh, A.G.; Brandt, T.; Zee, D.S.; Leigh, R.J. Pharmacotherapy of vestibular and ocular motor disorders, including nystagmus. J. Neurol. 2011, 258, 1207–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinosa-Sanchez, J.M.; Lopez-Escamez, J. Menière’s disease. In The Human Hypothalamus—Neuroendocrine Disorders; Elsevier BV: Amsterdam, The Netherlands, 2016; Volume 137, pp. 257–277. [Google Scholar]
- Greco, A.; Gallo, A.; Fusconi, M.; Marinelli, C.; Macri, G.; de Vincentiis, M. Meniere’s disease might be an autoimmune condition? Autoimmun. Rev. 2012, 11, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Bächinger, D.; Luu, N.-N.; Kempfle, J.S.; Barber, S.; Zürrer, D.; Lee, D.J.; Curtin, H.D.; Rauch, S.D.; Nadol, J.B.; Adams, J.C.; et al. Vestibular Aqueduct Morphology Correlates with Endolymphatic Sac Pathologies in Menière’s Disease—A Correlative Histology and Computed Tomography Study. Otol. Neurotol. 2019, 40, e548–e555. [Google Scholar] [CrossRef]
- Gallego-Martinez, A.; Requena, T.; Roman-Naranjo, P.; May, P.; A Lopez-Escamez, J. Enrichment of damaging missense variants in genes related with axonal guidance signalling in sporadic Meniere’s disease. J. Med. Genet. 2019, 57, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Martinez, A.; Requena, T.; Roman-Naranjo, P.; Lopez-Escamez, J.A. Excess of Rare Missense Variants in Hearing Loss Genes in Sporadic Meniere Disease. Front. Genet. 2019, 10, 76. [Google Scholar] [CrossRef]
- Jin, L.; Batra, S.; Douda, D.N.; Palaniyar, N.; Jeyaseelan, S. CXCL1 Contributes to Host Defense in Polymicrobial Sepsis via Modulating T Cell and Neutrophil Functions. J. Immunol. 2014, 193, 3549–3558. [Google Scholar] [CrossRef]
- Sawant, K.V.; Poluri, K.M.; Dutta, A.K.; Sepuru, K.M.; Troshkina, A.; Garofalo, R.P.; Rajarathnam, K. Chemokine CXCL1 mediated neutrophil recruitment: Role of glycosaminoglycan interactions. Sci. Rep. 2016, 6, 33123. [Google Scholar] [CrossRef] [Green Version]
- Atri, C.; Guerfali, F.Z.; Laouini, D. Role of Human Macrophage Polarization in Inflammation during Infectious Diseases. Int. J. Mol. Sci. 2018, 19, 1801. [Google Scholar] [CrossRef] [Green Version]
- Scheu, S.; Ali, S.; Ruland, C.; Arolt, V.; Alferink, J. The C-C Chemokines CCL17 and CCL22 and Their Receptor CCR4 in CNS Autoimmunity. Int. J. Mol. Sci. 2017, 18, 2306. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, U.; Kuroda, E. Regulation of Macrophage-Derived Chemokine (MDC/ CCL22) Production. Crit. Rev. Immunol. 2002, 22, 105–114. [Google Scholar] [CrossRef]
