
Cumulative Inflammation and HbA1c Levels Correlate with Increased Intima-Media Thickness in Patients with Severe Hidradenitis Suppurativa

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Variables of Interest
2.1.1. Main Variables
- The International HS severity scoring system (IHS4) was used to assess inflammatory activity. It was calculated using the following formula: (number of nodules × 1) + (number of abscesses × 2) + (number of fistulas × 4) [31].
- The Hurley classification was used to assess structural damage. It consists of 3 stages (I, presence of abscesses without fistulous tracts or scars; II, recurrent abscesses and single or multiple fistulae and scars widely separated between them; III, abscesses and confluent fistulas with large areas of extensive scarring) [32].
- Number of body areas affected by HS lesions.
- To assess symptoms, the Numeric Rating System (NRS) was used for pain, itching and suppuration. Values range between 0 and 10 [33].
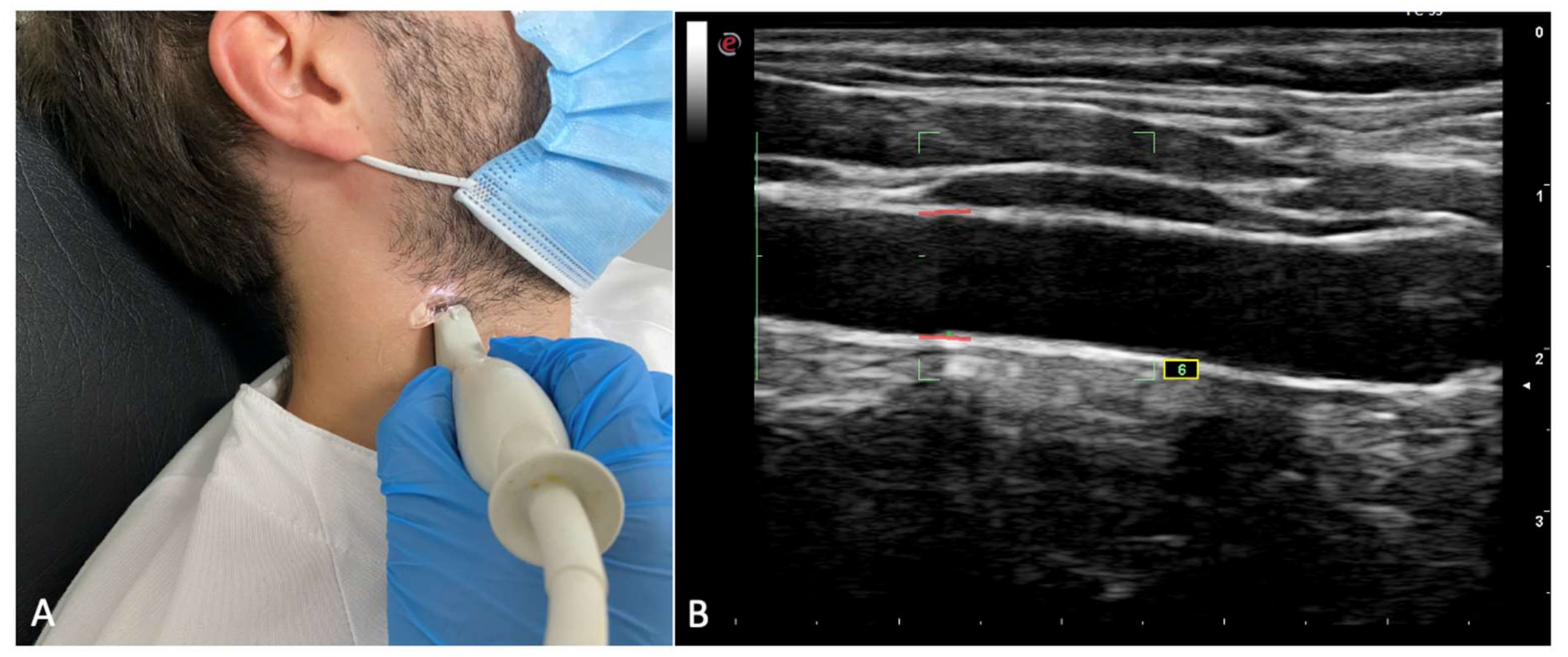
- Carotid intima-media thickness (IMT): IMT was assessed in both carotid arteries of the patients by using ultrasonography. Left, right, and mean IMT was recorded. The procedure was performed as previously described in similar investigations [25]: A complete examination of the left and right common carotid arteries was performed. Patients were in supine position with their necks being 60° laterally inclined. Six IMT measurements were performed, and in all of them, the probe was 10 mm away from the carotid bifurcation. Only those measurements with a standard deviation inferior to 20 μm were taken as valid measures. A high-resolution ultrasound scanner (Esaote MyLab Gold 25) with a 12 mHz sounding line running specific software for measuring ITM (Esaote QIMT Software) was employed. The definitive value of the IMT measurements was obtained by calculating the average of 6 valid measurements taken from the sonographic scanning. Figure 1 shows the IMT assessment.
