
Short-Term Outcomes of Surgery and Rehabilitation on Activities of Daily Living after Displaced Femoral Neck Fractures: Structural Equation Modeling



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takusari, E.; Sakata, K.; Hashimoto, T.; Fukushima, Y.; Nakamura, T.; Orimo, H. Trends in hip fracture incidence in Japan: Estimates based on nationwide hip fracture surveys from 1992 to 2017. JBMR Plus 2020, 5, e10428. [Google Scholar] [CrossRef] [PubMed]
- The Japanese Orthopaedic Association; Japanese Society for Fracture Repair. Japanese Orthopedic Association Clinical Practice Guideline on the Management of Hip Fractures, 3rd ed.; Nankodo: Tokyo, Japan, 2021. [Google Scholar]
- Xu, B.Y.; Yan, S.; Low, L.L.; Vasanwala, F.F.; Low, S.G. Predictors of poor functional outcomes and mortality in patients with hip fracture: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 568. [Google Scholar] [CrossRef] [PubMed]
- Hou, M.; Zhang, Y.; Chen, A.C.; Liu, T.; Yang, H.; Zhu, X.; He, F. The effects of dementia on the prognosis and mortality of hip fracture surgery: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 3161–3172. [Google Scholar] [CrossRef] [PubMed]
- Hulsbæk, S.; Juhl, C.; Røpke, A.; Bandholm, T.; Kristensen, M.T. Exercise therapy is effective at improving short- and long-term mobility, activities of daily living, and balance in older patients following hip fracture: A systematic review and meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Hagino, H.; Endo, N.; Harada, A.; Iwamoto, J.; Mashiba, T.; Mori, S.; Ohtori, S.; Sakai, A.; Takada, J.; Yamamota, T. Survey of hip fractures in Japan: Recent trends in prevalence and treatment. J. Orthop. Sci. 2017, 22, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.G.; Wenn, R.T.; Sikand, M.; Taylor, A.M. Early mortality after hip fracture: Is delay before surgery important? J. Bone Joint Surg. Am. 2005, 87, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Siegmeth, A.W.; Gurusamy, K.; Parker, M.J. Delay to surgery prolongs hospital stay in patients with fractures of the proximal femur. J. Bone Joint Surg. Br. 2005, 87, 1123–1126. [Google Scholar] [CrossRef] [PubMed]
- Novack, V.; Jotkowitz, A.; Etzion, O.; Porath, A. Does delay in surgery after hip fracture lead to worse outcomes? A multicenter survey. Int. J. Qual. Health Care 2007, 19, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, E.L.; Sternheim, A.; Kadar, A.; Sagi, Y.; Sherer, Y.; Chechik, O. Early operative intervention is associated with better patient survival in patients with intracapsular femur fractures but not extracapsular fractures. J. Arthroplast. 2014, 29, 1072–1075. [Google Scholar] [CrossRef] [PubMed]
