
Effects of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: A Randomized Controlled Trial

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Interventions
2.3.1. Fasting and Lifestyle Modification (F + LM)
2.3.2. Lifestyle Modification (LM)
2.4. Randomization
2.5. Outcome Measures
2.5.1. Physician-Assessed Outcomes
2.5.2. Laboratory Measures
2.5.3. PROCAM Score
2.6. Safety
2.7. Sample Size Calculation and Statistical Analysis
3. Results
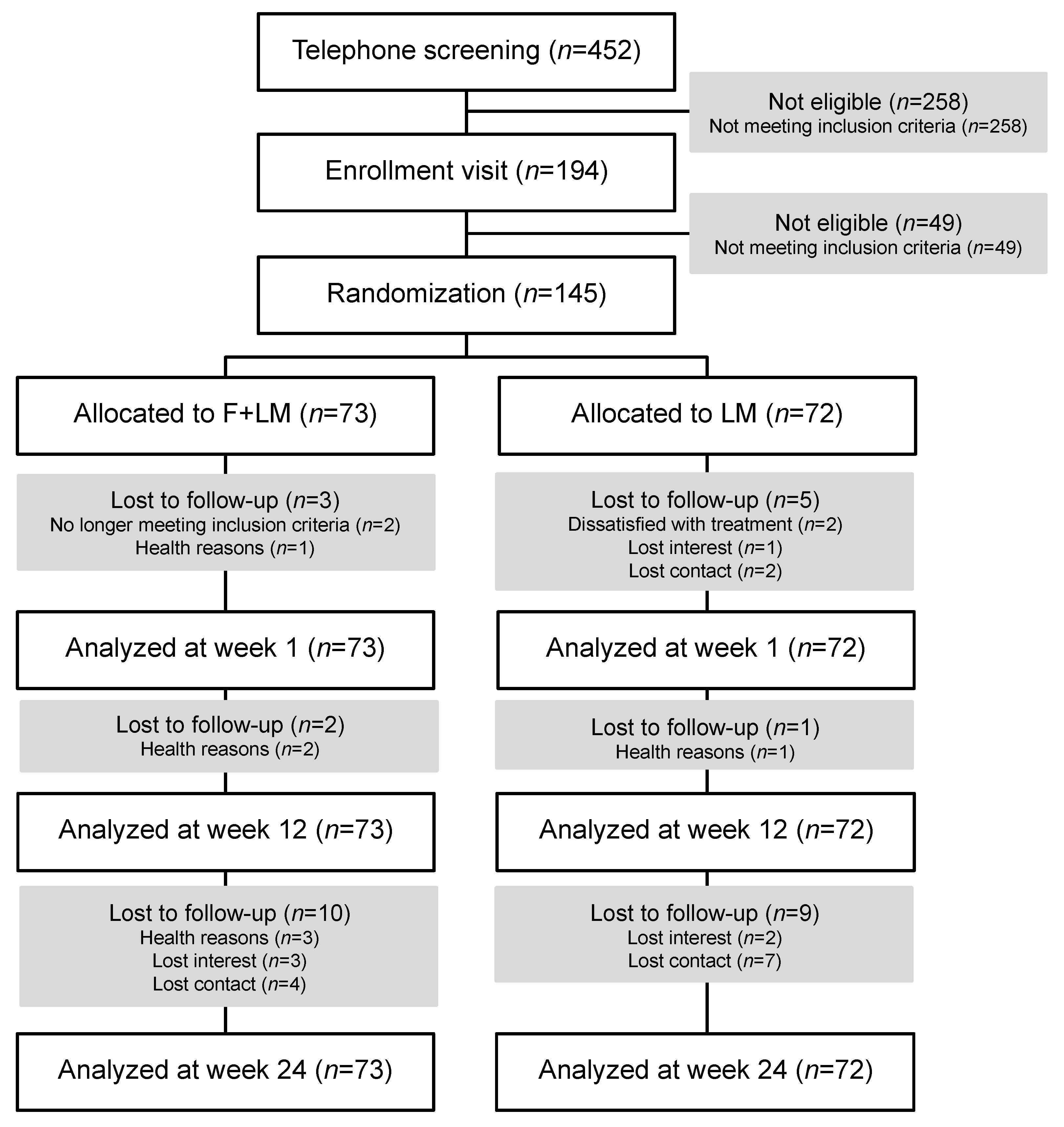
3.1. Patients
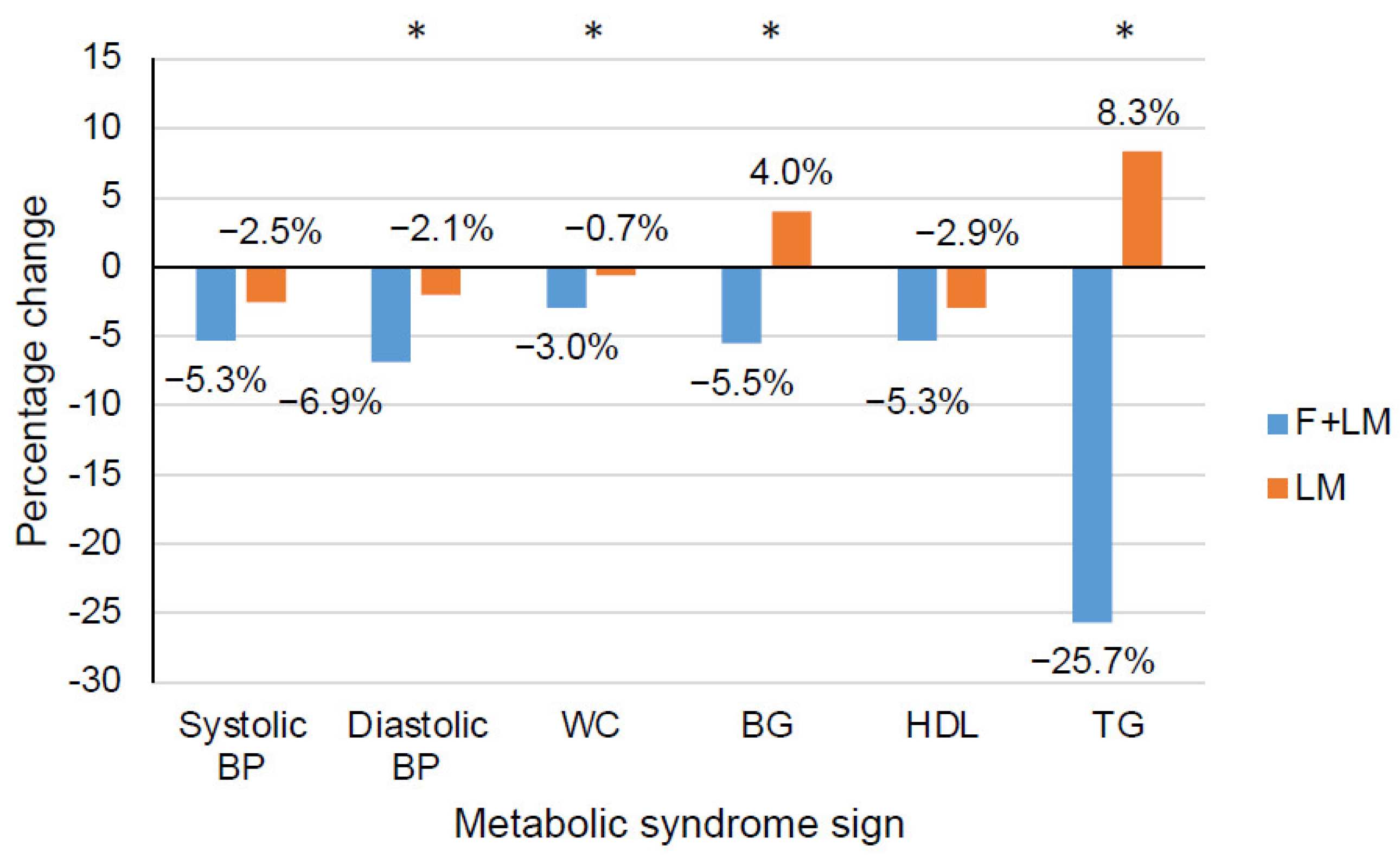
3.2. Primary Outcome Measures
3.3. Physician-Assessed Outcomes and PROCAM Score
3.4. Laboratory Parameters
3.5. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- Rosengren, A.; Hawken, S.; Ounpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthi-amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Ryden, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Champagne, C.M.; Harsha, D.W.; Cooper, L.S.; Obarzanek, E.; Elmer, P.J.; Stevens, V.J.; Vollmer, W.M.; Lin, P.H.; Svetkey, L.P.; et al. Effects of comprehensive lifestyle modification on blood pressure control: Main results of the PREMIER clinical trial. JAMA 2003, 289, 2083–2093. [Google Scholar] [PubMed]
- Ornish, D.; Brown, S.E.; Scherwitz, L.W.; Billings, J.H.; Armstrong, W.T.; Ports, T.A.; McLanahan, S.M.; Kirkeeide, R.L.; Brand, R.J.; Gould, K.L. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet 1990, 336, 129–133. [Google Scholar] [CrossRef]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Brown, S.E.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeeide, R.L.; et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef]
- Michalsen, A.; Grossman, P.; Lehmann, N.; Knoblauch, N.T.; Paul, A.; Moebus, S.; Budde, T.; Dobos, G.J. Psychological and quality-of-life outcomes from a comprehensive stress reduction and lifestyle program in patients with coronary artery disease: Results of a randomized trial. Psychother. Psychosom. 2005, 74, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Fruhbeck, G.; Ryan, D.H.; Wilding, J.P. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef]