- Blood biomarkers: Different measurements were performed in patients following an 8 h fasting period. Recorded blood parameters included: basal glucose, basal insulin, HOMA score, glycated hemoglobin, triglycerides, HDL and LDL cholesterol, transaminases, albumin, parathyrin, vitamin D, erythrocyte sedimentation rate (ESR), and C-Reactive Protein (CRP).
- Clinical data: Patients were explored to assess the Body Mass Index (BMI), the metabolic syndrome criteria (ATPIII criteria) [34], and tobacco consumption (cigarettes/day).
2.1.2. Other Variables
2.2. Statistical Analysis
3. Results
3.1. Socio-Demographic and Clinical Features of the Sample
3.2. Distribution of Cardiovascular Risk Markers in the Sample
3.3. Glycemic Disorders
3.4. Vitamin D
3.5. Intima-Media Thickness and Potential Associated Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Forouzanfar, M.H.; Moran, A.E.; Barber, R.; Nguyen, G.; Feigin, V.L.; Naghavi, M.; Mensah, G.A.; Murray, C.J. Demographic and Epidemiologic Drivers of Global Cardiovascular Mortality. N. Engl. J. Med. 2015, 372, 1333–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- North, B.J.; Sinclair, D.A. The Intersection between Aging and Cardiovascular Disease. Circ. Res. 2012, 110, 1097–1108. [Google Scholar] [CrossRef]
- Koliaki, C.; Liatis, S.; Kokkinos, A. Obesity and cardiovascular disease: Revisiting an old relationship. Metabolism 2019, 92, 98–107. [Google Scholar] [CrossRef]
- Badimon, L.; Chagas, P.; Chiva-Blanch, G. Diet and Cardiovascular Disease: Effects of Foods and Nutrients in Classical and Emerging Cardiovascular Risk Factors. Curr. Med. Chem. 2019, 26, 3639–3651. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.-W.; Kim, S.-H.; Kang, S.-H.; Kim, H.-J.; Yoon, C.-H.; Youn, T.-J.; Chae, I.-H. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur. Heart J. 2019, 40, 3547–3555. [Google Scholar] [CrossRef]
- Selvin, E.; Marinopoulos, S.; Berkenblit, G.; Rami, T.; Brancati, F.L.; Powe, N.R.; Golden, S.H. Meta-Analysis: Glycosylated Hemoglobin and Cardiovascular Disease in Diabetes Mellitus. Ann. Intern. Med. 2004, 141, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Zhao, D.; Wang, M.; Zhao, F.; Han, X.; Qi, Y.; Liu, J. Association Between Circulating Oxidized LDL and Atherosclerotic Cardiovascular Disease: A Meta-analysis of Observational Studies. Can. J. Cardiol. 2017, 33, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Nitsa, A.; Toutouza, M.; Machairas, N.; Mariolis, A.; Philippou, A.; Koutsilieris, M. Vitamin D in Cardiovascular Disease. Circ. Res. 2018, 32, 977–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ferranti, S.D.; Rifai, N. C-reactive protein: A nontraditional serum marker of cardiovascular risk. Cardiovasc. Pathol. Off. J. Soc. Cardiovasc. Pathol. 2007, 16, 14–21. [Google Scholar] [CrossRef]
- Frostegård, J. Immunity, atherosclerosis and cardiovascular disease. BMC Med. 2013, 11, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golia, E.; Limongelli, G.; Natale, F.; Fimiani, F.; Maddaloni, V.; Pariggiano, I.; Bianchi, R.; Crisci, M.; D’Acierno, L.; Giordano, R.; et al. Inflammation and Cardiovascular Disease: From Pathogenesis to Therapeutic Target. Curr. Atheroscler. Rep. 2014, 16, 435. [Google Scholar] [CrossRef]
- Ergun, T. Hidradenitis suppurativa and the metabolic syndrome. Clin. Dermatol. 2018, 36, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Bui, T.-L.; Silva-Hirschberg, C.; Torres, J.; Armstrong, A.W. Hidradenitis suppurativa and diabetes mellitus: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2018, 78, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Charlton, O.; Smith, S.D. Hidradenitis suppurativa and diabetes mellitus: Updated systematic review and adjusted meta-analysis. Clin. Exp. Dermatol. 2019, 44, e126–e132. [Google Scholar] [CrossRef] [PubMed]
