
Platelet-Derived Drug Targets and Biomarkers of Ischemic Stroke—The First Dynamic Human LC-MS Proteomic Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
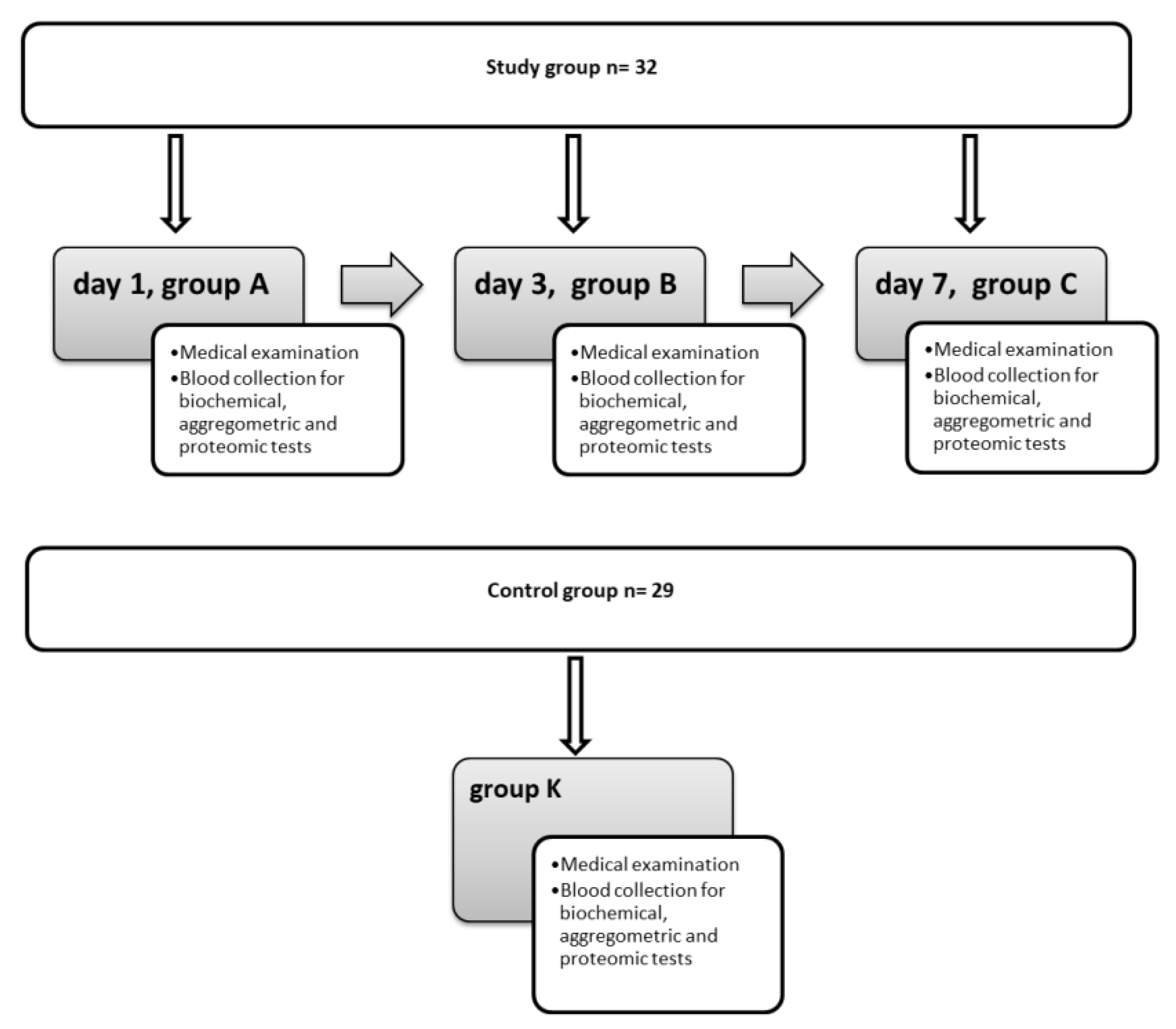
2.2. Study Design
2.3. Platelet Preparation
2.4. LC-MS Proteomic Analysis
2.5. Statistical Analysis
2.6. Bioethics Statement
3. Results
3.1. Demographic, Clinical, and Biochemical Characteristics of the Investigated Population
3.2. Proteomic Analysis
- Beta-amyloid A4 protein and amyloid-like protein 2;
- Coactosin-like protein;
- Thymidine phosphorylase TYMP-4;
- Interferon regulatory factor 7;
- Vitamin K-dependent protein S;
- Histone proteins (H2A type 1, H2A type 1-A, H2A type 2B, H2A J, and H2Av, -z, -x);
- Platelet basic protein.