- Crego-Vita, D.; Sanchez-Perez, C.; Gomez-Rico, J.A.; de Arriba, C.C. Intracapsular hip fractures in the elderly. Do we know what is important? Injury 2017, 48, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Blomfeldt, R.; Törnkvist, H.; Eriksson, K.; Söderqvist, A.; Ponzer, S.; Tidermark, J. A randomised controlled trial comparing bipolar hemiarthroplasty with total hip replacement for displaced intracapsular fractures of the femoral neck in elderly patients. J. Bone Joint Surg. Br. 2007, 89, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.J.; Gurusamy, K.S.; Azegami, S. Arthroplasties (with and without bone cement) for proximal femoral fractures in adults. Cochrane Database Syst. Rev. 2010, 6, CD001706. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and profile of Diagnosis Procedure Combination (DPC): Development of a real data collection system for acute inpatient care in Japan. J. Epidemiol. 2021, 31, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hartigan, I. A comparative review of the Katz ADL and the Barthel Index in assessing the activities of daily living of older people. Int. J. Older People Nurs. 2007, 2, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Penoni, D.C.; Vettore, M.V.; Torres, S.R.; Farias, M.L.F.; Leão, A.T.T. An investigation of the bidirectional link between osteoporosis and periodontitis. Arch. Osteoporos. 2019, 14, 94. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.; Shin, J.Y.; Yee, J.; Park, T.; Park, M. Structural equation modeling for hypertension and type 2 diabetes based on multiple SNPs and multiple phenotypes. PLoS ONE 2019, 14, e0217189. [Google Scholar] [CrossRef] [PubMed]
- Orimo, H.; Yaegashi, Y.; Hosoi, T.; Fukushima, Y.; Onoda, T.; Hashimoto, T.; Sakata, K. Hip fracture incidence in Japan: Estimates of new patients sin 2012 and 25-year trends. Osteoporos. Int. 2016, 27, 1777–1784. [Google Scholar] [CrossRef] [PubMed]
- Uhler, L.M.; Schultz, W.R.; Hill, A.D.; Koenig, K.M. Health Utility of Early Hemiarthroplasty vs. Delayed Total Hip Arthroplasty for Displaced Femoral Neck Fracture in Elderly Patients: A Markov Model. J. Arthroplast. 2017, 32, 1434–1438. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Einhorn, T.A.; Guyatt, G.; Schemitsch, E.H.; Zura, R.D.; Sprague, S.; Frihagen, F.; Guerra-Farfán, E.; Kleinlugtenbelt, Y.V.; Poolman, R.W.; et al. Total hip arthroplasty or hemiarthroplasty for hip fracture. N. Engl. J. Med. 2019, 381, 2199–2208. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| BHA (n = 223) | THA (n = 38) | p-Value | |
|---|---|---|---|
| Length of hospital stay, mean (SD) | 29.5 (16.8) | 26.7 (11.1) | 0.308 |
| Days from admission to surgery, mean (SD) | 4.0 (4.4) | 6.9 (4.4) | <0.001 |
| Number of rehabilitation units per day, mean (SD) | 1.5 (0.3) | 1.6 (0.3) | 0.037 |
