
Heterozygous Arrhythmogenic Cardiomyopathy-desmoplakin Mutation Carriers Exhibit a Subclinical Cutaneous Phenotype with Cell Membrane Disruption and Lack of Intercellular Adhesion

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Dermatological Evaluation and Skin Barrier Function Assessment
2.3. Samples Processing
2.4. Immunohistochemistry
2.5. Transmission Electron Microscopy
2.6. Statistical Analysis
3. Results
3.1. Dermatological Evaluation and Skin Barrier Function Assessment
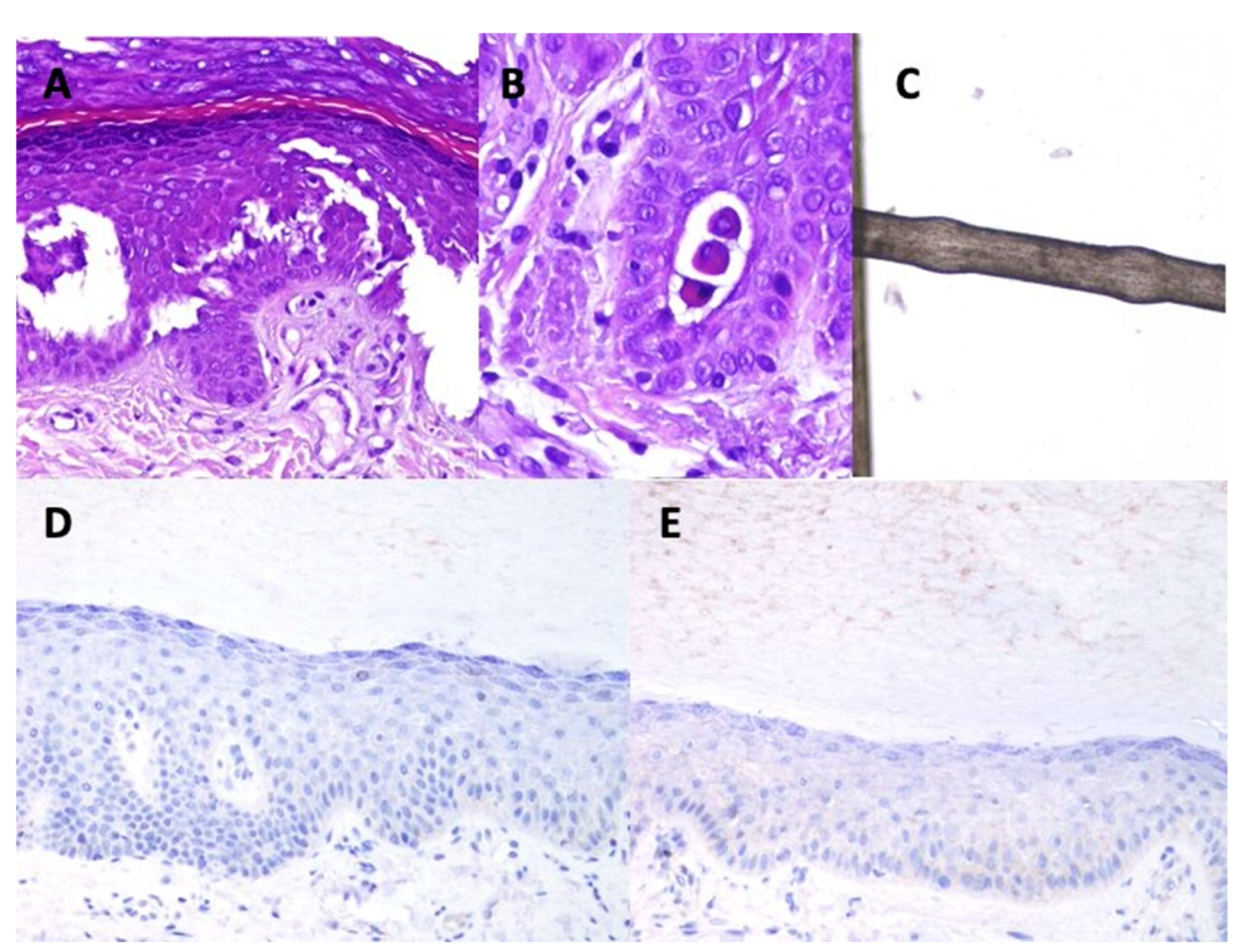
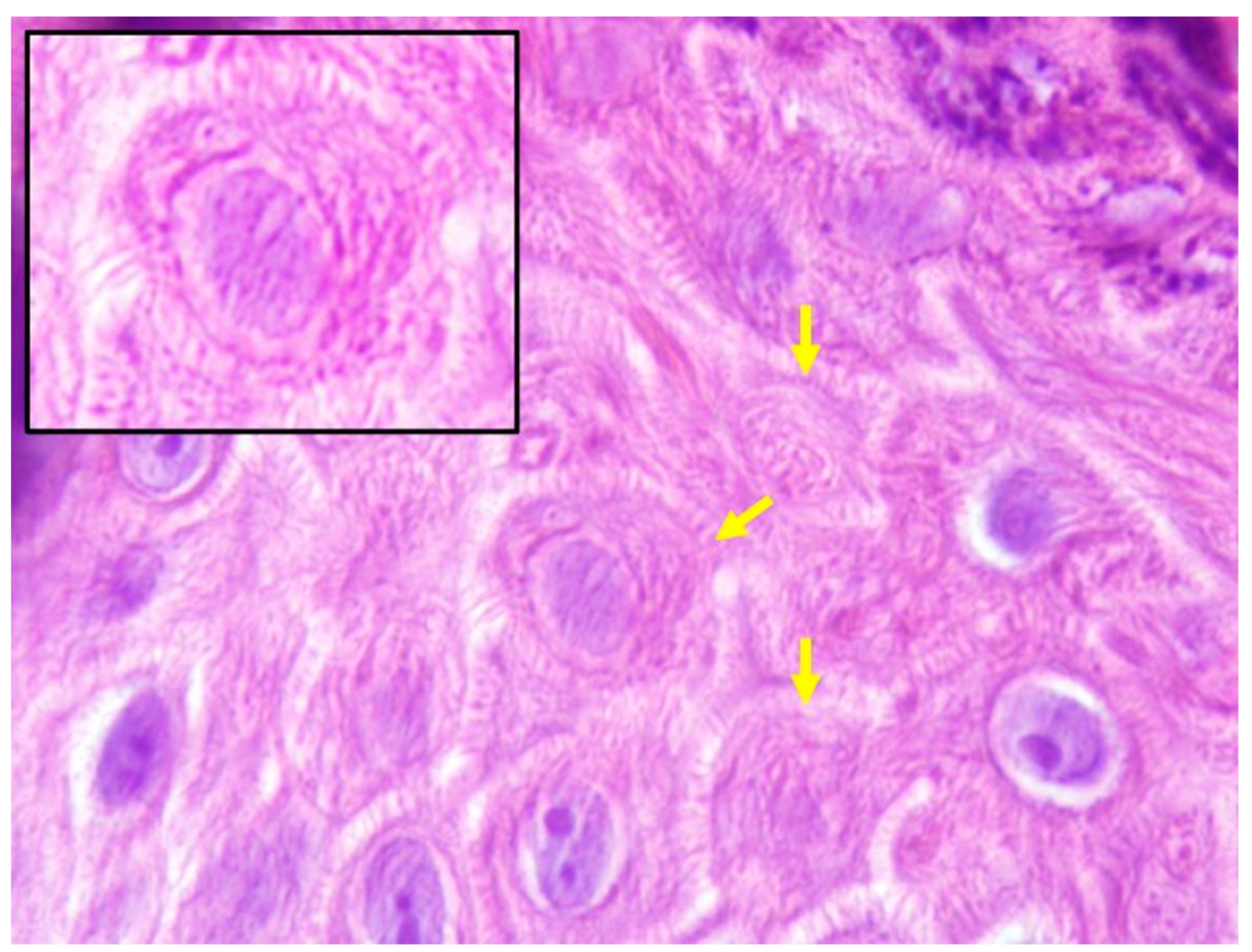
3.2. Histopathology
3.3. Trichogram
3.4. Immunohistochemistry
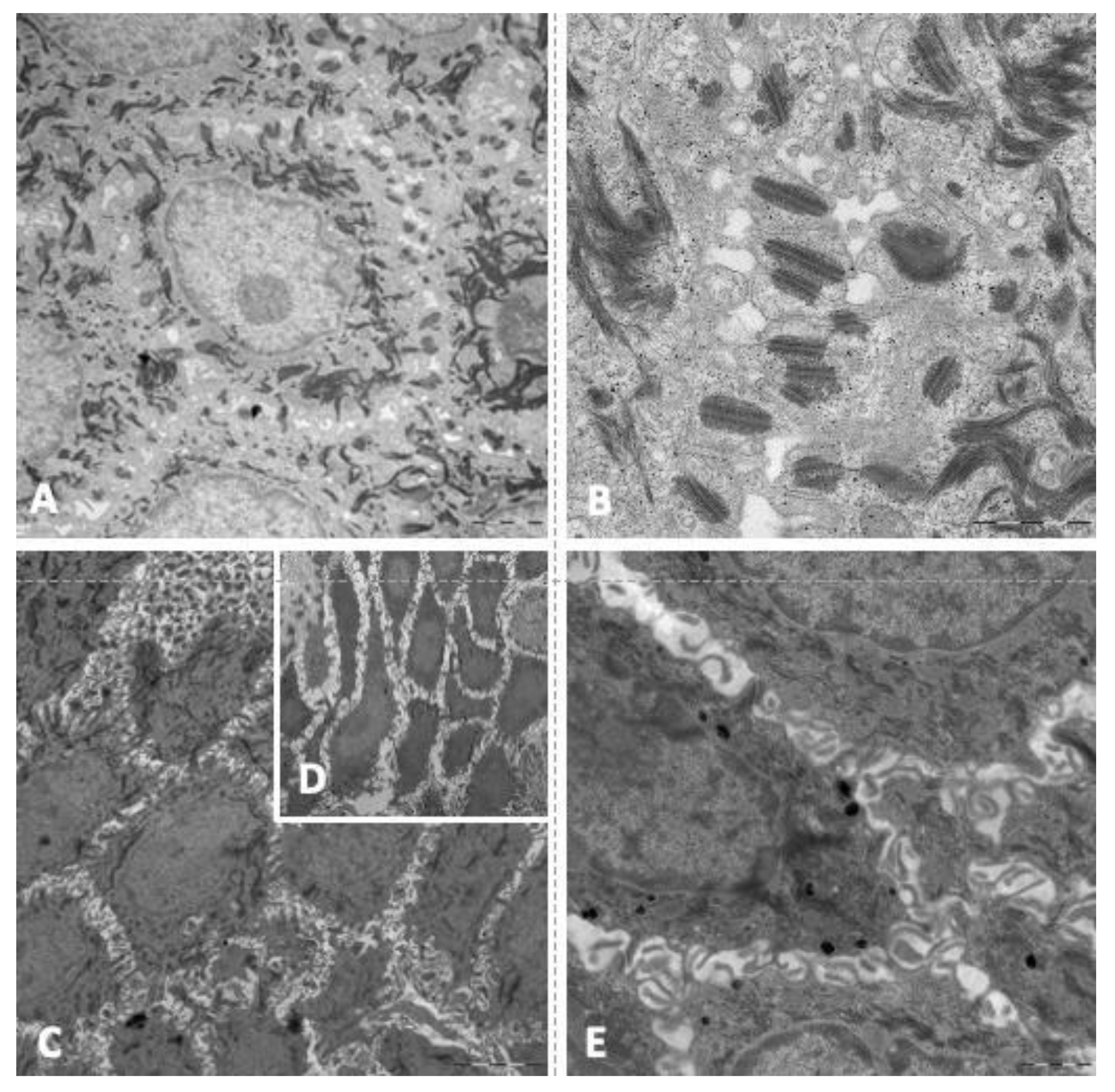
3.5. Transmission Electron Microscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Dilution | Incubation Time (minutes) | Antigen Retrieval pH | Visualization System | Manufacturer | Isotype | Type | Identification Number | Clone |
|---|---|---|---|---|---|---|---|---|---|
| Plakoglobin | 1/1000 | 30 | Low | Flex | BioNova | IgG1 | Monoclonal | A303-717A | 3728 |
| Desmoplakin | 1/25 | 30 | Low | Flex | PROGEN | IgG1 | Monoclonal | 61003 | DP1 + 2-2.15 |
| Conexin 43 | 1/400 | 30 | Low | Flex | Sigma Aldrich | IgG1 | Monoclonal | 045M4882V | C6219 |
| Filamin C | 1/50 | 45 | Low | Flex + Mouse | LSBio | IgG1 | Monoclonal | LS-B6314/47000 | N-terminus |
Appendix B

| Patient | Anagen/Telogen (%) | Dystrophic Hairs | Keratotis Material at the Proximal Areas of the Hair Shaft | Hair Dysplasia | Uniform Diameters of the Shafts | Cuticular Defects | Other Findings |
|---|---|---|---|---|---|---|---|
| 1 * | a | a | a | a | a | a | a |
| 2 | 0/100 | Pseudomonilethrix | No | No | No | Yes | None |
| 3 | 100/0 | Pseudomonilethrix | Yes | No | No | No | White hairs |
| 4 | 100/0 | Pseudomonilethrix. Fractures in trichoschisis. Periodic stem crunches. | Yes | No | Yes | No | White hairs |
| 5 | 40/60 | Pseudomonilethrix | Yes | No | No | No | None |
