
Lower SARS-CoV-2 Seroprevalence among Cancer Patients in Sub-Saharan Africa

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Subjects, and Samples
2.2. HIV-1 Serological Testing
2.3. Immunofluorescence Assay against SARS-CoV-2 Spike and Nucleocapsid Proteins
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Cohort
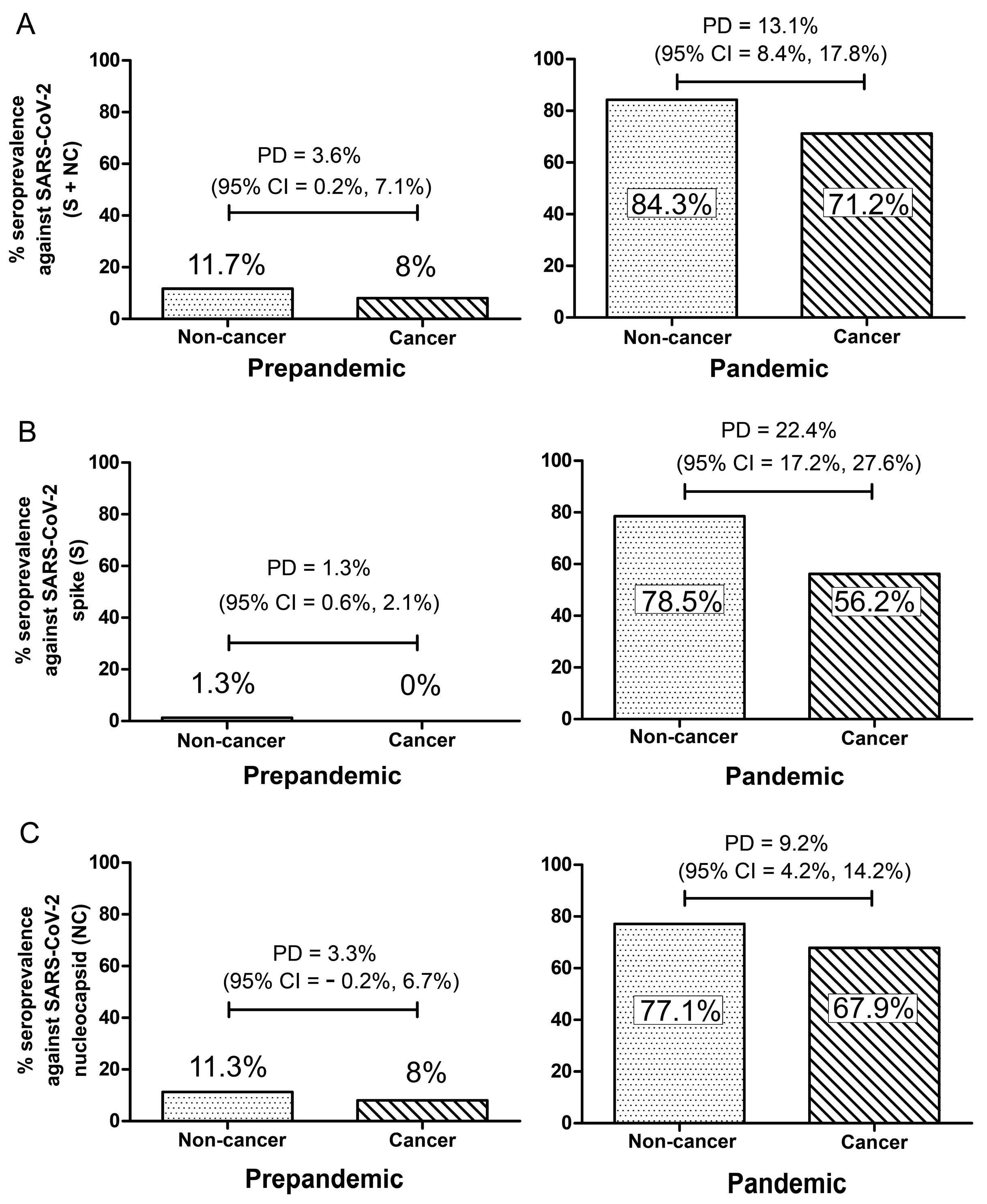
3.2. Seroprevalence against SARS-CoV-2 Spike and Nucleocapsid Proteins
3.3. Logistic Regression Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Treskova-Schwarzbach, M.; Haas, L.; Reda, S.; Pilic, A.; Borodova, A.; Karimi, K.; Koch, J.; Nygren, T.; Scholz, S.; Schonfeld, V.; et al. Pre-existing health conditions and severe COVID-19 outcomes: An umbrella review approach and meta-analysis of global evidence. BMC Med. 2021, 19, 212. [Google Scholar] [CrossRef] [PubMed]
- Gouda, H.N.; Charlson, F.; Sorsdahl, K.; Ahmadzada, S.; Ferrari, A.J.; Erskine, H.; Leung, J.; Santamauro, D.; Lund, C.; Aminde, L.N.; et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet Glob. Health 2019, 7, e1375–e1387. [Google Scholar] [CrossRef] [Green Version]
- Kharsany, A.B.; Karim, Q.A. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. Open AIDS J. 2016, 10, 34–48. [Google Scholar] [CrossRef] [Green Version]
- Chinula, L.; Moses, A.; Gopal, S. HIV-associated malignancies in sub-Saharan Africa: Progress, challenges, and opportunities. Curr. Opin. HIV AIDS 2017, 12, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Mellor, M.M.; Bast, A.C.; Jones, N.R.; Roberts, N.W.; Ordonez-Mena, J.M.; Reith, A.J.M.; Butler, C.C.; Matthews, P.C.; Dorward, J. Risk of adverse coronavirus disease 2019 outcomes for people living with HIV. AIDS 2021, 35, F1–F10. [Google Scholar] [CrossRef]
- Mirzaei, H.; McFarland, W.; Karamouzian, M.; Sharifi, H. COVID-19 Among People Living with HIV: A Systematic Review. AIDS Behav. 2021, 25, 85–92. [Google Scholar] [CrossRef]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat. Rev. Cancer 2021, 21, 345–359. [Google Scholar] [CrossRef]
- Overheu, O.; Quast, D.R.; Schmidt, W.E.; Sakinc-Guler, T.; Reinacher-Schick, A. Low Serological Prevalence of SARS-CoV-2 Antibodies in Cancer Patients at a German University Oncology Center. Oncol. Res. Treat. 2022, 45, 112–117. [Google Scholar] [CrossRef]
- Yazaki, S.; Yoshida, T.; Kojima, Y.; Yagishita, S.; Nakahama, H.; Okinaka, K.; Matsushita, H.; Shiotsuka, M.; Kobayashi, O.; Iwata, S.; et al. Difference in SARS-CoV-2 Antibody Status Between Patients with Cancer and Health Care Workers During the COVID-19 Pandemic in Japan. JAMA Oncol. 2021, 7, 1141–1148. [Google Scholar] [CrossRef]