| Age, mean (SD) | 84.5 (6.4) | 66.3 (9.8) | <0.001 |
| Female, n (%) | 170 (76.2) | 27 (71.1) | 0.541 |
| Patient with dementia, n (%) | 120 (53.8) | 5 (13.2) | <0.001 |
| BI on admission, mean (SD) | 15.6 (16.3) | 30.5 (23.4) | <0.001 |
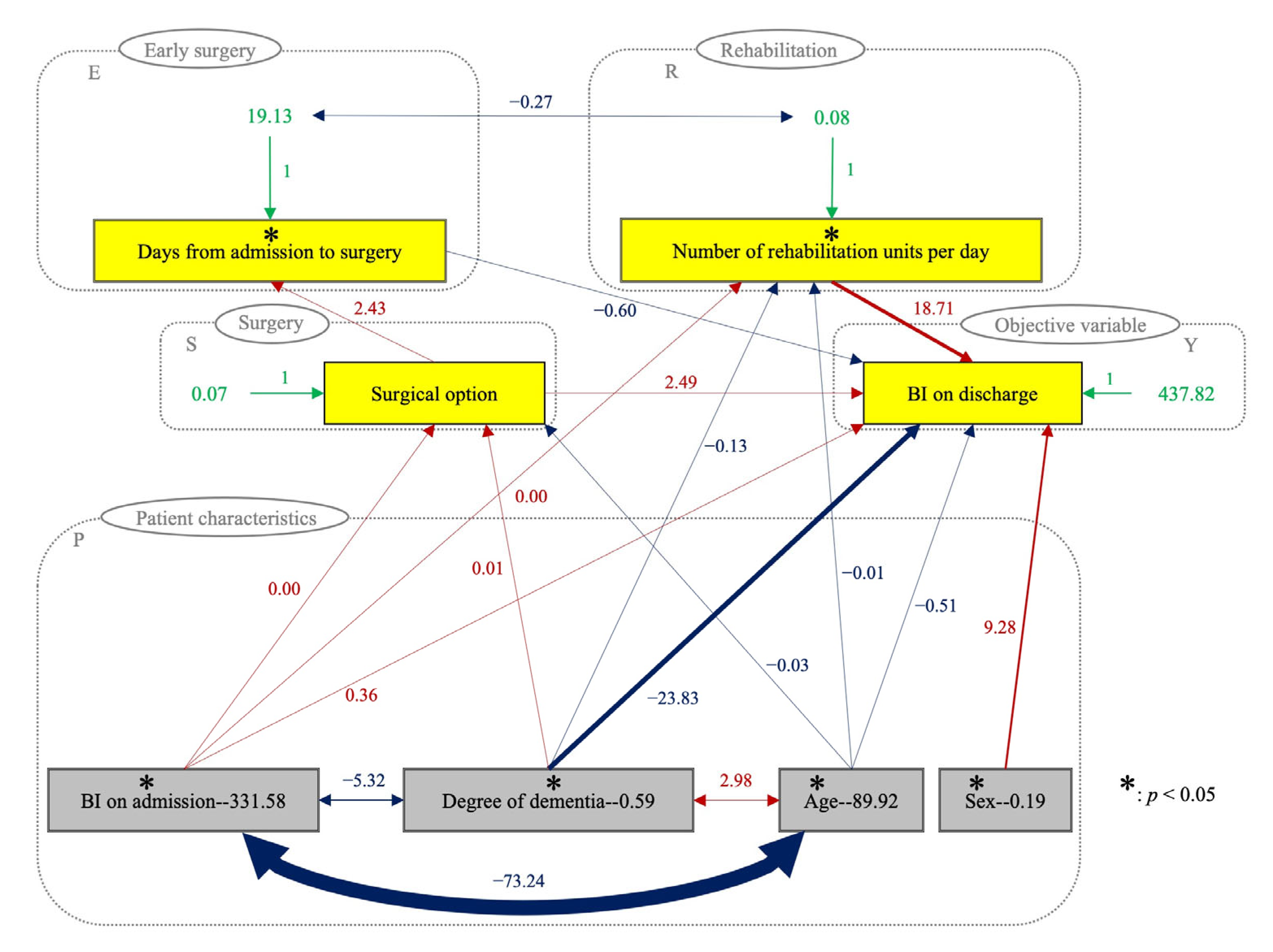
| Explanatory Variables | B a | SE | β b | p-Value c | VIF |
|---|---|---|---|---|---|
| (Constant) | 61.37 | 25.57 | 0.00 | 0.017 | |
| X1: age | −0.51 | 0.21 | −0.14 | 0.018 | 2.37 |
| X2: sex | 9.28 | 3.06 | 0.11 | 0.003 | 1.01 |
| X3: degree of dementia | −23.83 | 2.04 | −0.51 | <0.001 | 1.41 |
| X4: BI on admission | 0.36 | 0.08 | 0.18 | <0.001 | 1.36 |
| X5: days from admission to surgery | −0.60 | 0.31 | −0.08 | 0.056 | 1.14 |
| X6: surgical option | 2.49 | 5.24 | 0.02 | 0.635 | 1.98 |
| X7: number of rehabilitation units per day | 18.71 | 4.86 | 0.17 | <0.001 | 1.49 |
| X1 | X2 | X3 | X4 | X5 | X6 | X7 | |
|---|---|---|---|---|---|---|---|
| X1 | 1.000 † | ||||||
| X2 | 0.038 | 1.000 † | |||||
| X3 | 0.411 † | 0.002 | 1.000 † | ||||
| X4 | −0.424 † | −0.026 | −0.381 † | 1.000 † | |||
| X5 | −0.125 * | −0.071 | 0.050 | −0.067 | 1.000 † | ||
| X6 | −0.680 † | −0.043 | −0.271 † | 0.290 † | 0.222 † | 1.000 † | |
| X7 | −0.375 † | −0.005 | −0.442 † | 0.376 † | −0.208 † | 0.130 * | 1.000 † |
| Characteristics | Direct | Indirect | Total | p-Value |
|---|---|---|---|---|
| X1: age | −0.51 | −0.15 | −0.66 | 0.013 |
| X2: sex | 9.28 | 9.28 | 0.002 | |
| X3: degree of dementia | −23.8 | −2.3 | −26.1 | <0.001 |
| X4: BI on admission | 0.36 | 0.06 | 0.42 | <0.001 |
| X5: days from admission to surgery | −0.60 | −0.60 | 0.049 | |
| X6: surgical option | 2.49 | −1.46 | 1.03 | 0.623 |
| X7: number of rehabilitation units per day | 18.7 | 18.7 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yokoyama, K.; Katoh, H.; Bito, S.; Fujita, Y.; Yamauchi, K. Short-Term Outcomes of Surgery and Rehabilitation on Activities of Daily Living after Displaced Femoral Neck Fractures: Structural Equation Modeling. J. Clin. Med. 2023, 12, 1234. https://doi.org/10.3390/jcm12031234
Yokoyama K, Katoh H, Bito S, Fujita Y, Yamauchi K. Short-Term Outcomes of Surgery and Rehabilitation on Activities of Daily Living after Displaced Femoral Neck Fractures: Structural Equation Modeling. Journal of Clinical Medicine. 2023; 12(3):1234. https://doi.org/10.3390/jcm12031234
Chicago/Turabian StyleYokoyama, Kazutaka, Hiroyuki Katoh, Seiji Bito, Yoshinari Fujita, and Keita Yamauchi. 2023. "Short-Term Outcomes of Surgery and Rehabilitation on Activities of Daily Living after Displaced Femoral Neck Fractures: Structural Equation Modeling" Journal of Clinical Medicine 12, no. 3: 1234. https://doi.org/10.3390/jcm12031234