- Filamin A, filamin B, filamin C (group A vs. group B, following the first two days from the onset of the stroke)
- Thrombospondin-1, thrombospondin-2 (group A vs. group C, following one week from the onset of symptoms).
4. Discussion
4.1. Demographic and Clinical Characteristics
4.2. Proteomic Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics-2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e39. [Google Scholar] [CrossRef] [Green Version]
- Qiu, R.; Gao, Y.; Hou, D.; Wang, Y.; Yu, C.; Wang, W.; Liu, S.; Gao, C.; Tong, X.; Wu, J. Association between hs-CRP levels and the outcomes of patients with small-artery occlusion. Front. Aging Neurosci. 2016, 8, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strimbu, K.; Tavel, J.A. What are biomarkers? Curr. Opin. HIV AIDS 2010, 5, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Mischak, H.; Allmaier, G.; Apweiler, R. Recommendations for Biomarker Identification and Qualification in Clinical Proteomics. Sci. Transl. Med. 2010, 2, 46ps42. [Google Scholar] [CrossRef] [Green Version]
- Rist, P.M.; Buring, J.E.; Kase, C.S.; Ridker, P.M.; Kurth, T. Biomarkers and functional outcomes from ischaemic cerebral events in women: A prospective cohort study. Eur. J. Neurol. 2013, 20, 375–381. [Google Scholar] [CrossRef] [Green Version]
- Del Zoppo, G.J. The role of platelets in ischemic stroke. Neurology 1998, 51 (Suppl. 3), S9–S14. [Google Scholar] [CrossRef]
- Maynard, D.M.; Heijnen, H.F.G.; Horne, M.K.; White, J.G.; Gahl, W.A. Proteomic analysis of platelet α-granules using mass spectrometry. J. Thromb. Haemost. 2007, 5, 1945–1955. [Google Scholar] [CrossRef]
- Pennington, S.R.; Wilkins, M.R.; Hochstrasser, D.F.; Dunn, M.J. Proteome analysis: From protein characterization to biological function. Trends Cell Biol. 1997, 7, 168–173. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke A. Stroke 2019, 50, E344–E418. [Google Scholar] [CrossRef]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Rev. Esp. Cardiol. 2017, 70, 115. [Google Scholar] [CrossRef] [PubMed]
- Mikula, M.; Gaj, P.; Dzwonek, K.; Rubel, T.; Karczmarski, J.; Paziewska, A.; Dzwonek, A.; Bragoszewski, P.; Dadlez, M.; Ostrowski, J. Comprehensive Analysis of the Palindromic Motif TCTCGCGAGA: A Regulatory Element of the HNRNPK Promoter. DNA Res. 2010, 17, 245–260. [Google Scholar] [CrossRef] [Green Version]
- Malinowska, A.; Kistowski, M.; Bakun, M.; Rubel, T.; Tkaczyk, M.; Mierzejewska, J.; Dadlez, M. Diffprot—software for non-parametric statistical analysis of differential proteomics data. J. Proteom. 2012, 7, 4062–4073. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Baumgartner, C.; den Elzen, W.P. Thyroid Function Within the Reference Range and the Risk of Stroke: An Individual Participant Data Analysis. J. Clin. Endocrinol. Metab. 2016, 101, 4270–4282. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Baumgartner, C.; den Elzen, W.P. Subclinical Hypothyroidism and the Risk of Stroke Events and Fatal Stroke: An Individual Participant Data Analysis. J. Clin. Endocrinol. Metab. 