
Effect of Physical Therapy Modalities on Quality of Life of Head and Neck Cancer Survivors: A Systematic Review with Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
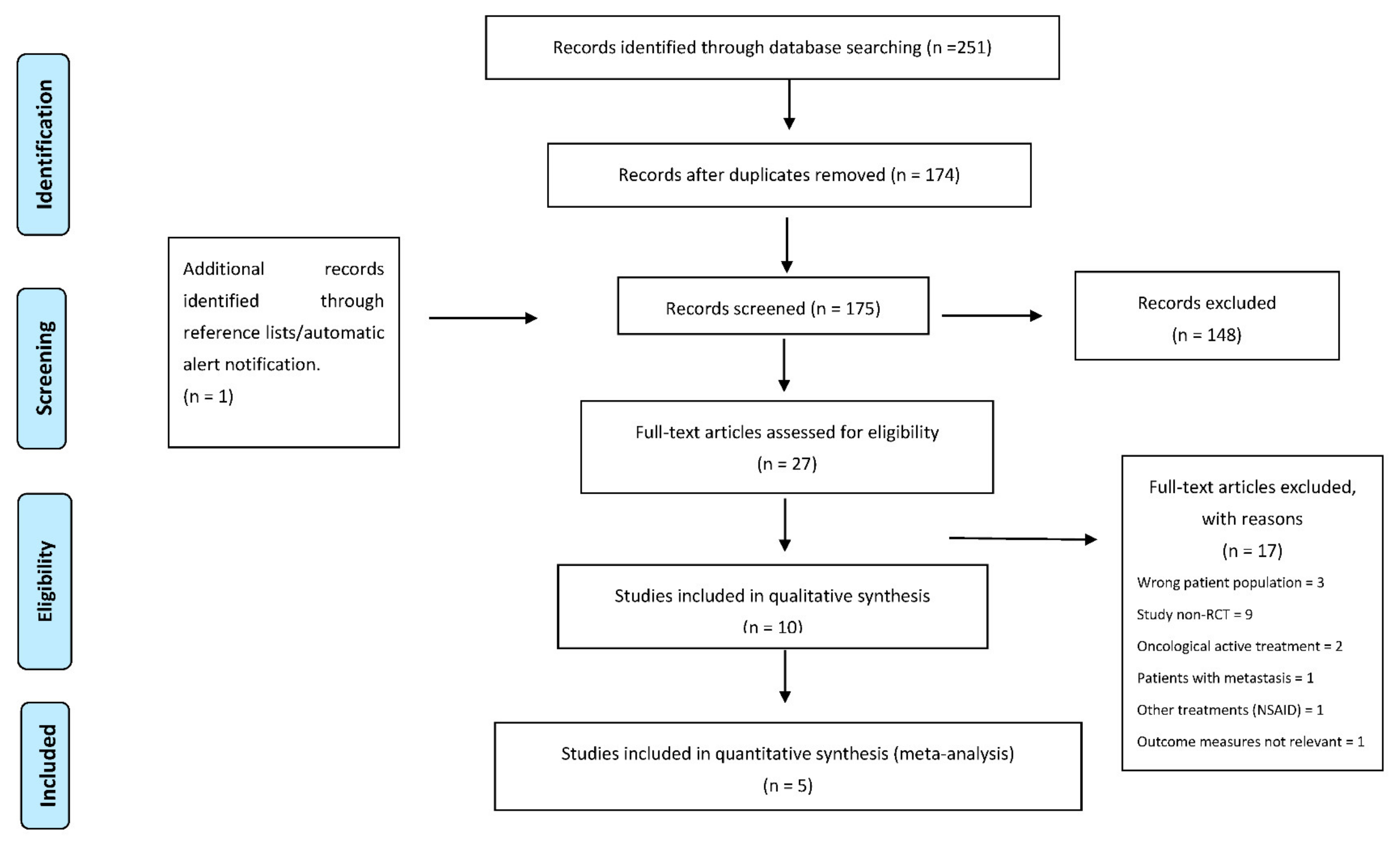
2.2. Search Strategy and Eligibility Criteria
2.3. Data Extraction and Quality Assessments
3. Results
3.1. Descriptive Synthesis
3.2. Adverse Events
3.3. Qualitative Analysis
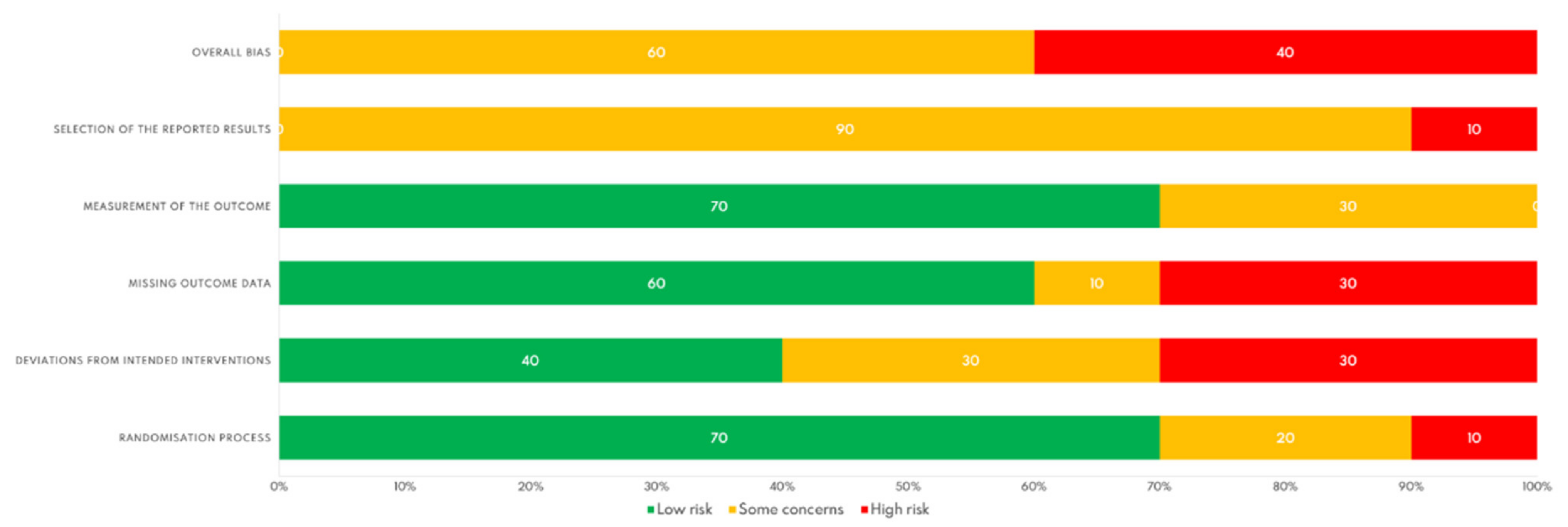
3.4. Risk of Bias in the Included RCTs
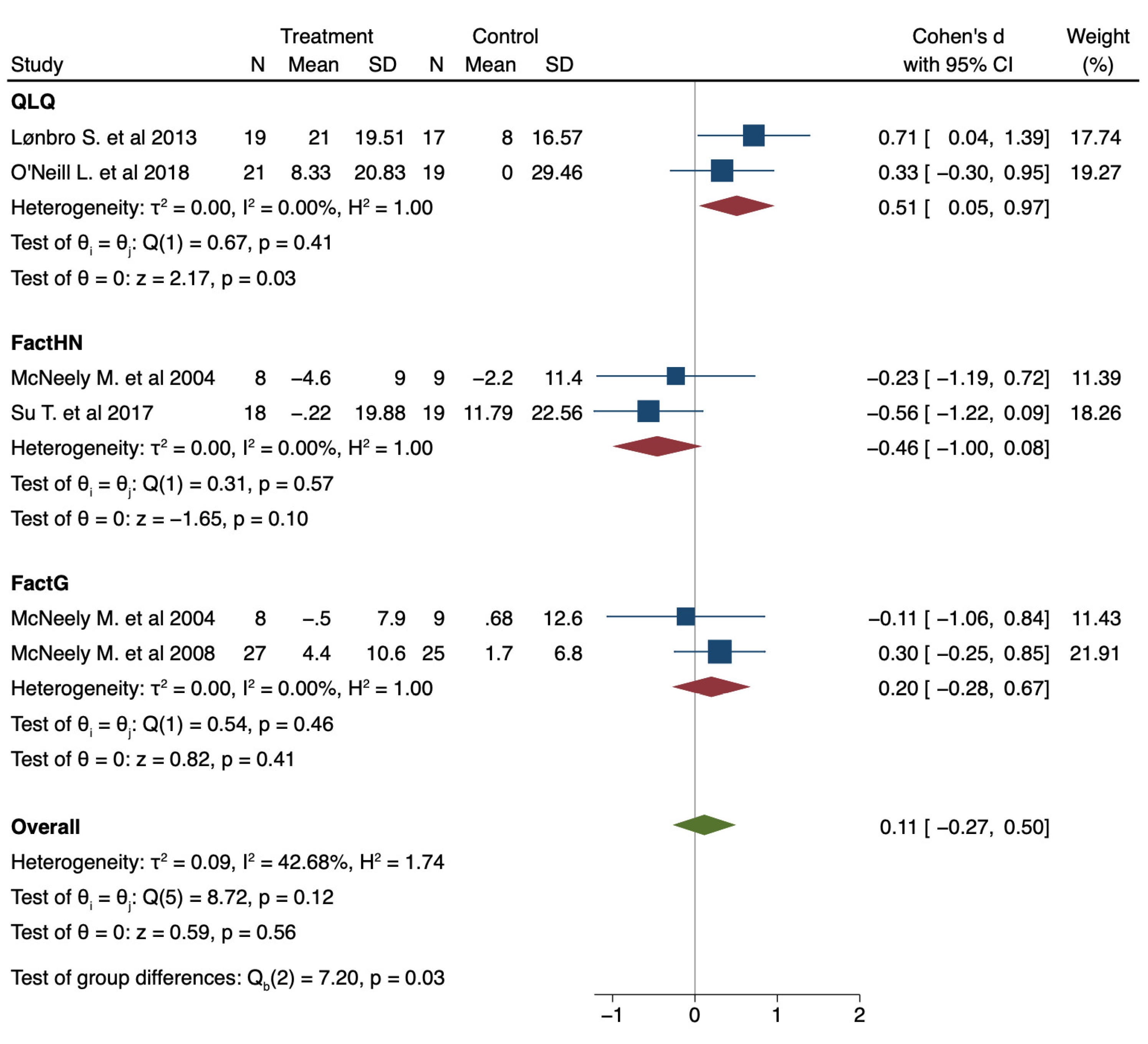
3.5. Meta-Analysis
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef]
- Haddad, R.I.; Shin, D.M. Recent Advances in Head and Neck Cancer. N. Engl. J. Med. 2008, 359, 1143–1154. [Google Scholar] [CrossRef]
- Haddad, R. Epidemiology, Staging, and Clinical Presentation of Human Papillomavirus-Associated Head and Neck Cancer. Available online: https://www.uptodate.com/contents/epidemiology-staging-and-clinical-presentation-of-human-papillomavirus-associated-head-and-neck-cancer?topicRef=89977&source=see_link (accessed on 14 November 2020).
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. National Cancer Institute SEER Cancer Statistics Review 1975–2013. Available online: http://seer.cancer.gov/csr/1975_2013/ (accessed on 13 October 2021).
- Cancer Research UK. Head and Neck Cancers Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/head-and-neck-cancers#heading-Two (accessed on 17 June 2020).