| 6 | 90/10 | No | No | No | No | No | None |
| 7 | 0/100 | Pseudomonilethrix | Yes | No | No | No | None |
| 8 | 80/20 | No | No | No | No | No | White hairs |
| 9 | 20/80 (small sample) | No | No | No | No | No | None |
| 10 | 95/5 | No | No | No | No | No | None |
| 11 | 0/100 | Pseudomonilethrix | No | No | No | No | White hairs |
| 12 | 98/2 | Pseudomonilethrix | Yes | No | No | No | None |
References
- Towbin, J.A.; McKenna, W.J.; Abrams, D.J.; Ackerman, M.J.; Calkins, H.; Darrieux, F.C.C.; Daubert, J.P.; de Chillou, C.; DePasquale, E.C.; Desai, M.Y.; et al. 2019 HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy: Executive summary. Heart Rhythm 2019, 16, e373–e407. [Google Scholar] [CrossRef] [Green Version]
- McKoy, G.; Protonotarios, N.; Crosby, A.; Tsatsopoulou, A.; Anastasakis, A.; Coonar, A.; Norman, M.; Baboonian, C.; Jeffery, S.; McKenna, W.J. Identification of a deletion in plakoglobin in arrhythmogenic right ventricular cardiomyopathy with palmoplantar keratoderma and woolly hair (Naxos disease). Lancet 2000, 355, 2119–2124. [Google Scholar] [CrossRef]
- Gandjbakhch, E.; Redheuil, A.; Pousset, F.; Charron, P.; Frank, R. Clinical Diagnosis, Imaging, and Genetics of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 784–804. [Google Scholar] [CrossRef]
- Smith, E.; Lakdawala, N.K.; Papoutsidakis, N.; Aubert, G.; Mazzanti, A.; McCanta, A.; Agarwal, P.P.; Arscott, P.; Dellefave-Castillo, L.M.; Vorovich, E.E.; et al. Desmoplakin Cardiomyopathy, a Fibrotic and Inflammatory Form of Cardiomyopathy Distinct From Typical Dilated or Arrhythmogenic Right Ventricular Cardiomyopathy. Circulation 2020, 141, 1872–1884. [Google Scholar] [CrossRef]
- Mazzanti, A.; Ng, K.; Faragli, A.; Maragna, R.; Chiodaroli, E.; Orphanou, N.; Monteforte, N.; Memmi, M.; Gambelli, P.; Novelli, V.; et al. Arrhythmogenic right ventricular cardiomyopathy: Clinical course and predictors of arrhythmic risk. J. Am. Coll. Cardiol. 2016, 68, 2540–2550. [Google Scholar] [CrossRef]
