
Whole-Body Vibration Impacts on the Degree of Toe Angle and Its Correlation to the Knee Osteoarthritis Index during Level Walking among Female University Students: A Randomized Controlled Trial
 , , ,
, , ,  and
and
Abstract
:1. Background
2. Methods
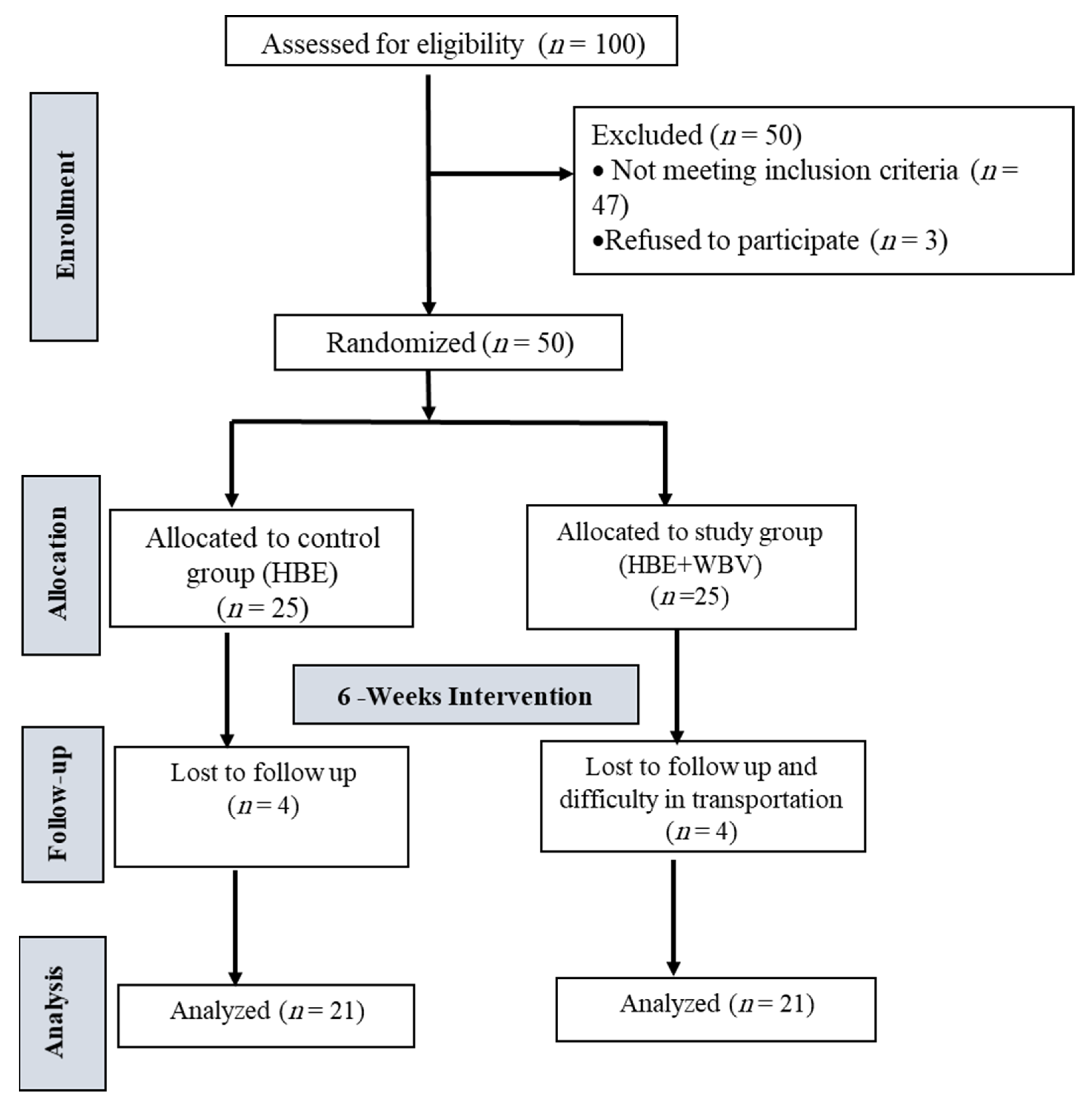
2.1. Design and Setting
2.2. Procedures
Sample Size Calculation
2.3. Participants
2.4. Randomization
3. Outcome Measures
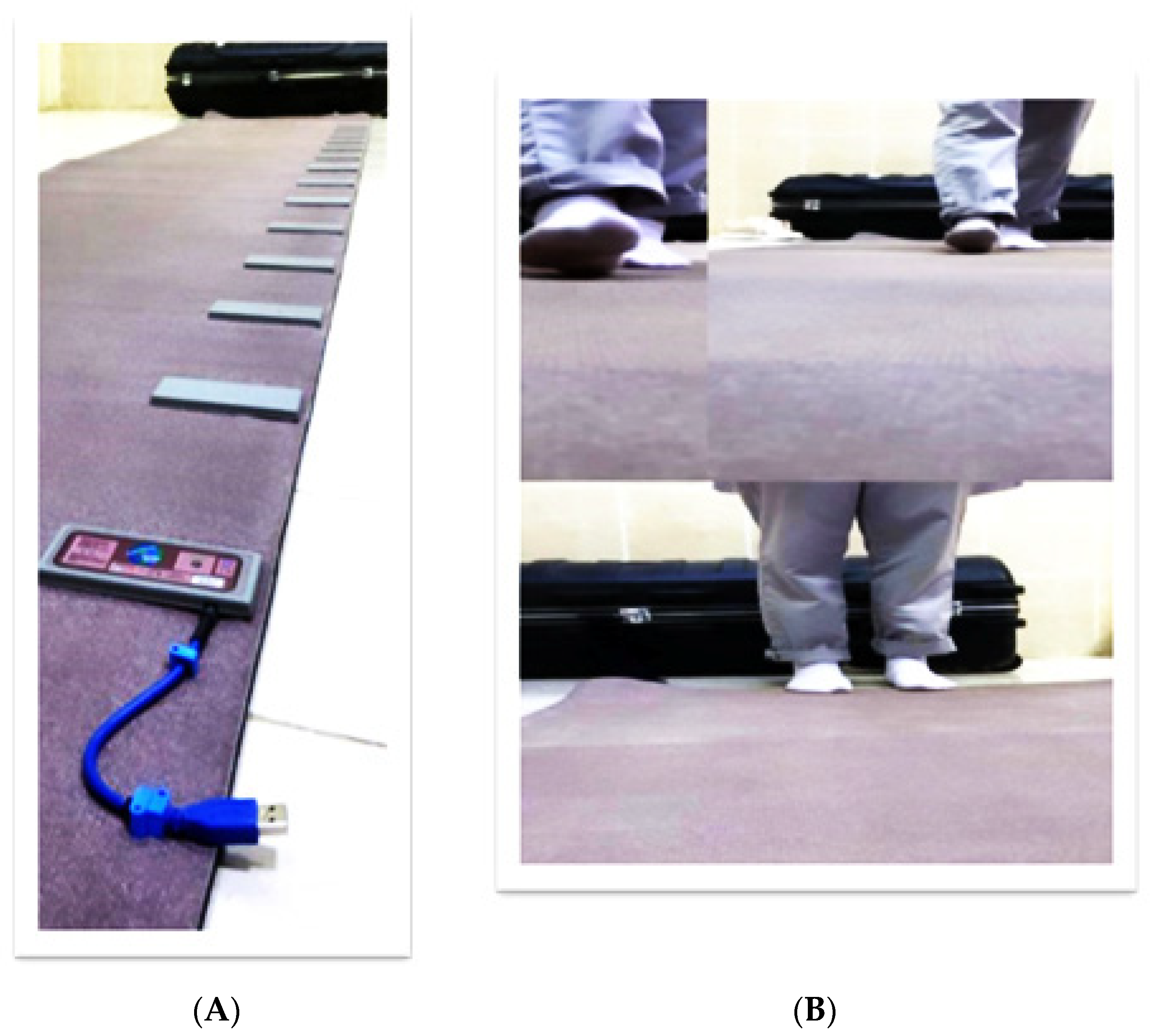
3.1. Primary Outcome
3.2. Secondary Outcome
4. Intervention
4.1. Whole-Body Vibration (WBV) Device
4.2. Home-Based Exercise
5. Statistical Analysis
6. Results
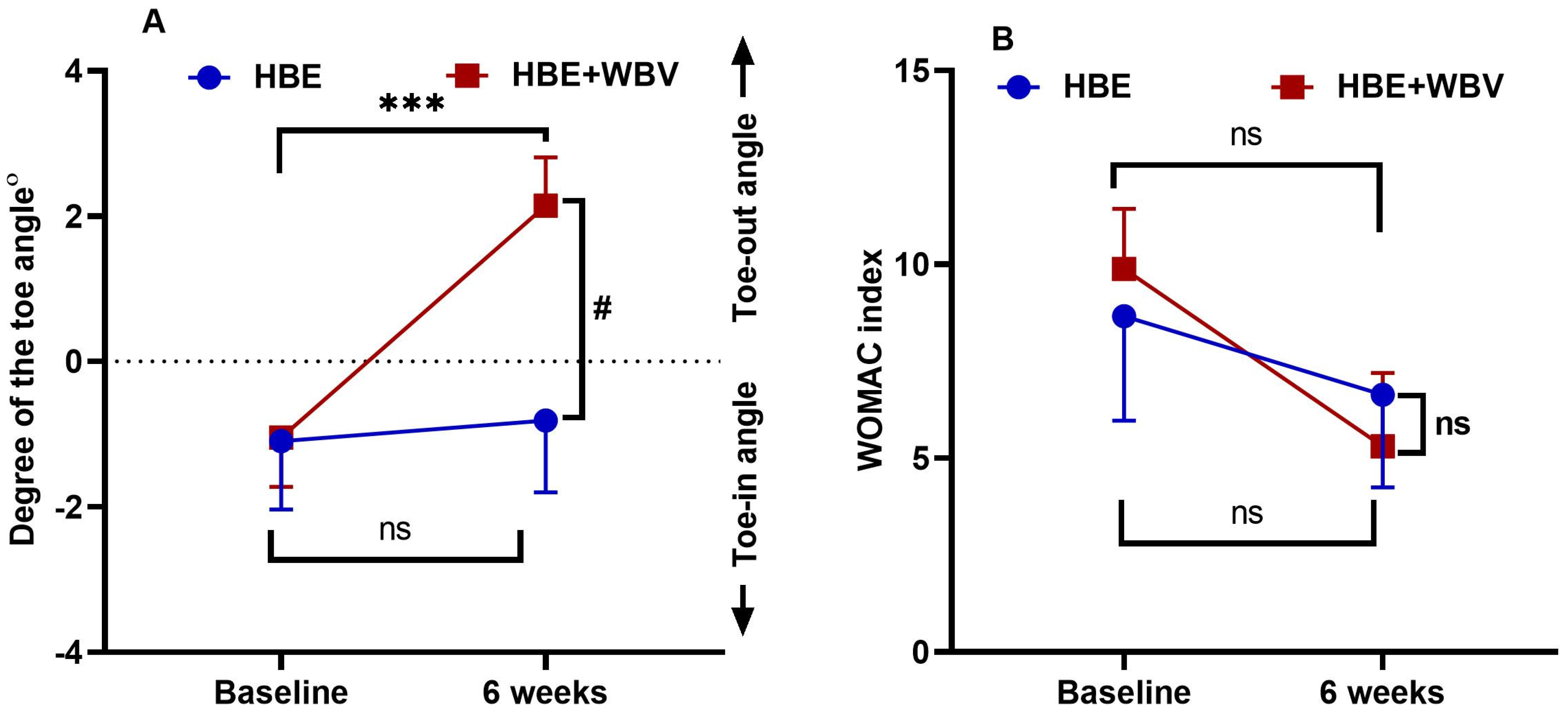
6.1. Toe Angle and WOMAC Index
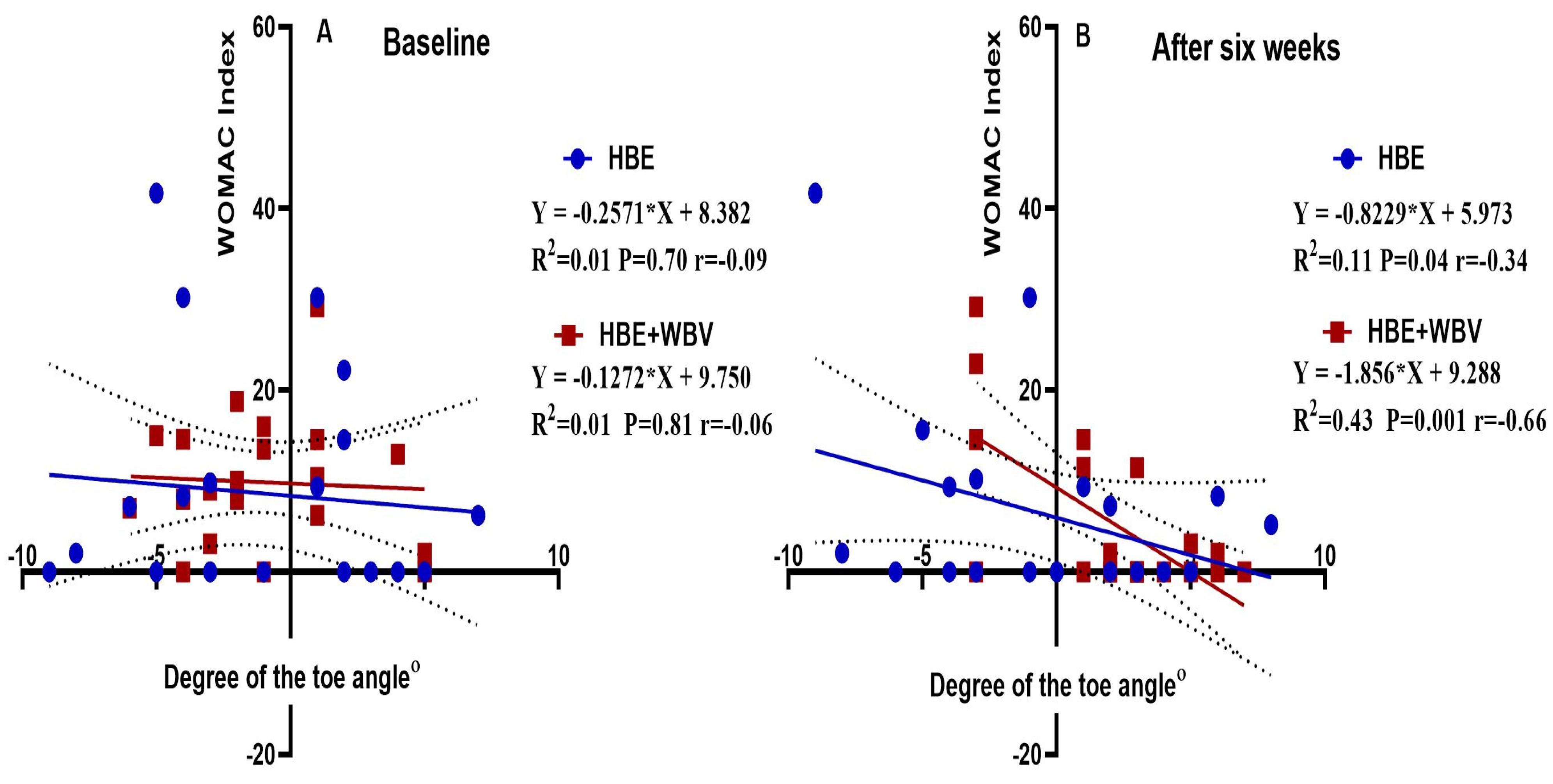
6.2. Correlation between Toe Angle and WOMAC Index
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| WBV | Whole-body vibration |
| HBE | Home-based exercise |
| WOMAC index | Western Ontario and McMaster osteoarthritis index |
| CONSORT | Consolidated Standards of Reporting Trials |
| MKS | Microsoft Kinect Sensor |
| OA | Osteoarthritis |
| GEE | Generalized estimating equations |
| η2 | eta squared |
References
- Chung, K.; Chung, H.; Halliday, N. Gross Anatomy, Board review series; 7th ed.; Lippincott Williams & Willkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Abd-Eltawab, A.E.; Ameer, M.A.; Eladl, M.A.; El-Sherbiny, M.; Ebrahim, H.A.; Elsherbini, D.M.A. Sexual dimorphism impact on the ground reaction force acting on the mediolateral direction during Level walking: Hip abductor muscle biomechanics and its correlation to GRF moment arm. Front. Bioeng. Biotechnol. 2022, 10, 863194. [Google Scholar] [CrossRef] [PubMed]
