
Efficacy of Intense Pulsed Light Combined Blood Extract Eye Drops for Treatment of Nociceptive Pain in Dry Eye Patients

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Questionnaires
2.2.1. Visual Analog Scale (VAS) of Ocular Pain
2.2.2. Ocular Surface Disease Index (OSDI)
2.2.3. Ocular Pain Assessment Survey (OPAS)
2.2.4. Patient Health Questionnaire-9 Items (PHQ-9)
2.2.5. Generalized Anxiety Disorder (GAD-7)
2.2.6. Athens Insomnia Scale (AIS)
2.3. DED Examination
2.3.1. Corneal Fluorescence Staining (CFS) Score
2.3.2. TBUT Test
2.3.3. Schirmer I Test (SIT)
2.3.4. Meibomian Gland Expressibility Score
2.3.5. Meibomian Gland Secretion Quality Score
2.3.6. In Vivo Confocal Microscopy (IVCM)
2.3.7. Tears Collection
2.3.8. Luminex Assay
2.3.9. ELISA Assay
2.4. Statistics
3. Results
3.1. Baseline Characteristics
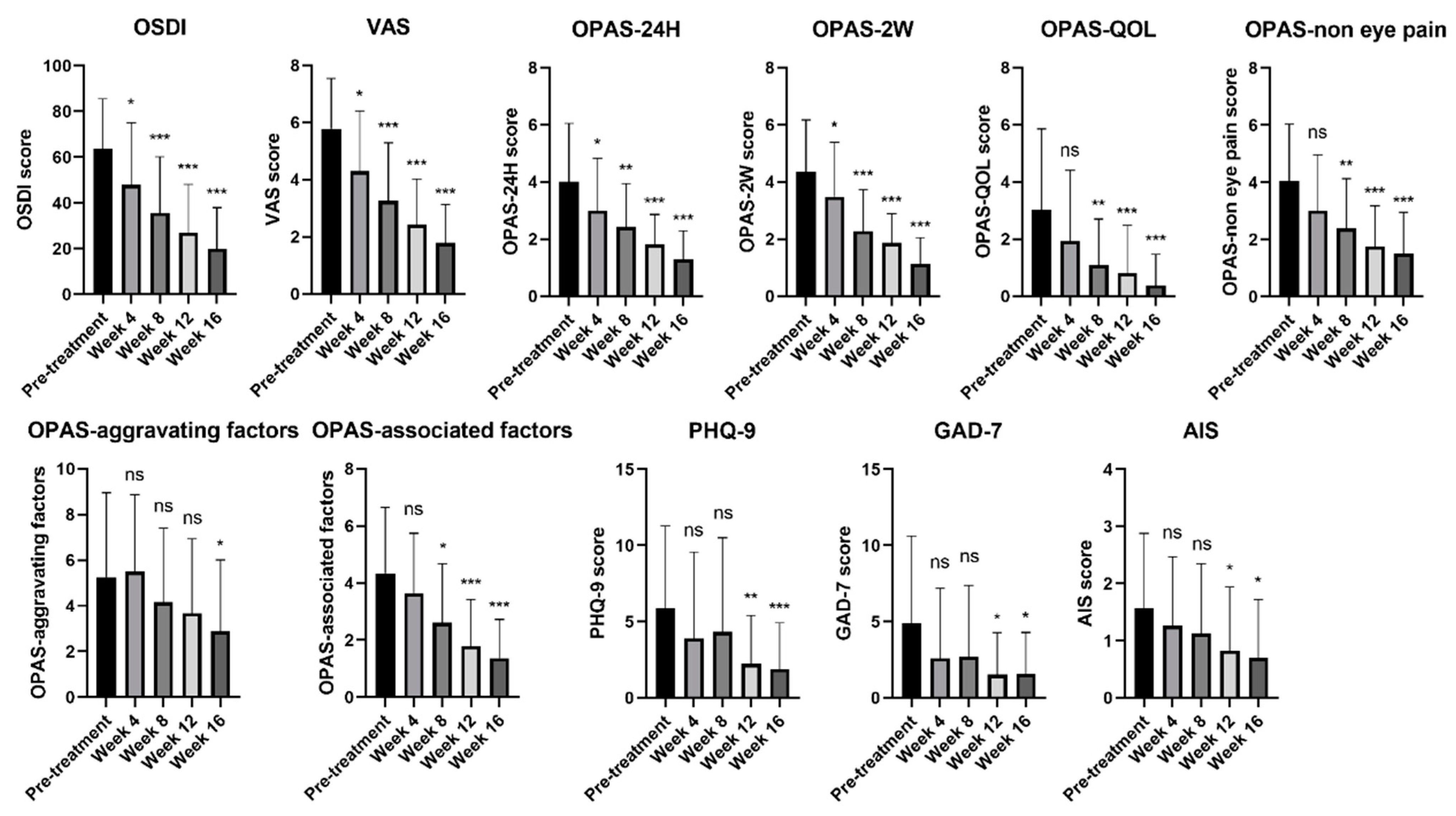
3.2. Improvements in Psychological Symptoms of DED Patients with Ocular Pain Using IPL Combined with DCBE Eye Drops
3.3. Dry-Eye-Related Signs of DED Patients with Ocular Pain Improved by IPL Combined with DCBE Eye Drops
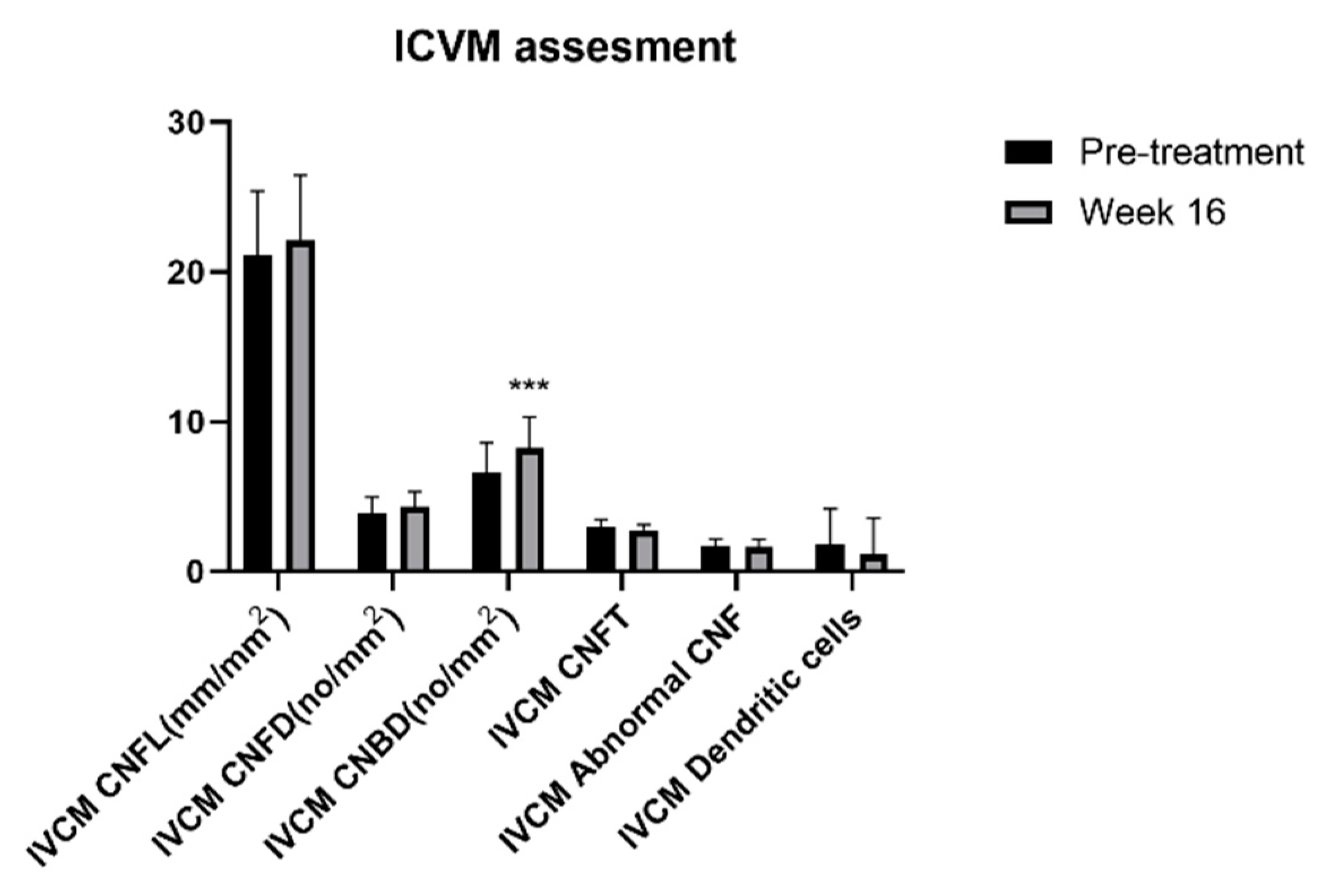
3.4. Corneal Nerves Brand Density of DED Patients with Ocular Pain Improved with IPL Combined with DCBE
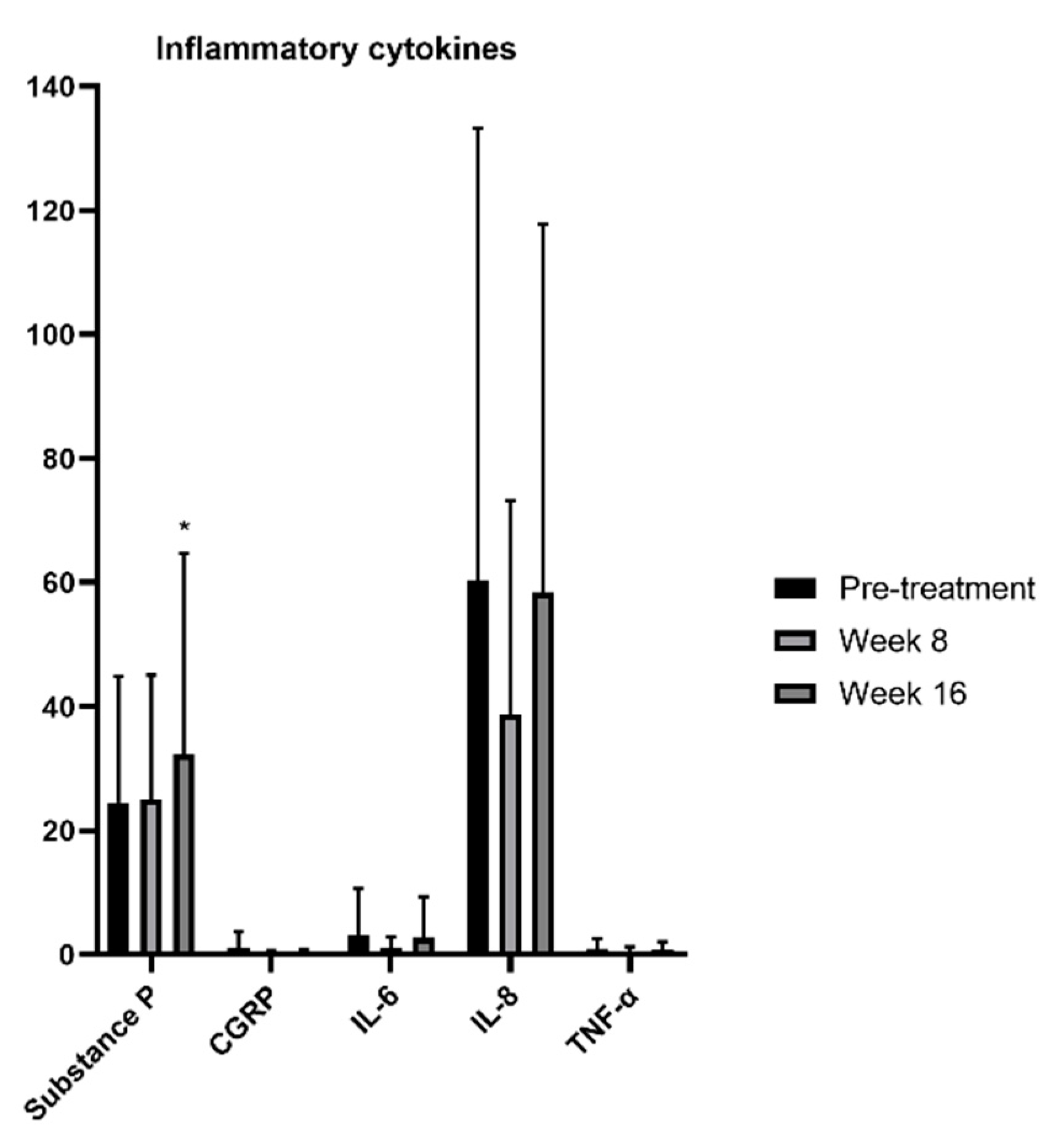
3.5. Substance P in DED Patients with Ocular Pain Increased with IPL Combined with DCBE Eye Drops
3.6. VAS Scores Were Affected by Several Factors after Combined IPL and DCBE Eye Drops Treatment of DED Patients with Ocular Pain
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.-S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.-K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- McDonald, M.; Patel, D.A.; Keith, M.S.; Snedecor, S.J. Economic and Humanistic Burden of Dry Eye Disease in Europe, North America, and Asia: A Systematic Literature Review. Ocul. Surf. 2016, 14, 144–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieckmann, G.; Goyal, S.; Hamrah, P. Neuropathic Corneal Pain: Approaches for Management. Ophthalmology 2017, 124, S34–S47. [Google Scholar] [CrossRef] [PubMed]