- Elmer, P.J.; Obarzanek, E.; Vollmer, W.M.; Simons-Morton, D.; Stevens, V.J.; Young, D.R.; Lin, P.H.; Champagne, C.; Harsha, D.W.; Svetkey, L.P.; et al. Effects of comprehensive lifestyle modification on diet, weight, physical fitness, and blood pressure control: 18-month results of a randomized trial. Ann. Intern. Med. 2006, 144, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Lauche, R.; Paul, A.; Langhorst, J.; Michalsen, A.; Dobos, G. Mind-Body Medicine in the Secondary Prevention of Coronary Heart Disease. Dtsch. Arztebl. Int. 2015, 112, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Ziv, A.; Vogel, O.; Keret, D.; Pintov, S.; Bodenstein, E.; Wolkomir, K.; Doenyas, K.; Mirovski, Y.; Efrati, S. Comprehensive Approach to Lower Blood Pressure (CALM-BP): A randomized controlled trial of a multifactorial lifestyle intervention. J. Hum. Hypertens. 2013, 27, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Malinowski, B.; Zalewska, K.; Węsierska, A.; Sokołowska, M.M.; Socha, M.; Liczner, G.; Pawlak-Osińska, K.; Wiciński, M. Intermittent Fasting in Cardiovascular Disorders-An Overview. Nutrients 2019, 11, 673. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Brandhorst, S.; Shelehchi, M.; Mirzaei, H.; Cheng, C.W.; Budniak, J.; Groshen, S.; Mack, W.J.; Guen, E.; Di Biase, S.; et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Sci. Transl. Med. 2017, 9, eaai8700. [Google Scholar] [CrossRef] [PubMed]
- Jamshed, H.; Steger, F.L.; Bryan, D.R.; Richman, J.S.; Warriner, A.H.; Hanick, C.J.; Martin, C.K.; Salvy, S.-J.; Peterson, C.M. Effectiveness of Early Time-Restricted Eating for Weight Loss, Fat Loss, and Cardiometabolic Health in Adults with Obesity: A Randomized Clinical Trial. JAMA Intern. Med. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Adafer, R.; Messaadi, W.; Meddahi, M.; Patey, A.; Haderbache, A.; Bayen, S.; Messaadi, N. Food Timing, Circadian Rhythm and Chrononutrition: A Systematic Review of Time-Restricted Eating’s Effects on Human Health. Nutrients 2020, 12, 3770. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Lu, L.W.; Ge, Q.; Feng, D.; Yu, J.; Liu, B.; Zhang, R.; Zhang, X.; Ouyang, C.; Chen, F. Missing puzzle pieces of time-restricted-eating (TRE) as a long-term weight-loss strategy in overweight and obese people? A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell Metab. 2020, 31, 92–104.e105. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P.; Longo, V.D.; Harvie, M. Impact of intermittent fasting on health and disease processes. Ageing Res. Rev. 2017, 39, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity 2019, 27, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Li, C. Fasting therapy for treating and preventing disease—Current state of evidence. Forsch. Komplement. 