- Wissinger, E.; Griebsch, I.; Lungershausen, J.; Foster, T.; Pashos, C.L. The Economic Burden of Head and Neck Cancer: A Systematic Literature Review. Pharmacoeconomics 2014, 32, 865–882. [Google Scholar] [CrossRef]
- Ortiz-Comino, L.; Fernández-Lao, C.; Castro-Martín, E.; Lozano-Lozano, M.; Cantarero-Villanueva, I.; Arroyo-Morales, M.; Martín-Martín, L. Myofascial Pain, Widespread Pressure Hypersensitivity, and Hyperalgesia in the Face, Neck, and Shoulder Regions, in Survivors of Head and Neck Cancer. Support. Care Cancer 2020, 28, 2891–2898. [Google Scholar] [CrossRef]
- Bozec, A.; Schultz, P.; Gal, J.; Chamorey, E.; Chateau, Y.; Dassonville, O.; Poissonnet, G.; Demard, F.; Peyrade, F.; Saada, E.; et al. Evolution and Predictive Factors of Quality of Life in Patients Undergoing Oncologic Surgery for Head and Neck Cancer: A Prospective Multicentric Study. Surg. Oncol. 2019, 28, 236–242. [Google Scholar] [CrossRef]
- Nayak, S.G.; Pai, M.S.; George, S.L. Quality of Life of Patients with Head and Neck Cancer. J. Cancer Res. Ther. 2019, 15, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, S.; Soni, B.W.; Bahl, A.; Ghoshal, S. Radiotherapy-Induced Oral Morbidities in Head and Neck Cancer Patients. Spec. Care Dentist 2020, 40, 238–250. [Google Scholar] [CrossRef] [PubMed]
- McDowell, L.J.; Rock, K.; Xu, W.; Chan, B.; Waldron, J.; Lu, L.; Ezzat, S.; Pothier, D.; Bernstein, L.J.; So, N.; et al. Long-Term Late Toxicity, Quality of Life, and Emotional Distress in Patients with Nasopharyngeal Carcinoma Treated With Intensity Modulated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 340–352. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, J.; Shi, C.; Liu, L.; Wei, Y. Survival, Recurrence and Toxicity of HNSCC in Comparison of a Radiotherapy Combination with Cisplatin versus Cetuximab: A Meta-Analysis. BMC Cancer 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Crowder, S.L.; Douglas, K.G.; Yanina Pepino, M.; Sarma, K.P.; Arthur, A.E. Nutrition Impact Symptoms and Associated Outcomes in Post-Chemoradiotherapy Head and Neck Cancer Survivors: A Systematic Review. J. Cancer Surviv. 2018, 12, 479–494. [Google Scholar] [CrossRef] [PubMed]
- Parke, S.C.; Oza, S.; Shahpar, S.; Ngo-Huang, A.; Herbert, A.; Barksdale, T.; Gerber, L. Identifying Gaps in Research on Rehabilitation for Patients with Head and Neck Cancer: A Scoping Review. Arch. Phys. Med. Rehabil. 2019, 100, 2381–2388. [Google Scholar] [CrossRef]
- Berry, L.L.; Davis, S.W.; Godfrey Flynn, A.; Landercasper, J.; Deming, K.A. Is It Time to Reconsider the Term “Cancer Survivor”? J. Psychosoc. Oncol. 2019, 37, 413–426. [Google Scholar] [CrossRef]
- Surbone, A.; Annunziata, M.A.; Santoro, A.; Tirelli, U.; Tralongo, P. Cancer Patients and Survivors: Changing Words or Changing Culture? Ann. Oncol. 2013, 24, 2468–2471. [Google Scholar] [CrossRef]
- Ringash, J.; Bernstein, L.J.; Devins, G.; Dunphy, C.; Giuliani, M.; Martino, R.; McEwen, S. Head and Neck Cancer Survivorship: Learning the Needs, Meeting the Needs. Semin. Radiat. Oncol. 2018, 28, 64–74. [Google Scholar] [CrossRef]
- Nilsen, M.L.; Mady, L.J.; Hodges, J.; Wasserman-Wincko, T.; Johnson, J.T. Burden of Treatment: Reported Outcomes in a Head and Neck Cancer Survivorship Clinic. Laryngoscope 2019, 129, E437–E444. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, M.; McQuestion, M.; Jones, J.; Papadakos, J.; Le, L.W.; Alkazaz, N.; Cheng, T.; Waldron, J.; Catton, P.; Ringash, J. Prevalence and Nature of Survivorship Needs in Patients with Head and Neck Cancer. Head Neck 2016, 38, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, M.; Papadakos, J.; Broadhurst, M.; Jones, J.; McQuestion, M.; Le, L.W.; Beck, L.; Waldron, J.; Ringash, J. The Prevalence and Determinants of Return to Work in Head and Neck Cancer Survivors. Support. Care Cancer 2019, 27, 539–546. [Google Scholar] [CrossRef]
- Haddad, R.I.; Limaye, S. Overview of Approach to Long-Term Survivors of Head and Neck Cancer. Available online: https://www.uptodate.com/contents/overview-of-approach-to-long-term-survivors-of-head-and-neck-cancer (accessed on 14 November 2020).
- Forsythe, L.P.; Alfano, C.M.; Leach, C.R.; Ganz, P.A.; Stefanek, M.E.; Rowland, J.H. Who Provides Psychosocial Follow-up Care for Post-Treatment Cancer Survivors? A Survey of Medical Oncologists and Primary Care Physicians. J. Clin. Oncol. 2012, 30, 2897–2905. [Google Scholar] [CrossRef]
- Nekhlyudov, L.; Lacchetti, C.; Davis, N.B.; Garvey, T.Q.; Goldstein, D.P.; Nunnink, J.C.; Ruades Ninfea, J.I.; Salner, A.L.; Salz, T.; Siu, L.L. Head and Neck Cancer Survivorship Care Guideline: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Cancer Society Guideline. J. Clin. Oncol. 2017, 35, 1606–1621. [Google Scholar] [CrossRef]
- Baldoman, D.; Vandenbrink, R. Physical Therapy Challenges in Head and Neck Cancer. Cancer Treat. Res. 2018, 174, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Galiano-Castillo, N.; Postigo-Martin, P.; Cantarero-Villanueva, I. The Role of Physical Therapists in Oncology: The Great Unknown. Phys. Ther. Rev. 2020, 25, 235–237. [Google Scholar] [CrossRef]
- Gamble, G.L.; Gerber, L.H.; Spill, G.R.; Paul, K.L. The Future of Cancer Rehabilitation. Am. J. Phys. Med. Rehabil. 2011, 90, S76–S87. [Google Scholar] [CrossRef]