- Al-kharaz, A.A.; Chong, A.K. Gender differences in ankle kinematics of adults during gait. J. Sex-Gend.-Specif. Med. 2022, 8, 147–153. [Google Scholar]
- Ristolainen, L.; Heinonen, A.; Waller, B.; Kujala, U.M.; Kettunen, J.A. Gender differences in sport injury risk and types of inju-ries: A retrospective twelve-month study on cross-country skiers, swimmers, long-distance runners and soccer players. J. Sports Sci. Med. 2009, 8, 443–451. [Google Scholar] [PubMed]
- Quatman, C.E.; Ford, K.R.; Myer, G.D.; Paterno, M.V.; Hewett, T.E. The effects of gender and pubertal status on generalized joint laxity in young athletes. J. Sci. Med. Sport. 2008, 11, 257–263. [Google Scholar] [CrossRef]
- Fukano, M.; Fukubayashi, T.; Banks, S.A. Sex differences in three-dimensional talocrural and subtalar joint kinematics during stance phase in healthy young adults. Hum. Mov. Sci. 2018, 61, 117–125. [Google Scholar] [CrossRef]
- de Sire, A.; Lippi, L.; Ammendolia, A.; Cisari, C.; Venetis, K.; Sajjadi, E.; Fusco, N.; Invernizzi, M. Physical exercise with or without whole-body vibration in breast cancer patients suffering from aromatase inhibitor—Induced musculoskeletal symptoms: A pilot randomized clinical study. J. Pers. Med. 2021, 11, 1369. [Google Scholar] [CrossRef] [PubMed]
- Cloak, R.; Nevill, A.; Day, S.; Wyon, M. Six-week combined vibration and wobble board training on balance and stability in footballers with functional ankle instability. Clin. J. Sport Med. 2013, 23, 384–391. [Google Scholar] [CrossRef]
- Cardinale, M.; Bosco, C. The use of vibration as an exercise intervention. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef]
- Pollock, R.D.; Woledge, R.C.; Martin, F.C.; Newham, D.J. Effects of whole body vibration on motor unit recruitment and threshold. J. Appl. Physiol. 2012, 112, 388–395. [Google Scholar] [CrossRef]