2013, 20, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Wilhelmi de Toledo, F.; Grundler, F.; Bergouignan, A.; Drinda, S.; Michalsen, A. Safety, health improvement and well-being during a 4 to 21-day fasting period in an observational study including 1422 subjects. PLoS ONE 2019, 14, e0209353. [Google Scholar] [CrossRef]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular mechanisms and clinical applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef]
- Fontana, L. Calorie restriction and cardiometabolic health. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 3–9. [Google Scholar] [CrossRef]
- Fanti, M.; Mishra, A.; Longo, V.D.; Brandhorst, S. Time-Restricted Eating, Intermittent Fasting, and Fasting-Mimicking Diets in Weight Loss. Curr. Obes. Rep. 2021, 10, 70–80. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef]
- Dobos, G.; Paul, A. Mind-Body-Medizin—Integrative Konzepte zur Ressourcenstärkung und Lebensstilveränderung; Urban & Fischer Verlag/Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Paul, A.; Lauche, R.; Cramer, H.; Altner, N.; Dobos, G. An Integrative Day-Care Clinic for chronically ill patients: Concept and case presentation. Eur. J. Integr. Med. 2012, 4, E455–E459. [Google Scholar] [CrossRef]
- de Lorgeril, M.; Renaud, S.; Mamelle, N.; Salen, P.; Martin, J.L.; Monjaud, I.; Guidollet, J.; Touboul, P.; Delaye, J. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994, 343, 1454–1459. [Google Scholar] [CrossRef]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Mamelle, N.; Monjaud, I.; Touboul, P.; Delaye, J. Effect of a mediterranean type of diet on the rate of cardiovascular complications in patients with coronary artery disease. Insights into the cardioprotective effect of certain nutriments. J. Am. Coll. Cardiol. 1996, 28, 1103–1108. [Google Scholar] [CrossRef]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. JAMA 2004, 292, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Kempner, W. Treatment of hypertensive vascular disease with rice diet. Arch. Intern. Med. 1974, 133, 758–790. [Google Scholar] [CrossRef]
- Saghaei, M. Random allocation software for parallel group randomized trials. BMC Med. Res. Methodol. 2004, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Maifeld, A.; Bartolomaeus, H.; Löber, U.; Avery, E.G.; Steckhan, N.; Markó, L.; Wilck, N.; Hamad, I.; Šušnjar, U.; Mähler, A.; et al. Fasting alters the gut microbiome reducing blood pressure and body weight in metabolic syndrome patients. Nat. Commun. 2021, 12, 1970. [Google Scholar] [CrossRef]