- Isaksson, J.; Wilms, T.; Laurell, G.; Fransson, P.; Ehrsson, Y.T. Meaning of Work and the Process of Returning after Head and Neck Cancer. Support. Care Cancer 2016, 24, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Effects of Supervised Exercise on Cancer-Related Fatigue in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. BMC Cancer 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Soares Falcetta, F.; de Araújo Vianna Träsel, H.; de Almeida, F.K.; Rangel Ribeiro Falcetta, M.; Falavigna, M.; Dornelles Rosa, D. Effects of Physical Exercise after Treatment of Early Breast Cancer: Systematic Review and Meta-Analysis. Breast Cancer Res. Treat. 2018, 170, 455–476. [Google Scholar] [CrossRef]
- Bekhet, A.H.; Abdalla, A.R.; Ismail, H.M.; Genena, D.M.; Osman, N.A.; El Khatib, A.; Abbas, R.L. Benefits of Aerobic Exercise for Breast Cancer Survivors: A Systematic Review of Randomized Controlled Trials. Asian Pac. J. Cancer Prev. 2019, 20, 3197–3209. [Google Scholar] [CrossRef] [PubMed]
- Del-Rosal-Jurado, A.; Romero-Galisteo, R.; Trinidad-Fernández, M.; González-Sánchez, M.; Cuesta-Vargas, A.; Ruiz-Muñoz, M. Therapeutic Physical Exercise Post-Treatment in Breast Cancer: A Systematic Review of Clinical Practice Guidelines. J. Clin. Med. 2020, 9, 1239. [Google Scholar] [CrossRef]
- Balhareth, A.; Aldossary, M.Y.; McNamara, D. Impact of Physical Activity and Diet on Colorectal Cancer Survivors’ Quality of Life: A Systematic Review. World J. Surg. Oncol. 2019, 17, 1–12. [Google Scholar] [CrossRef]
- Brandenbarg, D.; Korsten, J.H.W.M.; Berger, M.Y.; Berendsen, A.J. The Effect of Physical Activity on Fatigue among Survivors of Colorectal Cancer: A Systematic Review and Meta-Analysis. Support. Care Cancer 2018, 26, 393–403. [Google Scholar] [CrossRef]
- Liu, L.; He, X.; Feng, L. Exercise on Quality of Life and Cancer-Related Fatigue for Lymphoma Survivors: A Systematic Review and Meta-Analysis. Support. Care Cancer 2019, 27, 4069–4082. [Google Scholar] [CrossRef]
- Toohey, K.; Pumpa, K.; McKune, A.; Cooke, J.; Semple, S. High-Intensity Exercise Interventions in Cancer Survivors: A Systematic Review Exploring the Impact on Health Outcomes. J. Cancer Res. Clin. Oncol. 2018, 144. [Google Scholar] [CrossRef] [PubMed]
- Fuller, J.T.; Hartland, M.C.; Maloney, L.T.; Davison, K. Therapeutic Effects of Aerobic and Resistance Exercises for Cancer Survivors: A Systematic Review of Meta-Analyses of Clinical Trials. Br. J. Sports Med. 2018, 52, 1311. [Google Scholar] [CrossRef]
- Ma, S.J.; Rivers, C.I.; Serra, L.M.; Singh, A.K. Long-Term Outcomes of Interventions for Radiation-Induced Xerostomia: A Review. World J. Clin. Oncol. 2019, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Paim, É.D.; Berbert, M.C.B.; Zanella, V.G.; Macagnan, F.E. Electrical Stimulation in the Treatment of Radiotherapy-Induced Hyposalivation. Codas 2019, 31, 1–7. [Google Scholar] [CrossRef]
- Sousa, A.S.; Silva, J.F.; Pavesi, V.C.S.; Carvalho, N.A.; Ribeiro-Júnior, O.; Varellis, M.L.Z.; Prates, R.A.; Bussadori, S.K.; Gonçalves, M.L.L.; Horliana, A.C.R.T.; et al. Photobiomodulation and Salivary Glands: A Systematic Review. Lasers Med. Sci. 2020, 35, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, V.; Al Hamad, A.; Lodi, G.; Porter, S.; Fedele, S. Interventions for the Management of Radiotherapy-Induced Xerostomia and Hyposalivation: A Systematic Review and Meta-Analysis. Oral Oncol. 2017, 66, 64–74. [Google Scholar] [CrossRef]
- Shao, C.H.; Chiang, C.C.; Huang, T.W. Exercise Therapy for Cancer Treatment-Induced Trismus in Patients with Head and Neck Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Radiother. Oncol. 2020, 151, 249–255. [Google Scholar] [CrossRef]
- Almeida, K.A.M.; Rocha, A.P.; Carvas, N.; Pinto, A.C.P.N. Rehabilitation Interventions for Shoulder Dysfunction in Patients with Head and Neck Cancer: Systematic Review and Meta-Analysis. Phys. Ther. 2020, 100, 1997–2008. [Google Scholar] [CrossRef]
- Cousins, N.; MacAulay, F.; Lang, H.; MacGillivray, S.; Wells, M. A Systematic Review of Interventions for Eating and Drinking Problems Following Treatment for Head and Neck Cancer Suggests a Need to Look beyond Swallowing and Trismus. Oral Oncol. 2013, 49, 387–400. [Google Scholar] [CrossRef]
- Heiskanen, V.; Zadik, Y.; Elad, S. Photobiomodulation Therapy for Cancer Treatment-Related Salivary Gland Dysfunction: A Systematic Review. Photobiomodulation Photomed. Laser Surg. 2020, 38, 340–347. [Google Scholar] [CrossRef]
- Kamstra, J.I.; van Leeuwen, M.; Roodenburg, J.L.N.; Dijkstra, P.U. Exercise Therapy for Trismus Secondary to Head and Neck Cancer: A Systematic Review. Head Neck 2017, 39, 160–169. [Google Scholar] [CrossRef]
- Kraaijenga, S.A.C.; Van Der Molen, L.; Van Den Brekel, M.W.M.; Hilgers, F.J.M. Current Assessment and Treatment Strategies of Dysphagia in Head and Neck Cancer Patients: A Systematic Review of the 2012/13 Literature. Curr. Opin. Support. Palliat. Care 2014, 8, 152–163. [Google Scholar] [CrossRef]
- Perry, A.; Lee, S.H.; Cotton, S.; Kennedy, C. Therapeutic Exercises for Affecting Post-Treatment Swallowing in People Treated for Advanced-Stage Head and Neck Cancers. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Scherpenhuizen, A.; Van Waes, A.M.A.; Janssen, L.M.; Van Cann, E.M.; Stegeman, I. The Effect of Exercise Therapy in Head and Neck Cancer Patients in the Treatment of Radiotherapy-Induced Trismus: A Systematic Review. Oral Oncol. 2015, 51, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Tyker, A.; Franco, J.; Massa, S.T.; Desai, S.C.; Walen, S.G. Treatment for Lymphedema Following Head and Neck Cancer Therapy: A Systematic Review. Am. J. Otolaryngol. Head Neck Med. Surg. 2019, 40, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence Systematic Review Software. Available online: www.covidence.org (accessed on 13 October 2021).