2015, 100, 2181–2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhoundi, F.H.; Ghorbani, A.; Soltani, A. Favorable functional outcomes in acute ischemic stroke patients with subclinical hypothyroidism. Neurology 2011, 77, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Alevizaki, M.; Synetou, M.; Xynos, K. Hypothyroidism as a protective factor in acute stroke patients. Clin. Endocrinol. 2006, 65, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Coppinger, J.A.; Cagney, G.; Toomey, S.; Kislinger, T.; Belton, O.; McRedmond, J.P.; Cahill, D.J.; Emili, A.; Fitzgerald, D.J.; Maguire, P.B. Characterization of the proteins released from activated platelets leads to localization of novel platelet proteins in human atherosclerotic lesions. Blood 2004, 103, 2096–2104. [Google Scholar] [CrossRef] [Green Version]
- Blair, P.; Flaumenhaft, R. Platelet alpha-granules: Basic biology and clinical correlates. Blood Rev. 2009, 23, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Coppinger, J.A.; O’Connor, R.; Wynne, K.; Flanagan, M.; Sullivan, M.; Maguire, P.B.; Fitzgerald, D.J.; Cagney, G. Moderation of the platelet releasate response by aspirin. Blood 2007, 109, 4786–4792. [Google Scholar] [CrossRef]
- Radziwon-Balicka, A.; Moncada de la Rosa, C.; Zielnik, B.; Doroszko, A.; Jurasz, P. Temporal and pharmacological characterization of angiostatin release and generation by human platelets: Implications for endothelial cell migration. PLoS ONE 2013, 8, e59281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevik, O.; Baykal, A.T.; Sener, A. Platelets proteomic profiles of acute ischemic stroke patients. PLoS ONE 2016, 11, e0158287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Evin, G.; Small, D.; Multhaup, G.; Beyreuther, K.; Masters, C.L. Proteolytic processing of Alzheimer’s disease βA4 amyloid precursor protein in human platelets. J. Biol. Chem. 1995, 270, 14140–14147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herczenik, E.; Bouma, B.; Korporaal, S.J.A.; Strangi, R.; Zeng, Q.; Gros, P.; Van Eck, M.; Van Berkel, T.J.C.; Gebbink, M.F.B.G.; Akkerman, J.W.N. Activation of human platelets by misfolded proteins. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.Y.; Hsiao, G.; Fong, T.H.; Chen, H.M.; Chou, D.S.; Lin, C.H.; Sheu, J.R.; Hsu, C.Y. Amyloid beta peptide-activated signal pathways in human platelets. Eur. J. Pharmacol. 2008, 588, 259–266. [Google Scholar] [CrossRef]
- Wakita, H.; Tomimoto, H.; Akiguchi, I.; Ohnishi, K.; Nakamura, S.; Kimura, J. Regional accumulation of amyloid βA4 protein precursor in the gerbil brain following transient cerebral ischemia. Neurosci. Lett. 1992, 146, 135–138. [Google Scholar] [CrossRef]
- Hillen, H. The Beta Amyloid Dysfunction (BAD) Hypothesis for Alzheimer’s Disease. Front. Neurosci. 2019, 13, 1154. [Google Scholar] [CrossRef] [Green Version]
- Müller, U.C.; Deller, T.; Korte, M. Not just amyloid: Physiological functions of the amyloid precursor protein family. Nat. Rev. Neurosci. 2017, 18, 281–298. [Google Scholar] [CrossRef]
- Jevtic, S.; Provias, J. The Amyloid Precursor Protein: More than just Amyloid-Beta. J. Neurol. Exp. Neurosci. 2019, 5, 1–11. [Google Scholar] [CrossRef]
- Scheller, I.; Stritt, S.; Beck, S.; Peng, B.; Pleines, I.; Heinze, K.G.; Braun, A.; Otto, O.; Ahrends, R.; Sickmann, A.; et al. Coactosin-like 1 integrates signaling critical for shear-dependent thrombus formation in mouse platelets. Haematologica 2020, 105, 1667. [Google Scholar] [CrossRef] [Green Version]