- Tonndorf, J. Endolymphatic hydrops: Mechanical causes of hearing loss. Eur. Arch. Oto-Rhino-Laryngol. 1976, 212, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Vambutas, A.; Pathak, S. AAO: Autoimmune and Autoinflammatory (Disease) in Otology: What is New in Immune-Mediated Hearing Loss. Laryngoscope 2016, 1, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Empl, M.; Sostak, P.; Riedel, M.; Schwarz, M.; Müller, N.; Förderreuther, S.; Straube, A. Decreased Stnf-Ri in Migraine Patients? Cephalalgia 2003, 23, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Gurol, G.; Ciftci, I.H.; Harman, H.; Karakece, E.; Kamanli, A.; Tekeoglu, I. Roles of claudin-5 and von Willebrand factor in patients with rheumatoid arthritis. Int. J. Clin. Exp. Pathol. 2015, 8, 1979–1984. [Google Scholar]
- Yücel, M.; Kotan, D.; Gurol Çiftçi, G.; Çiftçi, I.H.; Cikriklar, H.I. Serum levels of endocan, claudin-5 and cytokines in mi-graine. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 930–936. [Google Scholar]
- Conti, P.; D’Ovidio, C.; Conti, C.; Gallenga, C.E.; Lauritano, D.; Caraffa, A.; Kritas, S.K.; Ronconi, G. Progression in migraine: Role of mast cells and pro-inflammatory and anti-inflammatory cytokines. Eur. J. Pharmacol. 2019, 844, 87–94. [Google Scholar] [CrossRef]
- Fidan, I.; Yüksel, S.; Ýmir, T.; Irkeç, C.; Aksakal, F.N. The importance of cytokines, chemokines and nitric oxide in pathophysiology of migraine. J. Neuroimmunol. 2006, 171, 184–188. [Google Scholar] [CrossRef]
- Oliveira, A.B.; Bachi, A.; Ribeiro, R.T.; de Mello, M.T.; Tufik, S.; Peres, M.F.P. Unbalanced plasma TNF-α and IL-12/IL-10 profile in women with migraine is associated with psychological and physiological outcomes. J. Neuroimmunol. 2017, 313, 138–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallego-Martinez, A.; Lopez-Escamez, J.A. Genetic architecture of Meniere’s disease. Hear. Res. 2020, 397, 107872. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unilateral Ménière’s Disease (UMD) |
|---|
| Type 1: Sporadic and classical MD. |
| Type 2: Delayed MD (hearing loss precedes vertigo attacks in months or years). |
| Type 3: Familial MD (at least two individuals with MD related in the first or second degree). |
| Type 4: Sporadic MD with migraine (temporal relationship not required). |
| Type 5: Sporadic MD plus an autoimmune disease. |
| Bilateral Ménière’s Disease (BMD) |
| Type 1: Unilateral hearing loss becomes bilateral. |
| Type 2: Sporadic, simultaneous hearing loss (usually symmetric). |