- Bjordal, K.; Graeff, A.; Fayers, P.M.; Hammerlid, E.; Pottelsberghe, C.V.; Arraras, J.J.; Feine, J.S.; Abendstein, H.; Morton, R.P. A 12 Country Eld Study of the EORTC QLQ-C30 (Version 3.0) and the Head and Neck Cancer Specific Module (EORTC QLQ-H&N35) in Head and Neck Patients. EORTC Quality of Life Group. Eur. J. Cancer 2000, 36, 1796–1807. [Google Scholar]
- Yount, S.; List, M.; Du, H.; Yost, K.; Bode, R.; Brockstein, B.; Argiris, A.; Vokes, E.; Cohen, E.E.W.; Campbell, B.; et al. A Randomized Validation Study Comparing Embedded versus Extracted FACT Head and Neck Symptom Index Scores. Qual. Life Res. 2007, 16, 1615–1626. [Google Scholar] [CrossRef]
- Funk, G.F.; Karnell, L.H.; Christensen, A.J.; Moran, P.J.; Ricks, J. Comprehensive Head and Neck Oncology Health Status Assessment. Head Neck 2003, 25, 561–575. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, 1–8. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. Landis Amd Koch1977_agreement of Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- McNeely, M.L.; Parliament, M.B.; Seikaly, H.; Jha, N.; Magee, D.J.; Haykowsky, M.J.; Courneya, K.S. Effect of Exercise on Upper Extremity Pain and Dysfunction in Head and Neck Cancer Survivors: A Randomized Controlled Trial. Cancer 2008, 113, 214–222. [Google Scholar] [CrossRef]
- McNeely, M.L.; Parliament, M.; Courneya, K.S.; Seikaly, H.; Jha, N.; Scrimger, R.; Henson, J. A Pilot Study of a Randomized Controlled Trial to Evaluate the Effects of Progressive Resistance Exercise Training on Shoulder Dysfunction Caused by Spinal Accessory Neurapraxia/Neurectomy in Head and Neck Cancer Survivors. Head Neck 2004, 26, 518–530. [Google Scholar] [CrossRef]
- Lavigne, C.; Twomey, R.; Lau, H.; Francis, G.; Culos-Reed, S.N.; Millet, G.Y. Feasibility of Eccentric Overloading and Neuromuscular Electrical Stimulation to Improve Muscle Strength and Muscle Mass after Treatment for Head and Neck Cancer. J. Cancer Surviv. 2020, 14, 790–805. [Google Scholar] [CrossRef]
- Wong, R.K.W.; Jones, G.W.; Sagar, S.M.; Babjak, A.F.; Whelan, T. A Phase I-II Study in the Use of Acupuncture-like Transcutaneous Nerve Stimulation in the Treatment of Radiation-Induced Xerostomia in Head-and-Neck Cancer Patients Treated with Radical Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 472–480. [Google Scholar] [CrossRef]
- Chang, Y.L.; Tsai, Y.F.; Hsu, C.L.; Chao, Y.K.; Hsu, C.C.; Lin, K.C. The Effectiveness of a Nurse-Led Exercise and Health Education Informatics Program on Exercise Capacity and Quality of Life among Cancer Survivors after Esophagectomy: A Randomized Controlled Trial. Int. J. Nurs. Stud. 2020, 101, 103418. [Google Scholar] [CrossRef]
- Su, T.L.; Chen, A.N.; Leong, C.P.; Huang, Y.C.; Chiang, C.W.; Chen, I.H.; Lee, Y.Y. The Effect of Home-Based Program and Outpatient Physical Therapy in Patients with Head and Neck Cancer: A Randomized, Controlled Trial. Oral Oncol. 2017, 74, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Lønbro, S.; Dalgas, U.; Primdahl, H.; Johansen, J.; Nielsen, J.L.; Aagaard, P.; Hermann, A.P.; Overgaard, J.; Overgaard, K. Progressive Resistance Training Rebuilds Lean Body Mass in Head and Neck Cancer Patients after Radiotherapy—Results from the Randomized DAHANCA 25B Trial. Radiother. Oncol. 2013, 108, 314–319. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, L.M.; Guinan, E.; Doyle, S.L.; Bennett, A.E.; Murphy, C.; Elliott, J.A.; O’Sullivan, J.; Reynolds, J.V.; Hussey, J. The RESTORE Randomized Controlled Trial: Impact of a Multidisciplinary Rehabilitative Program on Cardiorespiratory Fitness in Esophagogastric Cancer Survivorship. Ann. Surg. 2018, 268, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Saleh, J.; Figueiredo, M.A.Z.; Cherubini, K.; Braga-Filho, A.; Salum, F.G. Effect of Low-Level Laser Therapy on Radiotherapy-Induced Hyposalivation and Xerostomia: A Pilot Study. Photomed. Laser Surg. 2014, 32, 546–552. [Google Scholar] [CrossRef]
- Langmore, S.E.; McCulloch, T.M.; Krisciunas, G.P.; Lazarus, C.L.; Van Daele, D.J.; Pauloski, B.R.; Rybin, D.; Doros, G. Efficacy of Electrical Stimulation and Exercise for Dysphagia in Patients with Head and Neck Cancer: A Randomized Clinical Trial. Head Neck 2016, 38, E1221–E1231. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Services, H. Physical Activity Guidelines Advisory Committee Report, 2008: To the Secretary of Health and Human Services. Nutr. Rev. 2009, 67, 114–120. [Google Scholar] [CrossRef]
- Stubblefield, M.D. Radiation Fibrosis Syndrome: Neuromuscular and Musculoskeletal Complications in Cancer Survivors. PM&R 2011, 3, 1041–1054. [Google Scholar] [CrossRef]
- Van Wilgen, C.P.; Dijkstra, P.U.; van der Laan, B.F.A.M.; Plukker, J.T.; Roodenburg, J.L.N. Morbidity of the Neck after Head and Neck Cancer Therapy. Head Neck 2004, 26, 785–791. [Google Scholar] [CrossRef]
- Carr, S.D.; Bowyer, D.; Cox, G. Upper Limb Dysfunction Following Selective Neck Dissection: A Retrospective Questionnaire Study. Head Neck 2009, 31, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Gane, E.M.; O’Leary, S.P.; Hatton, A.L.; Panizza, B.J.; McPhail, S.M. Neck and Upper Limb Dysfunction in Patients Following Neck Dissection: Looking beyond the Shoulder. Otolaryngol. Neck Surg. 2017, 157, 631–640. [Google Scholar] [CrossRef]