- Belcher, A.; Zulfiker, A.H.M.; Li, O.Q.; Yue, H.; Gupta, A.S.; Li, W. Targeting Thymidine Phosphorylase with Tipiracil Hydrochloride Attenuates Thrombosis without Increasing Risk of Bleeding in Mice. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 668–682. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Gigante, A.; Perez-Perez, M.J.; Yue, H.; Hirano, M.; McIntyre, T.M.; Silverstein, R.L. Thymidine phosphorylase participates in platelet signaling and promotes thrombosis. Circ. Res. 2014, 115, 997–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Yue, H. Thymidine phosphorylase: A potential new target for treating cardiovascular disease. Trends Cardiovasc. Med. 2018, 28, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Anrather, J.; Iadecola, C. Inflammation and Stroke: An Overview. Neurotherapeutics 2016, 13, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.L.; Leung, P.Y.; Vartanian, K.B.; Gopalan, B.; Yang, T.; Simon, R.P.; Stenzel-Poore, M.P. Multiple preconditioning paradigms converge on interferon regulatory factor-dependent signaling to promote tolerance to ischemic brain injury. J. Neurosci. 2011, 31, 8456–8463. [Google Scholar] [CrossRef] [Green Version]
- Tahir, F.; Majid, Z.; Bin Arif, T.; Ahmed, J. Cerebral Infarction Followed by Myocardial Infarction in a Young Adult with Protein C and S Deficiency. Cureus 2020, 12, e6665. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, A.; Landi, G.; Vigano’ D’angelo, S.; Orazio, N.; Boccardi, E.; Candelise, L.; Mannucci, P.M. Protein C in acute stroke. Stroke 1988, 19, 579–583. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Guo, H.; Griffin, J.H.; Fernández, J.A.; Zlokovic, B.V. Protein S confers neuronal protection during ischemic/hypoxic injury in mice. Circulation 2003, 107, 1791–1796. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, H.P.; Heeb, M.J.; Wencel-Drake, J.D.; Griffin, J.H. Identification and quantitation of protein S in human platelets. Blood 1985, 66, 1452–1455. [Google Scholar] [CrossRef] [Green Version]
- Rosa, J.P.; Raslova, H.; Bryckaert, M. Filamin A: Key actor in platelet biology. Blood 2019, 134, 1279–1288. [Google Scholar] [CrossRef]
- Berrou, E.; Adam, F.; Lebret, M.; Fergelot, P.; Kauskot, A.; Coupry, I.; Jandrot-Perrus, M.; Nurden, A.; Favier, R.; Rosa, J.P.; et al. Heterogeneity of platelet functional alterations in patients with filamin a mutations. Arterioscler. Thromb. Vasc. Biol. 2013, 33, e11–e18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, J.; Chopp, M.; Zhang, L.; Wang, F.; Liu, Z.; Stroke, L.H. Abstract TP267: Plasminogen Inhances the Process of Angiogenesis After Cerebral Ischemia in Mice via Thrombospondin. Am Hear. Assoc. 2020, 51, ATP267. [Google Scholar] [CrossRef]
- Kawakita, F.; Kanamaru, H.; Asada, R.; Suzuki, H. Potential roles of matricellular proteins in stroke. Exp. Neurol. 2019, 322, 113057. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.C.; Tucker, R.P. The thrombospondin type 1 repeat (TSR) superfamily: Diverse proteins with related roles in neuronal development. Dev. Dyn. 2000, 218, 280–299. [Google Scholar] [CrossRef]