| Type 3: Familial MD (most families have bilateral hearing loss, but unilateral and bilateral cases may coexist in the same family). |
| Type 4: Sporadic MD with migraine. |
| Type 5: Sporadic MD with an autoimmune disease. |
| Patient | Gender | Ear | Age of Onset | Duration of Disease (y) | FMD | Migraine | MD Subgroup | IL-1β Level |
|---|---|---|---|---|---|---|---|---|
| 1 | Woman | Bilateral | 34 | 8 | Yes | Yes | 3 | 3.68 |
| 2 | Woman | Bilateral | 33 | 8 | Yes | Yes | 3 | 1.24 |
| 3 | Woman | Unilateral | 28 | 12 | No | Yes | 4 | 0.82 |
| 4 | Man | Unilateral | 29 | 9 | No | No | 1 | 1.57 |
| 5 | Woman | Bilateral | 33 | 24 | No | Yes | 4 | 3.20 |
| 6 | Woman | Bilateral | 18 | 34 | Yes | No | 3 | 4.74 |
| 7 | Woman | Unilateral | 28 | 27 | No | X | 4 | 1.41 |
| 8 | Woman | Unilateral | 20 | 1 | Yes | Yes | 3 | 18.64 |
| 9 | Woman | Unilateral | 28 | 8 | No | No | 2 | 3.69 |
| 10 | Woman | Unilateral | 29 | 20 | Yes | Yes | 3 | 2.79 |
| 11 | Man | Bilateral | 27 | 16 | No | No | 2 | 2.64 |
| 12 | Woman | Bilateral | 33 | 8 | No | Yes | 4 | 2.10 |
| 13 | Woman | Bilateral | 24 | 15 | No | Yes | 4 | 28.45 |
| 14 | Woman | Bilateral | 33 | 17 | No | No | 5 | 1.66 |
| 15 | Woman | Bilateral | 23 | 18 | No | Yes | 4 | 1.59 |
| 16 | Man | Bilateral | 31 | 15 | No | Yes | 1 | 1.25 |
| 17 | Man | Unilateral | 34 | 8 | No | No | 1 | 0.49 |
| 18 | Woman | Unilateral | 27 | 17 | No | No | 1 | 2.11 |
| 19 | Man | Bilateral | 35 | 16 | No | No | 1 | 0.92 |
| 20 | Woman | Bilateral | 34 | 20 | No | No | 1 | 3.68 |
| 21 | Woman | Unilateral | 35 | 20 | Yes | No | 3 | 0.01 |
| 22 | Man | Bilateral | 29 | 15 | No | No | 2 | 0.18 |
| 23 | Man | Unilateral | 29 | 11 | No | No | 1 | 0 |
| 24 | Man | Unilateral | 24 | 1 | No | No | 1 | 1.84 |
| 25 | Man | Unilateral | 30 | 27 | No | Yes | 1 | 46.41 |
| 26 | Man | Bilateral | 27 | 22 | No | No | 1 | 0 |
| 27 | Man | Unilateral | 32 | 3 | No | No | 1 | 2.77 |
| 28 | Man | Bilateral | 22 | 23 | Yes | Yes | 1 | 0.44 |
| 29 | Woman | Bilateral | 31 | 5 | No | Yes | 1 | 1.14 |
| 30 | Man | Bilateral | 22 | 22 | No | No | 1 | 1.57 |
| 31 | Man | Bilateral | 25 | 25 | No | No | 1 | 0.31 |
| 32 | Man | Bilateral | 34 | 34 | No | No | 1 | 1.14 |
| 33 | Man | Bilateral | 28 | 18 | No | No | 1 | 18.18 |
| 34 | Woman | Unilateral | 28 | 25 | No | No | 5 | 2.19 |
| 35 | Woman | Unilateral | 23 | 50 | No | No | 1 | 3.14 |
| 36 | Woman | Unilateral | 29 | 30 | No | No | 5 | 6.66 |
| 37 | Woman | Unilateral | 23 | 50 | No | No | 1 | 3.07 |
| 38 | Man | Unilateral | 27 | 5 | No | No | 1 | 1.79 |