- Martei, Y.M.; Rick, T.J.; Fadelu, T.; Ezzi, M.S.; Hammad, N.; Quadri, N.S.; Rodrigues, B.; Simonds, H.; Grover, S.; Incrocci, L.; et al. Impact of COVID-19 on Cancer Care Delivery in Africa: A Cross-Sectional Survey of Oncology Providers in Africa. JCO Glob. Oncol. 2021, 7, 368–377. [Google Scholar] [CrossRef]
- Diop, B.Z.; Ngom, M.; Pougue Biyong, C.; Pougue Biyong, J.N. The relatively young and rural population may limit the spread and severity of COVID-19 in Africa: A modelling study. BMJ Glob. Health 2020, 5, e002699. [Google Scholar] [CrossRef]
- Hamdi, Y.; Abdeljaoued-Tej, I.; Zatchi, A.A.; Abdelhak, S.; Boubaker, S.; Brown, J.S.; Benkahla, A. Cancer in Africa: The Untold Story. Front. Oncol. 2021, 11, 650117. [Google Scholar] [CrossRef]
- Haider, N.; Osman, A.Y.; Gadzekpo, A.; Akipede, G.O.; Asogun, D.; Ansumana, R.; Lessells, R.J.; Khan, P.; Hamid, M.M.A.; Yeboah-Manu, D.; et al. Lockdown measures in response to COVID-19 in nine sub-Saharan African countries. BMJ Glob. Health 2020, 5, e003319. [Google Scholar] [CrossRef]
- Abdul-Rasool, S.; Fielding, B.C. Understanding Human Coronavirus HCoV-NL63. Open Virol. J. 2010, 4, 76–84. [Google Scholar] [CrossRef]
- Tso, F.Y.; Lidenge, S.J.; Pena, P.B.; Clegg, A.A.; Ngowi, J.R.; Mwaiselage, J.; Ngalamika, O.; Julius, P.; West, J.T.; Wood, C. High prevalence of pre-existing serological cross-reactivity against severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in sub-Saharan Africa. Int. J. Infect. Dis. 2021, 102, 577–583. [Google Scholar] [CrossRef]
- Van Rooyen, C.; Brauer, M.; Swanepoel, P.; van den Berg, S.; van der Merwe, C.; van der Merwe, M.; Green, R.; Becker, P. Comparison of T-cell immune responses to SARS-CoV-2 spike (S) and nucleocapsid (N) protein using an in-house flow-cytometric assay in laboratory employees with and without previously confirmed COVID-19 in South Africa: Nationwide cross-sectional study. J. Clin. Pathol. 2022, 1–7. [Google Scholar] [CrossRef]
- Cabezon-Gutierrez, L.; Custodio-Cabello, S.; Palka-Kotlowska, M.; Oliveros-Acebes, E.; Garcia-Navarro, M.J.; Khosravi-Shahi, P. Seroprevalence of SARS-CoV-2-specific antibodies in cancer outpatients in Madrid (Spain): A single center, prospective, cohort study and a review of available data. Cancer Treat. Rev. 2020, 90, 102102. [Google Scholar] [CrossRef]