- Glovaci, D.; Fan, W.; Wong, N.D. Epidemiology of Diabetes Mellitus and Cardiovascular Disease. Curr. Cardiol. Rep. 2019, 21, 21. [Google Scholar] [CrossRef]
- Choi, F.; Lehmer, L.; Ekelem, C.; Mesinkovska, N.A. Dietary and metabolic factors in the pathogenesis of hidradenitis suppurativa: A systematic review. Int. J. Dermatol. 2019, 59, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Brandao, L.; Moura, R.; Tricarico, P.M.; Gratton, R.; Genovese, G.; Moltrasio, C.; Garcovich, S.; Boniotto, M.; Crovella, S.; Marzano, A.V. Altered keratinization and vitamin D metabolism may be key pathogenetic pathways in syndromic hidradenitis suppurativa: A novel whole exome sequencing approach. J. Dermatol. Sci. 2020, 99, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Al-Bayyari, N.; Hailat, R.; Subih, H.; AlKhalidy, H.; Eaton, A. Vitamin D3 reduces risk of cardiovascular and liver diseases by lowering homocysteine levels: Double-blinded, randomised, placebo-controlled trial. Br. J. Nutr. 2021, 125, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Trummer, C.; Theiler-Schwetz, V.; Lerchbaum, E.; März, W.; Pilz, S. Vitamin D and Cardiovascular Disease: An Updated Narrative Review. Int. J. Mol. Sci. 2021, 22, 2896. [Google Scholar] [CrossRef] [PubMed]
- Orgaz-Molina, J.; Magro-Checa, C.; Rosales-Alexander, J.L.; Arrabal-Polo, M.A.; Castellote-Caballero, L.; Buendía-Eisman, A.; Raya-Álvarez, E.; Arias-Santiago, S. Vitamin D insufficiency is associated with higher carotid intima-media thickness in psoriatic patients. Eur. J. Dermatol. 2014, 24, 53–62. [Google Scholar] [CrossRef]
- Kostopoulou, M.; Nikolopoulos, D.; Parodis, I.; Bertsias, G. Cardiovascular Disease in Systemic Lupus Erythematosus: Recent data on epidemiology, risk factors and prevention. Curr. Vasc. Pharmacol. 2020, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Cainzos-Achirica, M.; Glassner, K.; Zawahir, H.S.; Dey, A.K.; Agrawal, T.; Quigley, E.M.; Abraham, B.P.; Acquah, I.; Yahya, T.; Mehta, N.N.; et al. Inflammatory Bowel Disease and Atherosclerotic Cardiovascular Disease. J. Am. Coll. Cardiol. 2020, 76, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- England, B.R.; Thiele, G.M.; Anderson, D.R.; Mikuls, T.R. Increased cardiovascular risk in rheumatoid arthritis: Mechanisms and implications. BMJ 2018, 361, k1036. [Google Scholar] [CrossRef]
- Masson, W.; Lobo, M.; Molinero, G. Psoriasis and Cardiovascular Risk: A Comprehensive Review. Adv. Ther. 2020, 37, 2017–2033. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Lopez, A.; Blasco-Morente, G.; Perez-Lopez, I.; Tercedor-Sanchez, J.; Arias-Santiago, S. Studying the effect of systemic and biological drugs on intima-media thickness in patients suffering from moderate and severe psoriasis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Arias-Santiago, S.; Orgaz-Molina, J.; Castellote-Caballero, L.; Arrabal-Polo, M.Á.; García-Rodriguez, S.; Perandrés-López, R.; Ruiz, J.C.; Naranjo-Sintes, R.; Zubiaur, M.; Sancho, J.; et al. Atheroma plaque, metabolic syndrome and inflammation in patients with psoriasis. Eur. J. Dermatol. 2012, 22, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzellos, T.; Zouboulis, C.P.D.; Gulliver, W.; Cohen, A.; Wolkenstein, P.; Jemec, G. Cardiovascular disease risk factors in patients with hidradenitis suppurativa: A systematic review and meta-analysis of observational studies. Br. J. Dermatol. 2015, 173, 1142–1155. [Google Scholar] [CrossRef]