| 39 | Woman | Unilateral | 18 | 18 | Yes | Yes | 3 | 4.68 |
| 40 | Woman | Unilateral | 35 | 20 | No | No | 1 | 0 |
| 41 | Woman | Unilateral | 21 | 2 | Yes | No | 3 | 0 |
| 42 | Man | Unilateral | 24 | 28 | Yes | No | 3 | 0.80 |
| 43 | Woman | Unilateral | 18 | 9 | Yes | Yes | 2 | 0.69 |
| 44 | Woman | Unilateral | 24 | 28 | No | Yes | 4 | 1.37 |
| Patient | Gender | Ear | Age of Onset | Duration of Disease (y) | FMD | Migraine | MD Subgroup | IL-1β Level |
|---|---|---|---|---|---|---|---|---|
| 1 | Man | Bilateral | 55 | 20 | No | No | 2 | 0.83 |
| 2 | Woman | Unilateral | 65 | 8 | Yes | No | 3 | 1.23 |
| 3 | Man | Unilateral | 50 | 13 | No | No | 1 | 1.56 |
| 4 | Man | Bilateral | 55 | 30 | No | No | 2 | 2.24 |
| 5 | Man | Unilateral | 61 | 16 | No | No | 1 | 2.64 |
| 6 | Woman | Unilateral | 50 | 23 | Yes | No | 3 | 2.10 |
| 7 | Man | Bilateral | 53 | 16 | No | No | 2 | 3.14 |
| 8 | Woman | Unilateral | 50 | 8 | No | No | 1 | 2.67 |
| 9 | Man | Bilateral | 53 | 30 | No | No | 2 | 4.34 |
| 10 | Man | Unilateral | 50 | 14 | Yes | No | 3 | 6.93 |
| 11 | Man | Unilateral | 62 | 1 | No | Yes | 4 | 0.01 |
| 12 | Woman | Unilateral | 52 | 17 | No | Yes | 4 | 0.57 |
| 13 | Woman | Bilateral | 56 | 24 | No | No | 2 | 2.27 |
| 14 | Woman | Unilateral | 55 | 10 | No | No | 1 | 2.06 |
| 15 | Woman | Unilateral | 63 | 13 | Yes | Yes | 3 | 1.07 |
| 16 | Man | Bilateral | 56 | 5 | No | No | 2 | 0.58 |
| 17 | Man | Unilateral | 53 | 2 | Yes | Yes | 3 | 0.01 |
| 18 | Man | Bilateral | 54 | 3 | No | No | 2 | 1.03 |
| 19 | Woman | Bilateral | 53 | 4 | No | Yes | 4 | 2.67 |
| 20 | Man | Bilateral | 55 | 17 | Yes | No | 3 | 1.27 |
| 21 | Woman | Unilateral | 50 | 20 | Yes | No | 3 | 1.73 |
| 22 | Woman | Bilateral | 55 | 9 | Yes | Yes | 3 | 5.95 |
| 23 | Woman | Unilateral | 50 | 8 | No | No | 1 | 3.07 |
| 24 | Woman | Bilateral | 52 | 6 | No | No | 2 | 1.03 |
| 25 | Man | Bilateral | 53 | 2 | Yes | Yes | 3 | 3.68 |
| 26 | Woman | Unilateral | 56 | 2 | No | No | 1 | 0.83 |
| 27 | Man | Unilateral | 57 | 2 | No | No | 1 | 1.66 |
| 28 | Man | Bilateral | 53 | 7 | No | No | 2 | 0.39 |
| 29 | Woman | Unilateral | 65 | 1 | No | Yes | 4 | 4.96 |
| 30 | Man | Unilateral | 69 | 2 | No | No | 1 | 0.76 |
| 31 | Man | Unilateral | 66 | 5 | No | No | 1 | 2.33 |
| 32 | Woman | Unilateral | 51 | 5 | No | No | 1 | 4.67 |
| 33 | Woman | Unilateral | 63 | 6 | No | No | 1 | 3.94 |
| 34 | Woman | Unilateral | 61 | 6 | No | No | 1 | 1.25 |
| 35 | Man | Unilateral | 51 | 7 | No | No | 1 | 1.52 |