- Zhou, K.; Raoul, J.L.; Blanc-Lapierre, A.; Seegers, V.; Boisdron-Celle, M.; Bourdon, M.; Mahammedi, H.; Lambert, A.; Moreau-Bachelard, C.; Campone, M.; et al. COVID-19 Infections in Cancer Patients Were Frequently Asymptomatic: Description from a French Prospective Multicenter Cohort (PAPESCO-19). Clin. Med. Insights Oncol. 2022, 16, 11795549221090187. [Google Scholar] [CrossRef] [PubMed]
- Cantini, L.; Bastianelli, L.; Lupi, A.; Pinterpe, G.; Pecci, F.; Belletti, G.; Stoico, R.; Vitarelli, F.; Moretti, M.; Onori, N.; et al. Seroprevalence of SARS-CoV-2-Specific Antibodies in Cancer Patients Undergoing Active Systemic Treatment: A Single-Center Experience from the Marche Region, Italy. J. Clin. Med. 2021, 10, 1503. [Google Scholar] [CrossRef]
- Chisale, M.R.O.; Ramazanu, S.; Mwale, S.E.; Kumwenda, P.; Chipeta, M.; Kaminga, A.C.; Nkhata, O.; Nyambalo, B.; Chavura, E.; Mbakaya, B.C. Seroprevalence of anti-SARS-CoV-2 antibodies in Africa: A systematic review and meta-analysis. Rev. Med. Virol. 2022, 32, e2271. [Google Scholar] [CrossRef] [PubMed]
- Meinus, C.; Singer, R.; Nandi, B.; Jagot, O.; Becker-Ziaja, B.; Karo, B.; Mvula, B.; Jansen, A.; Baumann, J.; Schultz, A. SARS-CoV-2 prevalence and immunity: A hospital-based study from Malawi. Int. J. Infect. Dis. 2022, 116, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Uyoga, S.; Adetifa, I.M.O.; Karanja, H.K.; Nyagwange, J.; Tuju, J.; Wanjiku, P.; Aman, R.; Mwangangi, M.; Amoth, P.; Kasera, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Kenyan blood donors. Science 2021, 371, 79–82. [Google Scholar] [CrossRef]
- Lindahl, A.; Aro, M.; Reijula, J.; Makela, M.J.; Ollgren, J.; Puolanne, M.; Jarvinen, A.; Vasankari, T. Women report more symptoms and impaired quality of life: A survey of Finnish COVID-19 survivors. Infect. Dis. 2022, 54, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Chavez-MacGregor, M.; Lei, X.; Zhao, H.; Scheet, P.; Giordano, S.H. Evaluation of COVID-19 Mortality and Adverse Outcomes in US Patients with or Without Cancer. JAMA Oncol. 2022, 8, 69–78. [Google Scholar] [CrossRef]
- Randolph, H.E.; Barreiro, L.B. Herd Immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef]
- Cron, R.Q.; Caricchio, R.; Chatham, W.W. Calming the cytokine storm in COVID-19. Nat. Med. 2021, 27, 1674–1675. [Google Scholar] [CrossRef]
- UNAIDS. Global HIV & AIDS Statistics 2020 Fact Sheet. Available online: https://aidsinfo.unaids.org/ (accessed on 4 February 2022).