- Hung, C.; Chiang, C.; Tsao, C.; Chien, W.; Wang, W. Increased risk of cardiovascular comorbidities in hidradenitis suppurativa: A nationwide, population-based, cohort study in Taiwan. J. Dermatol. 2019, 46, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Emtestam, L.; Desai, N.; Hunger, R.; Zouboulis, C.C.; Ioannides, D.; Van Der Zee, H.H.; Prens, E.P.; Jemec, G.B.E.; Schneider-Burrus, S.; Revuz, J.; et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 619–644. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Tzellos, T.; Kyrgidis, A.; Jemec, G.B.E.; Bechara, F.G.; Giamarellos-Bourboulis, E.J.; Ingram, J.R.; Kanni, T.; Karagiannidis, I.; Martorell, A.; et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS 4), a novel dynamic scoring system to assess HS severity. Br. J. Dermatol. 2017, 177, 1401–1409. [Google Scholar] [CrossRef] [Green Version]
- Ovadja, Z.; Schuit, M.; van der Horst, C.; Lapid, O. Inter- and intrarater reliability of Hurley staging for hidradenitis suppurativa. Br. J. Dermatol. 2019, 181, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zouboulis, C.P.D.; Del Marmol, V.; Mrowietz, U.U.; Prens, E.; Tzellos, T.T.; Jemec, G. Hidradenitis Suppurativa/Acne Inversa: Criteria for Diagnosis, Severity Assessment, Classification and Disease Evaluation. Dermatology 2015, 231, 184–190. [Google Scholar] [CrossRef]
- Marchesini, G.; Forlani, G.; Cerrelli, F.; Manini, R.; Natale, S.; Baraldi, L.; Ermini, G.; Savorani, G.; Zocchi, D.; Melchionda, N. WHO and ATPIII proposals for the definition of the metabolic syndrome in patients with Type 2 diabetes. Diabet. Med. 2004, 21, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, T.Z.; Lee, M.-S. Carotid Intima-Media Thickness and Plaque in Cardiovascular Risk Assessment. JACC Cardiovasc. Imaging 2014, 7, 1025–1038. [Google Scholar] [CrossRef] [Green Version]
- Sillesen, H.; Sartori, S.; Sandholt, B.; Baber, U.; Mehran, R.; Fuster, V. Carotid plaque thickness and carotid plaque burden predict future cardiovascular events in asymptomatic adult Americans. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Cho, G.-Y.; Kim, H.-S.; Yoon, Y.E.; Lee, S.-P.; Kim, H.-K.; Kim, Y.-J.; Sohn, D.-W. Common carotid intima-media thickness as a risk factor for outcomes in Asian patients with acute ST-elevation myocardial infarction. Can. J. Cardiol. 2014, 30, 1620–1626. [Google Scholar] [CrossRef] [PubMed]
- Pinto, M.R.C.; Kakehasi, A.M.; Souza, A.J.; Tavares, W.C.; Rocha, M.A.; Trant, C.G.M.C.; Andrade, M.V. Methotrexate use, not interleukin 33, is associated with lower carotid intima-media thickness in patients with rheumatoid arthritis. Adv. Rheumatol. 2019, 59, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezaieyazdi, Z.; Sedighi, S.; Salari, M.; Fard, M.H.; Azarpazhooh, M.; Tabrizi, P.S.; Afshari, J.T.; Saghafi, M. Investigation of the Association Between Carotid Artery Intima-Media Thickness (IMT) and Cardiac Risk Factors in Patients with Systemic Lupus Erythematosus. Curr. Rheumatol. Rev. 2020, 16, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Santoliquido, A.; Danese, S.; Covino, M.; Di Campli, C.; Urgesi, R.; Grillo, A.; Guglielmo, S.; Tondi, P.; Guidi, L.; et al. Increased carotid intima-media thickness in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2005, 22, 839–846. [Google Scholar] [CrossRef]