- Desai, B.V.; Harmon, R.M.; Green, K.J. Desmosomes at a glance. J. Cell Sci. 2009, 122, 4401–4407. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.W.; McGrath, J.A. Mutations in genes encoding desmosomal proteins: Spectrum of cutaneous and extracutaneous abnormalities. Br. J. Dermatol. 2021, 184, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, T.B.; Nissen, P.H.; Palmfeldt, J.; Gehmlich, K.; Dalagen, S.; Jensen, U.B.; Kim, W.Y.; Heickendorff, L.; Mølgaard, H.; Jensen, H.K.; et al. Truncating plakophilin-2 mutations in arrhythmogenic cardiomyopathy are associated with protein haploinsufficiency in both myocardium and epidermis. Circ. Cardiovasc. Genet. 2014, 7, 230–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruthappu, T.; Posafalvi, A.; Castelletti, S.; Delaney, P.J.; Syrris, P.; O’Toole, E.A.; Green, K.J.; Elliott, P.M.; Lambiase, P.D.; Tinker, A.; et al. Loss-of-function desmoplakin I and II mutations underlie dominant arrhythmogenic cardiomyopathy with a hair and skin phenotype. Br. J. Dermatol. 2019, 180, 1114–1122. [Google Scholar] [CrossRef] [Green Version]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.; Basso, C.; Bauce, B.; Bluemke, D.A.; Calkins, H.; Corrado, D.; Cox, M.G.P.J.; Daubert, J.P. Diagnosis of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia Proposed Modification of the Task Force Criteria Special Report. Eur. Heart J. 2010, 31, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Bauce, B.; Basso, C.; Rampazzo, A.; Beffagna, G.; Daliento, L.; Frigo, G.; Malacrida, S.; Settimo, L.; Danieli, G.; Thiene, G.; et al. Clinical profile of four families with arrhythmogenic right ventricular cardiomyopathy caused by dominant desmoplakin mutations. Eur. Heart J. 2005, 26, 1666–1675. [Google Scholar] [CrossRef] [Green Version]