- Lidenge, S.J.; Tran, T.; Tso, F.Y.; Ngowi, J.R.; Shea, D.M.; Mwaiselage, J.; Wood, C.; West, J.T. Prevalence of Kaposi’s sarcoma-associated herpesvirus and transfusion-transmissible infections in Tanzanian blood donors. Int. J. Infect. Dis. 2020, 95, 204–209. [Google Scholar] [CrossRef]
- Moorlag, S.; van Deuren, R.C.; van Werkhoven, C.H.; Jaeger, M.; Debisarun, P.; Taks, E.; Mourits, V.P.; Koeken, V.; de Bree, L.C.J.; Ten Doesschate, T.; et al. Safety and COVID-19 Symptoms in Individuals Recently Vaccinated with BCG: A Retrospective Cohort Study. Cell Rep. Med. 2020, 1, 100073. [Google Scholar] [CrossRef]
- Rivas, M.N.; Ebinger, J.E.; Wu, M.; Sun, N.; Braun, J.; Sobhani, K.; Van Eyk, J.E.; Cheng, S.; Arditi, M. BCG vaccination history associates with decreased SARS-CoV-2 seroprevalence across a diverse cohort of health care workers. J. Clin. Investig. 2021, 131, e145157. [Google Scholar] [CrossRef]
- Wu, J.; Liang, B.; Chen, C.; Wang, H.; Fang, Y.; Shen, S.; Yang, X.; Wang, B.; Chen, L.; Chen, Q.; et al. SARS-CoV-2 infection induces sustained humoral immune responses in convalescent patients following symptomatic COVID-19. Nat. Commun. 2021, 12, 1813. [Google Scholar] [CrossRef]


{kind=link}
| Pre-Pandemic | Potential Blood Donors | Cancer | p-Value |
|---|---|---|---|
| Sample size, N | 900 | 373 | |
| Age, median (IQR) years | 31 (25–39) | 39 (33–45) | <0.0001 |
| Male, N (%) | 710 (78.9%) | 155 (41.6%) | <0.0001 |
| HIV+, N (%) | 29 (3.2%) | 282 (75.6%) | <0.0001 |
| Pandemic | Potential Blood Donors | Cancer | p-Value |
| Sample size, N | 899 | 479 | |
| Age, median (IQR) years | 33 (26–43) | 49 (40–60) | <0.0001 |
| Male, N (%) | 544 (60.5%) | 131 (27.4%) | <0.0001 |
| HIV+, N (%) | 60 (6.7%) | 150 (31.3%) | <0.0001 |
| Number of household members, median (IQR) Samples with missing information, N | 4 (2–5) 22 | 5 (3–7) 2 | <0.0001 |
| Received TB vaccination, N (%) Samples with missing information, N | 800 (89.5%) 5 | 418 (87.8%) 3 | 0.3488 |
| Have COVID-related symptoms, N (%) Samples with missing information, N | 62 (6.9%) 1 | 130 (27.3%) 3 | <0.0001 |
| Cancer Population | Unadjusted Analysis | p-Value | Adjusted Analysis | p-Value |
|---|---|---|---|---|
| Cancer type | ||||
| Breast cancer | 2.379 (1.012–5.592) | 0.047 | 2.023 (0.705–5.801) | 0.19 |
| Cervical cancer | 2.249 (1.105–4.580) | 0.026 | 1.984 (0.783–5.029) | 0.149 |
| Hematological malignancies | 1.133 (0.305–4.216) | 0.852 | 0.985 (0.255–3.805) | 0.982 |
| Other solid malignancies | 2.042 (0.989–4.216) | 0.054 | 1.885 (0.814–4.362) | 0.139 |