- Lawler, J. The functions of thrombospondin-1 and -2. Curr. Opin. Cell Biol. 2000, 12, 634–640. [Google Scholar] [CrossRef]
- Chamak, B.; Morandi, V.; Mallat, M. Brain macrophages stimulate neurite growth and regeneration by secreting thrombospondin. J. Neurosci. Res. 1994, 38, 221–233. [Google Scholar] [CrossRef]
- Möller, J.C.; Klein, M.A.; Haas, S.; Jones, L.L.; Kreutzberg, G.W.; Raivich, G. Regulation of thrombospondin in the regenerating mouse facial motor nucleus. Glia 1996, 17, 121–132. [Google Scholar] [CrossRef]
- Navarro-Sobrino, M.; Rosell, A.; Hernández-Guillamon, M.; Penalba, A.; Boada, C.; Domingues-Montanari, S.; Ribó, M.; Alvarez-Sabín, J.; Montaner, J. A large screening of angiogenesis biomarkers and their association with neurological outcome after ischemic stroke. Atherosclerosis 2011, 216, 205–211. [Google Scholar] [CrossRef]
- Krupinski, J.; Kaluza, J.; Kumar, P.; Kumar, S.; Wang, J.M. Role of Angiogenesis in Patients with Cerebral Ischemic Stroke. Stroke 1994, 25, 1794–1798. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.B.; Tang, W.D.; Wang, H.X.; Xu, Y. Predictive value of thrombospondin-1 for outcomes in patients with acute ischemic stroke. Clin. Chim. Acta 2015, 450, 176–180. [Google Scholar] [CrossRef]
- Isenberg, J.S.; Romeo, M.J.; Abu-Asab, M.; Tsokos, M.; Oldenborg, A.; Pappan, L.; Wink, D.A.; Frazier, W.A.; Roberts, D.D. Increasing survival of ischemic tissue by targeting CD47. Circ. Res. 2007, 100, 712–720. [Google Scholar] [CrossRef] [Green Version]
- Petryk, N.; Dalby, M.; Wenger, A.; Stromme, C.B.; Strandsby, A.; Andersson, R.; Groth, A. MCM2 promotes symmetric inheritance of modified histones during DNA replication. Science 2018, 361, 1389–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holdenrieder, S.; Stieber, P. Clinical use of circulating nucleosomes. Crit. Rev. Clin. Lab. Sci. 2009, 46, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Shilatifard, A. Epigenetic modifications of histones in cancer. Genome Biol. 2019, 20, 245. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, X.; Pelayo, R.; Monestier, M.; Ammollo, C.T.; Semeraro, F.; Taylor, F.B.; Esmon, N.L.; Lupu, F.; Esmon, C.T. Extracellular histones are major mediators of death in sepsis. Nat. Med. 2009, 15, 1318–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeksema, M.; Van Eijk, M.; Haagsman, H.P.; Hartshorn, K.L. Histones as mediators of host defense, inflammation and thrombosis. Future Microbiol. 2016, 11, 441–453. [Google Scholar] [CrossRef] [Green Version]
- Carestia, A.; Rivadeneyra, L.; Romaniuk, M.A.; Fondevila, C.; Negrotto, S.; Schattner, M. Functional responses and molecular mechanisms involved in histone-mediated platelet activation. Thromb. Haemost. 2013, 110, 1035–1045. [Google Scholar] [CrossRef] [Green Version]
- Rex, S.; Beaulieu, L.M.; Perlman, D.H.; Vitseva, O.; Blair, P.S.; McComb, M.E.; Costello, C.E.; Freedman, J.E. Immune versus thrombotic stimulation of platelets differentially regulates signalling pathways, intracellular protein-protein interactions, and α-granule release. Thromb. Haemost. 2009, 102, 97–110. [Google Scholar] [CrossRef] [Green Version]