- Kallio, K.; Jokinen, E.; Saarinen, M.; Hämäläinen, M.; Volanen, I.; Kaitosaari, T.; Rönnemaa, T.; Viikari, J.; Raitakari, O.T.; Simell, O. Arterial intima-media thickness, endothelial function, and apolipoproteins in adolescents frequently exposed to tobacco smoke. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 196–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Sui, J.; Wang, S.; Wang, X. Correlations of carotid intima-media thickness with endothelial function and atherosclerosis degree in patients with type 2 diabetes mellitus. Clin. Hemorheol. Microcirc. 2019, 72, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Im, C.H.; Kim, N.R.; Kang, J.W.; Kim, J.H.; Bae, G.B.; Nam, E.J.; Kang, Y.M. Inflammatory burden interacts with conventional cardiovascular risk factors for carotid plaque formation in rheumatoid arthritis. Rheumatology 2014, 54, 808–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smrzova, A.; Horák, P.; Skacelova, M.; Heřmanová, Z.; Langova, K.; Zadrazil, J.; Novotny, D. Intima media thickness measurement as a marker of subclinical atherosclerosis in SLE patient. Biomed. Pap. 2014, 158, 404–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-López, M.A.; Hernández, J.L.; Lacalle, M.; Mata, C.; López-Escobar, M.; López-Mejías, R.; Portilla, V.; Fuentevilla, P.; Corrales, A.; González-Vela, M.C.; et al. Increased prevalence of subclinical atherosclerosis in patients with hidradenitis suppurativa (HS). J. Am. Acad. Dermatol. 2016, 75, 329–335. [Google Scholar] [CrossRef]
- Plasencia-Martínez, J.M.; García-Santos, J.M.; Lozano-Herrero, J.; Hernández-Vidal, M.J. Carotid Intima-Media Thickness Manual Measurements: Intraoperator and Interoperator Agreements under A Strict Protocol in a Large Sample. Ultrasound Q. 2017, 33, 28–36. [Google Scholar] [CrossRef]
- Jarauta, E.; Mateo-Gallego, R.; Bea, A.; Burillo, E.; Calmarza, P.; Civeira, F. Carotid Intima-Media Thickness in Subjects with No Cardiovascular Risk Factors. Rev. Española Cardiol. 2010, 63, 97–102. [Google Scholar] [CrossRef]
- Cecelja, M.; Sriswan, R.; Kulkarni, B.; Kinra, S.; Nitsch, D. Association of pulse wave velocity and intima-media thickness with cardiovascular risk factors in young adults. J. Clin. Hypertens. 2020, 22, 174–184. [Google Scholar] [CrossRef]
- Podolec, M.; Siniarski, A.; Pająk, A.; Rostoff, P.; Gajos, G.; Nessler, J.; Olszowska, M.; Nowakowski, M.; Szafraniec, K.; Kopeć, G. Association between carotid-femoral pulse wave velocity and overall cardiovascular risk score assessed by the SCORE system in urban Polish population. Kardiol. Pol. 2019, 77, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Tripepi, G.; Agharazii, M.; Pannier, B.; D’Arrigo, G.; Mallamaci, F.; Zoccali, C.; London, G. Pulse Wave Velocity and Prognosis in End-Stage Kidney Disease. Hypertension 2018, 71, 1126–1132. [Google Scholar] [CrossRef]
- Sarafidis, P.A.; Loutradis, C.; Karpetas, A.; Tzanis, G.; Piperidou, A.; Koutroumpas, G.; Raptis, V.; Syrgkanis, C.; Liakopoulos, V.; Efstratiadis, G.; et al. Ambulatory Pulse Wave Velocity Is a Stronger Predictor of Cardiovascular Events and All-Cause Mortality Than Office and Ambulatory Blood Pressure in Hemodialysis Patients. Hypertension 2017, 70, 148–157. [Google Scholar] [CrossRef]
- Khaw, K.-T.; Wareham, N. Glycated hemoglobin as a marker of cardiovascular risk. Curr. Opin. Lipidol. 2006, 17, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhao, Y.; Chai, J.; Hao, D. The correlation between the Glycated hemoglobin (HbA1c) in non-diabetics and cardiovascular risk factors. Pak. J. Pharm. Sci. 2016, 29, 315–319. [Google Scholar] [PubMed]
- Vilanova, I.; Hernández, J.; Mata, C.; Durán, C.; García-Unzueta, M.; Portilla, V.; Fuentevilla, P.; Corrales, A.; González-Vela, M.; González-Gay, M.; et al. Insulin resistance in hidradenitis suppurativa: A case-control study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 820–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saisho, Y. Metformin and Inflammation: Its Potential Beyond Glucose-lowering Effect. Endocr. Metab. Immune Disord.-Drug Targets 2015, 15, 196–205. [Google Scholar] [CrossRef]