- Rendos, N.K.; Jun, H.-P.; Pickett, N.M.; Lew Feirman, K.; Harriell, K.; Lee, S.Y.; Signorile, J.F. Acute effects of whole body vibration on balance in persons with and without chronic ankle instability. Res. Sports Med. 2017, 25, 391–407. [Google Scholar] [CrossRef]
- Chang, W.-D.; Chen, S.; Tsou, Y.-A. Effects of whole-body vibration and balance training on female athletes with chronic ankle instability. J. Clin. Med. 2021, 10, 2380. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.-R.; Jeong, M.-B.; Lee, D.-W. The effect of whole body vibration exercise on ankle joint spasticity patients with chronic stroke. J. Korean Phys. Ther. 2018, 30, 135–140. [Google Scholar] [CrossRef]
- Hosea, T.M.; Carey, C.C.; Harrer, M.F. The gender issue: Epidemiology of ankle injuries in athletes who participate in basketball. Clin. Orthop. Relat. Res. 2000, 372, 45–49. [Google Scholar] [CrossRef]
- Brumitt, J.; Mattocks, A.; Loew, J.; Lentz, P. Preseason functional performance test measures are associated with injury in female college volleyball players. J. Sport Rehab. 2020, 29, 320–325. [Google Scholar] [CrossRef]
- McAlindon, T.E.; LaValley, M.P.; Harvey, W.F.; Price, L.L.; Driban, J.B.; Zhang, M.; Ward, R.J. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: A randomized clinical trial. JAMA 2017, 317, 1967–1975. [Google Scholar] [CrossRef] [PubMed]
- Sandler, E.B.; Condon, K.; Field-Fote, E.C. Efficacy of transcutaneous spinal stimulation versus whole body vibration for spasticity reduction in persons with spinal cord injury. J. Clin. Med. 2021, 10, 3267. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.G.; Chui, C.S.; Chow, S.K.H.; Cheung, W.