- Gane, E.M.; Michaleff, Z.A.; Cottrell, M.A.; McPhail, S.M.; Hatton, A.L.; Panizza, B.J.; O’Leary, S.P. Prevalence, Incidence, and Risk Factors for Shoulder and Neck Dysfunction after Neck Dissection: A Systematic Review. Eur. J. Surg. Oncol. 2017, 43, 1199–1218. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and Physical Activity Guidelines for Cancer Survivors. CA. Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.P.; Yi, J.; McClellan, J.; Kim, J.; Tian, T.; Grahmann, B.; Kirchhoff, A.C.; Holton, A.; Wright, J. Barriers and Facilitators of Healthy Diet and Exercise Among Adolescent and Young Adult Cancer Survivors: Implications for Behavioral Interventions. J. Adolesc. Young Adult Oncol. 2015, 4, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Cranen, K.; Groothuis-Oudshoorn, C.G.; Vollenbroek-Hutten, M.M.; IJzerman, M.J. Toward Patient-Centered Telerehabilitation Design: Understanding Chronic Pain Patients’ Preferences for Web-Based Exercise Telerehabilitation Using a Discrete Choice Experiment. J. Med. Internet Res. 2017, 19, e26. [Google Scholar] [CrossRef] [PubMed]
- Batalik, L.; Winnige, P.; Dosbaba, F.; Vlazna, D.; Janikova, A. Home-Based Aerobic and Resistance Exercise Interventions in Cancer Patients and Survivors: A Systematic Review. Cancers 2021, 13, 1915. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Ariza-García, A.; Díaz-Rodríguez, L.; Del-Moral-Ávila, R.; Arroyo-Morales, M. Telehealth System: A Randomized Controlled Trial Evaluating the Impact of an Internet-Based Exercise Intervention on Quality of Life, Pain, Muscle Strength, and Fatigue in Breast Cancer Survivors. Cancer 2016, 122, 3166–3174. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Sweeney, F.C.; Stewart, C.; Buchanan, T.A.; Spicer, D.; Tripathy, D.; et al. Aerobic and Resistance Exercise Improves Physical Fitness, Bone Health, and Quality of Life in Overweight and Obese Breast Cancer Survivors: A Randomized Controlled Trial. Breast Cancer Res. 2018, 20, 124. [Google Scholar] [CrossRef] [PubMed]
- Penttinen, H.; Utriainen, M.; Kellokumpu-Lehtinen, P.-L.; Raitanen, J.; Sievänen, H.; Nikander, R.; Blomqvist, C.; Huovinen, R.; Vehmanen, L.; Saarto, T. Effectiveness of a 12-Month Exercise Intervention on Physical Activity and Quality of Life of Breast Cancer Survivors; Five-Year Results of the BREX-Study. In Vivo 2019, 33, 881–888. [Google Scholar] [CrossRef]
- Kim, J.Y.; Lee, M.K.; Lee, D.H.; Kang, D.W.; Min, J.H.; Lee, J.W.; Chu, S.H.; Cho, M.S.; Kim, N.K.; Jeon, J.Y. Effects of a 12-Week Home-Based Exercise Program on Quality of Life, Psychological Health, and the Level of Physical Activity in Colorectal Cancer Survivors: A Randomized Controlled Trial. Support. Care Cancer 2019, 27, 2933–2940. [Google Scholar] [CrossRef]
- Brown, J.C.; Damjanov, N.; Courneya, K.S.; Troxel, A.B.; Zemel, B.S.; Rickels, M.R.; Ky, B.; Rhim, A.D.; Rustgi, A.K.; Schmitz, K.H. A Randomized Dose-Response Trial of Aerobic Exercise and Health-Related Quality of Life in Colon Cancer Survivors. Psychooncology 2018, 27, 1221–1228. [Google Scholar] [CrossRef]
- Cantarero-Villanueva, I.; Cuesta-Vargas, A.I.; Lozano-Lozano, M.; Fernández-Lao, C.; Fernández-Pérez, A.; Galiano-Castillo, N. Changes in Pain and Muscle Architecture in Colon Cancer Survivors After a Lumbopelvic Exercise Program: A Secondary Analysis of a Randomized Controlled Trial. Pain Med. 2017, 18, 1366–1376. [Google Scholar] [CrossRef]
- Postigo-Martin, P.; Peñafiel-Burkhardt, R.; Gallart-Aragón, T.; Alcaide-Lucena, M.; Artacho-Cordón, F.; Galiano-Castillo, N.; Fernández-Lao, C.; Martín-Martín, L.; Lozano-Lozano, M.; Ruíz-Vozmediano, J.; et al. Attenuating Treatment-Related Cardiotoxicity in Women Recently Diagnosed With Breast Cancer via a Tailored Therapeutic Exercise Program: Protocol of the ATOPE Trial. Phys. Ther. 2021, 101. [Google Scholar] [CrossRef]
- Furness, S.; Worthington, H.V.; Bryan, G.; Birchenough, S.; McMillan, R. Interventions for the Management of Dry Mouth: Topical Therapies. Cochrane Database Syst. Rev. 2011, 12, CD008934. [Google Scholar] [CrossRef]
- Doering, B.K.; Rief, W.; Petrie, K.J. Lessons to Be Learned from Placebo Arms in Psychopharmacology Trials. In Placebo; Springer: Heidelberg, Germany, 2014; pp. 273–290. [Google Scholar]
- Wong, R.K.W.; James, J.L.; Sagar, S.; Wyatt, G.; Nguyen-Tân, P.F.; Singh, A.K.; Lukaszczyk, B.; Cardinale, F.; Yeh, A.M.; Berk, L. Phase 2 Results from Radiation Therapy Oncology Group Study 0537. Cancer 2012, 118, 4244–4252. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Liu, L.; Lozano-Lozano, M.; Tumilty, S.; Cantarero-Villanueva, I.; Baxter, G.D. Acute and Cumulative Benefits of Photobiomodulation for Xerostomia: A Systematic Review and Meta-analysis. Oral Dis. 2021, 27, 1115–1126. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Hodgson, T.A.; Ship, J.A.; Schiødt, M. Management of Salivary Hypofunction during and after Radiotherapy. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. Endodontology 2007, 103, S66.e1–S66.e19. [Google Scholar] [CrossRef]