| 36 | Woman | Unilateral | 50 | 8 | No | No | 1 | 5.79 |
| 37 | Woman | Unilateral | 54 | 1 | Yes | No | 3 | 1.32 |
| 38 | Woman | Unilateral | 57 | 6 | Yes | No | 3 | 1.47 |
| 39 | Woman | Unilateral | 54 | 7 | No | Yes | 1 | 3.47 |
| Variable | EOMD (n = 44) | LOMD (n = 39) | p-Value |
|---|---|---|---|
| Duration of the disease (mean ± SD) | 18.0 ± 11.4 | 9.8 ± 7.9 | 0.0004 |
| Age of onset (mean ± SD) | 27.7 ± 4.9 | 55.6± 5.2 | <0.0001 |
| Sex (% female) | 59.0 | 53.8 | 0.195 |
| Bilateral hearing loss (%) | 45.5 | 33.3 | 0.545 |
| Hearing loss (% synchronic) | 29.5 | 12.8 | 0.338 |
| MD type | 0.589 | ||
| 1 | 21 | 15 | |
| 2 | 4 | 9 | |
| 3 | 9 | 4 | |
| 4 | 7 | 3 | |
| 5 | 3 | 0 | |
| Hearing loss (%) | 0.357 | ||
| High frequency | 61.4 | 69.2 | |
| Low frequency | 38.6 | 30.8 | |
| Family History of hearing loss (%) | 25.0 | 28.2 | 0.999 |
| Any Headache (%) | 59.0 | 56.4 | 0.440 |
| Migraine (%) | 38.6 | 23.0 | 0.045 |
| Arterial Hypertension (%) | 22.7 | 25.6 | 0.948 |
| Smoking (%) | 13.6 | 10.3 | 0.532 |
| Dyslipidemia (%) | 18.2 | 28.2 | 0.400 |
| Diabetes Mellitus (%) | 25.0 | 25.6 | 0.854 |
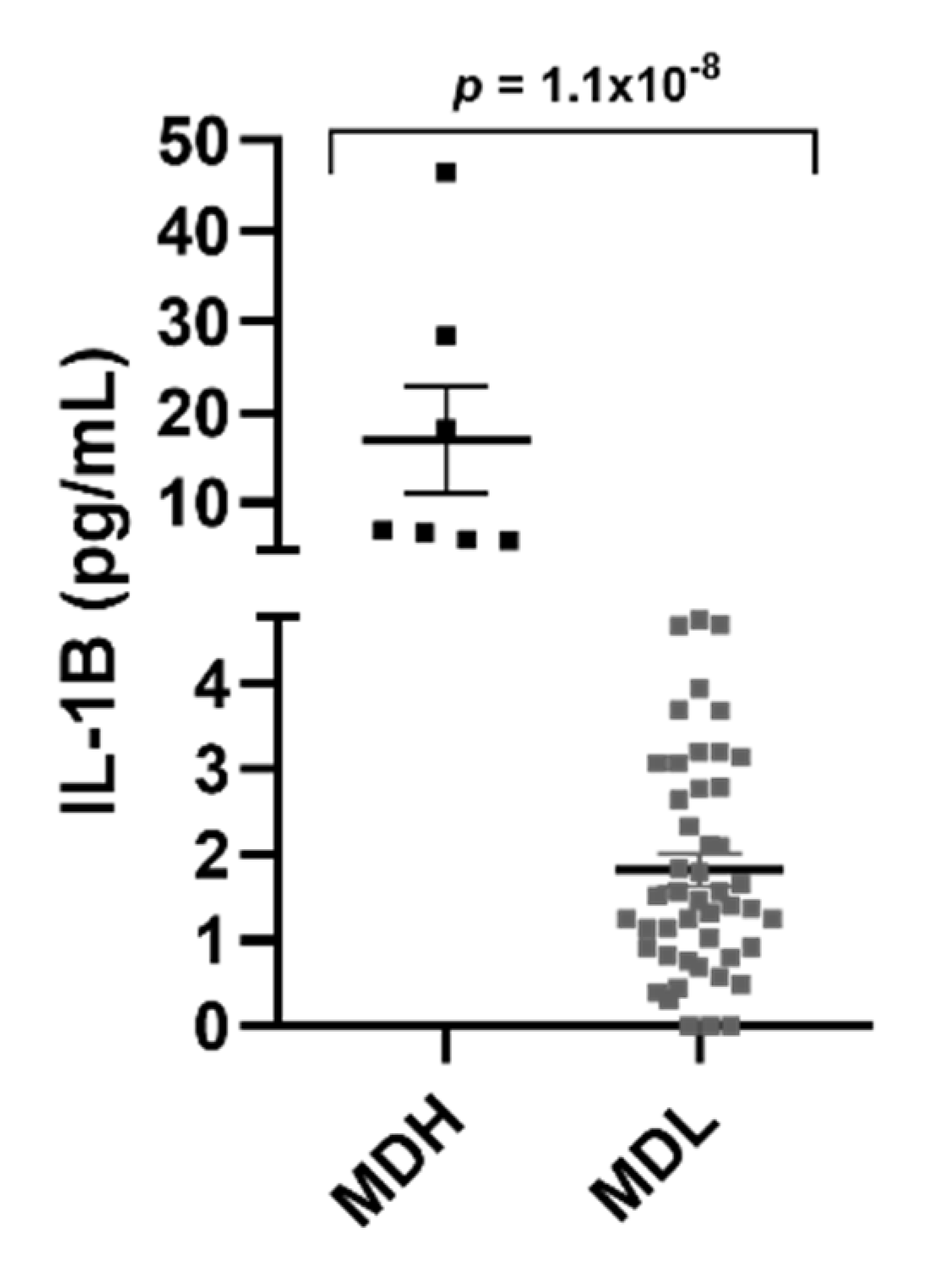
| Variable | MDH (n = 9) | MDL (n = 74) | p-Value |
|---|---|---|---|
| MD type (%) | 0.9924 | ||
| 1 | 3 (33.3) | 33 (44) | |
| 2 | 0 (0) | 13 (14.6) | |
| 3 | 3 (33.3) | 17 (22.9) | |
| 4 | 2 (22.2) | 9 (12.1) | |
| 5 | 1 (11.1) | 2 (2.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moleon, M.-D.-C.; Martinez-Gomez, E.; Flook, M.; Peralta-Leal, A.; Gallego, J.A.; Sanchez-Gomez, H.; Montilla-Ibañez, M.A.; Dominguez-Durán, E.; Soto-Varela, A.; Aran, I.; et al. Clinical and Cytokine Profile in Patients with Early and Late Onset Meniere Disease. J. Clin. Med. 2021, 10, 4052. https://doi.org/10.3390/jcm10184052
Moleon M-D-C, Martinez-Gomez E, Flook M, Peralta-Leal A, Gallego JA, Sanchez-Gomez H, Montilla-Ibañez MA, Dominguez-Durán E, Soto-Varela A, Aran I, et al. Clinical and Cytokine Profile in Patients with Early and Late Onset Meniere Disease. Journal of Clinical Medicine. 2021; 10(18):4052. https://doi.org/10.3390/jcm10184052
Chicago/Turabian StyleMoleon, Maria-Del-Carmen, Estrella Martinez-Gomez, Marisa Flook, Andreina Peralta-Leal, Juan Antonio Gallego, Hortensia Sanchez-Gomez, Maria Alharilla Montilla-Ibañez, Emilio Dominguez-Durán, Andres Soto-Varela, Ismael Aran, and et al. 2021. "Clinical and Cytokine Profile in Patients with Early and Late Onset Meniere Disease" Journal of Clinical Medicine 10, no. 18: 4052. https://doi.org/10.3390/jcm10184052