-H.; Wong, R.M.Y. Effects of whole-body vibration therapy on knee Osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 2022, 54, jrm00266. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves de Oliveira, R.; Coutinho, H.M.E.L.; Martins, M.N.M.; Bernardo-Filho, M.; de Sá-Caputo, D.d.C.; Campos de Oliveira, L.; Taiar, R. Impacts of whole-body vibration on muscle strength, power, and endurance in older adults: A systematic review and meta-analysis. J. Clin. Med. 2023, 12, 4467. [Google Scholar] [CrossRef]
- Amoako, A.O.; Pujalte, G.G.A. Osteoarthritis in young, active, and athletic individuals. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2014, 7, 27–32. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Wang, P.; Yang, L.; Liu, C.; Wei, X.; Yang, X.; Zhou, Y.; Jiang, H.; Lei, Z.; Reinhardt, J.D.; He, C. Effects of whole body vibration exercise associated with quadriceps resistance exercise on functioning and quality of life in patients with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2016, 30, 1074–1087. [Google Scholar] [CrossRef]
- Park, Y.G.; Kwon, B.S.; Park, J.-W.; Cha, D.Y.; Nam, K.Y.; Sim, K.B.; Chang, J.; Lee, H.J. Therapeutic effect of whole body vibration on chronic knee osteoarthritis. Ann. Rehabil. Med. 2013, 37, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Lai, Z.; Lee, S.; Hu, X.; Wang, L. Effect of adding whole-body vibration training to squat training on physical function and muscle strength in individuals with knee osteoarthritis. J. Musculoskelet. Neuron Interact. 2019, 19, 333–341. [Google Scholar]
- Webster, K.E.; Wittwer Je Fau-Feller, J.A.; Feller, J.A. Validity of the GAITRite walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture 2005, 22, 317–321. [Google Scholar] [CrossRef] [PubMed]