- Albu, D.E.; Copotoiu, M.; Szmuk, P.; Copotoiu, S.M. Platelets and infections. Rev. Rom. Med. Lab. 2018, 26, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Rossaint, J.; Margraf, A.; Zarbock, A. Role of platelets in leukocyte recruitment and resolution of inflammation. Front. Immunol. 2018, 9, 2712. [Google Scholar] [CrossRef]
- Krijgsveld, J.; Zaat, S.A.J.; Meeldijk, J.; Van Veelen, P.A.; Fang, G.; Poolman, B.; Brandt, E.; Ehlert, J.E.; Kuijpers, A.J.; Engbers, G.H.M.; et al. Thrombocidins, microbicidal proteins from human blood platelets, are C-terminal deletion products of CXC chemokines. J. Biol. Chem. 2000, 275, 20374–20381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalska, M.A.; Rauova, L.; Poncz, M. Role of the platelet chemokine platelet factor 4 (PF4) in hemostasis and thrombosis. Thromb. Res. 2010, 125, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.; Yang, H.; Wang, Y.; Yang, Y.; Guo, C.F.; Wang, C.S.; Ji, Q. Protomic Profiles of Patients with Atrial Fibrillation Provide New Candidate Biomakers for Diagnosis. SSRN Electron. J. 2020, 344, 205–212. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Stroke Group 1 Day of Hospitalization (A) (Mean ± SD) | Control Group (K) (Mean ± SD) | p | |
|---|---|---|---|
| n | 31 | 29 | |
| Age (years) | 62.7 ± 9.35 | 62 ± 11.4 | >0.10 |
| F/M | 13/18 | 14/15 | >0.10 |
| Hypertension | 21/10 | 17/12 | >0.10 |
| Previous MI or PCI/CABG | 6/25 | 3/26 | >0.05 |
| CKD | 0/31 | 0/29 | >0.10 |
| DM | 8/23 | 6/23 | >0.10 |
| Hb (g/dL) | 14.39 ± 1.63 | 13.78 ± 1.66 | >0.10 |
| Ht (%) | 42.65 ± 4.45 | 40.87 ± 4.90 | >0.10 |
| RBC (106/µL) | 4.79 ± 0.59 | 4.68 ± 0.60 | >0.10 |
| MCH (pg) | 30.44 ± 1.62 | 29.48 ± 1.95 | <0.05 * |
| MCV (fL) | 90.19 ± 4.69 | 87.38 ± 4.86 | >0.10 |
| MCHC (g/dL) | 33.71 ± 0.83 | 33.73 ± 1.34 | >0.10 |
| WBC (103/µL) | 9.16 ± 3.48 | 7.03 ± 2.60 | <0.001 * |
| Lymphocytes (103/µL) | 1.91 ± 0.68 | 2.01 ± 0.78 | >0.10 |
| Neutrophils (103/µL) | 6.49 ± 3.28 | 4.50 ± 2.46 | <0.025 * |
| PLT (103/µL) | 220.57 ± 59.87 | 244.58 ± 46.99 | >0.10 |
| MPV (fL) | 9.38 ± 1.26 | 10.87 ± 0.83 | <0.005 * |
| hsCRP (mg/L) | 4.98 ± 5.39 | 5.51 ± 6.00 | >0.10 |
| Potassium (mmol/L) | 3.85 ± 0.34 | 4.14 ± 0.43 | <0.001 * |
| Sodium (mmol/L) | 138.77 ± 2.50 | 140.19 ± 2.43 | >0.10 |
| Glucose (mg/dL) | 126.90 ± 48.35 | 109.87 ± 55.32 | <0.005 * |
| Creatinine (mg/dL) | 0.92 ± 0.26 | 0.89 ± 0.28 | >0.10 |
| AST (AU) | 19.00 ± 7.06 | 23.35 ± 12.71 | >0.10 |
| ALT (AU) | 21.63 ± 9.79 | 25.73 ± 14.82 | >0.10 |
| Bilirubin (mg/dL) | 0.54 ± 0.07 | 0.73 ± 0.29 | >0.10 |
| TCh (mg/dL) | 184.27 ± 48.20 | 203.38 ± 53.80 | >0.10 |
| HDL (mg/dL) | 49.20 ± 13.6 | 56.57 ± 17.08 | >0.10 |
| LDL (mg/dL) | 108.83 ± 41.5 | 122.81 ± 47.45 | >0.10 |
| TG (mg/dL) | 124.28 ± 60.28 | 128.23 ± 61.20 | >0.10 |
| TSH (µIU/mL) | 3.58 ± 2.68 | 1.53 ± 0.81 | <0.025 * |
| APTT (s) | 27.66 ± 3.59 | 28.73 ± 5.35 | >0.10 |
| INR | 0.96 ± 0.07 | 0.99 ± 0.05 | >0.10 |
| Protein | Compared Group | q Value | Ratio | Change Multiplier | Number of Peptides |
|---|---|---|---|---|---|
| Beta-amyloid protein A4 | K vs. A | 0.00836 * | 0.76 | 1.31 | 12 |
| K vs. B | 1 | 0.53 | 1.89 | 14 | |