- Galor, A.; Covington, D.; Levitt, A.E.; McManus, K.T.; Seiden, B.; Felix, E.; Kalangara, J.; Feuer, W.; Patin, D.J.; Martin, E.R.; et al. Neuropathic Ocular Pain due to Dry Eye is Associated with Multiple Comorbid Chronic Pain Syndromes. J. Pain 2016, 17, 310–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galor, A.; Levitt, R.C.; Felix, E.R.; Martin, E.R.; Sarantopoulos, C.D. Neuropathic ocular pain: An important yet underevaluated feature of dry eye. Eye 2015, 29, 301–312. [Google Scholar] [CrossRef]
- Saldanha, I.J.; Petris, R.; Han, G.; Dickersin, K.; Akpek, E.K. Research Questions and Outcomes Prioritized by Patients With Dry Eye. JAMA Ophthalmol. 2018, 136, 1170–1179. [Google Scholar] [CrossRef] [Green Version]
- Galor, A.; Moein, H.-R.; Lee, C.; Rodriguez, A.; Felix, E.; Sarantopoulos, K.D.; Levitt, R.C. Neuropathic pain and dry eye. Ocul. Surf. 2018, 16, 31–44. [Google Scholar] [CrossRef]
- Belmonte, C.; Nichols, J.J.; Cox, S.M.; Brock, J.; Begley, C.G.; Bereiter, D.A.; Dartt, D.A.; Galor, A.; Hamrah, P.; Ivanusic, J.; et al. TFOS DEWS II pain and sensation report. Ocul. Surf. 2017, 15, 404–437. [Google Scholar] [CrossRef] [Green Version]
- Lekhanont, K.; Rojanaporn, D.; Chuck, R.S.; Vongthongsri, A. Prevalence of dry eye in Bangkok, Thailand. Cornea 2006, 25, 1162–1167. [Google Scholar] [CrossRef]
- Lin, P.Y.; Tsai, S.Y.; Cheng, C.Y.; Liu, J.H.; Chou, P.; Hsu, W.M. Prevalence of dry eye among an elderly Chinese population in Taiwan: The Shihpai Eye Study. Ophthalmology 2003, 110, 1096–1101. [Google Scholar] [CrossRef]