- McConnell, S.; Kolopack, P.; Davis, A.M. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): A review of its utility and measurement properties. Arthritis Rheum. 2001, 45, 453–461. [Google Scholar] [CrossRef]
- Cibulka, M.T.; Winters, K.; Kampwerth, T.; McAfee, B.; Payne, L.; Roeckenhaus, T.; Ross, S.A. Predicting foot progression angle during gait using two clinical measures in healthy adults, a preliminary study. Int. J. Sports Phys. Ther. 2016, 11, 400–408. [Google Scholar] [PubMed]
- Cameron, K.L.; Hsiao, M.S.; Owens, B.D.; Burks, R.; Svoboda, S.J. Incidence of physician-diagnosed osteoarthritis among active duty United States military service members. Arthritis Rheum. 2011, 63, 2974–2982. [Google Scholar] [CrossRef]
- Rehn, B.; Lidström, J.; Skoglund, J.; Lindström, B. Effects on leg muscular performance from whole-body vibration exercise: A systematic review. Scand. J. Med. Sci. Sports 2007, 17, 2–11. [Google Scholar] [CrossRef]
- Silva, P.; Seabra, E.; Mendes, J. Design, development, and validation of a whole-body vibration measurement device. ASME Open J. Eng. 2022, 1, 011035. [Google Scholar] [CrossRef]
- Fitzgerald, G.K.; Oatis, C. Role of physical therapy in management of knee osteoarthritis. Curr. Opin. Rheumatol. 2004, 16, 143–147. [Google Scholar] [CrossRef]
- Chan, C.W.; Rudins, A. Foot Biomechanics during Walking and Running. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 1994; pp. 448–461. [Google Scholar]
- Sierra-Guzmán, R.; Jiménez, J.F.; Ramírez, C.; Esteban, P.; Abián-Vicén, J. Effects of synchronous whole body vibration training on a soft, unstable surface in athletes with chronic ankle instability. Int. J. Sports Med. 2017, 38, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Kim, E.; Choi, H. Effects of a 6-week neuromuscular rehabilitation program on Ankle-Evertor strength and postural stability in elite women field hockey players with chronic ankle instability. J. Sport Rehab. 