- Westhoff, T.H.; Straub-Hohenbleicher, H.; Schmidt, S.; Tolle, M.; Zidek, W.; van der Giet, M. Convenience of ambulatory blood pressure monitoring: Comparison of different devices. Blood Press. Monit. 2005, 10, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Later, W.; Hitze, B.; Sato, T.; Kossel, E.; Gluer, C.C.; Heller, M.; Muller, M.J. Accuracy of bioelectrical impedance consumer devices for measurement of body composition in comparison to whole body magnetic resonance imaging and dual X-ray absorptiometry. Obes. Facts 2008, 1, 319–324. [Google Scholar] [CrossRef]
- World Health Organization. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Rudenski, A.S.; Matthews, D.R.; Levy, J.C.; Turner, R.C. Understanding “insulin resistance”: Both glucose resistance and insulin resistance are required to model human diabetes. Metab. Clin. Exp. 1991, 40, 908–917. [Google Scholar] [CrossRef]
- Assmann, G.; Cullen, P.; Schulte, H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Munster (PROCAM) study. Circulation 2002, 105, 310–315. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Haller, H.; Steckhan, N.; Michalsen, A.; Dobos, G. Effects of yoga on cardiovascular disease risk factors: A systematic review and meta-analysis. Int. J. Cardiol. 2014, 173, 170–183. [Google Scholar] [CrossRef]
- Hughes, J.W.; Fresco, D.M.; Myerscough, R.; van Dulmen, M.H.; Carlson, L.E.; Josephson, R. Randomized controlled trial of mindfulness-based stress reduction for prehypertension. Psychosom. Med. 2013, 75, 721–728. [Google Scholar] [CrossRef]
- Esposito, K.; Ciotola, M.; Giugliano, D. Mediterranean diet and the metabolic syndrome. Mol. Nutr. Food Res. 2007, 51, 1268–1274. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: New York, NY, USA, 1987. [Google Scholar]
- Schafer, J.L. Analysis of Incomplete Multivariate Data; Chapman and Hall: New York, NY, USA, 1997. [Google Scholar]
- Di Francesco, A.; Di Germanio, C.; Bernier, M.; de Cabo, R. A time to fast. Science 2018, 362, 770–775. [Google Scholar] [CrossRef]
- Li, N.; Guenancia, C.; Rigal, E.; Hachet, O.; Chollet, P.; Desmoulins, L.; Leloup, C.; Rochette, L.; Vergely, C. Short-term moderate diet restriction in adulthood can reverse oxidative, cardiovascular and metabolic alterations induced by postnatal overfeeding in mice. Sci. Rep. 2016, 6, 30817. [Google Scholar] [CrossRef]
- National Kidney Foundation. Estimated Glomerular Filtration Rate (eGFR). Available online: https://www.kidney.org/atoz/content/gfr (accessed on 12 June 2022).