- López-Ayala, J.M.; Gomez-Milanes, I.; Sanchez Munoz, J.J.; Ruiz-Espejo, F.; Ortíz, M.; González-Carrillo, J.; López-Cuenca, D.; Oliva-Sandoval, M.J.; Monserrat, L.; Valdés, M.; et al. Desmoplakin truncations and arrhythmogenic left ventricular cardiomyopathy: Characterizing a phenotype. Europace 2014, 16, 1838–1846. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Manchón, J.; Fernández, E.; Igual, B.; Asimaki, A.; Syrris, P.; Osca, J.; Salvador, A.; Zorio, E. Left Dominant Arrhythmogenic Cardiomyopathy Caused by a Novel Nonsense Mutation in Desmoplakin. Rev. Española Cardiol. 2011, 64, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Norman, M.; Simpson, M.; Mogensen, J.; Shaw, A.; Hughes, S.; Syrris, P.; Sen-Chowdhry, S.; Rowland, E.; Crosby, A.; McKenna, W.J. Novel Mutation in Desmoplakin Causes Arrhythmogenic Left Ventricular Cardiomyopathy. Circulation 2005, 112, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Montero-Vílchez, T.; Segura-Fernández-Nogueras, M.-V.; Pérez-Rodríguez, I.; Soler-Góngora, M.; Martínez-López, A.; Fernández-González, A.; Molina-Leyva, A.; Arias-Santiago, S. Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity. J. Clin. Med. 2021, 10, 359. [Google Scholar] [CrossRef]
- Protonotarios, N.; Tsatsopoulou, A. Naxos disease and Carvajal syndrome: Cardiocutaneous disorders that highlight the pathogenesis and broaden the spectrum of arrhythmogenic right ventricular cardiomyopathy. Cardiovasc. Pathol. 2004, 13, 185–194. [Google Scholar] [CrossRef]
- Winik, B.C.; Asial, R.A.; McGrath, J.A.; South, A.P.; Boente, M.C. Acantholytic ectodermal dysplasia: Clinicopathological study of a new desmosomal disorder. Br. J. Dermatol. 2009, 160, 868–874. [Google Scholar] [CrossRef]
- Ahranjani, B.M.; Moradi, P.; Nazari, S.; Farshadfar, S. A nine-year-old girl with left ventricle non-compaction and skin lesions (Carvajal syndrome). Iran J. Pediatr. 2015, 25, e370. [Google Scholar] [CrossRef] [Green Version]