| K vs. C | 1 | 0.48 | 2.07 | 14 | |
| A vs. B | 1 | 0.8 | 1.24 | 14 | |
| A vs. C | 1 | 0.87 | 1.15 | 14 | |
| Amyloid-like protein 2 | K vs. A | 0.00836 * | 0.76 | 1.31 | 12 |
| K vs. B | 1 | 0.53 | 1.89 | 14 | |
| K vs. C | 1 | 0.48 | 2.07 | 14 | |
| A vs. B | 1 | 0.8 | 1.24 | 14 | |
| A vs. C | 1 | 0.87 | 1.15 | 14 | |
| Coactosin-like protein | K vs. A | 0.02739 * | 1.48 | 1.48 | 7 |
| K vs. B | 0.92572 | 1.55 | 1.55 | 7 | |
| K vs. C | 1 | 1.32 | 1.32 | 7 | |
| A vs. B | 1 | 1.11 | 1.11 | 7 | |
| A vs. C | 1 | 0.93 | 1.08 | 7 | |
| Thymidine phosphorylase-4 | K vs. A | 0.00041 * | 0.74 | 1.36 | 41 |
| K vs. B | 0.01351 * | 0.66 | 1.57 | 47 | |
| K vs. C | 1 | 0.71 | 0.41 | 48 | |
| A vs. B | 1 | 0.99 | 1.01 | 48 | |
| A vs. C | 1 | 0.99 | 1.01 | 48 | |
| Interferon regulatory factor 7 | K vs. A | 0.00041 * | 0.74 | 1.36 | 41 |
| K vs. B | 0.01351 * | 0.66 | 1.57 | 47 | |
| K vs. C | 1 | 0.71 | 0.41 | 48 | |
| A vs. B | 1 | 0.99 | 1.01 | 48 | |
| A vs. C | 1 | 0.99 | 1.01 | 48 | |
| S protein dependent on vitamin K | K vs. A | 0.00836 * | 0.55 | 1.82 | 7 |
| K vs. B | 1 | 0.92 | 1.09 | 9 | |
| K vs. C | 1 | 0.92 | 1.09 | 9 | |
| A vs. B | 1 | 1.37 | 1.37 | 9 | |
| A vs. C | 1 | 1.12 | 1.12 | 9 | |
| Filamine A Filamine B Filamine C | K vs. A | 1 | 0.96 | 1.04 | 211 |
| K vs. B | 0.21428 | 1.13 | 1.13 | 238 | |
| K vs. C | 1 | 1.11 | 1.11 | 243 | |
| A vs. B | 0.04415 * | 1.15 | 1.15 | 239 | |
| A vs. C | 0.98621 | 1.16 | 1.16 | 244 | |
| Thrombospondin-1 Thrombospondin-2 | K vs. A | 0.94972 | 0.9 | 1.12 | 86 |
| K vs. B | 1 | 0.8 | 1.24 | 98 | |
| K vs. C | 0.00061 * | 0.7 | 1.44 | 100 | |
| A vs. B | 1 | 0.98 | 1.02 | 99 | |
| A vs. C | 0.02598 * | 0.86 | 1.16 | 100 | |
| Histone proteins | K vs. A | 0.04951 * | 0.16 | 6.12 | 2 |
| K vs. B | 1 | 0.68 | 1.47 | 2 | |
| K vs. C | 1 | 0.83 | 1.21 | 2 | |
| A vs. B | 1 | 4.19 | 4.19 | 2 | |
| A vs. C | 1 | 4.63 | 4.63 | 2 | |
| Platelet basic protein | K vs. A | 0.00041 * | 0.62 | 1.62 | 12 |
| K vs. B | 0.08849 | 0.76 | 1.31 | 14 | |
| K vs. C | 0.12338 | 0.71 | 1.4 | 14 | |
| A vs. B | 1 | 0.93 | 1.08 | 14 | |
| A vs. C | 1 | 0.93 | 1.08 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawryś, K.; Turek-Jakubowska, A.; Gawryś, J.; Jakubowski, M.; Dębski, J.; Szahidewicz-Krupska, E.; Trocha, M.; Derkacz, A.; Doroszko, A. Platelet-Derived Drug Targets and Biomarkers of Ischemic Stroke—The First Dynamic Human LC-MS Proteomic Study. J. Clin. Med. 2022, 11, 1198. https://doi.org/10.3390/jcm11051198
Gawryś K, Turek-Jakubowska A, Gawryś J, Jakubowski M, Dębski J, Szahidewicz-Krupska E, Trocha M, Derkacz A, Doroszko A. Platelet-Derived Drug Targets and Biomarkers of Ischemic Stroke—The First Dynamic Human LC-MS Proteomic Study. Journal of Clinical Medicine. 2022; 11(5):1198. https://doi.org/10.3390/jcm11051198
Chicago/Turabian StyleGawryś, Karolina, Aleksandra Turek-Jakubowska, Jakub Gawryś, Maciej Jakubowski, Janusz Dębski, Ewa Szahidewicz-Krupska, Małgorzata Trocha, Arkadiusz Derkacz, and Adrian Doroszko. 2022. "Platelet-Derived Drug Targets and Biomarkers of Ischemic Stroke—The First Dynamic Human LC-MS Proteomic Study" Journal of Clinical Medicine 11, no. 5: 1198. https://doi.org/10.3390/jcm11051198