| Kaposi’s sarcoma | ref | ref | ||
| Age | 0.997 (0.983–1.011) | 0.653 | 0.992(0.977–1.007) | 0.29 |
| Sex | ||||
| Female | 1.257 (0.965–1.637) | 0.2346 | 1.121 (0.615–2.043) | 0.7089 |
| Male | ref | ref | ||
| HIV status | ||||
| Negative | 1.193 (0.783–1.818) | 0.4106 | 1.1 (0.672–1.801) | 0.705 |
| Positive | ref | ref | ||
| Received TB vaccination | ||||
| Yes | 1.358 (0.917–2.013) | 0.3074 | 1.401 (0.767–2.558) | 0.2731 |
| No | ref | ref | ||
| COVID-19-related symptoms | ||||
| Yes | 0.755 (0.488–1.166) | 0.2052 | 0.726 (0.465–1.135) | 0.1604 |
| No | ref | ref | ||
| Household size | 0.992 (0.924–1.064) | 0.8181 | 0.984 (0.915–1.059) | 0.6702 |
| Potential Blood Donors Population | Unadjusted Analysis OR (95% CI) | p-Value | Adjusted Analysis OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | 1.002 (0.988–1.017) | 0.7428 | 1.003 (0.987–1.018) | 0.7309 |
| Sex | ||||
| Female | 0.860 (0.597–1.238) | 0.4177 | 0.946 (0.642–1.393) | 0.7779 |
| Male | ref | ref | ||
| HIV status | ||||
| Negative | 1.224 (0.620–2.417) | 0.5596 | 1.268 (0.627–2.562) | 0.5088 |
| Positive | ref | ref | ||
| Received TB vaccination | ||||
| Yes | 1.304 (0.753–2.256) | 0.3432 | 1.210 (0.683–2.143) | 0.5141 |
| No | ref | ref | ||
| COVID-19-related symptoms | ||||
| Yes | 1.104 (0.532–2.293) | 0.7904 | 1.161 (0.551–2.444) | 0.6946 |
| No | ref | ref | ||
| Household size | 0.954 (0.878–1.036) | 0.2609 | 0.972 (0.891–1.061) | 0.5282 |
| Potential Blood Donors Population | Unadjusted Analysis OR (95% CI) | p-Value | Adjusted Analysis OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | 1.016 (0.997–1.036) | 0.1074 | 1.007 (0.987–1.029) | 0.4798 |
| Sex | ||||
| Female | 1.958 (1.165–3.291) | 0.0112 | 1.510 (0.870–2.624) | 0.1433 |
| Male | ref | ref | ||
| HIV status | ||||
| Negative | 0.383 (0.179–0.819) | 0.0134 | 0.389 (0.176–0.858) | 0.0194 |
| Positive | ref | ref | ||
| Received TB vaccination | ||||
| Yes | 0.577 (0.283–1.178) | 0.131 | 0.611 (0.290–1.288) | 0.1953 |
| No | ref | ref | ||
| SARS-CoV-2 seroprevalence | ||||
| Yes | 1.104 (0.532–2.293) | 0.7904 | 1.156 (0.549–2.436) | 0.7025 |
| No | ref | ref | ||
| Household size | 1.127 (1.006–1.261) | 0.0386 | 1.100 (0.974–1.242) | 0.1244 |
| Cancer Population | Unadjusted Analysis | p-Value | Adjusted Analysis | p-Value |
|---|---|---|---|---|
| Age | 1.01 (0.996–1.024) | 0.1683 | 1.012 (0.997–1.027) | 0.1199 |
| Sex | ||||
| Female | 1.129 (0.713–1.788) | 0.6057 | 1.021 (0.633–1.647) | 0.9324 |
| Male | ref | ref | ||
| HIV status | ||||