- Cramp, F.; James, A.; Lambert, J. The Effects of Resistance Training on Quality of Life in Cancer: A Systematic Literature Review and Meta-Analysis. Support. Care Cancer 2010, 18, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- McNeely, M.L. Effects of Exercise on Breast Cancer Patients and Survivors: A Systematic Review and Meta-Analysis. Can. Med. Assoc. J. 2006, 175, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Nadler, M.B.; Desnoyers, A.; Langelier, D.M.; Amir, E. The Effect of Exercise on Quality of Life, Fatigue, Physical Function, and Safety in Advanced Solid Tumor Cancers: A Meta-Analysis of Randomized Control Trials. J. Pain Symptom Manag. 2019, 58, 899–908. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Country | Study Design | Sample Size | Gender (% Male) | Mean Age (Years) | Stage of Cancer at Diagnosis (%) | Location of HNC (%) | Oncological Treatment (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I–II | III–IV | Pharynx | Larynx | Oral Cavity | Lip | Others | RT | CT | S | CRT | S + RT | S + CT | RT + S+CT | ||||||
| Chang et al., 2020 | China | RCT | 88 | 91% | 56 | * | * | 20 | 0 | 0 | 0 | 80 | 0 | 0 | 100 | 0 | 0 | 0 | 0 |
| Langmore et al., 2016 | United States | RCT | 170 | 86% | 61.9 | 15 | 85 | 70 | 12 | 8 | 0 | 10 | 29 | 0 | 0 | 71 | 0 | 0 | 0 |
| Lavigne et al., 2020 | Canada | RCT | 22 | 64% | 52 | 45 | 55 | 59 | 5 | 18 | 0 | 18 | 0 | 82 | 18 | 0 | 0 | 0 | 0 |
| Lønbro et al., 2013 | Denmark | RCT | 41 | 66% | 57 | 20 | 80 | 73 | 2 | 7 | 0 | 17 | 49 | 51 | 0 | 0 | 0 | 0 | 0 |
| McNeely et al., 2004 | Canada | RCT | 20 | 82% | 61 | 18 | 82 | 47 | 29 | 12 | 0 | 12 | 0 | 0 | 6 | 0 | 94 | 0 | 0 |
| McNeely et al., 2008 | Canada | RCT | 52 | 71% | 52 | 18 | 82 | 62 | 23 | 0 | 0 | 15 | 0 | 0 | 0 | 0 | 75 | 25 | 0 |
| O’Neill et al., 2018 | Ireland | RCT | 43 | 81% | 66 | 49 | 51 | 0 | 0 | 0 | 0 | 100 | 0 | 0 | 100 | 0 | 0 | 0 | 0 |
| Saleh et al., 2014 | Brazil | RCT | 23 | 65% | 57 | 17 | 83 | * | * | * | * | * | 0 | 0 | 0 | 26 | 43 | 0 | 30 |
| Su et al., 2017 | China | RCT | 37 | 92% | 48 | 30 | 70 | 0 | 0 | 81 | 0 | 19 | 30 | 43 | 27 | 0 | 30 | 43 | 0 |
| Wong et al., 2003 | Canada | RCT | 37 | 75% | 59 | * | * | * | * | * | * | * | 100 | 0 | 0 | 0 | 0 | 0 | 0 |
| Exercise | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Sample Size | Intervention | Frequency | Duration | Comparison | Outcome Measures | Adverse Events | Measured Time Points | IG (Mean, SD) | CG (Mean, SD) | Mean Change (Mean, SD) | Group Differences in Mean Change: Mean (95% CI) | p-Values | |
| Chang et al., 2020 | 44 IG 44 CG | Walking exercise and nursing education health informatics program | 3–5 days per week for 30 min each time, or a total of 150 min per week (from 55% to 65% of HRR) | 12 weeks | Usual Care | EORTC QLQ-C30 | Not reported | Baseline, week 4, week 12, 3-month follow-up | Baseline: 47.5 (5.64) | Baseline: 44.5 (8.50) | Not reported | Not reported | Within groups Baseline–week 4: IG and CG p < 0.001 Baseline–week 12: IG and CG p < 0.001 Baseline–3-month follow-up: IG and CG p < 0.001 Between groups (IG vs. CG) Week 4: IG > CG p < 0.05 | |
| Lønbro et al., 2013 | 20 IG 21 CG | PRT: leg press, knee extension, hamstring curls, chest press, sit ups, back extensions and lateral pull down. | 2–3 sets of 8–15 RM of 7 exercises. 2 to 3 sessions per week. 30 sessions total | 12 weeks | Usual Care | EORTC QLQ-C30 | No | Baseline and week 12 | Baseline: 53 ± 19 Week 12: 74 ± 20 | Baseline: 70 ± 15 Week 12: 78 ± 18 | Baseline–week 12: IG: 19 ± 14//CG: 6 ± 12 | Not reported | Within groups Baseline–week 12: IG p < 0.001/CG p < 0.05 Between groups (IG vs. CG) Baseline–week 12: IG >CG p < 0.05 | |
| McNeely et al., 2004 | 10 IG 10 CG | PRT on upper limbs and scapular muscles | 1-2 sets of 15 to 25 RM of 6 exercises. 3 times per week | 12 weeks | Usual Care | FACT H&N | No | Baseline and week 12 | Baseline: 109.5 (12.2) Week 12: 104.8 (18.5) | Baseline: 103.1 (22.4) Week 12: 100.9 (23.9) | CG: −2.2 (11.4) IG: −4.6 (9.0) | −2.4 (−13.2 to 8.3) | Within groups Baseline–week 12: IG and CG p > 0.05 Between groups (IG vs. CG) Baseline–week 12: p = 0.639 | |
| McNeely et al., 2008 | 27 IG 25 CG | PRT on upper limbs and scapular muscles | 2 sets of 10 to 15 repetitions of 5 to 8 exercises. Between 25% at initial and 70% at the end of the program of the 1-RM, 3 times per week | 12 weeks | Usual Care | FACT G | Pain | Baseline and week 12 | Baseline: 79.4 (13.7) Week 12: 83.9 (15.6) | Baseline: 76.4 (18.4) Week 12: 78.1 (19.3) | CG: +1.7 (6.9) IG: +4.4 (10.6) | +4.5 (−0.7 to 9.7) | Within groups Not reported Between groups (IG vs. CG) Baseline–week 12: p = 0.091 | |
| O’Neill et al., 2018 | 21 IG 22 CG | Aerobic: walking, stationary cycling and cross training PRT: upper and lower limb muscles | Aerobic: 3 to 5 days per week (from 30% of HRR at initial weeks to 60% of HRR at the end of the program)PRT: twice a week (from 2 sets/muscle groups at initial weeks to 6 sets/muscle groups at the end of the program) | 12 weeks | Usual Care | EORTC QLQ-C30 | No | Baseline, immediately postintervention and at 3-month follow-up | Baseline: 75.00 (20.83) Week 12: 83.33 (20.83) 3-month follow up: 79.17 (29.16) | Baseline: 66.67 (33.33) Week 12: 66.67 (25.00) 3-month follow up: 75.00 (16.6) | Not reported | Not reported | Within groups Not reported Between groups (IG vs. CG) Baseline–week 12: p = 0.433 Baseline–3-month follow-up: p = 0.887 | |
| Su et al., 2017 | 18 IG/19 CG | HBP Aerobic: walking PRT: upper limb muscles | Once a day/5 days per week Aerobic: 50 min PRT: 2 sets/10 repetitions/muscle group | 12 consecutive weeks | OPT: Aerobic: Walking was performed on treadmill. No PRT | FACT H&N | Not reported | Baseline, week 6, week 12 | Baseline: 93.83 (19.73) Week 6: 94.89 (22.44) Week 12: 93.61 (21.487) | Baseline: 91.63 (23.59) Week 6: 95.21 (22.27) Week 12: 103.42 (20.02) | Not reported | Not reported | Within groups Baseline–week 12: IG and CG p > 0.05 Between groups (IG vs. CG) Baseline–week 12: p = 0.074 | |