- Baykan, A.; Olgar, Ş.; Argun, M.; Özyurt, A.; Pamukçu, Ö.; Üzüm, K.; Narin, N. Different clinical presentations of Naxos disease and Carvajal syndrome: Case series from a single tertiary center and review of the literature. Anatol J Cardiol. 2015, 15, 404–408. [Google Scholar] [CrossRef]
- Salam, A.A.; Remadevi, K.S.; Kurup, R.P. Naxos disease and Carvajal variant. Indian Pediatr. 2013, 50, 596–598. [Google Scholar]
- Sun, Q.; Wine Lee, L.; Hall, E.K.; Choate, K.A.; Elder, R.W. Hair and skin predict cardiomyopathies: Carvajal and erythrokeratodermia cardiomyopathy syndromes. Pediatr. Dermatol. 2021, 38, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Chidgey, M.A. Desmosomes and disease: An update. Histol. Histopathol. 2002, 17, 1179–1192. [Google Scholar] [CrossRef]
- Jurčić, V.; Kukovič, J.; Zidar, N. Expression of desmosomal proteins in acantholytic squamous cell carcinoma of the skin. Histol. Histopathol. 2015, 30, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Setoyama, M.; Choi, K.C.; Hashimoto, K.; Ishihara, M.; Predeteanu, G.S.; Dinehart, S.; Predeteanu, C.; Hamzavi, L.H.; Etoh, H. Desmoplakin I and II in acantholytic dermatoses: Preservation in pemphigus vulgaris and pemphigus erythematosus and dissolution in Hailey-Hailey’s disease and Darier’s disease. J. Dermatol. Sci. 1991, 2, 9–17. [Google Scholar] [CrossRef]
- Jonkman, M.F.; Pasmooij, A.M.G.; Pasmans, S.G.M.A.; Van Den Berg, M.; Ter Horst, H.; Timmer, A.; Pas, H.H. Loss of desmoplakin tail causes lethal acantholytic epidermolysis bullosa. Am. J. Hum. Genet. 2005, 77, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Age (Years) | Sex | Genetic Variant | LVEF (%) | Status TFC | Late Gadolinium Enhancement | VPB 24 h-ambulatory ECG | NSVT | Sustained Ventricular Arrhythmias | |
|---|---|---|---|---|---|---|---|---|---|
| Patient 1 | 24 | Female | p.Asp960Glnfs*16 | 55 | Borderline | Subepicardial patching in LV | 102 | No | No |