- de Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 145) | F + LM (n = 73) | LM (n = 72) | |
|---|---|---|---|
| Sociodemographic characteristics | |||
| Gender female n (%) | 91 (62.8%) | 48 (65.8%) | 43 (59.7%) |
| Age years | 59.7 ± 9.3 | 58.6 ± 10.8 | 60.8 ± 7.5 |
| Marital status n (%) | |||
| Single | 15 (10.3%) | 6 (8.2%) | 9 (12.5%) |
| Married | 98 (67.6%) | 49 (67.1%) | 49 (68.1%) |
| Divorced | 21 (14.5%) | 12 (16.4%) | 9 (12.5%) |
| Widowed | 5 (3.4%) | 3 (4.1%) | 2 (2.8%) |
| Education n (%) | |||
| Secondary modern school (“Hauptschule”) qualification | 25 (17.2%) | 9 (12.3%) | 16 (22.2%) |
| High school (“Realschule”) qualification | 41 (28.3%) | 19 (26.0%) | 22 (30.6%) |
| A level (“Abitur”) | 18 (12.4%) | 12 (16.4%) | 6 (8.3%) |
| University degree | 53 (36.6%) | 28 (38.3%) | 25 (34.7%) |
| Employment n (%) | |||
| Employed full-time | 41 (28.3%) | 20 (27.4%) | 21 (29.2%) |
| Employed part-time | 19 (13.1%) | 11 (15.1%) | 8 (11.1%) |
| Occasionally | 5 (3.4%) | 3 (4.1%) | 2 (2.8%) |
| On sick leave | 3 (2.1%) | 2 (2.7%) | 1 (1.4%) |
| Unemployed | 3 (2.1%) | 2 (2.7%) | 1 (1.4%) |
| Retired age-related | 44 (30.3%) | 20 (27.4%) | 24 (33.3%) |
| Retired health-related | 15 (10.3%) | 7 (9.6%) | 8 (11.1%) |
| Homekeeper | 10 (6.9%) | 6 (8.2%) | 4 (5.6%) |
| Clinical characteristics | |||
| Weight kg | 97.0 ± 15.8 | 98.1 ± 16.1 | 95.9 ± 15.5 |
| Body Mass Index kg/m2 | 33.3 ± 4.5 | 33.7 ± 4.5 | 32.84.5 |
| Diagnosis of obesity since months | 65.0 ± 123.6 | 73.3 ± 140.7 | 56.5 ± 103.8 |
| Diagnosis of hypertension since months | 119.5 ± 112.4 | 119.3 ± 113.8 | 119.7 ± 111.8 |
| Antihypertensive drugs since months | 106.0 ± 108.6 | 98.7 ± 101.7 | 113.4 ± 115.4 |
| Diagnosis of coronary artery disease n (%) | 5 (3.4%) | 2 (2.7%) | 3 (4.2%) |
| Diagnosis of peripheral artery disease n (%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Diagnosis of hyperlipidemia since months | 62.2 ± 83.1 | 63.7 ± 91.9 | 60.7 ± 73.9 |
| Lipid-lowering drugs since months | 30.4 ± 59.0 | 28.3 ± 56.9 | 32.6 ± 61.4 |
| Diagnosis of hyperglycemia since months | 11.5 ± 39.0 | 10.2 ± 32.6 | 12.7 ± 44.8 |
| Anti-hyperglycemic drugs since months | 17.2 ± 36.1 | 9.0 ± 24.8 | 25.6 ± 43.3 |