- Jie, Y.; Xu, L.; Wu, Y.Y.; Jonas, J.B. Prevalence of dry eye among adult Chinese in the Beijing Eye Study. Eye 2009, 23, 688–693. [Google Scholar] [CrossRef] [Green Version]
- Siak, J.J.; Tong, L.; Wong, W.L.; Cajucom-Uy, H.; Rosman, M.; Saw, S.M.; Wong, T.Y. Prevalence and risk factors of meibomian gland dysfunction: The Singapore Malay eye study. Cornea 2012, 31, 1223–1228. [Google Scholar] [CrossRef]
- Uchino, M.; Dogru, M.; Yagi, Y.; Goto, E.; Tomita, M.; Kon, T.; Saiki, M.; Matsumoto, Y.; Uchino, Y.; Yokoi, N.; et al. The features of dry eye disease in a Japanese elderly population. Optom. Vis. Sci. 2006, 83, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Rong, B.; Tu, P.; Tang, Y.; Song, W.; Toyos, R.; Toyos, M.; Yan, X. Analysis of Cytokine Levels in Tears and Clinical Correlations After Intense Pulsed Light Treating Meibomian Gland Dysfunction. Am. J. Ophthalmol. 2017, 183, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Xue, A.L.; Wang, M.T.M.; Ormonde, S.E.; Craig, J.P. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for meibomian gland dysfunction. Ocul. Surf. 2020, 18, 286–297. [Google Scholar] [CrossRef]
- Piyacomn, Y.; Kasetsuwan, N.; Reinprayoon, U.; Satitpitakul, V.; Tesapirat, L. Efficacy and Safety of Intense Pulsed Light in Patients With Meibomian Gland Dysfunction-A Randomized, Double-Masked, Sham-Controlled Clinical Trial. Cornea 2020, 39, 325–332. [Google Scholar] [CrossRef]
- Toyos, R.; McGill, W.; Briscoe, D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; A 3-year retrospective study. Photomed. Laser Surg. 2015, 33, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Jin, X.; Mou, Y.; Yuan, K.; Min, J.; Huang, X. A 4-week, randomized, double-masked study to evaluate efficacy of deproteinized calf blood extract eye drops versus sodium hyaluronate 0.3% eye drops in dry eye patients with ocular pain. Ann. Palliat. Med. 2021, 10, 3617–3625. [Google Scholar] [CrossRef]