- Jennings, L.; Hambly, R.; Hughes, R.; Moriarty, B.; Kirby, B. Metformin use in hidradenitis suppurativa. J. Dermatol. Treat. 2020, 31, 261–263. [Google Scholar] [CrossRef]
- Garbossa, S.G.; Folli, F. Vitamin D, sub-inflammation and insulin resistance. A window on a potential role for the interaction between bone and glucose metabolism. Rev. Endocr. Metab. Disord. 2017, 18, 243–258. [Google Scholar] [CrossRef]
- Gonçalves de Carvalho, C.M.R.; Ribeiro, S.M.L. Aging, low-grade systemic inflammation and vitamin D: A mini-review. Eur. J. Clin. Nutr. 2017, 71, 434–440. [Google Scholar] [CrossRef]
- Gubatan, J.; Moss, A.C. Vitamin D in inflammatory bowel disease: More than just a supplement. Curr. Opin. Gastroenterol. 2018, 34, 217–225. [Google Scholar] [CrossRef]
- Dall’Ara, F.; Cutolo, M.; Andreoli, L.; Tincani, A.; Paolino, S. Vitamin D and systemic lupus erythematous: A review of immunological and clinical aspects. Clin. Exp. Rheumatol. 2017, 36, 153–162. [Google Scholar]
- Fabbrocini, G.; Marasca, C.; Luciano, M.A.; Guarino, M.; Poggi, S.; Fontanella, G.; Cacciapuoti, S. Vitamin D deficiency and hidradenitis suppurativa: The impact on clinical severity and therapeutic responsivity. J. Dermatol. Treat. 2021, 32, 843–844. [Google Scholar] [CrossRef]
- Ponikowska, M.; Matusiak, L.; Kasztura, M.; Jankowska, E.A.; Szepietowski, J.C. Deranged Iron Status Evidenced by Iron Deficiency Characterizes Patients with Hidradenitis Suppurativa. Dermatology 2020, 236, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Fang, M.; Cheng, R.; Zhang, Z.; Wang, Y.; Shen, C.; Han, Y.; Lu, Q.; Du, Y.; Liu, Y.; et al. Iron-Deficiency and Estrogen Are Associated With Ischemic Stroke by Up-Regulating Transferrin to Induce Hypercoagulability. Circ. Res. 2020, 127, 651–663. [Google Scholar] [CrossRef] [PubMed]
- Matusiak, Ł.; Batycka-Baran, A.; Bieniek, A.; Szepietowski, J.C. Decreased number of circulating endothelial progenitor cells in hidradenitis suppurativa patients. Dermatology 2015, 230, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Elnabawi, Y.A.; Dey, A.K.; Goyal, A.; Groenendyk, J.W.; Chung, J.H.; Belur, A.D.; Rodante, J.; Harrington, C.L.; Teague, H.L.; Baumer, Y.; et al. Coronary artery plaque characteristics and treatment with biologic therapy in severe psoriasis: Results from a prospective observational study. Cardiovasc. Res. 2019, 115, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Caiazzo, G.; Fabbrocini, G.; Di Caprio, R.; Raimondo, A.; Scala, E.; Balato, N.; Balato, A. Psoriasis, Cardiovascular Events, and Biologics: Lights and Shadows. Front. Immunol. 2018, 9, 1668. [Google Scholar] [CrossRef] [Green Version]
- Ntusi, N.A.; Francis, J.M.; Sever, E.; Liu, A.; Piechnik, S.K.; Ferreira, V.M.; Matthews, P.M.; Robson, M.D.; Wordsworth, P.B.; Neubauer, S.; et al. Anti-TNF modulation reduces myocardial inflammation and improves cardiovascular function in systemic rheumatic diseases. Int. J. Cardiol. 2018, 270, 253–259. [Google Scholar] [CrossRef]
- Ait-Oufella, H.; Libby, P.; Tedgui, A. Anticytokine Immune Therapy and Atherothrombotic Cardiovascular Risk. Arter. Thromb. Vasc. Biol. 2019, 39, 1510–1519. [Google Scholar] [CrossRef]
- Van den Oever, I.A.M.; Baniaamam, M.; Simsek, S.; Raterman, H.G.; van Denderen, J.C.; van Eijk, I.C.; Peters, M.J.L.; van der Horst-Bruinsma, I.E.; Smulders, Y.M.; Nurmohamed, M.T. The effect of anti-TNF treatment on body composition and insulin resistance in patients with rheumatoid arthritis. Rheumatol. Int. 2021, 41, 319–328. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables All Patients (n = 50) | |||