| Bariatric surgery n (%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Outcome | Group | Week 0 | Week 1 | Week 1 | Week 12 | Week 12 | Week 24 | Week 24 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group Difference (95% CI) | p | Group Difference (95% CI) | p | Group Difference (95% CI) | p | ||||||
| Ambulatory systolic BP | F + LM | 131.1 ± 9.1 | NA | NA | NA | 126.9 ± 8.9 | −0.5 (−5.0, 3.9) | 0.813 | 130.0 ± 9.0 | −1.2 (−5.6, 2.1) | 0.366 |
| LM | 132.5 ± 11.0 | NA | 129.3 ± 10.8 | 130.7 ± 9.7 | |||||||
| Ambulatory diastolic BP | F + LM | 80.1 ± 8.2 | NA | NA | NA | 78.4 ± 8.2 | −1.3 (−4.8, 2.1) | 0.450 | 79.1 ± 7.6 | −1.0 (−4.2, 2.3) | 0.501 |
| LM | 82.0 ± 8.3 | NA | 80.2 ± 8.7 | 80.6 ± 8.5 | |||||||
| Clinical systolic BP | F + LM | 138.9 ± 14.4 | 130.9 ± 16.1 | −4.1 (−11.3, 3.2) | 0.270 | 133.7 ± 13.5 | 1.6 (−4.4, 7.5) | 0.609 | 138.3 ± 14.4 | 2.5 (−3.6, 8.5) | 0.417 |
| LM | 141.2 ± 19.0 | 136.2 ± 14.5 | 134.5 ± 12.3 | 135.2 ± 10.8 | |||||||
| Clinical diastolic BP | F + LM | 88.3 ± 10.6 | 81.5 ± 9.7 | −4.8 (−9.6, −0.06) | 0.047 | 86.5 ± 11.2 | 3.4 (−0.7, 7.5) | 0.106 | 88.7 ± 10.3 | −2.7 (−6.8, 1.4) | 0.200 |
| LM | 89.5 ± 11.2 | 87.0 ± 11.1 | 86.7 ± 8.7 | 87.7 ± 8.8 | |||||||
| Weight | F + LM | 98.1 ± 16.1 | 93.2 ± 15.2 | −4.8 (−5.5, −4.1) | <0.001 | 92.8 ± 15.4 | −3.5 (−5.1, −1.8) | <0.001 | 93.3 ± 15.5 | −2.7 (−4.8, −0.5) | 0.014 |
| LM | 95.9 ± 15.5 | 95.8 ± 15.3 | 94.3 ± 15.1 | 93.8 ± 15.1 | |||||||
| Body Mass Index | F + LM | 33.7 ± 4.5 | 32.1 ± 4.3 | −1.7 (−2.0, −1.4) | <0.001 | 31.9 ± 4.3 | −1.3 (−1.9, −0.7) | <0.001 | 32.1 ± 4.4 | −1.0 (−1.8, −0.3) | 0.007 |
| LM | 32.8 ± 4.5 | 32.8 ± 4.4 | 32.3 ± 4.4 | 32.1 ± 4.3 | |||||||
| Waist circumference | F + LM | 114.1 ± 10.5 | 110.7 ± 11.2 | −2.6 (−5.0, −0.2) | 0.035 | 108.2 ± 11.5 | −3.5 (−5.8, −1.1) | 0.004 | 108.9 ± 10.9 | −1.2 (−6.3, 3.9) | 0.633 |
| LM | 112.1 ± 11.1 | 111.3 ± 11.1 | 109.4 ± 10.9 | 107.2 ± 16.5 | |||||||
| Waist/hip Ratio | F + LM | 1.0 ± 0.5 | 1.0 ± 0.1 | −0.01 (−0.05, 0.03) | 0.486 | 1.0 ± 0.1 | −0.03 (−0.06, 0.01) | 0.192 | 1.0 ± 0.1 | −0.01 (−0.06, 9.04) | 0.658 |
| LM | 1.0 ± 0.2 | 1.0 ± 0.1 | 1.0 ± 0.1 | 1.0 ± 0.1 | |||||||
| Body fat percentage | F + LM | 41.5 ± 8.9 | 42.0 ± 9.1 | 0.6 (−0.8, 1.9) | 0.420 | 39.4 ± 8.9 | −2.2 (−3.4, 0.9) | 0.001 | 40.1 ± 9.2 | −1.0 (−2.6, 0.6) | 0.214 |
| LM | 39.4 ± 8.6 | 39.9 ± 8.6 | 39.2 ± 8.7 | 39.1 ± 8.8 | |||||||