| Patient 2 | 28 | Male | p.Arg2284* | 50 | Definitive | Subepicardial circumferential in LV and RV free wall | 2916 | No | No |
| Patient 3 | 61 | Female | g.7568140G > A | 53 | Definitive | Subepicardial circumferential in LV | 679 | No | No |
| Patient 4 | 60 | Male | p.Arg2284* | 58 | Silent carrier | No | 21 | No | No |
| Patient 5 | 48 | Male | p.Arg1045* | 48 | Definitive | Lineal infero-lateral in LV and RV free wall | 1544 | No | Yes |
| Patient 6 | 50 | Male | p.Arg1045* | 60 | Silent carrier | No | 51 | No | No |
| Patient 7 | 39 | Male | p.Arg2284* | 41 | Definitive | Subepicardial circumferential in LV | 381 | No | No |
| Patient 8 | 58 | Male | p.Asp960Glnfs*16 | 30 | Definitive | Subepicardial circumferential in LV | 3363 | Yes | No |
| Patient 9 | 31 | Male | p.Asp960Glnfs*16 | 55 | Silent carrier | No | 4 | No | No |
| Patient 10 | 62 | Female | p.Asp960Glnfs*16 | 57 | Definitive | No | 474 | No | No |
| Patient 11 | 62 | Male | p.Ile228Hisfs*29 | 22 | Definitive | CMR could not be performed | 29234 | No | Yes |
| Patient 12 | 53 | Female | p.Val2567Cys.Fs* | 60 | Definitive | No | <500 | No | No |
| Histopathological findings (H&E) | Immunohistochemistry | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| P | Epidermolysis | Parakeratosis | Hiper-Granulosis | Intercellular Spaces | Dehiscence | Fingerprint-Sign | Plakoglobin | Filamin C | Desmoplakin | Conexin 43 |
| 1 | No | Focal | Yes | Yes | Yes | Yes | Positive | Positive | Positive weak | Positive |
| 2 | No | Focal | Yes | Yes | Yes | Yes | Positive | Positive | Negative | Positive |
| 3 | No | No | Yes | Yes | No | Yes | Positive | Positive | Negative | Positive |
| 4 | No | Focal | Yes | Yes | No | Yes | Positive | Positive | Negative | Positive |
| 5 | No | No | Yes | Yes | Yes | Yes | Positive | Positive | Positive weak | Positive |
| 6 | No | No | Yes | Yes | No | Yes | Positive | Positive | Positive weak | Positive |
| 7 | Yes | No | Yes | Yes | Yes | Yes | Positive | Positive | Negative | Positive |