|---|---|---|---|
| Age (years) | 38 (SD 18.85) | Pilonidal sinus (%) | 38% (19/50) |
| Age of onset (years) | 21.83 (SD 9.81) | Number or areas affected | 4.53 (SD 2.06) |
| Disease duration (years) | 16.6 (SD 13.54) | NRS pain | 6.84 (SD 3.10) |
| Family history of HS (%) | 44% (22/50) | NRS pruritus | 5.84 (SD 3.23) |
| Previous biologic treatment (%) | 22% (11/50) | NRS malodor | 6.36 (SD 3.31) |
| Previous surgical interventions for HS (%) | 34% (17/50) | NRS suppuration | 6.62 (SD 3.02) |
| Dissecting cellulitis of the scalp (%) | 10% (5/50) | General NRS | 6.68 (SD 2.69) |
| Acne conglobate (%) | 36% (18/50) | IHS4 index | 21.6 (SD 12.59) |
| Hurley Stage (%) | I: 8% (4/50) | II: 36% (18/50) | III: 56% (28/50) |
| Cardiovascular Risk Markers All Patients (n = 50) | |||
|---|---|---|---|
| Diabetes mellitus (%) | 10% (5/50) | Dyslipidemia (%) | 10% (5/50) |
| Basal glycemia (mg/dL) | 90.5 (SD 15.71) | Triglycerides (mg/dL) | 130.13 (SD 62.72) |
| Basal insulin (microU/mL) | 15.17 (SD 23.43) | HDL (mg/dL) | 51.71 (SD 17.87) |
| HOMA index | 3.79 (SD 7.74) | High blood pressure (%) | 18% (9/50) |
| HbA1c (%) | 5.57 (SD 0.73) | Systolic blood pressure (mmHg) | 129.08 (SD 7.75) |
| Tobacco (cig/day) | 4.84 (SD 8.15) | Diastolic blood pressure (mmHg) | 83.44 (SD 6.81) |
| Obesity (%) | 42% (21/50) | Metabolic syndrome (%) | 26% (13/50) |
| Body Mass Index (kg/m2) | 30.36 (SD 7.45) | Vitamin D (ng/mL) | 19.80 (SD 7.08) |
| Abdominal circumference (cm) | 98.18 (SD 16.26) | Intima-media thickness (μm) | 651.30 (SD 130.90) |
| Factors | HbA1c | Vitamin D | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| Difference/β | p Value | β | p Value | Difference/β | p Value | β | p Value | |
| Sex | Male: 5.49 (SE 0.09) | 0.95 | - | - | Male: 19.76 (SE 1.34) | 0.99 | - | - |
| Female: 5.49 (SE 0.12) | Female: 19.78 (SE 1.62) | |||||||
| Age | 0.006 (SE 0.008) | 0.35 | - | - | −0.13 (SE 0.08) | 0.09 | −0.08 (SE 0.07) | 0.26 |
| Age of onset | 0.01(SE 0.007) | 0.16 | 0.011 (SE 0.006) | 0.046 | 0.047 (SE 0.11) | 0.66 | - | - |
| Duration of disease | −0.002 (SE 0.005) | 0.75 | - | - | −0.13 (SE 0.07) | 0.09 | - | - |
| Family history | Yes: 5.52 (SE 0.11) | 0.65 | - | - | Yes: 20.48 (SE 1.39) | 0.54 | - | - |
| No: 5.47 (SE 0.10) | No: 19.19 (SE 1.39) | |||||||
| Previous biologic treatments | Yes: 5.33 (SE 0.16) | 0.24 | - | - | Yes: 18.39 (SE 2.28) | 0.28 | - | - |
| No: 5.54 (SE 0.09) | No: 20.12 (Se 1.15) | |||||||
| Previous surgical interventions for HS | Yes: 5.43 (SE 0.13) | 0.54 | - | - | Yes: 19.13 (SE 1.75) | 0.68 | - | - |
| No: 5.53 (SE 0.09) | No: 20.11 (SE 1.27) | |||||||
| High blood pressure | Yes: 5.18 (SE 0.18) | 0.053 | 0.21 (SE 0.07) | 0.006 | Yes: 18.97 (SE 2.40) | 0.42 | - | - |
| No: 5.57 (SE 0.08) | No: 19.98 (SE 1.15) | |||||||
| Tobacco | 0.01 (SE 0.009) | 0.29 | - | - | 0.10 (SE 0.16) | 0.50 | - | - |
| Body mass index | 0.02 (SE 0.009) | 0.04 | 0.007 (SE 0.008) | 0.42 | −0.042 (SE 0.14) | 0.76 | - | - |
| Metabolic syndrome | Yes: 5.87 (SE 0.13) | 0.002 | 0.15 (SE 0.07) | 0.03 | 1.72 | 0.43 | - | - |
| No: 5.36 (SE 0.08) | ||||||||
| Number of areas affected | 0.008 (SE 0.04) | 0.82 | - | - | −1.57 (SE 0.49) | 0.002 | −1.17 (SE 0.57) | 0.047 |
| IHS4 index | 0.007 (SE 0.006) | 0.27 | - | - | −0.24 (SE 0.09) | 0.014 | −0.0005 (SE 0.12) | 0.99 |
| Hurley | I: 5.31 (SE 0.27) | 0.75 | - | - | I: 26.81 (SE 3.28) | 0.067 | 2.95 (SE 2.34) | 0.21 |
| II: 5.48 (SE 0.3) | II: 22.12 (SE1.55) | |||||||
| III: 5.53 (SE 0.1) | III: 17.16 (SE 1.26) | 0.60 (SE 1.52) | 0.69 | |||||
| Basal glucose | 0.02 (SE 0.003) | <0.001 | 0.017 (SE 0.004) | <0.0001 | −0.08 (SE 0.06) | 0.25 | - | - |