| PROCAM Score | F + LM | 48.4 ± 13.6 | 45.4 ± 13.2 | −2.4 (−5.6, 0.8) | 0.139 | 45.8 ± 13.4 | −3.4 (−6.7, −0.2) | 0.048 | 47.3 ± 12.7 | −2.0 (−5.5, 1.4) | 0.242 |
| LM | 50.1 ± 11.8 | 50.9 ± 13.2 | 49.7 ± 12.9 | 50.0 ± 11.6 | |||||||
| 10-year coronary risk | F + LM | 14.9 ± 12.6 | 12.1 ± 11.2 | −4.9 (−9.5, −0.4) | 0.033 | 12.6 ± 11.8 | −6.2 (−10.3, −2.0) | 0.004 | 13.7 ± 12.0 | −3.8 (−8.2, 0.5) | 0.080 |
| LM | 16.0 ± 13.6 | 17.4 ± 15.2 | 15.5 ± 12.9 | 15.8 ± 12.5 | |||||||
| Outcome | Group | Week 0 | Week 1 | Week 1 | Week 12 | Week 12 | Week 24 | Week 24 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group Difference (95% CI) | p | Group Difference (95% CI) | p | Group Difference (95% CI) | p | ||||||
| HOMA index | F + LM | 3.5 ± 2.5 | 2.0 ± 1.6 | −0.8 (−1.7, −0.1) | 0.046 | 3.2 ± 2.2 | 0.2 (−0.7, 1.1) | 0.676 | 3.0 ± 1.9 | −0.2 (−0.9, 0.6) | 0.639 |
| LM | 3.7 ± 2.4 | 3.4 ± 2.3 | 3.4 ± 2.2 | 3.6 ± 2.0 | |||||||
| Blood glucose | F + LM | 113.3 ± 18.9 | 107.0 ± 18.3 | −10.3 (−19.0, −1.6) | 0.022 | 106.2 ± 13.4 | −7.7 (−17.2, 1.9) | 0.113 | 110.5 ± 12.8 | −7.7 (−13.5, −1.8) | 0.011 |
| LM | 110.1 ± 22.0 | 114.4 ± 26.9 | 109.3 ± 24.4 | 111.5 ± 20.3 | |||||||
| Blood insulin | F + LM | 12.4 ± 7.3 | 8.0 ± 5.4 | −2.9 (−5.3, −0.4) | 0.024 | 11.6 ± 6.6 | 0.9 (−1.4, 3.3) | 0.428 | 10.9 ± 5.9 | −0.5 (−2.7, 1.7) | 0.641 |
| LM | 13.0 ± 7.5 | 12.4 ± 7.0 | 11.9 ± 5.9 | 12.4 ± 5.7 | |||||||
| HbA1c | F + LM | 5.9 ± 0.5 | 5.8 ± 0.5 | −0.2 (−0.4, −0.05) | 0.010 | 5.8 ± 0.5 | −0.08 (−0.3, 0.1) | 0.485 | 5.9 ± 0.4 | −0.2 (−0.4, 0.04) | 0.122 |
| LM | 5.9 ± 0.7 | 6.0 ± 0.7 | 5.9 ± 0.7 | 6.0 ± 0.7 | |||||||
| Total cholesterol | F + LM | 224.4 ± 50.0 | 208.4 ± 47.6 | −6.9 (−25.3, 11.5) | 0.458 | 214.3 ± 40.6 | −4.0 (−19.7, 11.7) | 0.616 | 227.7 ± 39.9 | 9.5 (−9.7, 27.9) | 0.339 |
| LM | 224.3 ± 48.3 | 224.9 ± 47.5 | 212.8 ± 42.2 | 216.8 ± 42.0 | |||||||
| HDL cholesterol | F + LM | 53.4 ± 16.0 | 49.2 ± 12.0 | −1.1 (−4.4, 2.3) | 0.531 | 53.4 ± 14.7 | 3.3 (−1.0, 7.7) | 0.134 | 55.3 ± 13.3 | 5.1 (1.5, 8.8) | 0.007 |
| LM | 56.6 ± 19.0 | 54.1 ± 16.0 | 53.1 ± 15.7 | 53.5 ± 15.1 | |||||||
| LDL cholesterol | F + LM | 140.2 ± 37.3 | 134.1 ± 40.3 | −0.9 (−16.3, 14.5) | 0.904 | 135.2 ± 34.5 | −3.6 (−17.1, 9.9) | 0.598 | 144.9 ± 32.1 | 7.1 (−7.7, 21.9) | 0.344 |
| LM | 139.6 ± 43.5 | 142.3 ± 42.6 | 132.8 ± 37.4 | 137.8 ± 37.5 | |||||||