- Lv, H.; Liu, Z.; Li, X.; Wang, W. Effect of lacrimal plugs combined with deproteinized calf blood extract eye gel for filamentary keratitis. J. Ocul. Biol. Dis. Inform. 2010, 3, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, X.-D.; Gong, L.; Sun, X.-H.; Zhao, N.-Q.; Zhu, Z.-R.; Li, Y.-M.; Yao, K.; Zhao, W.-L. Efficacy of Protein-Free Calf Blood Extract for Mechanical Corneal Epithelial Defects in Human Eyes. Chin. J. Ophthalmol. 2008, 44, 720–725. [Google Scholar]
- Chen, M.J.; Gong, L.; Qiu, X.D. Efficacy of Protein-Free Calf Blood Extract Ophthalmic Gel for Diffuse Punctate Corneal Epithelial Defects. Chin. J. Ophthalmol. 2012, 48, 1083–1087. [Google Scholar]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Qazi, Y.; Hurwitz, S.; Khan, S.; Jurkunas, U.V.; Dana, R.; Hamrah, P. Validity and Reliability of a Novel Ocular Pain Assessment Survey (OPAS) in Quantifying and Monitoring Corneal and Ocular Surface Pain. Ophthalmology 2016, 123, 1458–1468. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9 validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder the GAD-7. Arch. Intern. Med. 2006, 22, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Willcox, M.D.; Argüeso, P.; Georgiev, G.; Holopainen, J.M.; Laurie, G.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Siedlecki, A.N.; Smith, S.D.; Siedlecki, A.R.; Hayek, S.M.; Sayegh, R.R. Ocular pain response to treatment in dry eye patients. Ocul. Surf. 2020, 18, 305–311. [Google Scholar] [CrossRef]