| Basal Insulin | 0.0005 (SE 0.003) | 0.88 | - | - | −0.027 (SE 0.04) | 0.54 | - | - |
| HOMA index | 0.002 (SE 0.009) | 0.82 | - | - | −0.088 (SE 0.13) | 0.50 | - | - |
| HbA1c | 1 | <0.001 | - | - | −1.20 (SE 1.40) | 0.39 | - | - |
| Triglycerides | 0.002 (SE 0.001) | 0.068 | - | - | 0.012 (SE 0.01) | 0.47 | - | - |
| LDL cholesterol | 0.003 (SE 0.002) | 0.12 | - | - | −0.009 (SE 0.03) | 0.74 | - | - |
| Parathyrin | −0.002 (SE 0.003) | 0.57 | - | - | −0.056 (SE 0.04) | 0.17 | - | - |
| Vitamin D | −0.003 (SE 0.01) | 0.79 | - | - | 1 | <0.001 | - | - |
| ESR | −0.009 (SE 0.004) | 0.83 | - | - | −0.042 (SE 0.05) | 0.44 | - | - |
| CRP | −0.00002 (SE 0.003) | 0.99 | - | - | −0.016 (SE 0.04) | 0.73 | - | - |
| Ferritin | 0.001 (SE 0.009) | 0.22 | - | - | −0.0005 (SE 0.01) | 0.97 | - | - |
| R2 | - | 0.5848 | - | 0.2968 | ||||
| Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Difference/β | p Value | β Coefficient | p Value | |
| Sex | Male: 659 (SD 23.9) | 0.77 | - | - |
| Female 648 (SD 30) | ||||
| Age | 5.64 (SE 1.21) | <0.001 | - | - |
| Age of onset | 4.96 (SE 1.80) | <0.01 | - | - |
| Duration of disease | 3.53 (SE 1.30) | <0.01 | 3.61 (SE 1.51) | 0.02 |
| Family history | Yes: 626.57 (SD 27.34) | 0.17 | - | - |
| No: 678.37 (SD 24.68) | ||||
| Previous biologic treatments | Yes: 663.59 (SD 39.45) | 0.84 | - | - |
| No: 652.66 (SD 21.22) | ||||
| Previous surgical interventions for HS | Yes: 673.29 (SD 31.58) | 0.48 | - | - |
| No: 645.45 (SD 32.02) | ||||
| High blood pressure | Yes: 699.06 (SD 40.93) | 0.17 | - | - |
| No: 637.60 (SD 19.67) | ||||
| Tobacco | 4.86 (SE 2.62) | 0.07 | 5.52 (SE 2.49) | 0.03 |
| Body mass index | 2.12 (SE 2.50) | 0.40 | - | - |
| Metabolic syndrome | Yes: 659.85 (SD 36.3) | 0.89 | - | - |
| No: 653.40 (SD 21.8) | ||||
| Number of areas affected | 4.08 (SE 9.37) | 0.67 | - | - |
| IHS4 index | 0.36 (SE 1.49) | 0.81 | - | - |
| Hurley | I: 606.87 (SE 65.29) | 0.53 | - | - |
| II: 678.49 (SE 30.78) | ||||
| III: 646.53 (SE 25.13) | ||||
| Basal glucose | 1.14 (SE 1.19) | 0.34 | - | - |
| Basal insulin | −1.58 (SE 0.76) | 0.04 | −0.70 (SE 6.92) | 0.92 |
| HOMA index | −4.20 (SE 2.32) | 0.07 | −0.41 (SE 20.51) | 0.98 |
| HbA1c | 62.60 (SE 23.9) | 0.01 | 64.76 (SE 24.62) | 0.01 |
| Triglycerides | 0.14 (SE 0.30) | 0.63 | - | - |
| LDL cholesterol | −0.88 (SE 0.53) | 0.10 | - | - |
| Parathyrin | 0.95 (SE 0.73) | 0.20 | - | - |
| Vitamin D | −2.59 (SE 2.63) | 0.33 | - | - |
| ESR | −0.91 (SE 0.98) | 0.20 | - | - |
| CRP | −1.33 (SE 0.80) | 0.10 | - | - |
| Ferritin | 0.39 (SE 0.24) | 0.11 | - | - |
| R2 | - | - | 0.4230 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Díaz, M.; Salvador-Rodríguez, L.; Montero-Vílchez, T.; Martínez-López, A.; Arias-Santiago, S.; Molina-Leyva, A. Cumulative Inflammation and HbA1c Levels Correlate with Increased Intima-Media Thickness in Patients with Severe Hidradenitis Suppurativa. J. Clin. Med. 2021, 10, 5222. https://doi.org/10.3390/jcm10225222
Sánchez-Díaz M, Salvador-Rodríguez L, Montero-Vílchez T, Martínez-López A, Arias-Santiago S, Molina-Leyva A. Cumulative Inflammation and HbA1c Levels Correlate with Increased Intima-Media Thickness in Patients with Severe Hidradenitis Suppurativa. Journal of Clinical Medicine. 2021; 10(22):5222. https://doi.org/10.3390/jcm10225222
Chicago/Turabian StyleSánchez-Díaz, Manuel, Luis Salvador-Rodríguez, Trinidad Montero-Vílchez, Antonio Martínez-López, Salvador Arias-Santiago, and Alejandro Molina-Leyva. 2021. "Cumulative Inflammation and HbA1c Levels Correlate with Increased Intima-Media Thickness in Patients with Severe Hidradenitis Suppurativa" Journal of Clinical Medicine 10, no. 22: 5222. https://doi.org/10.3390/jcm10225222