| Negative | 1.049 (0.678–1.621) | 0.8312 | 0.924 (0.568–1.503) | 0.7498 |
| Positive | ref | ref | ||
| Received TB vaccination | ||||
| Yes | 2.602 (1.198–5.652) | 0.0157 | 2.511 (1.114–5.661) | 0.0264 |
| No | ref | ref | ||
| SARS-CoV-2 seroprevalence | ||||
| Yes | 0.755 (0.488–1.166) | 0.2052 | 0.702 (0.449–1.098) | 0.1213 |
| No | ref | ref | ||
| Household size | 0.975 (0.905–1.050) | 0.4973 | 0.977 (0.905–1.054) | 0.5478 |
| Potential Blood Donors Population | Unadjusted Analysis OR (95% CI) | p-Value | Adjusted Analysis OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | 1.018 (0.997–1.039) | 0.0999 | 1.007 (0.984–1.031) | 0.5272 |
| Sex | ||||
| Female | 2.571 (1.452–4.551) | 0.0012 | 1.950 (1.062–3.581) | 0.0312 |
| Male | ref | ref | ||
| HIV status | ||||
| Negative | 0.295 (0.134–0.646) | 0.0023 | 0.305 (0.134–0.694) | 0.0047 |
| Positive | ref | ref | ||
| Received TB vaccination | ||||
| Yes | 0.441 (0.212–0.918) | 0.0287 | 0.482 (0.223–1.042) | 0.0635 |
| No | ref | ref | ||
| Household size | 1.088 (0.958–1.237) | 0.1931 | 1.050 (0.914–1.208) | 0.49 |
| Cancer Population | Unadjusted Analysis | p-Value | Adjusted Analysis | p-Value |
|---|---|---|---|---|
| Age | 1.026 (1.007–1.045) | 0.006 | 1.029 (1.010–1.049) | 0.0034 |
| Sex | ||||
| Female | 1.213 (0.685–2.150) | 0.508 | 0.957 (0.524–1.746) | 0.8849 |
| Male | ref | ref | ||
| HIV status | ||||
| Negative | 1.032 (0.607–1.756) | 0.907 | 0.885 (0.493–1.591) | 0.6837 |
| Positive | ref | ref | ||
| Received TB vaccination | ||||
| Yes | 1.982 (0.799–4.916) | 0.1401 | 1.894 (0.722–4.969) | 0.1944 |
| No | ref | ref | ||
| Household size | 0.945 (0.860–1.038) | 0.2356 | 0.943 (0.854–1.042) | 0.251 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tso, F.Y.; Lidenge, S.J.; Ngowi, J.R.; Peña, P.B.; Clegg, A.A.; Ngalamika, O.; Mwita, C.J.; Mwaiselage, J.; Wood, C. Lower SARS-CoV-2 Seroprevalence among Cancer Patients in Sub-Saharan Africa. J. Clin. Med. 2022, 11, 4428. https://doi.org/10.3390/jcm11154428
Tso FY, Lidenge SJ, Ngowi JR, Peña PB, Clegg AA, Ngalamika O, Mwita CJ, Mwaiselage J, Wood C. Lower SARS-CoV-2 Seroprevalence among Cancer Patients in Sub-Saharan Africa. Journal of Clinical Medicine. 2022; 11(15):4428. https://doi.org/10.3390/jcm11154428
Chicago/Turabian StyleTso, For Yue, Salum J. Lidenge, John R. Ngowi, Phoebe B. Peña, Ashley A. Clegg, Owen Ngalamika, Chacha J. Mwita, Julius Mwaiselage, and Charles Wood. 2022. "Lower SARS-CoV-2 Seroprevalence among Cancer Patients in Sub-Saharan Africa" Journal of Clinical Medicine 11, no. 15: 4428. https://doi.org/10.3390/jcm11154428