| 8 | Yes | No | Yes | Yes | Yes | Yes | Positive | Positive | Negative | Positive |
| 9 | Yes | No | Yes | Yes | Yes | Yes | Positive | Positive | Negative | Positive |
| 10 | No | No | Yes | Yes | Yes | Yes | Positive | Positive | Negative | Positive |
| 11 | Yes | No | Yes | Yes | Yes | Yes | Positive | Positive | Negative | Positive |
| 12 * | - | - | - | - | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabrera-Borrego, E.; Montero-Vilchez, T.; Bermúdez-Jiménez, F.J.; Tercedor-Sánchez, J.; Tercedor-Sánchez, L.; Sánchez-Díaz, M.; Macías-Ruiz, R.; Molina-Jiménez, M.; Cañizares-García, F.J.; Fernández-Segura, E.; et al. Heterozygous Arrhythmogenic Cardiomyopathy-desmoplakin Mutation Carriers Exhibit a Subclinical Cutaneous Phenotype with Cell Membrane Disruption and Lack of Intercellular Adhesion. J. Clin. Med. 2021, 10, 4608. https://doi.org/10.3390/jcm10194608
Cabrera-Borrego E, Montero-Vilchez T, Bermúdez-Jiménez FJ, Tercedor-Sánchez J, Tercedor-Sánchez L, Sánchez-Díaz M, Macías-Ruiz R, Molina-Jiménez M, Cañizares-García FJ, Fernández-Segura E, et al. Heterozygous Arrhythmogenic Cardiomyopathy-desmoplakin Mutation Carriers Exhibit a Subclinical Cutaneous Phenotype with Cell Membrane Disruption and Lack of Intercellular Adhesion. Journal of Clinical Medicine. 2021; 10(19):4608. https://doi.org/10.3390/jcm10194608
Chicago/Turabian StyleCabrera-Borrego, Eva, Trinidad Montero-Vilchez, Francisco José Bermúdez-Jiménez, Jesús Tercedor-Sánchez, Luis Tercedor-Sánchez, Manuel Sánchez-Díaz, Rosa Macías-Ruiz, María Molina-Jiménez, Francisco Javier Cañizares-García, Eduardo Fernández-Segura, and et al. 2021. "Heterozygous Arrhythmogenic Cardiomyopathy-desmoplakin Mutation Carriers Exhibit a Subclinical Cutaneous Phenotype with Cell Membrane Disruption and Lack of Intercellular Adhesion" Journal of Clinical Medicine 10, no. 19: 4608. https://doi.org/10.3390/jcm10194608