2017, 26, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Wu, X.; Clark, C.C.; Barton, V.; Chen, S.; Liu, S.; Zhou, X.; Xu, C.; Ma, T.; Qi, B.; et al. The effect of whole body vibration on sensorimotor deficits in people with chronic ankle instability: A systematic review and meta-analysis. Clin. Rehabil. 2022, 36, 1016–1031. [Google Scholar] [CrossRef] [PubMed]
- Bonanni, R.; Cariati, I.; Romagnoli, C.; D’Arcangelo, G.; Annino, G.; Tancredi, V. Whole body vibration: A valid alternative strategy to exercise? J. Funct. Morphol. Kinesiol. 2022, 7, 99. [Google Scholar] [CrossRef]
- Guler, H.; Karazincir, S.; Turhanoglu, A.D.; Sahin, G.; Balci, A.; Ozer, C. Effect of coexisting foot deformity on disability in women with knee osteoarthritis. J. Am. Podiatr. Med. Assoc. 2009, 99, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Corum, M.; Basoglu, C.; Yakal, S.; Sahinkaya, T.; Aksoy, C. Effects of whole body vibration training on isokinetic muscular performance, pain, function, and quality of life in female patients with patellofemoral pain: A randomized controlled trial. J. Musculoskelet. Neuron Interact. 2018, 18, 473–484. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | HBE Group (n = 21) | HBE + WBV Group (n = 21) | p-Value | Effect Size (η2) |
|---|---|---|---|---|
| Age (yr) | 20.76 ± 0.32 | 21.48 ± 0.22 | 0.08 | 0.07 |
| BMI (kg/m2) | 22.35 ± 0.89 | 23.50 ± 0.74 | 0.33 | 0.03 |