- Gao, Y.-F.; Liu, R.-J.; Li, Y.-X.; Huang, C.; Liu, Y.-Y.; Hu, C.-X.; Qi, H. Comparison of anti-inflammatory effects of intense pulsed light with tobramycin/dexamethasone plus warm compress on dry eye associated meibomian gland dysfunction. Int. J. Ophthalmol. 2019, 12, 1708–1713. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Chen, Y.H.; Turnbull, P.R. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest. Ophthalmol. Vis. Sci. 2015, 56, 1965–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mashaghi, A.; Marmalidou, A.; Tehrani, M.; Grace, P.M.; Pothoulakis, C.; Dana, R. Neuropeptide substance P and the immune response. Cell. Mol. Life Sci. 2016, 73, 4249–4264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwal, A.; Hao, J.L.; Zhou, D.D.; Liu, X.F.; Suwal, R.; Lu, C.W. Use of Intense Pulsed Light to Mitigate Meibomian Gland Dysfunction for Dry Eye Disease. Int. J. Med. Sci. 2020, 17, 1385–1392. [Google Scholar] [CrossRef]
- Dell, S.J. Intense pulsed light for evaporative dry eye disease. Clin. Ophthalmol. 2017, 11, 1167–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiev, G.A.; Eftimov, P.; Yokoi, N. Structure-function relationship of tear film lipid layer: A contemporary perspective. Exp. Eye Res. 2017, 163, 17–28. [Google Scholar] [CrossRef]
- Albietz, J.M.; Schmid, K.L. Intense pulsed light treatment and meibomian gland expression for moderate to advanced meibomian gland dysfunction. Clin. Exp. Optom. 2018, 101, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, S.; Kheirkhah, A.; Cavalcanti, B.; Cruzat, A.; Colon, C.; Brown, E.; Borsook, D.; Prüss, H.; Hamrah, P. Autologous Serum Tears for Treatment of Photoallodynia in Patients with Corneal Neuropathy: Efficacy and Evaluation with In Vivo Confocal Microscopy. Ocul. Surf. 2015, 13, 250–262. [Google Scholar] [CrossRef] [Green Version]