| Triglyceride | F + LM | 188.0 ± 210.6 | 116.4 ± 53.9 | −48.9 (−81.0, −16.9) | 0.003 | 157.4 ± 89.5 | −23.0 (−58.2, 12.1) | 0.197 | 157.3 ± 93.9 | −21.9 (−59.4, 15.6) | 0.250 |
| LM | 175.5 ± 111.1 | 169.9 ± 93.4 | 175.3 ± 101.9 | 161.0 ± 78.4 | |||||||
| Uric acid | F + LM | 6.3 ± 1.7 | 8.0 ± 2.2 | 1.0 (0.1, 1.9) | 0.026 | 6.3 ± 1.6 | −0.1 (−0.9, 0.6) | 0.710 | 6.2 ± 1.6 | 0.1 (−0.5, 0.7) | 0.650 |
| LM | 6.6 ± 1.5 | 6.7 ± 1.7 | 6.2 ± 1.5 | 6.2 ± 1.2 | |||||||
| Creatinine | F + LM | 0.9 ± 0.2 | 1.0 ± 0.2 | 0.04 (−0.05, 0.1) | 0.383 | 0.9 ± 0.2 | −0.03 (−0.1, 0.04) | 0.354 | 0.8 ± 0.2 | −0.04 (−0.1, 0.02) | 0.187 |
| LM | 0.9 ± 0.2 | 0.9 ± 0.2 | 0.9 ± 0.2 | 0.9 ± 0.2 | |||||||
| eGFR | F + LM | 83.5 ± 15.7 | 73.4 ± 17.5 | −11.9 (−21.8, −2.0) | 0.019 | 85.8 ± 13.6 | 1.4 (−6.4, 9.1) | 0.728 | 86.6 ± 14.6 | 2.4 (−6.1, 11.0) | 0.577 |
| LM | 82.4 ± 14.5 | 81.5 ± 14.5 | 82.9 ± 13.6 | 82.1 ± 12.2 | |||||||
| CRP | F + LM | 0.4 ± 0.4 | 0.5 ± 0.4 | 0.03 (−0.1, 0.2) | 0.677 | 0.4 ± 0.5 | 0.04 (−0.1, 0.2) | 0.628 | 0.4 ± 0.5 | 0.2 (0.03, 0.4) | 0.024 |
| LM | 0.3 ± 0.3 | 0.4 ± 0.3 | 0.3 ± 0.3 | 0.4 ± 0.3 | |||||||
| IGF-1 | F + LM | 119.9 ± 38.1 | 104.1 ± 40.6 | −13.6 (−28.8, 1.5) | 0.077 | 123.7 ± 38.6 | −7.6 (−20.2, 5.0) | 0.235 | 126.5 ± 40.6 | 2.4 (−11.7, 16.6) | 0.736 |
| LM | 126.2 ± 48.2 | 120.0 ± 44.2 | 129.9 ± 43.7 | 128.4 ± 43.7 | |||||||
| IL-6 | F + LM | 3.1 ± 2.0 | 2.8 ± 2.7 | −1.2 (−2.5, −0.005) | 0.049 | 3.4 ± 4.7 | −1.5 (−3.5, 0.5) | 0.149 | 2.9 ± 1.7 | −0.5 (−1.5, 0.6) | 0.358 |
| LM | 2.8 ± 2.2 | 3.1 ± 2.8 | 3.7 ± 4.2 | 3.2 ± 1.6 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cramer, H.; Hohmann, C.; Lauche, R.; Choi, K.-E.; Schneider, N.; Steckhan, N.; Rathjens, F.; Anheyer, D.; Paul, A.; von Scheidt, C.; et al. Effects of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 4751. https://doi.org/10.3390/jcm11164751
Cramer H, Hohmann C, Lauche R, Choi K-E, Schneider N, Steckhan N, Rathjens F, Anheyer D, Paul A, von Scheidt C, et al. Effects of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(16):4751. https://doi.org/10.3390/jcm11164751
Chicago/Turabian StyleCramer, Holger, Christoph Hohmann, Romy Lauche, Kyung-Eun (Anna) Choi, Nadia Schneider, Nico Steckhan, Florian Rathjens, Dennis Anheyer, Anna Paul, Christel von Scheidt, and et al. 2022. "Effects of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 16: 4751. https://doi.org/10.3390/jcm11164751