| Variable | HBE Group | HBE + WBV Group | Group X Time Interaction p-Value | Pb) between Groups | Effect Size (η2) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | After Six Weeks | MD (95%CI) | Pa) within Group | Baseline | After Six Weeks | MD (95%CI) | Pa) within Group | ||||
| Toe angle | −1.10 ± 0.94 | −0.81 ± 0.99 | 0.29 (−0.07–0.64) | 0.11 | −1.05 ± 0.68 | 2.14 ± 0.67 | 3.19 (1.59–4.79) | <0.001 | 0.04 | 0.02 | 0.13 |
| WOMAC index | 8.66 ± 2.70 | 6.64 ± 2.39 | −2.03 (−5.61–4.56) | 0.25 | 9.89 ± 1.56 | 5.31 ± 1.89 | −4.57 (−10.68–1.53) | 0.13 | 0.12 | 0.66 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abd-Eltawab, A.E.; Elbandrawy, A.M.; Ghanem, H.B.; Ebrahim, H.A.; El-Sherbiny, M.; Ibrahim, A.M.; Eladl, M.A.; Elsherbini, D.M.A. Whole-Body Vibration Impacts on the Degree of Toe Angle and Its Correlation to the Knee Osteoarthritis Index during Level Walking among Female University Students: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 5735. https://doi.org/10.3390/jcm12175735
Abd-Eltawab AE, Elbandrawy AM, Ghanem HB, Ebrahim HA, El-Sherbiny M, Ibrahim AM, Eladl MA, Elsherbini DMA. Whole-Body Vibration Impacts on the Degree of Toe Angle and Its Correlation to the Knee Osteoarthritis Index during Level Walking among Female University Students: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(17):5735. https://doi.org/10.3390/jcm12175735
Chicago/Turabian StyleAbd-Eltawab, Amany E., Asmaa M. Elbandrawy, Heba B. Ghanem, Hasnaa A. Ebrahim, Mohamed El-Sherbiny, Ateya Megahed Ibrahim, Mohamed Ahmed Eladl, and Dalia Mahmoud Abdelmonem Elsherbini. 2023. "Whole-Body Vibration Impacts on the Degree of Toe Angle and Its Correlation to the Knee Osteoarthritis Index during Level Walking among Female University Students: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 17: 5735. https://doi.org/10.3390/jcm12175735