- Attal, N. Neuropathic pain: Mechanisms, therapeutic approach, and interpretation of clinical trials. Contin. Lifelong Learn. Neurol. 2012, 18, 161–175. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 4, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Kurose, M.; Meng, I.D. Dry eye modifies the thermal and menthol responses in rat corneal primary afferent cool cells. J. Neurophysiol. 2013, 110, 495–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergés, C.; Salgado-Borges, J.; Ribot, F.M. Prospective evaluation of a new intense pulsed light, thermaeye plus, in the treatment of dry eye disease due to meibomian gland dysfunction. J. Optom. 2021, 14, 103–113. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject (n = 23) | |
|---|---|
| Age | 46.83 ± 14.77 |
| Sex (male:female) | 5:18 |
| Years after diagnosis | 1.91 ± 1.12 |
| Double eye pain | 23 |
| No headache or facial pain | 8 |
| Right side headache or facial pain (with right eye pain) | 1 |
| Left side headache or facial pain (with left eye pain) | 0 |
| Bilateral headache or facial pain | 14 |
| Insomnia | 10 |
| Depression | 5 |
| Anxiety | 5 |
| Ocular disease or with history of ocular trauma or surgery | 9 |
| Systemic diseases | 9 |
| Sjogren Syndrom | 1 |
| Pre-Treatment | Week 16 | |||||
|---|---|---|---|---|---|---|
| Normal-Response Group | Sensitive-Response Group | p | Normal-Response Group | Sensitive-Response Group | p | |
| VAS | 4.92 ± 1.78 | 6.73 ± 1.19 | 3.13 ± 1.37 | 1.18 ± 1.08 | ||
| OSDI | 65.82 ± 22.58 | 61.02 ± 22.10 | 0.689 | 22.31 ± 18.06 | 17.58 ± 18.30 | 0.478 |
| OPAS | ||||||
| OPAS-24H | 3.78 ± 2.26 | 4.27 ± 1.84 | 0.174 | 1.83 ± 0.96 | 0.7 ± 0.66 | 0.004 ** |
| OPAS-2W | 3.94 ± 2.3 | 4.79 ± 1.02 | 0.169 | 1.92 ± 1.14 | 1.82 ± 0.92 | 0.701 |
| OPAS QOL | 3.22 ± 2.99 | 2.82 ± 2.80 | 0.709 | 0.56 ± 1.45 | 0.21 ± 0.40 | 0.968 |
| OPAS non-eye pain | 3.75 ± 1.51 | 4.4 ± 2.42 | 0.518 | 2.01 ± 1.42 | 0.97 ± 1.31 | 0.026 * |