| Electrophysical Agent | ||||||||||||||
| Author | Sample Size | Intervention | Parameters | Frequency | Time | Comparison | Outcome Measures | Adverse Events | Measured Time Points | QoL IG (Mean, SD) | QoL CG (Mean, SD) | Mean Change (Mean, SD) | Group Differences in Mean Change: Mean (95% CI) | p-Values |
| Wong et al., 2003 | Group A: 13 Group B: 10 Group C: 14 | ALTENS Group A: Sp6, St36, LI4 (active electrodes) and CV24 (indifferent electrode) | Nonpolarizing, balanced, biphasic, square electrical pulses of 250-ms. Trains with a repetition rate of 4 Hz. Each acupuncture point was randomly stimulated for 10 s each time | Twice weekly | 6 weeks | ALTENS Group B: Sp6, St36, P6 (active electrodes) and CV24 (indifferent electrode) Group C: Sp6, St5 and 6, P6 (active electrodes) and CV24 (indifferent electrode) | Head and Neck Radiotherapy Questionnaire | No | Baseline and 6, 8 and 12 weeks after treatment began and at 3, 6 and 12 months after treatment completion. | Not reported | Not reported | Not reported | Not reported | Within groups Not reported Between groups (IG vs. CG) Baseline–6 month follow-up: p > 0.05 |
| Saleh et al., 2014 | 12 IG/11 CG | Laser therapy Application on major salivary glands, parotid, submandibular and sublingual glands | Continuous wave mode. 830nm (infrared) wavelength, 100 mW output power, 3.57 W/cm2 power density, 71 J/cm2 dose per point, 2 J energy per point, application time 20 sec per point and 28 J dose per session. The area of the spot was 0.028 cm2 | Twice a week | 6 weeks | Sham laser therapy | OHIP-14 | Not reported | Baseline, 6th session, 12th session | Baseline: 10.48 (6.82–14.00) 6th session: 7.55 (5.65–11.19) 12th session: 2.5(1.69–9.84) | Baseline:10.23 (6.39–12.82) 6th session: 5.17 (2.28–10.69) 12th session: 3.53 (0.66–10.44) | Not reported | Not reported | Within groups Baseline–12th session IG and CG p < 0.05 Between groups (IG vs. CG) Baseline, p = 0.786 6th session, p = 0.413 12th session, p = 0.976 |
| Langmore et al., 2016 | 116 IG/54 CG | E-stim device: Electrical Stimulation to stimulate the suprahyoid muscles + swallow exercises. 5-minute warmup stretching protocol followed by swallowing 60 times in synchrony with the stimulation | Frequency 70 Hz Pulse width 300 microseconds (range, 130–300) Contraction 4 s (range, 4–8) Relaxation 12 s (range, 12–16) Ramp up 2 s (range, 2–4) Ramp down 0 s Amplitude limit 0–99 Treatment time 20 min or longer if needed | Twice per day, 6 days per week | 12 weeks | Sham device+ swallow exercises. 5-minute warmup stretching protocol followed by swallowing 60 times in synchrony with the stimulation | HNCI | Not reported | Week 7 and week 12 | Baseline: 32.54 (21.04) Week 12: 38.85 (23.97) | Baseline: 24.18 (18.58) Week 12: 30.93 (20.46) | IG: 6.31 (17.92) CG: 6.74 (15.59) | HNCI Speech:−3.37 (29.81 to 3.06) HNCI eating 1.41 (25.28 to 8.10) HNCI aesthetics 0.49 (27.98 to 8.95) HNCI social disruption −3.11 (210.28 to 4.05) | Within groups Baseline–week 12 IG: HNCI speech: p = 0.016 HNCI eating: p < 0.001 CG: HNCI speech: p = 0.001 HNCI eating: p = 0.003 Between groups (IG vs. CG) Baseline–week 12 HNCI Speech: p = 0.304 HNCI Eating: p = 0.679 HNCI aesthetics: p = 0.910 HNCI social disruption: p = 0.395 |
| Lavigne et al., 2020 | 11 IG/11 CG | NMES and eccentrically overloaded unilateral squats | 2 sets × 8 repetitions of unilateral squats. Negative electrode over the femoral triangle of each leg, 1–3 cm below the inguinal ligament. The positive electrodes over the vastus lateralis and distally over the vastus medialis of each leg Frequency: 40 Hz Pulse duration: 180 μs. Contraction–relaxation period: 5 s/10 sRamp-up time: 1.5 s Ramp-down time: 0–75 s | Three times per week | 12 weeks | Conventional strength training | FACT H&N | No | Baseline and week 12 | Baseline: 116 (18) Week 12: 126 (14) | Baseline: 103 (17) Week 12: 122 (13) | IG: 10 (9) CG: 18 (9) | Not reported | Within groups Baseline–week 12 IG and CG p = 0.001 Between groups (IG vs. CG) Baseline–week 12 p > 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgos-Mansilla, B.; Galiano-Castillo, N.; Lozano-Lozano, M.; Fernández-Lao, C.; Lopez-Garzon, M.; Arroyo-Morales, M. Effect of Physical Therapy Modalities on Quality of Life of Head and Neck Cancer Survivors: A Systematic Review with Meta-Analysis. J. Clin. Med. 2021, 10, 4696. https://doi.org/10.3390/jcm10204696
Burgos-Mansilla B, Galiano-Castillo N, Lozano-Lozano M, Fernández-Lao C, Lopez-Garzon M, Arroyo-Morales M. Effect of Physical Therapy Modalities on Quality of Life of Head and Neck Cancer Survivors: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2021; 10(20):4696. https://doi.org/10.3390/jcm10204696
Chicago/Turabian StyleBurgos-Mansilla, Barbara, Noelia Galiano-Castillo, Mario Lozano-Lozano, Carolina Fernández-Lao, Maria Lopez-Garzon, and Manuel Arroyo-Morales. 2021. "Effect of Physical Therapy Modalities on Quality of Life of Head and Neck Cancer Survivors: A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 10, no. 20: 4696. https://doi.org/10.3390/jcm10204696