| OPAS aggravating factors | 5.36 ± 3.3 | 5.14 ± 4.25 | 0.802 | 3.17 ± 2.84 | 2.59 ± 3.52 | 0.474 |
| OPAS associated factors | 4.15 ± 2.53 | 4.55 ± 2.14 | 0.779 | 1.38 ± 0.86 | 1.36 ± 1.78 | 0.223 |
| PHQ-9 | 7.00 ± 6.34 | 4.64 ± 4.13 | 0.353 | 2.58 ± 3.90 | 1.18 ± 1.47 | 0.548 |
| GAD-7 | 4.75 ± 6.15 | 5.00 ± 5.59 | 0.900 | 2.75 ± 3.36 | 0.27 ± 0.65 | 0.011 * |
| AIS | 1.58 ± 1.24 | 1.55 ± 1.44 | 0.948 | 0.83 ± 1.03 | 0.55 ± 1.04 | 0.361 |
| CFS | 2.08 ± 2.19 | 1.36 ± 1.03 | 0.743 | 0.58 ± 0.9 | 0.27 ± 0.65 | 0.270 |
| TBUT (s) | 1.76 ± 0.81 | 2.33 ± 1.38 | 0.389 | 7.80 ± 4.42 | 6.97 ± 3.63 | 0.854 |
| Schirmer I test (mm) | 9.50 ± 7.63 | 6.45 ± 6.11 | 0.138 | 14.08 ± 8.50 | 12.00 ± 9.53 | 0.439 |
| MGYSS | 33.92 ± 6.56 | 29.55 ± 8.57 | 0.109 | 21.92 ± 5.73 | 14.82 ± 9.24 | 0.024 * |
| MGYLS | 12.58 ± 5.23 | 9.91 ± 4.74 | 0.115 | 9.42 ± 4.19 | 5 ± 3.82 | 0.019 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.; Mou, Y.; Zhang, Y.; Han, Y.; Lin, L.; Huo, Y.; Zhu, Y.; Yang, S.; Huang, X. Efficacy of Intense Pulsed Light Combined Blood Extract Eye Drops for Treatment of Nociceptive Pain in Dry Eye Patients. J. Clin. Med. 2022, 11, 1312. https://doi.org/10.3390/jcm11051312
Wu Y, Mou Y, Zhang Y, Han Y, Lin L, Huo Y, Zhu Y, Yang S, Huang X. Efficacy of Intense Pulsed Light Combined Blood Extract Eye Drops for Treatment of Nociceptive Pain in Dry Eye Patients. Journal of Clinical Medicine. 2022; 11(5):1312. https://doi.org/10.3390/jcm11051312
Chicago/Turabian StyleWu, Yaying, Yujie Mou, Yu Zhang, Yu Han, Lin Lin, Yanan Huo, Yirui Zhu, Shuo Yang, and Xiaodan Huang. 2022. "Efficacy of Intense Pulsed Light Combined Blood Extract Eye Drops for Treatment of Nociceptive Pain in Dry Eye Patients" Journal of Clinical Medicine 11, no. 5: 1312. https://doi.org/10.3390/jcm11051312